Thermography and Infrared Spectroscopy in the Detection of Periodontal Inflammation In Vivo: A Systematic Review
Heythem Nassim Guetatlia, Mickael Gette, Laurent Estrade, Victor Rimbaud, Frédéric Denis, Gaël Y. Rochefort, Matthieu Renaud

TL;DR
This systematic review explores the use of thermography and infrared spectroscopy as non-invasive tools for detecting periodontal inflammation, offering an alternative to traditional methods.
Contribution
The paper systematically evaluates the potential of thermography and infrared spectroscopy for in vivo periodontal inflammation detection.
Findings
Thermography and infrared spectroscopy show feasibility in detecting periodontal inflammation in vivo.
These techniques offer non-invasive and radiation-free alternatives to traditional diagnostic methods.
Further research is needed to standardize methodologies and validate clinical applicability.
Abstract
Background/Objectives: Periodontal inflammation is a key feature of periodontal diseases, but traditional diagnostic methods are limited by invasiveness and radiation exposure. This systematic review aims to evaluate the potential of thermography and infrared spectroscopy for the in vivo detection of periodontal inflammation and to assess their reliability for clinical use. Methods: In accordance with PRISMA guidelines, an electronic search of the MEDLINE (PubMed) database was conducted to identify relevant studies published between 2000 and October 2025 that investigated these imaging modalities in periodontal inflammation diagnosis. Results: The search identified 310 records; after exclusions, 13 studies were included, comprising 7 thermography studies and 6 infrared spectroscopy studies, for a total of 712 patients. The included studies demonstrated the feasibility of thermography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
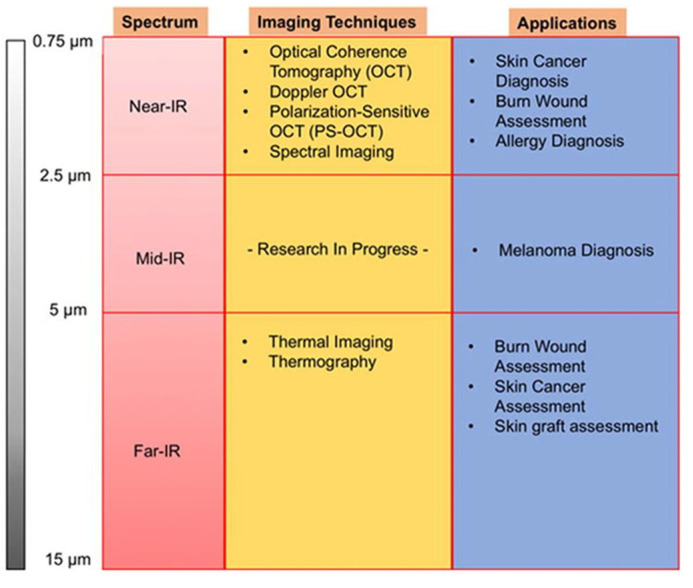 Figure 1
Figure 1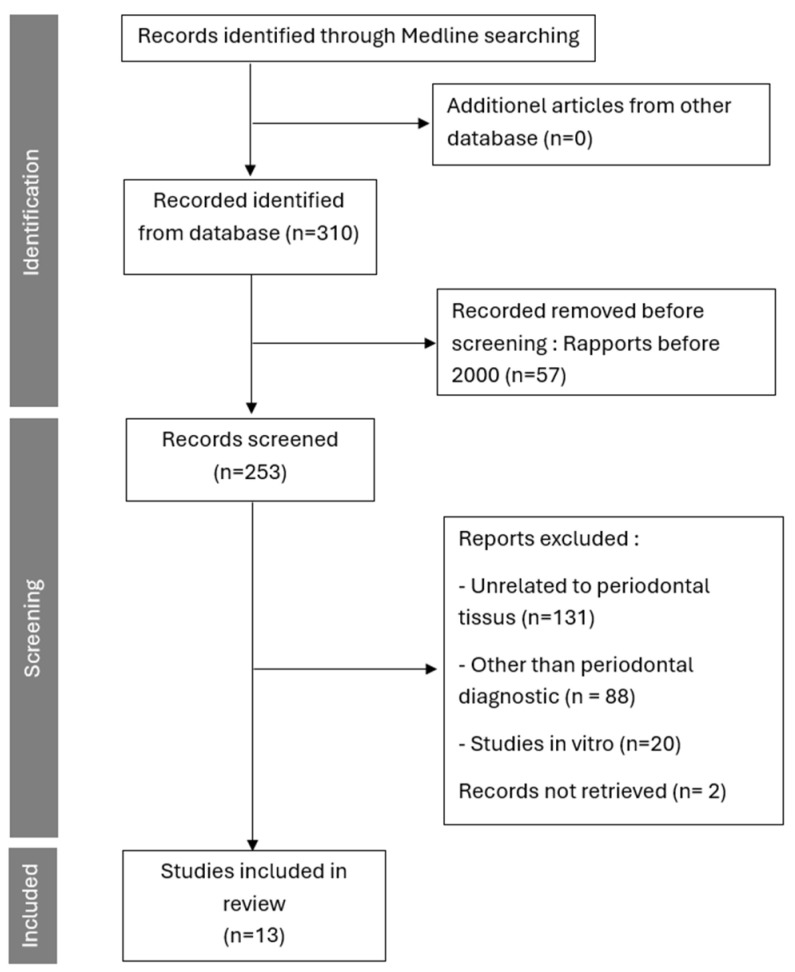 Figure 2
Figure 2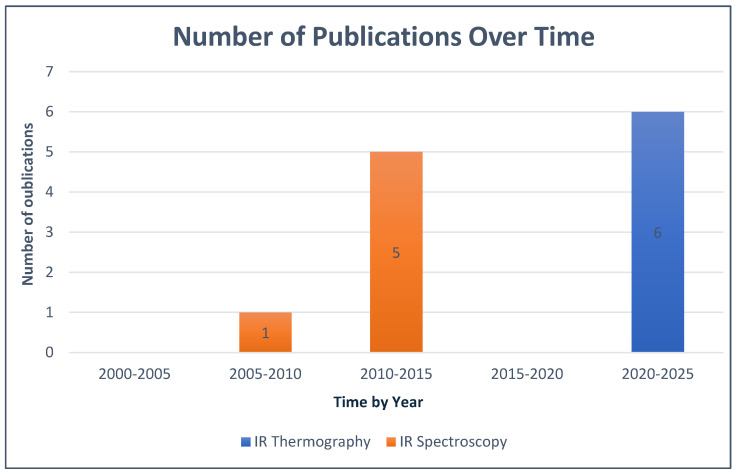 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfrared Thermography in Medicine · Oral microbiology and periodontitis research · Laser Applications in Dentistry and Medicine
