Discrepancies in the Detection of PML::RARA Gene Rearrangement by Fluorescent In Situ Hybridization Using Commonly Used Dual Color Dual Fusion Probes
Hanan S. Elsarraj, Karsten Evans, Sydney Graham, Shivani Golem

TL;DR
This paper shows that standard FISH tests can miss certain gene rearrangements in a type of leukemia, requiring better diagnostic methods.
Contribution
The study identifies limitations in current FISH probes for detecting PML::RARA rearrangements and advocates for alternative probes and molecular testing.
Findings
Two APL cases showed atypical PML::RARA rearrangements missed by standard FISH probes.
Metaphase FISH and qRT-PCR confirmed the presence of PML::RARA transcripts in both cases.
Different probe sets failed to detect rearrangements in each case, highlighting diagnostic variability.
Abstract
Background/Objectives: Acute promyelocytic leukemia (APL) is a medical emergency associated with life-threatening complications such as disseminated intravascular coagulation (DIC), necessitating prompt therapeutic intervention and rapid diagnostic confirmation. APL is characterized by a translocation of the PML gene (15q24) with the RARA gene (17q21), resulting in the PML::RARA fusion gene on the derivative chromosome 15. Atypical PML::RARA rearrangements may escape detection by standard FISH probes. This study highlights limitations of commonly used probe sets and underscores the need for alternative FISH probe sets and complementary molecular testing. Methods: Two unique APL cases with atypical PML::RARA rearrangements were identified in our laboratory. Each case was evaluated at diagnosis using two commercially available FISH probe sets from Abbott Molecular and Cytocell. Metaphase…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
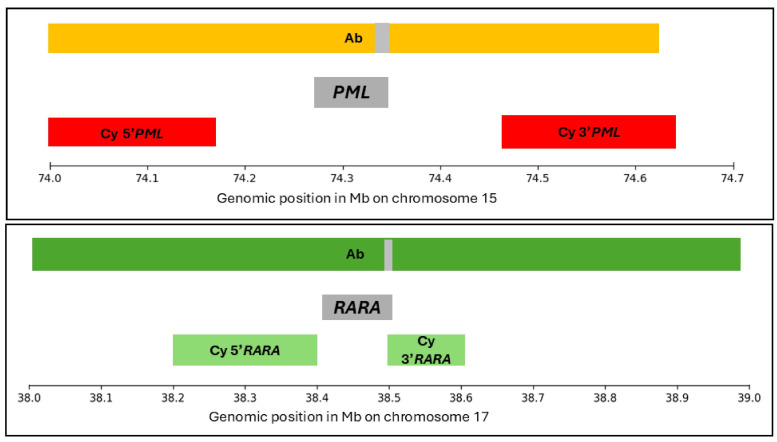 Figure 1
Figure 1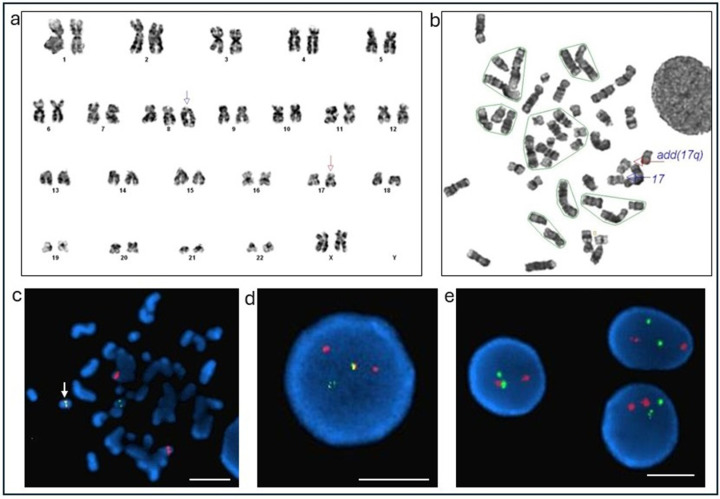 Figure 2
Figure 2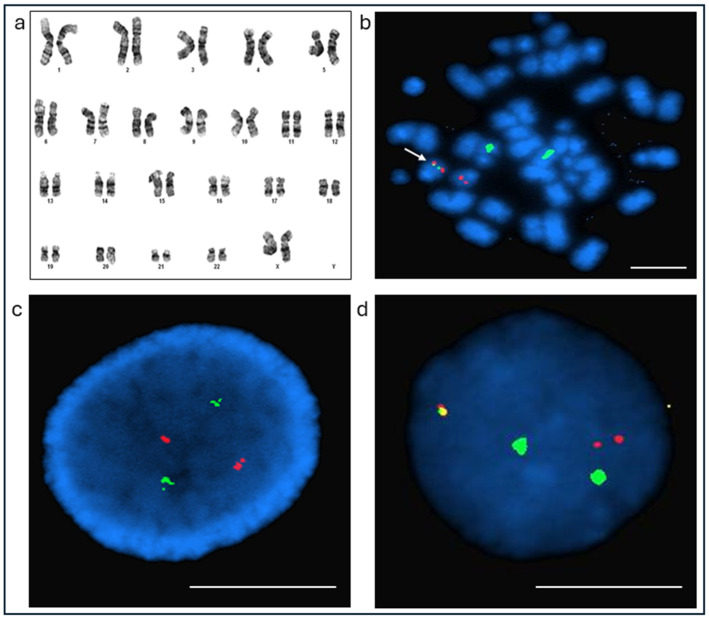 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinoids in leukemia and cellular processes · Acute Myeloid Leukemia Research · Genomic variations and chromosomal abnormalities
1. Introduction
Acute promyelocytic leukemia (APL) is a medical emergency that necessitates prompt therapeutic intervention to prevent life-threatening complications, most notably disseminated intravascular coagulation (DIC). Due to the urgency of treatment, a rapid diagnostic turnaround time (TAT) is essential. APL is characterized by a specific chromosomal translocation involving the PML gene located at 15q24 and the RARA gene at 17q21, resulting in the