Capillary Leakage on Ultrasound in Children with Dengue
María Teresa Gutiérrez-Arcos, Carlos Alberto Velasco-Benítez, Daniela Alejandra Velasco-Suárez

TL;DR
This study shows that ultrasound is highly effective at detecting capillary leakage in children with dengue, especially in school-age and adolescent patients with liver involvement.
Contribution
The study demonstrates the high sensitivity of ultrasound for detecting capillary leakage in pediatric dengue patients.
Findings
Ultrasound detected capillary leakage in 95.5% of children with dengue.
School-age/adolescent children and elevated liver enzymes were strongly associated with capillary leakage.
Thrombocytopenia and hypoalbuminemia were common in patients with capillary leakage.
Abstract
Background/Objectives: Dengue is one of the leading causes of morbidity in children in endemic regions. Capillary leakage is the pathophysiological hallmark of severe dengue, and ultrasound has established as a sensitive tool for its early detection. However, evidence in the pediatric population remains limited. The aim of this study was to identify the presence of capillary leakage detected by ultrasound and its associations in children with dengue. Methods: Observational/descriptive/cross-sectional/retrospective study conducted in patients between 6 months and 14 years old with confirmed dengue and warning signs or severe dengue, treated at the Hospital Universitario del Valle in Cali, Colombia, between July 2019 and June 2020. Ultrasound examinations were performed and interpreted by radiologists following an institutional standardized protocol. Associations with capillary leakage…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
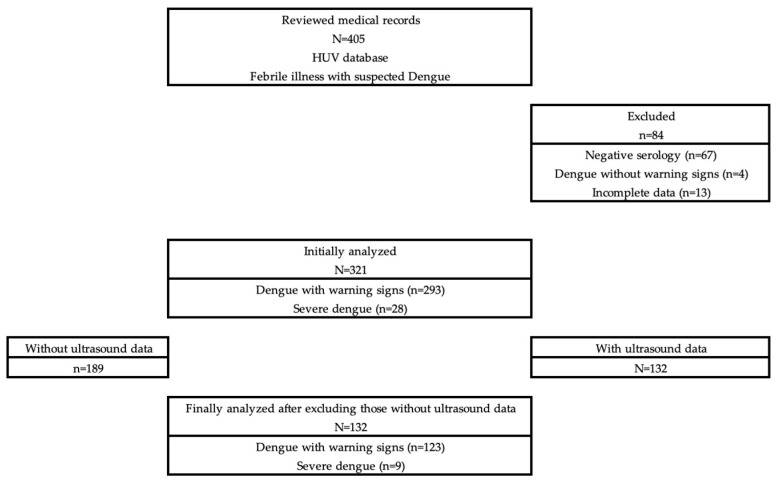 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Mosquito-borne diseases and control · Amoebic Infections and Treatments
1. Introduction
Dengue is a viral disease caused by the DENV, a complex of four distinct serotypes (DENV-1 to DENV-4) [1]. All serotypes can cause acute disease and are transmitted mainly by bites from Aedes aegypti, an anthropophilic mosquito widely distributed in tropical and subtropical regions [2,3].
Dengue is considered one of the most important tropical diseases worldwide, with its incidence increasing more than thirtyfold in recent decades, in parallel with the geographical expansion of the vectors and, therefore, of the virus [4,5]. Dengue epidemics have a significant economic and social impact, imposing high costs on health services, families, and the productive systems of the affected countries [4,6,7].
Approximately 95.0% of dengue cases occur in children under 15 years old, with infants under one year old and children between four and nine years of age being the most likely to develop severe forms of the disease [6,8]. In the endemic regions of Asia and Latin America, including Colombia, about 10.0% of febrile episodes in children under 16 years old correspond to acute dengue infection [5,8]. Of these, about 19.0% of cases in Asia and 11.0% in Latin America require hospitalization [8].