1. Introduction
Periodontal disease is characterized by persistent inflammatory damage to the periodontal tissues [1,2]. Periodontal inflammation refers to the host’s immune response to microbial plaque, manifesting as redness, swelling, and bleeding of the gingival tissues, which can progress to tissue destruction in periodontitis. It is a key diagnostic criterion for periodontal diseases, including gingivitis (reversible inflammation confined to the gingiva) and periodontitis (irreversible loss of attachment and bone). It manifests as inflammation leading to the degradation and progressive destruction of the tooth-supporting structures, including gingiva, periodontal ligament, cementum, and alveolar bone [3]. Numerous studies also link it to the exacerbation of systemic conditions, such as cardiovascular diseases and diabetes [4,5,6]. The inflammatory process in periodontal disease is complex, involving a dysbiotic microbiome triggering a hyperinflammatory response, leading to tissue breakdown in periodontitis, unlike gingivitis, which is characterized by pathognomonic signs such as reversible gingival erythema, edema, and bleeding without attachment loss.
Diagnosis depends traditionally on clinical parameters, including periodontal pocket depth, bleeding on probing, and attachment loss [7]. These are supplemented by radiological assessments, which detect macroscopic signs of the pathology, such as alveolar bone resorption and loss of periodontal attachment [8,9]. However, early detection remains challenging due to the limitations of these methods. Limitations include the subjectivity and invasiveness of probing (causing patient discomfort and potential tissue trauma), delayed detection via radiography (only showing bone loss after 30–50% destruction), and radiation exposure. Emerging technologies like thermography and spectroscopy could improve early detection by non-invasively capturing subclinical inflammation through heat and hemodynamic changes.
