Air Pollution and Preterm Birth: A Scoping Review Focused on Preterm Birth Phenotype and Specific Lengths of Gestation
Lindsey Abellard, Vy Le, Timothy D. Nelin, Sara B. DeMauro, Kristan Scott, Jane E. Clougherty, Heather H. Burris

TL;DR
This review finds that most studies on air pollution and preterm birth do not break down the different types and lengths of preterm birth, limiting understanding of how pollution affects these outcomes.
Contribution
The paper highlights a critical gap in the literature by showing that few studies analyze specific preterm birth phenotypes or gestational lengths in relation to air pollution.
Findings
Only 25% of studies report on specific lengths of gestation related to preterm birth.
Just 6.7% of studies examine specific preterm birth phenotypes (spontaneous or medically indicated).
Associations between pollutants and preterm birth vary in magnitude and direction across studies.
Abstract
What are the main findings? •While there have been over 100 studies of ambient PM2.5 and NO2 with preterm birth since 2011, only one in four studies reports on specific lengths of gestation.•Even fewer (one in fifteen) report on specific preterm birth phenotypes (i.e., spontaneous or medically indicated). While there have been over 100 studies of ambient PM2.5 and NO2 with preterm birth since 2011, only one in four studies reports on specific lengths of gestation. Even fewer (one in fifteen) report on specific preterm birth phenotypes (i.e., spontaneous or medically indicated). What are the implications of the main finding? •Preterm birth is heterogeneous with respect to lengths of gestation as well as the etiology, but is often analyzed as a single outcome in environmental health studies.•Future studies of air pollution and other environmental exposures with preterm birth should…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
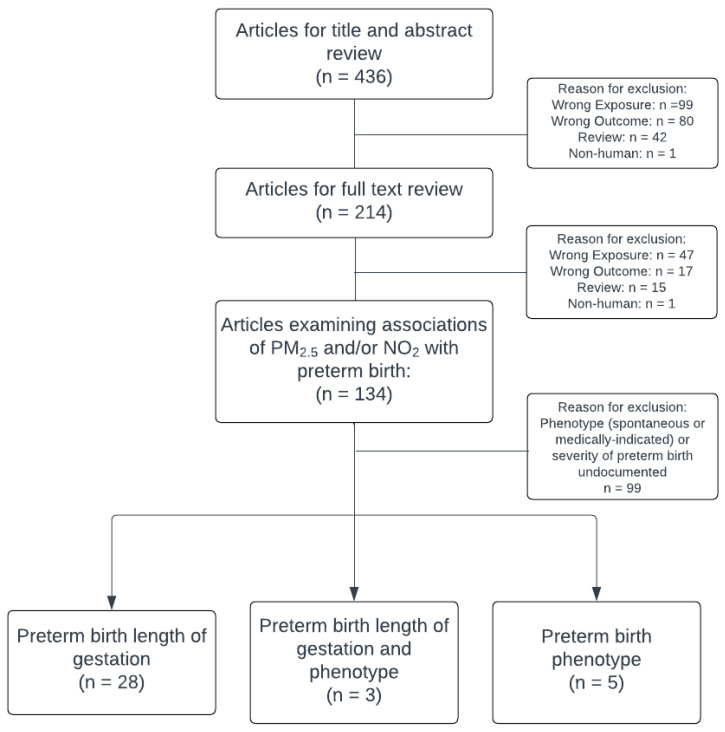 Figure 1
Figure 1- —National Institutes of Health (NIH) Environmental influences on Child Health Outcomes (ECHO) Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAir Quality and Health Impacts · Neonatal Respiratory Health Research · Pregnancy and preeclampsia studies
1. Introduction
Air pollution represents an important macro-environmental exposure associated with several health outcomes, including adverse pregnancy outcomes. Air pollution is a complex mixture of gases, chemicals, and particulate matter emitted through natural processes and human activities such as fossil fuel combustion. Two measures of air pollution, particulate matter < 2.5 microns in diameter (PM_2.5_) and nitrogen dioxide (NO_2_), have been consistently linked to preterm birth (PTB), a major contributor to infant morbidity and mortality [1]. Based on these data, the American College of Obstetricians and Gynecologists and the American Academy of Pediatrics have released statements regarding the impact of environmental factors, especially ambient air pollution, on perinatal health outcomes [2,3].