The pathophysiology of dengue is complex and multifactorial [9,10], characterized by systemic involvement and a wide spectrum of clinical manifestations, ranging from asymptomatic cases to severe and unpredictable presentations [2]. The clinical course depends on various factors, such as the host’s immune status, the viral strain, individual genetics, and age [11,12]. Among the most relevant pathophysiological alterations is capillary leak syndrome, which results from endothelial cells being activated by the viral NS1 protein through Toll-like receptor 4 signaling [13,14,15]. This process triggers the release of inflammatory cytokines and alters endothelial permeability and the glycocalyx [2]. The main mediators involved are tumor necrosis factor alpha (TNF-α), interferon gamma (IFN-γ), interleukins IL-2 and IL-8, vascular endothelial growth factor (VEGF), and components of the complement system [15,16]. However, the exact mechanisms that determine the peak vascular permeability during the defervescence phase are not yet fully understood [2].
Increased vascular permeability can manifest in multiple systems, clinically evident from pleural and [17,18] pericardial effusion, ascites, hepatomegaly, splenomegaly, or thickening of the vesicular wall, among other findings [15,17,18,19,20,21,22]. However, these signs often go unnoticed in the early stages of clinical presentation through conventional physical evaluation [15]. In this scenario, capillary leakage is defined as the presence of ultrasound findings compatible with plasma extravasation, such as ascites, pleural effusion, or gallbladder wall thickening [1].
In this context, ultrasound is established as a highly useful noninvasive diagnostic tool to evaluate and manage pediatric patients with dengue virus infection [23,24,25,26]. Its use allows for the early detection of plasma leakage, classification of the severity of clinical presentation, and estimation of the progression risk to severe forms of the disease [25,26]. Although several studies have described ultrasound findings associated with dengue, most have focused on adult populations, while few investigations have characterized capillary leak syndrome in children or identified the risk factors associated with its development [15,27]. Furthermore, much of the available evidence comes from other countries, highlighting the limited information on the clinical and ultrasound behavior of pediatric dengue in Colombia.
Therefore, the objective of this study was to identify the presence of capillary leak syndrome using ultrasound and to explore its possible associations with clinical, laboratory, and imaging variables in pediatric patients with dengue treated at the Hospital Universitario del Valle “Evaristo García” (HUV) in Cali, Colombia.
2. Materials and Methods
An observational, descriptive, cross-sectional, and retrospective study was conducted based on a database of pediatric patients between 6 months and 14 years old treated at the HUV in Cali, Colombia, a referral center in the southwestern part of the country. The patients were diagnosed with acute dengue virus infection, confirmed by serological tests (positive NS1 antigen or positive dengue-specific IgM), and presented warning signs or severe dengue according to the World Health Organization classification [28]. The study period was from 1 July 2019 to 30 June 2020.
From this database, the patient’s medical records were compiled, including sociodemographic (age, sex, and origin), clinical (anthropometric measurements, type and severity of infection, symptoms, and need for intensive care unit (ICU) admission), paraclinical (NS1 antigen, IgM and IgG for dengue, aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin, complete blood count, and coagulation times), imaging (chest X-ray and abdominal ultrasound reports, chest ultrasound, and echocardiogram), and therapeutic variables (administration of albumin and blood products). All ultrasound examinations were performed and interpreted by radiologists from the HUV with training in pediatric ultrasonography, following an institutional standardized protocol to ensure consistency in image acquisition and enhance the reproducibility of the findings.
The information obtained was exported to Stata version 16.0 for statistical analysis. In the univariate analysis, sociodemographic, clinical, paraclinical, imaging, and therapeutic variables were described using measures of central tendency and dispersion (absolute and relative frequencies, means, and standard deviations). Bivariate analysis was performed using the chi-squared (χ^2^) test to explore associations between the presence of capillary leakage and the aforementioned variables. Odds ratios (ORs) were calculated with their respective 95% confidence intervals (95% CIs). Differences were considered statistically significant when the p-value was less than 0.05.