The diagnostic methods for periodontal diseases in dental medicine have stagnated for years, prompting the exploration of alternative imaging modalities less ionizing and capable of providing an earlier diagnosis of periodontal inflammation, while ensuring their effectiveness in the daily practice of clinicians. Common tools include periodontal probes for pocket depth, bleeding on probing, and ionizing radiographs (e.g., periapical X-rays, CBCT) for bone assessment. Infrared technologies are considered due to their non-ionizing nature, reducing risks like cumulative radiation exposure, while providing real-time, contactless inflammation detection [10,11,12].
Infrared radiation was discovered by William Herschel (1738–1822) through experiments on “dark light,” extending Newton’s work on light diffraction. Herschel observed increasing temperatures beyond the visible red spectrum, revealing infrared radiation [13]. Unlike visible light, infrared wavelengths (0.7–1000 μm) are imperceptible to the human eye but ideal for analyzing tissue structure and dynamics. The infrared spectrum is divided into near-infrared (NIR; 0.75–2.5 μm), mid-infrared (MIR; 2.5–5 μm), and far-infrared (FIR; 5–15 μm) [14], each suited to specific imaging techniques (Figure 1). These technologies enable early visualization by detecting parameters like temperature gradients (in thermography, e.g., ΔT > 0.5 °C for inflammation) and tissue oxygenation levels (in spectroscopy, e.g., reduced oxyhemoglobin in inflamed sites), distinguishing from non-inflammatory processes like cancer, which may show different spectral signatures.
The two main analysis techniques for this spectrum of electromagnetic waves are thermography and spectroscopy:
Since the mid-1960s, multiple publications have introduced the use of infrared thermography as a potential non-ionizing tool for the detection of inflammation [15,16,17]. Far-infrared imaging, also known as infrared thermal imaging (IRT) or thermography, is a non-invasive, contactless imaging technique that provides real-time temperature measurements of the structures being analyzed by detecting their emitted far-infrared radiation (5–15 μm). This emitted thermal radiation is then converted into a visible and quantifiable infrared thermal image [18]. The measurement in this technique relies on detectors such as bolometers. These sensors receive the infrared emissions from objects, caused by the rise in their temperature. This thermal variation modifies the conductance of the sensor material, resulting in a change in the electrical signal measured at the output [14]. IRT has been rarely used in biomedical applications due to the limitations of early IR cameras in terms of performance and size. First-generation cameras provided insufficient thermal and spatial resolution, making the results unsatisfactory for many medical applications. Today, modern appliances with high sensitivity are used to produce high-resolution thermal images. As just seen, thermographic devices convert captured infrared radiation into electrical signals, which are then transformed into a thermogram visually representing temperature variations using a colormap [19]. The colors displayed on the generated images represent temperature gradients, ranging from the warmest shades, such as red, to the coolest ones, such as green and blue [18]. Some reviews have already discussed thermography in other fields, but studies dedicated to periodontology applications of this technique remain relatively rare. Up until now, no review has been conducted to highlight the use of these technologies in the diagnosis of periodontal inflammation.
Moreover, spectroscopy refers to the interaction between electromagnetic waves and analyses based on their wavelength. These interactions can be measured using various spectroscopic techniques that cover different wavelength ranges [20]. In the infrared region, spectroscopy can be used to analyze the spectra of near-infrared (NIR), mid-infrared (MIR), and far-infrared (FIR) [20,21,22,23]. Light penetration in imaging is strongly influenced by its interaction with chromophores, particularly hemoglobin and water. In the near-infrared (NIR) range (0.75–2.5 μm), water absorption remains low, allowing light to reach greater depths [14], making this spectral range a preferred alternative for this technique. Although many studies have demonstrated its effectiveness in other medical fields, the recent literature does not provide a comprehensive review of the current state of research and the prospects of IR spectroscopy in the diagnosis of periodontal inflammation, especially for its in vivo use.