Despite the widespread recognition of the harms of air pollution on perinatal outcomes, mechanisms linking air pollution exposure to PTB are unknown. Discovering mechanisms by which pollution contributes to PTB risk is especially challenging because PTB is a composite phenotype that can range from spontaneous (sPTB), from preterm labor or rupture of membranes, to medically indicated (mPTB), for conditions such as severe preeclampsia or impaired fetal growth [4]. Furthermore, PTB is heterogeneous with respect to lengths of gestation, ranging from 20 to 36 completed weeks, and is commonly classified as moderate to late preterm (32 to <37 weeks), very preterm (28 to <32 weeks), and extremely preterm (<28 weeks) [5]. Due to variation in the prevalence of morbidities leading into pregnancy, populations are more or less susceptible to conditions that may lead to mPTB due to maternal health (e.g., hypertensive disorder of pregnancy) or fetal health (e.g., fetal growth restriction). Due to differences in exposure and susceptibility, air pollution exposure–outcome associations may vary [6].
Taken together, these methodological challenges underscore that pregnancy is a uniquely time-limited period characterized by substantial cohort attrition and multifaceted risk, making rigorous and bias-aware approaches essential in perinatal research [7]. Given the variability in PTB phenotypes and lengths of gestation, this scoping review synthesizes existing evidence on associations of PM_2.5_ and NO_2_ with PTB phenotype and lengths of gestation.
2. Methods
2.1. Scope of Review
We evaluated studies examining associations of PM_2.5_ and NO_2_ exposure with PTB phenotypes and specific lengths of PTB gestation. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
2.2. Research Question
What proportion of studies investigating associations of prenatal exposure to PM_2.5_ or NO_2_ with PTB consider phenotypes or specific lengths of gestation?
2.3. Eligibility Criteria and Study Selection
Studies published between 1 January 2011 and 28 February 2024 were deemed eligible for inclusion. Stieb et al. published a comprehensive systematic review and meta-analysis of ambient air pollution, birth weight, and PTB in 2012, including studies published through January 2011 [8]. We were specifically interested in the more recent literature and its focus, or lack thereof, on PTB phenotypes and specific lengths of gestation, and chose to include only studies after the Stieb review. Studies that included either PM_2.5_ or NO_2_ and the outcome of PTB were included for abstract and title review. A literature search was performed using PubMed to identify studies published in English. We used the following syntax and Medical Subject Headings (MeSH) terms for our search: (“PM_2.5_” [All Fields] OR “NO_2_” [All Fields] OR “Particulate matter” [MeSH Terms] OR “Air Pollution” [MeSH Terms:noexp]) AND (“Premature Birth” [MeSH Terms] OR “infant, premature” [MeSH Terms] OR “preterm delivery” [All Fields] or “preterm birth” [All Fields]). There were no sample size or geographic inclusion or exclusion criteria. Two independent research assistants (LA, VL) performed a title and abstract review followed by a preliminary full-text review, excluding review articles, articles that investigated non-human subjects, articles that did not include PM_2.5_ or NO_2_, and articles that did not include PTB as an outcome. Secondary, full-text review identified articles that specified PTB phenotype or specific lengths of gestation as outcome measures. Any discrepancies in study selection were resolved through consensus and reviewed by a neonatologist (TDN). Of note, we did not mandate the use of singular definitions for specific lengths of gestation, such as the World Health Organization categories of extremely, very, and moderate to late PTB. Instead, we included manuscripts with any specific distinctions made among various lengths of gestation.
2.4. Study Categorization
The primary outcome was whether a study evaluated either PTB phenotype or specific lengths of gestation. We categorized articles based on the exposures used and the outcomes measured. We then classified each study as positive, negative, null, or mixed with respect to results and reported whether they evaluated specific windows of exposure, such as trimester-specific associations.
3. Results
We identified 436 eligible articles that met our search criteria within the study period (Figure 1). We excluded 222 articles in title and abstract review for being a review (n = 42), focusing on non-human subjects (n = 1), or including the wrong exposure (n = 99) or outcome (n = 80). We further excluded 80 articles in preliminary full text review for being a review (n = 15), non-human subjects research (n = 1), or including the wrong exposure (n = 47) or outcome (n = 17). Of the remaining 134 studies, 36 (26.9%) included PTB phenotype or specific lengths of gestation; five reported on phenotype alone, 28 reported on lengths of gestation alone, and three reported on both phenotype and lengths of gestation. Given the substantial difference in PM_2.5_ and NO_2_ exposures between studies conducted in China and those conducted elsewhere, results are presented separately by geographic location in each sub-section below.