formation of a PML::RARA fusion gene on the derivative chromosome 15. Multiple breakpoints have been identified within both genes. The PML gene contains three well-defined breakpoint cluster regions (bcr) 1-3: bcr1 in intron 6, bcr2 in exon 6, and bcr3 in intron 3. Additionally, a rare bcr within the PML gene has been identified in intron 7, contributing to a less common variant of the PML::RARA fusion transcript. In contrast, the majority of RARA breakpoints are located within intron 2. These variations give rise to four distinct PML::RARA fusion transcripts [1].
While most PML::RARA fusions result from balanced translocations, a subset of cases arises from insertional events, where PML is inserted into RARA or vice versa. These atypical rearrangements are often referred to as “cryptic” or “masked” translocations because they can evade detection by conventional cytogenetic methods [2]. Fluorescence in situ hybridization (FISH) is a widely utilized diagnostic tool for APL, offering rapid TAT and high sensitivity for typical rearrangements. However, the design and genomic coverage of commercially available dual-color, dual-fusion PML::RARA FISH probe sets can impact their ability to detect rare, atypical rearrangements. This study presents two cases of APL with cryptic PML::RARA rearrangements, highlighting the limitations of standard FISH probes and emphasizing the importance of using alternative probe sets and complementary molecular testing for accurate diagnosis.
2. Materials and Methods
A retrospective review of newly diagnosed APL cases from 2020 and 2021 was performed. Eight cases were identified: four exhibited the typical PML::RARA rearrangement FISH signal pattern with two fusion signals, while the remaining four showed atypical patterns. Two of the atypical cases were excluded—one due to the absence of conventional karyotype results and the other because the atypical FISH pattern resulted from a three-way translocation. The remaining two atypical APL cases, suspected to involve cryptic insertion events of either PML or RARA, were further investigated. The institutional review board approved this review.
Diagnostic evaluation included morphological evaluation of blood or bone marrow, flow cytometry, conventional karyotyping, FISH, next-generation sequencing (NGS) using a 141-targeted myeloid gene panel, and quantitative real-time PCR (qRT-PCR) for PML::RARA transcript detection. Morphologic, flow cytometry, and qRT-PCR results were obtained as part of the patients’ clinical care and collected from the electronic health records.