Therefore, the aim of this systematic review was to explore the potential use of thermography and infrared spectroscopy in periodontology, with a particular focus on their in vivo application in the diagnosis of gingival inflammation.
2. Materials and Methods
This review was conducted following the principles established by the PRISMA guidelines [24]. The PRISMA 2020 checklist is provided in supplementary material. Despite promising applications in other fields, a knowledge gap exists in periodontology regarding their diagnostic performance (e.g., sensitivity/specificity), methodological standardization, and clinical readiness for routine in vivo use.
2.1. Search Strategy
The search covered publications available in the MEDLINE (PubMed) database over the past 25 years, aiming to identify studies published between 2000 and October 2025, analyzing the contribution of thermography and infrared spectroscopy in the diagnosis of periodontal inflammation. The following search terms and keywords were used, either alone or combined using the Boolean operators “AND”/“OR,” according to the following equation:
((infrared Spectroscopy) OR (near-infrared Spectroscopy)) AND ((Diagnosis) OR (Examination)) AND ((Periodontal inflammation) OR (periodontitis)) OR ((Thermography infrared) OR (Far-Infrared)) AND ((Diagnosis) OR (Examination)) AND ((periodontitis) OR (inflammation) OR (Periodontal inflammation)).
2.2. Study Detection
References of the eligible studies on the topic were manually checked, and two independent operators (N.G. and M.R.) screened the studies according to the inclusion/exclusion criteria. In case of disagreement, a 3rd reviewer (G.R.) was asked. No formal risk-of-bias tool was used due to study heterogeneity (e.g., varying designs, small samples); potential biases include selection (convenience sampling) and measurement (non-standardized protocols), addressed qualitatively. Quantitative synthesis/meta-analysis was not performed due to heterogeneity in designs, protocols, and outcomes (e.g., different temperature thresholds, spectral ranges).
Inclusion and Exclusion Criteria
The articles included in this review pertain to clinical studies conducted on human subjects with inflammation of the periodontal tissues. These studies focus on the diagnosis of inflammation in one or more periodontal tissues using real-time thermography or infrared spectroscopy, performed directly in a clinical setting on patients. Studies comparing inflamed to normal tissues were prioritized, with normal parameters defined as baseline temperature (e.g., 32–35 °C) or oxygenation levels (>60% oxyhemoglobin) from healthy controls.
The references of eligible studies on the topic were screened by abstract and full text, and studies were selected based on the inclusion/exclusion criteria.
Only studies concerning the use of the infrared subrange for periodontal inflammation detection were analyzed and included in this review, except for studies conducted on healthy periodontal tissues. These studies, which compare clinical and technical results in the evaluation of inflammation parameters, such as probing depth, were excluded in order to examine how infrared imaging can estimate these parameters and assess its potential for detecting inflammation.
Articles were excluded either directly from the title if they met an exclusion criterion, such as animal studies, or after reviewing the abstract or full text for the remaining articles.
The exclusion criteria were studies involving non-human subjects, those using techniques other than thermography or infrared spectroscopy, as well as articles addressing objectives unrelated to diagnosis (e.g., monitoring healing, evaluating therapy effects, or post-therapeutic outcomes), or diagnoses not related to periodontal tissues were excluded. Additionally, studies conducted outside the in vivo setting (ex vivo or in vitro) were also excluded.
Each study meeting the inclusion criteria was analyzed according to several parameters, including the study design, number of patients, age range, publication date, description of the camera or device used, as well as the objectives and findings.
3. Results
3.1. Study Selection
The search identified 310 published articles, 253 were published since the 1 January 2000. After applying the inclusion and exclusion criteria, 13 articles were included in this review (Figure 2). Among these articles, 7 focused on thermography, and 6 on spectroscopy as techniques for detecting periodontal inflammation, with a total of 712 patients.
3.1.1. Presentation of IR Thermography Studies
Regarding thermography, among the 7 studies included in the analysis (Table 1), we were able to identify three common themes: room temperature, camera distance, and the spectrum used by the camera. Studies included in the analysis were clinical trials using thermography technique in comparison with standard clinical examination. Thermography studies consistently showed temperature increases of 0.5–2 °C in inflamed sites compared to controls, with methodological variability in camera distances (20–50 cm) and room temperatures (20–25 °C).