3.1. Studies Reporting PTB Phenotype (sPTB or mPTB)
Table 1, Table 2 and Table 3 display studies that analyzed PTB phenotype (n = 5 without specific lengths of gestation) [9,10,11,12,13]. Studies of PM_2.5_ in Australia, Israel, New York City and Philadelphia were largely null with respect to sPTB or mPTB, with the exception of one study in Victoria, Australia that reported 4% higher risk of sPTB per IQR increment of PM_2.5_ exposure. The three studies of NO_2_ with PTB phenotype were outside of China and reported no increased risk (Table 1).
A cohort of 1515 twins in Shanghai, China reported that PM_2.5_ exposure was associated with 48% higher odds of sPTB per interquartile range (IQR) increase in PM_2.5_ during the second semester (OR 1.48; 95% CI: 1.06, 2.05) while associations in the first and third trimesters and entire pregnancy were null (Table 3) [12]. In another study of 179,385 singleton births in Shanghai, China, PM_2.5_ exposure in the third trimester had the strongest and most consistent association with sPTB (aOR 1.042; 95% CI: 1.018, 1.065) [13].
3.2. Studies Reporting Positive Findings with PTB Specific Lengths of Gestation
Table 4, Table 5, Table 6 and Table 7 display studies that measured specific lengths of gestation (n = 28, without PTB phenotype) [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44]. There were 12 studies that consistently found positive associations of PM_2.5_ or NO_2_ exposure with specific lengths of gestation. Often, effect estimates were strongest for very PTB.
3.3. Studies Reporting Positive Findings with Specific Lengths of Gestation—PM2.5
Sheridan et al. analyzed over two million births in California and positive associations with PTB (HR 1.12; 95% CI: 1.09, 1.14), moderate PTB (HR 1.11; 95% CI: 1.09, 1.14), and very PTB (HR 1.19; 95% CI: 1.14, 1.25) per 10 μg/m^3^ increment of PM_2.5_ exposure over the entire pregnancy (Table 4) [19]. A study in Florida also reported a positive association; each IQR increment of PM_2.5_ exposure over the entire pregnancy was associated with very PTB (aOR 1.082; 95% CI: 1.048, 1.117) [22]. A nested case–control population in California observed slightly stronger associations of PM_2.5_ with moderate PTB compared to very PTB [26]. In an ecological study of 5 million births in France, associations of 7-year averaged, spatially resolved PM_2.5_ exposure were analyzed with PTB length of gestation revealing moderate positive associations with very early and extreme PTB [30]. In a time-stratified case-crossover study investigating short-term increases in PM_2.5_ during the cold season (November–April) in 196,970 singleton pregnancies in San Joaquin Valley, CA, per IQR increment, PM_2.5_ exposure was associated with a 5–6% increased odds of very PTB beginning 3 days prior to birth (lag 3), but no significant associations were detected with moderate PTB [17].
A retrospective cohort in Henan Province, China observed a 9.8% increase in early PTB < 34 weeks’ gestation and an 18.3% increase in late PTB between 34 and 36 weeks’ gestation per standard deviation increment of PM_2.5_ exposure (Table 6) [47]. A study of 2101 births in Wuhan, China also found that the strongest associations were with very PTB [47]. Another Chinese study of more than 2 million births reported that third trimester exposures had the strongest association with very and moderate PTB [21,22]. In contrast, another nationwide study of singleton births in China found that PM_2.5_ exposure was most associated with late PTB, followed by moderate PTB, and very PTB [36].