Conventional cytogenetics was performed on the bone marrow aspirate culture, and analysis of 20 G-banded metaphases was performed using the Cytovision automated imaging system (Leica Biosystems, Nussloch, Germany). FISH was performed on the fixed cells using a dual-color dual-fusion PML::RARA probe set for the two cases investigated in this study. These FISH probes included LSI PML/RARA t(15;17) 05J70-001 PML orange and RARA green from Abbott (Ab) Molecular Inc, USA, and/or LPH501-A FAST PML in Texas red and LPH501-A FAST RARA in FITC from CytoCell (Cy) Ltd., Cambridge, UK [3], Figure 1.
The Cy probe utilizes flanking centromeric and telomeric probes for each gene, providing partial coverage of RARA and no direct coverage of PML. In contrast, the Abbott probe spans a broader region, covering most of the PML (15q22–24) and RARA (17q21) loci, including substantial flanking sequences (Figure 1). All eight APL cases identified were processed with the Cy-dual-color dual-fusion probe. The two cases that were further evaluated were also processed using the Ab probe set. The 2024 International System for Human Cytogenetic Nomenclature was used for reporting karyotype and FISH results.
Genomic DNA extracted from the collected bone marrow samples was processed using the QIAseq Targeted DNA Human Myeloid Neoplasms Panel (QIAGEN GmbH, Hilden, Germany), involving the 141 myeloid-related genes [6]. Detected variant calls were classified according to the American College of Medical Genetics and Genomics (ACMG) and American Molecular Pathology guidelines using QIAGEN Clinical Insight–Interpret software, version 6.0.20200522 [7].
3. Results
The conventional cytogenetic and FISH results using the PML::RARA probe(s) are presented in Table 1.
3.1. Case 1
The first case of interest, received in the cytogenetics laboratory in October 2020, involved a bone marrow specimen from a 29-year-old female who presented with persistent fevers and malaise and tested positive for COVID-19. She continued to have fevers despite taking acetaminophen and ibuprofen at high doses. She was subsequently admitted to the emergency department with anemia, thrombocytopenia, and leukocytosis. On Day 1, laboratory evaluation at an outside institution revealed a white blood cell count of 26,000/μL and circulating blasts on peripheral smear, raising clinical suspicion for APL. All-trans retinoic acid (ATRA) 40 mg twice daily was given pending an APL diagnosis. Diagnostic bone marrow aspirate revealed a hypercellular marrow (100%) with 92% blast equivalents, including atypical hypogranular promyelocytes and markedly decreased trilineage hematopoiesis. Morphologic evaluation showed blasts with a spectrum of appearances, including folded cerebriform nuclei and a subset with bilobed nuclei typical of microgranular APL. Occasional Auer rods were identified. Empiric treatment with prednisone and tretinoin was initiated. Due to worsening leukocytosis, a bone marrow biopsy was performed on Day 4, and the morphologic assessment was concerning for APL. The patient care was transferred to the current institution for further treatment on Day 8. Peripheral blood flow cytometry demonstrated that atypical myeloid precursors accounted for 93% of total events. These cells expressed CD11b, CD13, CD15 (dim), CD33, CD38, CD64, CD117 (dim), CD123, and cytoplasmic MPO, while lacking expression of CD11c, CD14, CD34, HLA-DR, and all lymphoid markers. NGS detected four variants in the diagnostic sample: a tier 1A FLT3 p.D835V variant and three tier 3 KDM6A p.R1111P, RELN p.T3242M, and RELN p.D293N variants. Follow-up NGS performed 1 month after the initial test detected a single RELN p.D293N variant. Conventional cytogenetics yielded 47,XX,+der(8)add(8)(p11.2)dup(8)(q13q22),add(17)(q21)[cp9]/46,XX[11] karyotype (Figure 2a).
Initial FISH analysis using the Cy dual-color, dual-fusion probe for PML::RARA rearrangement was negative (Figure 2e). Conventional karyotyping revealed additional genetic material at the 17q21 breakpoint (Figure 2a,b). The patient was started on hydroxyurea on Day 4 for hyperleukocytosis and developed spontaneous tumor lysis syndrome and DIC. She received allopurinol. Fresh-frozen plasma was administered to manage low fibrinogen levels.