Regarding spectroscopy, among the 6 studies included in the analysis (Table 2), two common themes were highlighted: the biophysical properties used, and the spectrum range of the camera. The studies included in the analysis were clinical trials based on spectroscopy technique and compared to standard clinical examination. Spectroscopy studies demonstrated reduced tissue oxygenation (e.g., 10–20% lower in inflamed vs. normal sites) and elevated total hemoglobin, with consistencies in NIR range use but discrepancies in patient subgroups (e.g., higher variability in diabetics). Across thermography and spectroscopy, similarities include non-invasive detection of vascular changes, but discrepancies involve measurement depth and quantitative vs. qualitative outputs.
3.1.2. Evolution of the Studies
The application of IR spectroscopy and thermography for in vivo periodontal inflammation visualization was not widely practiced, and publications on this topic were limited. According to the publication periods used in this review, studies focusing on IR spectroscopy in this context only began in 2009, with no publications since 2015, while those on IR thermography in the same context only started later, in 2021. These data are presented below in Figure 3.
3.1.3. Presentation of Cameras Used for IR Thermography
This section provides a brief overview of the most important aspects of infrared cameras used for periodontal inflammation detection through thermography.
The literature presents various camera models and their characteristics (thermal resolution, infrared sensor, acquisition frequency) collected directly from articles data or camera’s technical specifications available on the manufacturer’s website [38] (The data collected outside of the scientific articles from the PubMed database are indicated with an asterisk* in the table.) It is worth noting that all the articles included in the review mentioned the type of camera used.
The collected characteristics, along with the image analysis software, are presented in Table 3 below. The image analysis and processing software are listed for reference, with various software packages being used, including ThermaCam and Researcher Pro, which were employed twice in two different studies by the same team with two different versions.
3.1.4. Overview of Devices Used for IR Spectroscopy
All spectroscopy studies utilized a miniaturized NIR device (e.g., Inspectra Spectrometer) with fiber-optic probes, measuring hemoglobin indices at 700–1000 nm, analyzed via custom software. All the studies included on infrared spectroscopy technology used the same diagnostic device because they were conducted by the same research team members, with the aim of validating the device on different subjects. The device and associated equipment used for performing the diagnosis and analyzing the results are presented in detail in Table 4 below.
4. Discussion
The host’s immune and inflammatory responses play a key role in the pathogenesis of periodontal disease. To formulate hypotheses and assess the feasibility of new periodontal diagnostic techniques, it is essential to first identify the clinical signs upon which we can rely to detect them in accordance with the technology used. In this review, two key signs were considered both reliable and potentially useful for improving periodontal diagnosis: edema and tissue temperature increase [39].
The heat emitted by tissues is a specific property detectable by infrared thermography [40]. In the context of periodontal inflammation, the increase in vascular dilation and permeability of the gingival tissues causes a higher heat production compared to normal state, which allows inflammation to be characterized using this technical criterion.
The included articles show that thermography can serve as an innovative diagnostic alternative or complement due to its non-invasive nature, particularly when radiological examination is contraindicated [25] such as in pregnant women during their first trimester. However, thermography has several limitations, such as limited tissue penetration [29], making it difficult to detect inflammation in the deeper tissues.
On a different note, IR spectroscopy primarily relies on edema to detect inflammation. Edema is a macroscopic sign resulting from the worsening of several microscopic processes related to hemodynamic changes during periodontal inflammation [37]. Among these changes, vascular dilation and increased permeability, as previously mentioned, are some of the most characteristic markers of gingival inflammation [35]. When infrared light passes through tissues, it selectively interacts with chromophores associated with oxygen, allowing for the real-time measurement of various tissue parameters like hemoglobin (oxygen carrier). This method offers a direct link to the oxygenation status and tissue perfusion. Most studies confirm that decreased tissue oxygenation is associated with an inflammatory state of the tissues, with a notable difference between periodontitis and gingivitis depending on the degree of inflammation. The more the inflammation progresses, the more tissue oxygenation decreases. In parallel, the tHB (total hemoglobin) index, which reflects regional blood volume, serves as an indicator of tissue perfusion status. Its elevation in periodontal areas, reflects altered vascularization, a characteristic of periodontal inflammation [32,33,34] as found in gingivitis or periodontitis.