This project was endorsed by the Ethics Committee of the HUV in Cali, Colombia, with approval number 065-2019.
3. Results
A total of 405 children under 14 years old who presented to the Emergency Department of the HUV in Cali, Colombia, with clinical suspicion of acute dengue virus infection were identified. In total, 84 children were excluded: 67 with negative dengue serology, 4 with dengue without warning signs, and 13 with incomplete data. This resulted in 321 children with confirmed dengue and warning signs or severe dengue. Among these 321 patients, 189 were excluded from the main analysis due to the absence of ultrasound data, leaving a final study population of 132 children, including 123 with dengue with warning signs and 9 with severe dengue; this population was included in the ultrasound-based analysis (Figure 1).
3.1. General Characteristics
A total of 132 children between 6 months and 14 years old (7.8 ± 3.6 years old, 54.6% schoolchildren) were included, 52.3% of whom were male and 93.9% of whom were from southwestern Colombia. Most had secondary infection, were eutrophic according to the Body Mass Index, and more than half had abdominal pain and vomiting. About one-third of the children had an extended hospital stay lasting more than 5 days, and one-quarter required management in the ICU. More than half of the children had hypoalbuminemia, thrombocytopenia, leukopenia, and grade C aminotransferase levels according to the de Souza classification [29]; 0.8% had prolonged coagulation times, and 6.1% had leukocytosis. Therapeutic management included intravenous albumin and blood products, among other treatments (Table 1).
3.2. Imaging
The main finding on chest X-rays was pleural effusion (65.7%). The time elapsed between symptom onset and ultrasound was 6.0 ± 2.1 days, which was considered late (more than 5 days) in 40.1% of cases. In 126 children (95.5%), capillary leakage was evident on ultrasound, involving ascites (83.3%), pleural effusion (46.2%), hepatomegaly (40.9%), a thickened gallbladder (39.4%), and pericardial effusion (3.0%) (Table 2).
3.3. Possible Risk Factors
The schoolchildren and adolescent age groups were possibly at higher risk for developing capillary leakage (OR = 13.52, 95% CI = 1.41–646.51, p = 0.0031); other risk factors included elevated ALT (OR = 11.06, 95% CI = 1.32–94.82, p = 0.0007) and aminotransferase levels grades C + D according to the de Souza classification (OR = 6.87, 95% CI = 0.82–54.59, p = 0.0110) (Table 3).
Some associations showed a wide 95% CI, reflecting statistical imprecision due to the small number of patients without ultrasound evidence of capillary leakage. Therefore, these estimates should be interpreted with caution, focusing on the direction of the association rather than the OR magnitude.
3.4. Mortality
Three children died (0.9% of the initially confirmed cohort of 321 patients), and due to the severity of their condition, they did not undergo ultrasound examinations. Therefore, they were not included in the final ultrasound-based analysis (N = 132). These cases are described separately to provide contextual evidence highlighting the clinical relevance of the identified risk factors. In all cases, two or more characteristics considered risk factors for capillary leakage were identified according to the criteria established in this study: one patient was a schoolchild, three had elevated ALT, and all three had aminotransferase levels of grades C – D according to the de Souza classification [29] (Table 4).
Although ultrasound findings were not available, the clinical and laboratory characteristic analysis showed that all three patients presented abdominal pain, liver involvement evidenced by elevated AST, hypoalbuminemia, and thrombocytopenia. Two of them had secondary infection, grade D aminotransferase levels according to the de Souza classification [29], severe thrombocytopenia, pleural effusion confirmed by chest X-rays, and required intravenous albumin administration, while the third had grade C aminotransferase levels according to the de Souza classification [29] and mild thrombocytopenia (Table 5).