Given the high clinical suspicion for APL, molecular analysis for PML::RARA mRNA was performed, which confirmed a fusion involving RARA and the breakpoint cluster region 3 (bcr3, intron 3) of the PML gene. Due to the limited genomic coverage of the Cytocell probe, FISH was repeated using the Ab probe, which targets a broader region of the PML and RARA loci (Figure 1). The Ab probe yielded a positive result, demonstrating an atypical PML::RARA fusion (Figure 2d). Metaphase FISH confirmed a cryptic fusion signal on the abnormal chromosome 17q (Figure 2c).
The patient initially received four days of induction chemotherapy with a 7+3 regimen beginning on Day 9 and was subsequently transitioned to a high-risk APL treatment protocol with ATRA and arsenic trioxide (AO), initiated on Day 12. Prophylaxis for differentiation syndrome was completed on Day 20. The patient remains in remission (last assessed March 2025).
3.2. Case 2
The second case involved a 30-year-old female who presented to an outside hospital emergency department in December 2021 (Day 1), with left wrist erythema, swelling, and a fever of 100.7 °F. Laboratory evaluation revealed pancytopenia, prompting a bone marrow biopsy that was suspicious for APL. Outside bone marrow evaluation reported hypercellular marrow with decreased trilineage hematopoiesis and 77% blasts and promyelocytes. She was subsequently transferred to the University of Kansas Health System, where a repeat bone marrow biopsy was performed on Day 2. Morphologic evaluation of the bone marrow revealed a hypercellular marrow (~90%) with markedly decreased trilineage hematopoiesis and 77% blasts, including atypical promyelocytes with abundant cytoplasmic granules and occasional Auer rods. Flow cytometry findings were consistent with APL. The NGS study detected no clinically actionable or oncogenic gene variants. A KLHL6 p.Y129N variant of unknown significance was detected at an allelic fraction of 49.0%. The functional consequences and clinical significance of this variant are not established.
Treatment with ATRA and arsenic trioxide was initiated the same day. Cytogenetic analysis revealed a normal karyotype (Figure 3a), and initial FISH testing with the Ab probe for the PML::RARA rearrangement was negative (Figure 3c). Given the strong clinical suspicion for APL, additional molecular studies were pursued. qRT-PCR confirmed the presence of the PML::RARA fusion transcript. FISH analysis was repeated using the Cy probe, which yielded a positive result with an atypical signal pattern (Figure 3d). Metaphase FISH using the Cy probe confirmed a cryptic PML::RARA fusion on chromosome 15, consistent with a cryptic RARA insertion event (Figure 3b). The patient was discharged on January 13 with close outpatient follow-up through the University of Kansas Health System Hematology service for continued management of ATRA/arsenic therapy and monitoring of neutropenia. No further bone marrow biopsies were performed, and yearly complete blood count (CBC) evaluations remained unremarkable. For non-hematologic concerns with autism with cognitive delay, bipolar disorder, seizures, and prior cardiac problems, the patient is followed up by the general medicine and psychiatric teams. The patient was last followed in December 2025, with an unremarkable CBC. The peripheral blood test for quantitative evaluation of the PML::RARA transcripts is pending at the time of manuscript preparation.
4. Discussion
The diagnosis of APL is typically confirmed by detection of the reciprocal translocation t(15;17)(q24;q21), which results in the PML::RARA gene fusion. Conventional cytogenetic techniques, such as karyotyping and FISH, are commonly used to identify this rearrangement. However, in rare cases, the characteristic translocation may be absent due to cryptic rearrangements, including submicroscopic insertions of RARA into PML or other complex structural variants. These cryptic forms of APL may present with variable cytogenetic findings or even a normal karyotype, and may yield negative FISH results, increasing the risk of misdiagnosis and delayed treatment.