3.4. Studies Reporting Positive Findings with Specific PTB Lengths of Gestation—NO2
Similar findings were reported for exposure to NO_2_ and PTB. A 2011 retrospective cohort study reported a significant positive association per IQR increment of NO_2_ with very PTB in Los Angeles (aOR 1.46; 95% CI: 1.11, 1.92) and Orange County (aOR 1.43; 95% CI: 1.02, 2.01) (Table 5) [29]. A retrospective study in the San Joaquin Valley of California of 252,205 live births by Weber et al. found a slight positive association with NO_2_ exposure during entire pregnancy with PTB at 34–36 weeks among individuals without hypertension (aOR 1.07; 95% CI: 1.04, 1.11 per IQR increase in NO_2_) [35]. Genin et al. reported a positive association of NO_2_ exposure with extreme PTB (RR 1.114; 95% CI: 1.094, 1.135), very PTB (RR 1.046; 95% CI: 1.034, 1.059), and moderate PTB (RR 1.011; 95% CI: 1.006, 1.016) per each unit increase in NO_2_ [30]. In a study investigating PM_2.5_ exposure and proximity to power plants in California, Ha et al. observed higher adjusted odds of PTB (aOR 1.018; 95% CI: 1.013, 1.23) and very PTB (aOR 1.022; 95% CI: 1.010, 1.034) for each 5 km closer residential proximity to a power plant (Table 5) [21].
The same retrospective cohort in Henan Province, China, reported a slight positive association of each standard deviation of total pregnancy NO_2_ exposure with early PTB (aOR 1.682; 95% CI: 1.623, 1.744) and late PTB (aOR 1.593; 95% CI: 1.559, 1.627) (Table 7) [47]. In Tianjin, China, Chen et al. measured associations of exposure to the proportion of days with daily average NO_2_ above the threshold set by the Ambient Air Quality Standards of China (80 μg/m^3^) throughout the entire pregnancy, with PTB length of gestation and reported higher risks of moderate, very, and extreme PTB [45].
3.5. Studies Reporting Mixed Findings with Specific PTB Lengths of Gestation—PM2.5
A time-stratified case-crossover study of 24,001 singleton live births in Beijing, China measured average exposure during the week before pregnancy and found 5% higher odds of very PTB per 10 µg/m^3^ with no significant associations for moderate PTB (Table 6) [37].
3.6. Studies Reporting Mixed Findings with Specific PTB Lengths of Gestation—NO2
In a study of 2,928,515 live births in Canada, Stieb et al. reported a positive association of NO_2_ exposure over the entire pregnancy with extreme PTB but null associations with PTB later in gestation (Table 5) [48]. A cohort of 23,086 births in Scotland reported higher risk of very PTB (RR 1.013; 95% CI: 1.00–1.03), but not moderate PTB, per 1 µg/m^3^ of NO_2_ residential exposure [34]. Mendola et al. investigated associations of PM_2.5_ and Nitrogen Oxides (NOx) exposure throughout pregnancy with early PTB < 34 weeks’ gestation and found associations with early PTB among pregnant individuals with asthma (aOR 1.11; 95% CI: 1.01, 1.22) per IQR of PM_2.5_, but a null association among pregnant individuals without asthma. For NOx exposure, the authors reported lower odds of early PTB per IQR of exposure throughout pregnancy (aOR 0.84; 95% CI: 0.79, 0.90) [32].
3.7. Studies Reporting Null Findings of PM2.5 and NO2 with Specific PTB Lengths of Gestation
Several studies reported null findings for the association of PM_2.5_ with PTB length of gestation. Arroyo detected no association of PM_2.5_ or NO_2_ with very PTB or extreme PTB in a study of 298,705 live births in Madrid [27]. In a study of 103,961 singleton births in Florida, Salihu et al. reported a null association of PM_2.5_ exposure with very PTB (Table 4) [24].
A study of 196,780 singleton births in the Huai River Basin of China found no significant associations of PM_2.5_ exposure with moderate PTB or very PTB (Table 6) [38]. Guo et al. reported null associations between preconception PM_2.5_ exposure and extreme PTB, moderate PTB, and very PTB in a birth cohort of 10,916 infants in Tianjin, China [40].
3.8. Studies Reporting Both PTB Phenotype and Specific PTB Lengths of Gestation
There were just three studies that analyzed both PTB phenotype and specific lengths of gestation [14,15,16]. A study in New South Wales, Australia of 1,318,570 births found that longer-term exposure to PM_2.5_ was associated with sPTB (HR 1.07; 95% CI: 1.02, 1.12) (Table 1), extreme sPTB (HR 1.34; 95% CI: 1.10, 1.64) and very sPTB (HR 1.20; 95% CI: 1.02, 1.43) per 5 µg/m^3^ of PM_2.5_, while no significant association was detected for moderate to late sPTB (Table 4) [14]. In a study of 285,294 singleton births in New York City, Johnson et al. found no association of first or second trimester PM_2.5_ exposure with sPTB or mPTB and no association of PM_2.5_ with early PTB. Similarly, the authors reported no significant association of first or second trimester NO_2_ exposure with early sPTB or early PTB; however, the authors reported a significant negative association of second trimester NO_2_ exposure with sPTB [15].