Research teams have developed a miniaturized spectroscopy device suitable for periodontal use, based on near-infrared spectrum, the preferred choice for this technology [14]. This device has been validated by included studies investigating its applications on various subjects with different systemic conditions, such as diabetes, heart disease [32,33], or varying habits like smokers [34]. Overall, regarding infrared spectroscopy, the literature remains limited in its exploration beyond the use of a single device. This gap highlights the need for further research to expand its applications and compare them with other existing technologies for periodontal diagnosis. Compared to probing (invasive, subjective) and radiography (ionizing, late-stage detection), thermography offers real-time, non-contact heat mapping with high sensitivity for superficial inflammation, though limited penetration; spectroscopy provides quantitative hemodynamic data, superior for deeper assessment but requires device miniaturization. Advantages include safety and early detection, but challenges like cost and standardization persist. Thermography and spectroscopy share non-invasive feasibility but differ in depth (superficial vs. deeper); while technically viable, clinical applicability remains exploratory without validated thresholds, emphasizing need for larger trials over immediate use.
Because we focused on in vivo detection approach, the studies included in this review concentrate on periodontal inflammation tissue signs. However, this does not exclude the relevance for in vitro techniques, such as spectroscopy on saliva samples [41,42] or crevicular fluid [43,44], which remain potentially useful for early periodontal diagnosis.
In the same context, periodontal inflammation detection has been shown to be possible using near-infrared spectrum (near-infrared) through spectroscopy. However, there are other potential ways to exploit this light spectrum through similar innovative techniques, such as near-infrared Imaging (NIRI) technology, which is making its way into the oral healthcare field with the latest generation intraoral scanners [45,46]. Further studies are therefore needed to explore these new technologies through techniques already integrated into devices used in dental clinics.
Finally, to improve our review, it would be relevant to explore sources from other scientific disciplines, particularly databases used by biomedical imaging technicians and engineers, in order to obtain more detailed technical information on the technologies employed.
This review reveals the current literature on periodontal inflammation detection through the near and far IR spectrum. However, studies have shown the usefulness of other spectra on different tissues, such as skin tissue [14], Due to the histological similarity between mucosal and skin tissues, it is estimated that other spectra (mid-IR) and other techniques (Raman Spectroscopy) could be useful and exploitable for the detection of periodontal inflammation [43,47].
The use of medical imaging techniques in dental medicine is, to date, an underexplored field, which is why it represents an interesting research area.
5. Perspectives
The infrared spectrum, through these two approaches, shows promising potential that could contribute to improving the early diagnosis of periodontal diseases soon. However, further research is needed to identify the best practices for using this spectrum in this context.
With recent technological advancements in thermal cameras, infrared thermography is now a promising method for the detection of periodontal inflammation [30]. However, given these limitations, it is important to note that the clinical use of this technique still requires further in-depth studies to validate its effectiveness and improve its specific utility as an independent diagnostic tool.
Recent advancements, such as the integration of artificial intelligence with thermography, have shown enhanced accuracy in classifying gingival inflammation, particularly in specific populations like mouth breathers. This highlights the potential for AI to address limitations in manual analysis and improve diagnostic precision [31].
On the other hand, infrared spectroscopy, which has been used for years in the medical field, is making its way into periodontology through innovative devices designed by research teams [35,37]. This offers better prospects for reducing the size of spectrographs and facilitating their use by periodontists. This review highlights a promising start and the potential for exploiting this technique in the diagnosis of periodontal diseases, but there is still a long way to go before thermography becomes widely used in dental clinics.