The PML and RARA FISH probe coverage differs significantly between Ab and Cy. The Ab probe is larger and spans both the PML and RARA genes, whereas the Cy probes primarily target the flanking regions of these genes, covering only a small portion of 3′ RARA. As shown in Figure 1, the Cy probes are shorter than the Ab probes. In a typical 15;17 translocation, the derivative chromosome 15 is pathognomonic and leads to expression of the PML::RARA fusion transcript [8]. In Case 1, molecular RT-PCR detected a BCR3-PML::RARA fusion transcript, while FISH using an Ab probe revealed a cryptic PML insertion into the RARA region on chromosome 17 and Cy was normal. Because the Ab probe spans the entire PML gene, it offers a broader advantage over the Cy probe set for detecting cryptic PML insertion events that are missed by Cy probes, which do not cover the PML gene but its flanking regions (Figure 1). Molecular qRT-PCR confirmed the presence of the PML::RARA fusion transcript in Case 2, the medical records lacked details regarding the isoform in Case 2. A normal karyotype in this case did not help to further investigate the discrepancy in results between the Ab and Cy PML::RARA probes. The two cases presented in this study are limited by the absence of direct sequencing of the PML and RARA genes due to insufficient diagnostic specimens. This would have enabled precise breakpoint mapping at the PML and RARA loci on chromosomes 15 and 17, respectively, and provided better insight into the limitations of the Ab and Cy probe sets.
Several studies have described cryptic and atypical PML::RARA gene fusions, occurring with or without a normal conventional karyotype, primarily detected using the Abbott dual-color dual-fusion FISH probe set [9,10,11]. In one such study, FISH analysis revealed a submicroscopic insertion of chromosome 15 material into 17q, despite a normal karyotype [10]. While FISH-negative cases were infrequent, these studies did not evaluate alternative FISH probe sets from other vendors, which may differ in genomic coverage and sensitivity. As a result, the limitation of these alternative probe sets for detecting PML::RARA rearrangements remains unaddressed. Consequently, the findings from these prior studies cannot be directly correlated with the cases presented in the current study.
In APL, co-occurring mutations are present in 70% of the cases [8,12]. FLT3-ITD and FLT3-D835 are the most common gene mutations seen in both pediatric and adult populations. Other non-recurring mutations involve genes in the MAPK pathway and transcription regulatory genes, including KDM6A [8,13,14]. However, there is limited evidence of co-occurring mutations in the literature with a variant or atypical PML::RARA gene rearrangement [8,15,16,17]. A synergistic antileukemogenic effect of ATRA and AO therapy was observed in APL harboring the FLT3 mutation [18,19]. This observation is supported by the current finding in case 1, in which, after post-ATRA and AO therapy, NGS of the follow-up specimen showed loss of the FLT3 oncogenic variant.
Advanced cytogenetic techniques offer a valuable alternative for investigating atypical insertional translocations. Optical genome mapping (OGM), an emerging and cutting-edge cytogenomic molecular technology, enables genome-wide detection of structural rearrangements at gene-level resolution. Multiple studies have demonstrated its utility in identifying submicroscopic structural abnormalities that are often missed by conventional karyotyping. Furthermore, OGM has proven effective in elucidating complex chromosomal rearrangements, including cryptic fusion genes, thereby enhancing diagnostic precision and genomic characterization [20,21]. OGM has identified a similar insertion event involving the PML: RARA fusion insertion into the RARA gene on 17q in a normal karyotype, and an atypical PML::RARA FISH signal pattern was detected using the Ab PML::RARA dual color dual fusion FISH probe [22].
The two cases presented here illustrate that neither the Ab nor the Cy FISH probes alone are sufficient to detect all possible rare PML::RARA fusion variants. However, using both probe sets may improve detection sensitivity. A study by Campbell et al. [23] evaluated ten cases of APL with RARA insertions into PML using both Ab and Cy dual-fusion FISH probes. The Cy probe detected the fusion in 7 of 10 cases, while the Ab probe yielded equivocal results in 3 cases and was negative in the remaining 7 cases. Notably, our first case demonstrated the opposite outcome: the Ab probe was positive while the Cy probe was negative. This case involved a PML insertion into RARA, whereas the Campbell study focused exclusively on RARA insertions into PML. These findings suggest that reflex testing with an alternate FISH probe is warranted in rare cases with high clinical suspicion for APL and negative initial FISH results. In both cases, ATRA therapy was initiated based on a strong clinical suspicion of APL, before diagnostic confirmation, to prevent DIC. FISH studies did not delay therapy initiation in either case. However, subsequent diagnostic confirmation was crucial for continuing ATRA therapy and avoiding unnecessary chemotherapy [24,25].