In a study of 19,900 singleton births in Shanghai, China, Jiang et al. found no significant association of whole-pregnancy PM_2.5_ with sPTB (Table 3) [16]. However, they observed higher odds of sPTB for third trimester exposures (aOR 1.53; 95% CI: 1.17, 2.01) per IQR of PM_2.5_. The authors also reported a significant association of PM_2.5_ exposure throughout the entire pregnancy with early PTB (aOR 1.80; 95% CI: 1.47, 2.19) and late PTB (aOR 1.35; 95% CI: 1.18, 1.55) per IQR of PM_2.5_, with significant associations also existing for first, second, and third trimester PM_2.5_ exposures with early and late PTB (Table 6).
4. Discussion
Among the 134 studies linking PM_2.5_ or NO_2_ to PTB, fewer than one-third addressed either phenotype or specific lengths of gestation. Studies of PTB phenotype are exceedingly rare; just five (3.7%) specify examining either sPTB or mPTB. Findings varied among studies that examined phenotype or specific lengths of gestation; while often positive, some have mixed results and others are null. Results likely vary from differences in exposure timing and level, outcome definition, population, covariates included, and statistical approach. One included study examined twins, a population with inherently higher preterm birth risk; moreover, chorionicity, an important determinant of PTB risk among twins, was not reported, limiting interpretability of these results [12]. Given the extent of heterogeneity across studies in exposure timing, magnitude, and measurement, as well as in outcome definitions and analytic methods, a formal meta-analysis would not be interpretable, as it would synthesize data that are not directly comparable.
4.1. Implications of Dearth of Information Regarding PTB Phenotype
While a fair number of studies examine specific lengths of gestation, few examined the reason for PTB. There are likely several reasons for the dearth of data in this area.
One major challenge in investigating air pollution and PTB is the difficulty of phenotyping PTB. PTB is not a singular entity—it arises from diverse and often overlapping pathophysiologic pathways [46,49,50,51,52,53,54]. Broadly, PTB can be categorized as spontaneous, resulting from spontaneous labor or preterm rupture of membranes, or medically indicated, typically due to maternal or fetal conditions such as preeclampsia or fetal growth restriction [53,54,55]. However, in practice, clear-cut differentiation is not always feasible. A pregnancy complicated by fetal growth restriction may lead to mPTB, but that same mother might also be at higher risk for spontaneous labor. Similarly, hypertensive disorders may co-exist with spontaneous membrane rupture, blurring categorical lines.
Studies rarely include standardized or validated algorithms for phenotype assignment and often rely on available administrative codes or chart abstraction with varying degrees of granularity and accuracy [56]. This heterogeneity introduces substantial variability into phenotypic outcome classification [57,58]. By aggregating all PTB cases into a single outcome, most studies risk obscuring important distinctions in biological mechanisms and susceptibility to environmental exposures. If air pollution is associated with specific PTB phenotypes, aggregation could dilute true associations or mask them entirely. Conversely, combining phenotypes with different risk factors and confounders (e.g., socioeconomic status, access to prenatal care, or smoking) may introduce spurious associations, thereby compromising causal inference. Precision in phenotyping is essential to advance mechanistic understanding and to design targeted public health interventions. Without refined outcome definitions, we risk both misclassification and missed opportunities to improve pregnancy outcomes.
A wide range of factors influence the likelihood of sPTB, including genetic predisposition, maternal health conditions, and lifestyle behaviors [55]. Even without fully elucidating the mechanisms of sPTB, identifying associations with air pollution exposure remains critical for informing population-level prevention strategies. In contrast, mPTB is most commonly prompted by conditions such as severe preeclampsia and fetal growth restriction—vascular complications that may themselves be influenced by air pollution. For example, in a study of 34,705 singleton births in Pittsburgh, PA, Lee et al. reported associations between PM_2.5_ exposure and both preeclampsia and gestational hypertension [59]. Urban residence, often linked to higher air pollution levels, along with exposures to other stressors associated with urban life in the U.S., may increase the risk of hypertensive disorders of pregnancy and, in turn, the likelihood of mPTB. Moreover, chronic conditions such as pre-pregnancy hypertension and obesity, which also elevate mPTB risk, may be exacerbated by long-term pollution exposure [60,61].