4. Discussion
4.1. Prevalence of Capillary Leakage Ultrasound Findings
Our study identified a high prevalence of ultrasound signs of capillary leakage, especially pleural effusion, ascites, and thickening of the vesicular wall, findings that are consistent with the international literature on pediatric populations [15,17,18,19,20,21]. Rather than reflecting only disease severity, this high prevalence underscores the ability of ultrasound to detect subclinical plasma leakage that may not yet be apparent on a physical examination, supporting its role as an early diagnostic tool in pediatric dengue.
In the HUV cohort, more than 90.0% of patients with dengue presented at least one sign of plasma extravasation, which supports the role of ultrasound as a sensitive tool to detect complications in dengue early on. These results are in line with those reported by Foucambert et al. [1], who found signs of capillary leakage in 80.0% of children with severe dengue and demonstrated that vesicular wall thickening > 3 mm is associated with greater severity. In our population, the presence of vesicular thickening in patients with dengue and other warning signs suggests that this finding may represent an early marker of endothelial dysfunction, preceding overt clinical deterioration, reinforcing the value of ultrasound beyond its use in advanced disease stages.
4.2. Implementation of Ultrasound Protocols and Serial Assessment
In our cohort, the high frequency of ultrasound-detected capillary leakage, even among children with dengue and other warning signs, supports the AEDES approach of systematic and sequential ultrasound assessment [30], which proposes repeated evaluations to monitor hemodynamic progression. These findings suggest that the early identification of subtle imaging changes, such as mild ascites, minimal pleural effusion, or vesicular wall thickening, may precede clinical deterioration and allow for timely risk stratification, closer monitoring, and optimizing fluid management. Therefore, our results provide clinical evidence that reinforces the applicability of the AEDES protocol in pediatric populations, particularly in referral centers and endemic settings where recognizing severe dengue early on is critical.
Similarly, the meta-analysis conducted by Kaagaard et al. [17] reported an overall prevalence of pleural effusion of 33.0% (95% CI: 29.0–37.0%), higher in children (43.0%) and in severe cases of dengue (48.0%). The higher frequency observed in our cohort (46.2%) likely reflects the referral nature of our institution, which concentrates moderate and severe cases from southwestern Colombia, highlighting how the healthcare setting and evaluation timing may influence ultrasound detection rates.
Parmar [31] previously warned that ultrasound should not be considered an isolated screening method, as its sensitivity depends on the clinical phase of the disease and the operator. This observation is particularly relevant for dengue, where vascular permeability fluctuates dynamically, thus reinforcing the need to interpret ultrasound findings in conjunction with clinical and laboratory parameters rather than as standalone indicators. In our study, ultrasound examinations were performed by trained radiologists using an institutional protocol; however, variability in the timing of image acquisition in relation to the clinical phase of dengue may have influenced the detection of subtle or early manifestations of capillary leakage.
4.3. Factors Associated with Capillary Leakage
From a pathophysiological point of view, Qiu et al. [16] demonstrated in murine models that heterologous secondary infections increase capillary permeability through antibody-mediated immunopathological mechanisms. Consistent with this, 76.5% of our population had secondary infection, and this group showed a higher frequency of liver and ultrasound abnormalities, supporting the hypothesis that abnormal immune response plays a decisive role in capillary leakage.
The Colombian study conducted by Osorio et al. [19] found that point-of-care ultrasound (POCUS) detected capillary leakage in 85.1% of patients and was associated with thrombocytopenia and an increased risk of hospitalization, findings that are consistent with our results. Our findings extend this observation by demonstrating laboratory markers with hepatic involvement and hypoalbuminemia parallel imaging evidence of plasma leakage, reinforcing the concept that capillary leakage represents a multisystem process rather than an isolated imaging phenomenon, as previously suggested by Sivasubramanian et al. [14] in adults.