The proposed FISH testing algorithm for APL diagnosis should begin with dual-color, dual-fusion FISH for PML::RARA using a commercially available probe validated in a clinical laboratory in accordance with regulatory guidelines. A positive result confirms APL. If FISH is negative but morphology and/or immunophenotype strongly suggest APL, reflex testing should include an alternative vendor’s FISH probe with different genomic coverage and RT-PCR for PML::RARA transcript detection to capture rare cryptic rearrangements. If the second FISH probe is negative but RT-PCR is positive, direct sequencing or OGM should be considered to identify rare RARA fusions and determine precise breakpoints in PML and RARA genes.
5. Conclusions
Cryptic PML::RARA rearrangements in APL can evade detection by standard FISH probes due to limitations in probe design and genomic coverage. FISH remains the essential diagnostic assay for detecting the PML::RARA rearrangement, given its short TAT. These cases underscore the need for reflex testing with alternative probe sets in patients with an initial negative FISH result and for further follow-up with molecular confirmation via qRT-PCR or OGM in patients with high clinical suspicion for APL. This approach helps prevent false-negative FISH results, reducing diagnostic delays and enabling timely initiation of life-saving therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dekking E.H. van der Velden V.H. Varro R. Wai H. Böttcher S. Kneba M. Sonneveld E. Koning A. Boeckx N. Van Poecke N. Flow cytometric immunobead assay for fast and easy detection of PML-RARA fusion proteins for the diagnosis of acute promyelocytic leukemia Leukemia 2012261976198510.1038/leu.2012.12522948489 PMC 3437408 · doi ↗ · pubmed ↗
- 2Platzbecker U. Khoury J.D. Akkari Y. Mathews V. Tembhare P. Haferlach T. Acute promyelocytic leukaemia with PML::RARA fusion WHO Classification of Haematolymphoid Tumours 5th ed. WHO Classification of Tumours Editorial Board International Agency for Research on Cancer Lyon, France 2024 Volume 11Available online: https://publications.iarc.who.int/637(accessed on 2 November 2025)
- 3Brown L.E. Zhang D. Persons D.L. Yacoub A. Ponnala S. Cui W. A 26-Year-Old Female with Systemic Mastocytosis with Associated Myeloid Neoplasm with Eosinophilia and Abnormalities of PDGFRB, t(4;5)(q 21;q 33)Case Rep. Hematol.20162016415856710.1155/2016/415856727648315 PMC 5014931 · doi ↗ · pubmed ↗
- 4Cyto Cell PML/RARα (RARA) Translocation, Dual Fusion Cytocell Available online: https://www.ogt.com/products/product-search/cytocell-pml-rar%CE%B 1-rara-translocation-dual-fusion/(accessed on 2 November 2025)
- 5ASR Vysis LSI PML/RARA Dual Color, Dual Fusion Translocation Probe Available online: https://www.molecular.abbott/int/en/chromosome-main/15(accessed on 2 November 2025)
- 6Tatarian J. Tupper N. Li P. Feusier J. Abdo M. Hyter S. Gonzales P.R. Zhang D. Woodroof J. Kelting S. Morphologic, Immunophenotypic, Molecular Genetic, and Clinical Characterization in Patients with SRSF 2-Mutated Acute Myeloid Leukemia Am. J. Clin. Pathol.2023160490499 Erratum in Am. J. Clin. Pathol. 2023, 160, 544. https://doi.org/10.1093/ajcp/aqad 14110.1093/ajcp/aqad 07737458189 PMC 10629464 · doi ↗ · pubmed ↗
- 7Richards S. Aziz N. Bale S. Bick D. Das S. Gastier-Foster J. Grody W.W. Hegde M. Lyon E. Spector E. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology Genet. Med.20151740542410.1038/gim.2015.3025741868 PMC 4544753 · doi ↗ · pubmed ↗
- 8Liquori A. Ibañez M. Sargas C. Sanz M.Á. Barragán E. Cervera J. Acute Promyelocytic Leukemia: A Constellation of Molecular Events around a Single PML-RARA Fusion Gene Cancers 20201262410.3390/cancers 1203062432182684 PMC 7139833 · doi ↗ · pubmed ↗