4.2. Reasons for Variation in Findings in Studies That Examine PTB Phenotype or Specific Lengths of Gestation
4.2.1. Duration and Timing of Exposure
Across studies, the timing of air pollution exposure varied considerably, with associations assessed over diverse intervals ranging from short-term (e.g., days prior to delivery), to trimester-specific windows, to entire pregnancy averages. This heterogeneity reflects both differing methodological approaches (e.g., time-series analyses, case–control, ecological regression, logistic regression, Cox regression, Poisson regression, etc.) and underlying hypotheses about when the maternal–fetal dyad may be most vulnerable. While early pregnancy may represent a critical window for placentation and fetal programming, late gestation may be more relevant for triggering labor [62]. Importantly, not all studies align regarding which trimester confers the highest risk, and findings often diverge by pollutant, population, and outcome definition. These inconsistencies highlight the complexity of understanding exposure timing with PTB risk. Moreover, pollution metrics also differ: some report IQR increment, others per 10 µg/m^3^, and some use standardized z-scores. These discrepancies further complicate meta-analytic synthesis and interpretation of effect sizes. This heterogeneity underscores the need for standardized, granular assessments to identify critical periods to clarify potential mechanisms. Future work should also consider how differences in exposure intervals, population demographics, and PTB classification may shape observed associations.
4.2.2. Difference in Air Pollution Exposures and Shape of the Relationship
Ambient PM_2.5_ and NO_2_ exposures vary across the world [63,64]. Huang et al. highlight this, as the annual mean PM_2.5_ was less than 15 µg/m^3^ in the United States in 2015, while it was 58.4 µg/m^3^ in China [65]. This heterogeneity in exposure level may explain variability in results across studies. When interpreting the findings of the included studies, the relationship of PM_2.5_ with PTB is often modeled assuming a linear relationship, but exposure to pollutants at extremely high concentrations likely does not cause the same biological effect as pollutants exposure at low concentrations. In addition, the pollution burden differs substantially by location. Studies conducted in regions with higher concentrations of PM_2.5_ or NO_2_ may observe different dose–response relationships compared to studies in cleaner air environments. Furthermore, PM_2.5_ is highly heterogeneous in terms of pollution source and thus composition and PM_2.5_ species may vary with respect to their biologic impacts. For example, PM_2.5_ composition varies by geographic region in the United States with heavy metals in major urban metropolitan areas from traffic and industrial sources, nitrates and sulfates from coal emissions in Pennsylvania, and organic and elemental carbon from wildfire smoke in the West, while in China PM_2.5_ is sulfate-heavy from coal-based emissions [66,67,68,69,70]. Therefore, results of studies conducted in countries with high pollution burden, such as China, may not be generalizable to the United States. The inclusion of different countries and pollutant exposures complicates the interpretation of exposure–outcome relationships.
4.2.3. Spatial Units
The spatial resolution at which exposure is assigned plays a crucial role in accuracy and inference. Some studies assign exposure based on large administrative regions (e.g., counties, ZIP codes), which may mask significant within-area heterogeneity. Others use fine-scale exposure surfaces (e.g., 1 × 1 km grids or address-level modeling), offering more precise estimation of ambient exposure but often limited to urban or high-resource settings. However, this should be interpreted with nuance as a 1 × 1 km exposure grid has different implications for PM_2.5_ compared to NO_2_ [71,72].
Moreover, exposure is generally assigned based on the maternal residence at delivery, which may not reflect the residential location across all trimesters or account for time spent in other environments (e.g., workplaces, community settings, stores, on vacation). This introduces potential exposure misclassification, especially for time-varying or transient populations. In addition, people often change residences during pregnancy and studies rarely incorporate residential mobility data, despite its relevance for air pollution exposure.
4.2.4. Population and Analytic Approach
Analytical methods used to study air pollution and PTB also vary considerably. Some studies apply individual-level multivariable logistic regression or Cox proportional hazards models, adjusting for sociodemographic and clinical confounders. Others employ spatial ecological models, such as Bayesian Poisson regressions, especially when individual-level data are unavailable. Time-stratified case-crossover designs were used to study short-term effects of air pollution spikes near delivery while limiting confounding [73,74,75].