Although nutritional alterations were common, no statistically significant association with capillary leakage was identified. This finding may be related to incomplete anthropometric data and limited sample size rather than the absence of a true biological relationship, especially given emerging evidence suggesting that both malnutrition and obesity may modulate immune and inflammatory responses in dengue [12]. Even so, almost half of the children had some degree of anthropometric abnormality, suggesting that extreme nutritional conditions, such as malnutrition or obesity, could influence the immunometabolic response to the virus and, potentially, the risk of developing capillary leakage.
4.4. Clinical Implications, Prognostic Value, and Mortality
Thanh Vo [32] showed that the use of POCUS to guide resuscitation in children with dengue shock reduced mortality from 64.0% to 15.0%. Although our study was retrospective and did not evaluate ultrasound-guided interventions, the strong association between ultrasound findings and recognized risk factors suggests that the early identification of capillary leakage could meaningfully influence clinical decision-making, particularly regarding fluid management and monitoring intensity.
At the national level, the systematic review conducted by Rodríguez-Morales et al. [5] confirms Colombia’s hyperendemic pattern with a predominance of the DENV-2 serotype, which is disproportionately affecting children and adolescents, especially in Valle del Cauca. Our local data fit this epidemiological pattern: almost all cases were in children and adolescents, a group identified as being at higher risk for severe dengue.
Although mortality in our cohort was low, the fact that all fatal cases shared multiple laboratory and clinical risk factors for capillary leakage reinforces the prognostic relevance of these variables, even in the absence of ultrasound data. These findings are consistent with those reported in previous studies, where the combination of liver involvement, hematological abnormalities, and plasma extravasation has been associated with an increased risk of fatal outcomes in pediatric dengue [1,14]. The absence of imaging in these rapidly evolving cases highlights the importance of early bedside assessment and supports the growing role of POCUS in acute pediatric care [19,32]. This aspect is particularly relevant in endemic regions such as Colombia, where the burden of disease and pediatric hospitalization remain high [5]. Collectively, this evidence supports the need to implement structured ultrasound evaluation protocols in emergency departments and hospitals, especially during epidemic outbreaks.
Overall, our findings align with the growing body of evidence indicating that ultrasound, particularly when integrated with clinical and paraclinical data, offers relevant prognostic value in pediatric dengue within hospitalized and clinically selected populations. However, the high frequency of ultrasound-detected capillary leakage observed in this cohort should be interpreted considering a potential selection bias, as ultrasound examinations were preferentially performed in children with warning signs or severe disease. Consequently, variations across studies likely reflect not only differences in epidemiological context, evaluation timing, and healthcare system complexity but also differences in patient selection rather than inconsistencies in ultrasound performance itself.
In addition, note that the outcome “capillary leakage” was defined as a composite variable, based on the presence of any ultrasound finding compatible with plasma extravasation. In this clinically selected cohort, this resulted in a very high prevalence of the outcome, which limited variability and reduced the discriminative capacity of bivariate analyses. Consequently, the observed associations should be interpreted primarily in terms of their direction rather than their magnitude. Future studies may benefit from evaluating predictors of specific ultrasound findings, such as ascites, or from stratifying capillary leakage according to the number of affected compartments to better capture gradients of severity and improve clinical applicability.
Finally, comparative evidence highlights that implementing standardized ultrasound protocols, such as AEDES, and training clinical staff can improve the reproducibility and impact of this tool in pediatric practice. Our results support the need to incorporate systematic ultrasound into the evaluation of pediatric patients with dengue, especially in endemic regions such as southwestern Colombia, where the burden of disease and infant mortality remains high.