Although no study has addressed this topic so far, a clinical study combining both techniques in a single device for periodontal diagnosis could be useful to maximize the effectiveness of these two techniques and achieve better diagnostic performance. This approach would allow one technique to offset the limitations of the other and/or simultaneously collect data from both techniques in order to achieve the best possible result through an expanded analysis of this data, facilitated by the introduction of artificial intelligence.
6. Conclusions
Numerous publications have demonstrated the potential of thermography and infrared spectroscopy (IR) for the in vivo detection of periodontal inflammation. These findings open new perspectives regarding the integration of these technologies into clinical periodontal practice in the near future. These non-invasive methods could allow a more precise and rapid assessment of the inflammatory status of periodontal tissues, providing a complementary tool to current diagnostic techniques. Although preliminary results are promising, this field remains largely underexplored, and several challenges must be addressed before widespread adoption. Further studies are needed to confirm the effectiveness, reliability, and reproducibility of these technologies in the daily practice of periodontists, considering the pathophysiological variables specific to each patient and the lack of standardized thresholds or validated metrics like sensitivity/specificity. These studies will help to determine the optimal conditions for their use and assess their impact on the early diagnosis of periodontal diseases in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chapple I.L.C. Mealey B.L. Van Dyke T.E. Bartold P.M. Dommisch H. Eickholz P. Geisinger M.L. Genco R.J. Glogauer M. Goldstein M. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions J. Clin. Periodontol.201845 S 68S 772992649910.1111/jcpe.12940 · doi ↗ · pubmed ↗
- 2Papapanou P.N. Sanz M. Buduneli N. Dietrich T. Feres M. Fine D.H. Flemmig T.F. Garcia R. Giannobile W.V. Graziani F. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions J. Clin. Periodontol.201845 S 162S 170Available online: https://onlinelibrary.wiley.com/doi/10.1111/jcpe.12946(accessed on 5 January 2026)2992649010.1111/jcpe.12946 · doi ↗ · pubmed ↗
- 3Herrera D. Sanz M. Shapira L. Brotons C. Chapple I. Frese T. Graziani F. Hobbs F.D.R. Huck O. Hummers E. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: Consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe)J. Clin. Periodontol.2023508198413693520010.1111/jcpe.13807 · doi ↗ · pubmed ↗
- 4Bui F.Q. Almeida-da-Silva C.L.C. Huynh B. Trinh A. Liu J. Woodward J. Asadi H. Ojcius D.M. Association between periodontal pathogens and systemic disease Biomed. J.201942273510.1016/j.bj.2018.12.00130987702 PMC 6468093 · doi ↗ · pubmed ↗
- 5Preshaw P.M. Alba A.L. Herrera D. Jepsen S. Konstantinidis A. Makrilakis K. Taylor R. Periodontitis and diabetes: A two-way relationship Diabetologia 20125521312205719410.1007/s 00125-011-2342-y PMC 3228943 · doi ↗ · pubmed ↗
- 6Sanz M. Marco Del Castillo A. Jepsen S. Gonzalez-Juanatey J.R. D’Aiuto F. Bouchard P. Chapple I. Dietrich T. Gotsman I. Graziani F. Periodontitis and cardiovascular diseases: Consensus report J. Clin. Periodontol.20204726828810.1111/jcpe.1318932011025 PMC 7027895 · doi ↗ · pubmed ↗
- 7Caton J.G. Armitage G. Berglundh T. Chapple I.L.C. Jepsen S. Kornman K.S. Mealey B.L. Papapanou P.N. Sanz M. Tonetti M.S. A New Classification Scheme for Periodontal and Peri-Implant Diseases and Conditions—Introduction and Key Changes from the 1999 Classification J. Clin. Periodontol.201845 S 1S 8Available online: https://onlinelibrary.wiley.com/doi/10.1111/jcpe.12935(accessed on 5 January 2026)2992648910.1111/jcpe.12935 · doi ↗ · pubmed ↗
- 8Chen I.D.S. Yang C.M. Chen M.J. Chen M.C. Weng R.M. Yeh C.H. Deep Learning-Based Recognition of Periodontitis and Dental Caries in Dental X-ray Images Bioengineering 2023109113762779610.3390/bioengineering 10080911 PMC 10451544 · doi ↗ · pubmed ↗