Outcome definitions also varied across studies. Some studies used a binary definition of PTB (<37 weeks), while others stratified outcomes by gestational age bands (e.g., <28 weeks, 28–32 weeks, 32–36 weeks). Few studies treated gestational age as a continuous variable. These distinctions are important, as risk factors and biological plausibility may differ across the gestational age spectrum [6,76]. Furthermore, few studies examined temporal trends in PTB risk in the context of changing pollution levels or health policies. The use of numerous modeling strategies—coupled with differing definitions of exposure and outcome—complicates efforts to synthesize findings and draw overarching conclusions about the association of PM_2.5_ and NO_2_ exposure with PTB phenotype and length of gestation.
Another source of heterogeneity across studies may stem from live birth bias. Many investigations of air pollution and PTB include only live births, excluding fetal losses or stillbirths that may themselves be related to higher pollution exposure [77]. If exposure increases the risk of pregnancy loss before viability, the remaining live birth cohort may represent a healthier or less susceptible subset, resulting in associations that do not capture all of the risk or accurately quantify effect sizes. This selection bias is especially concerning when exposure timing or intensity affects both early fetal survival and gestational length. Addressing live birth bias through designs that incorporate fetal loss data or sensitivity analyses will improve causal inference in future studies. Specific recommendations to enhance the rigor of studies focused on pollution and PTB are presented in the Supplementary Materials.
4.3. Conclusion and Implications for Future Research and Public Health
Although many studies report associations of air pollution with PTB, findings vary because of differences in study design, exposure context, and outcome definition. Few studies of common pollutants such as PM_2.5_ and NO_2_ have examined specific PTB phenotypes (sPTB or mPTB). Lack of outcome specificity limits the understanding of potential mechanisms by which pollution may shorten gestation. Importantly, associations could be missed or diluted. Furthermore, without understanding of pollutants’ associations with distinct phenotypes, targeted exposure mitigation efforts for communities at varying risk for these distinct outcomes is difficult and limits personalized and community-specific public health prevention strategies. Future work to delineate pollution’s contribution to specific PTB phenotypes will enhance efforts to improve birth outcomes around the globe.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Veber T. Dahal U. Lang K. Orru K. Orru H. Industrial Air Pollution Leads to Adverse Birth Outcomes: A Systematized Review of Different Exposure Metrics and Health Effects in Newborns Public Health Rev.202243160477510.3389/phrs.2022.160477536035982 PMC 9400407 · doi ↗ · pubmed ↗
- 2American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice Reducing Prenatal Exposure to Toxic Environmental Agents Obstet. Gynecol.2021138 e 40e 5410.1097/AOG.000000000000444934259492 · doi ↗ · pubmed ↗
- 3Brumberg H.L. Karr C.J. Ambient Air Pollution: Health Hazards to Children Pediatrics 2021147 e 202105148410.1542/peds.2021-05148434001642 · doi ↗ · pubmed ↗
- 4Ananth C.V. Vintzileos A.M. Epidemiology of Preterm Birth and Its Clinical Subtypes J. Matern.-Fetal Neonatal Med.20061977378210.1080/1476705060096588217190687 · doi ↗ · pubmed ↗
- 5World Health Organization Preterm Birth Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth(accessed on 31 October 2025)
- 6Chang H.H. Warren J.L. Darrow L.A. Reich B.J. Waller L.A. Assessment of Critical Exposure and Outcome Windows in Time-to-Event Analysis with Application to Air Pollution and Preterm Birth Study Biostatistics 20141650952110.1093/biostatistics/kxu 06025572998 PMC 5963471 · doi ↗ · pubmed ↗
- 7Neophytou A.M. Kioumourtzoglou M.A. Goin D.E. Darwin K.C. Casey J.A. Educational Note: Addressing Special Cases of Bias That Frequently Occur in Perinatal Epidemiology Int. J. Epidemiol.20215033734510.1093/ije/dyaa 25233367719 PMC 8453403 · doi ↗ · pubmed ↗
- 8Stieb D.M. Chen L. Eshoul M. Judek S. Ambient Air Pollution, Birth Weight and Preterm Birth: A Systematic Review and Meta-Analysis Environ. Res.201211710011110.1016/j.envres.2012.05.00722726801 · doi ↗ · pubmed ↗