4.5. Limitations
This study has several limitations. First, the high prevalence of ultrasound-detected capillary leakage likely reflects a selection bias, as ultrasound examinations were preferentially performed in hospitalized children with warning signs or severe dengue, and a substantial number of patients were excluded due to the absence of ultrasound data. Therefore, the prevalence reported should not be extrapolated to unselected pediatric dengue populations or to patients with mild disease. Its retrospective design limited the availability of some variables that were not consistently recorded in the medical records during patient care, which may have resulted in missing data for certain analyses. In addition, the single-center nature of the study may limit the generalizability of the findings to other settings or populations with different epidemiological or healthcare characteristics. Furthermore, some variables showed a wide 95% CI, likely reflecting the limited sample size, suggesting that future studies with larger populations, preferably multicenter in design, are needed to improve the precision of the estimates. Finally, none of the patients who died underwent ultrasound evaluation due to rapid clinical deterioration, highlighting the potential value of bedside ultrasound (POCUS) and supporting the need to incorporate structured ultrasound training into pediatric residency and specialization curricula.
5. Conclusions
In this selected pediatric cohort of hospitalized children with dengue and warning signs or severe disease, ultrasound was used to detect a high frequency of capillary leakage, which was associated with clinical and laboratory markers of severity. These findings support the clinical utility of ultrasound as an adjunct tool for early identification and risk stratification in pediatric dengue while acknowledging that prevalence estimates cannot be extrapolated to unselected populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Foucambert P. Esbrand F.D. Zafar S. Panthangi V. Cyril A.R. Raju A. Luthra G. Shahbaz M. Almatooq H. Khan S. Efficacy of Dengue Vaccines in the Prevention of Severe Dengue in Children: A Systematic Review Cureus 202214 e 2891610.7759/cureus.2891636225478 PMC 9542041 · doi ↗ · pubmed ↗
- 2Wilder-Smith A. Eng-Eong O. Horstick O. Wills B. Dengue Lancet 201939335036310.1016/S 0140-6736(18)32560-130696575 · doi ↗ · pubmed ↗
- 3Moras E. Achappa B. Murlimanju B.V. Naveen G.M. Holla R. Madi D. D’Souza N.V. Mahalingam S. Early diagnostic markers in predicting the severity of dengue disease Biotech 20221226810.1007/s 13205-022-03334-9PMC 946138836091089 · doi ↗ · pubmed ↗
- 4Rabaan A.A. Alshengeti A. Alrasheed H.A. Al-Subaie M.F. Aljohani M.H. Almutawif Y.A. Yousuf A.A. Alsuliman S.A. Al-Jishi J.M. Almalki F. Dengue virus infection in Saudi Arabia from 2003 to 2023: A systematic review and meta-analysis Pathog. Glob. Health 202411854955810.1080/20477724.2024.242549339508063 PMC 11892044 · doi ↗ · pubmed ↗
- 5Rodríguez-Morales A.J. López-Medina E. Arboleda I. Cardona-Ospina J.A. Castellanos J.E. Faccini-Martínez A.A. Gallagher E. Hanley R. Lopez P. Mattar S. The Epidemiological Impact of Dengue in Colombia: A Systematic Review J. Trop. Med. Hyg.202511218218810.4269/ajtmh.23-0907 PMC 1172075639471503 · doi ↗ · pubmed ↗
- 6Hause A.M. Perez-Padilla J. Horiuchi K. Han G.S. Hunsperger E. Aiwazian J. Margolis H.S. Tomashek K.M. Epidemiology of Dengue Among Children Aged < 18 Months—Puerto Rico, 1999–2011 Am. J. Trop. Med. Hyg.2016944044082671151910.4269/ajtmh.15-0382 PMC 4751950 · doi ↗ · pubmed ↗
- 7Mishra S. Ramanathan R. Kumar S. Clinical Profile of Dengue Fever in Children: A Study from Southern Odisha, India Scientifica 20162016639159410.1155/2016/639159427213083 PMC 4860230 · doi ↗ · pubmed ↗
- 8L’Azou M. Moureau A. Sarti E. Nealon J. Zambrano B. Wartel T.A. Villar L. Capeding M.R. Ochiai R.L. Symptomatic Dengue in Children in 10 Asian and Latin American Countries N. Engl. J. Med.20163741155116610.1056/NEJ Moa 150387727007959 · doi ↗ · pubmed ↗