Clinical Impact of Multifocality and Bilaterality on Lymph Node Metastasis in Papillary Thyroid Microcarcinoma
Merima Goran, Marko Buta, Srdjan Nikolic, Nada Santrac, Nikola Jeftic, Nevena Savkovic, Jovan Raketic, Zoran Kozomara, Natasa Medic-Milijic, Ana Cvetkovic, Saska Pavlovic, Ivan Markovic

TL;DR
This study finds that multifocal papillary thyroid microcarcinomas are linked to more aggressive features and higher lymph node metastasis rates, guiding treatment strategies.
Contribution
The study establishes a strong link between multifocality and increased lymph node metastasis in PTMC, informing clinical risk stratification.
Findings
Multifocal PTMC tumors are associated with larger size, capsular invasion, and higher lymph node metastasis rates.
The number of tumor foci is strongly linked to both central and lateral lymph node metastases.
Bilaterality correlates with aggressive tumor features but not independently with lymph node metastasis.
Abstract
Objective: Papillary thyroid microcarcinoma (PTMC) often presents with multifocality and bilaterality, but the clinical significance of these features and their association with cervical lymph node metastases (LNMs) remain debated. The aim of this study was to investigate the patterns of multifocality and bilaterality in PTMC and their association with central and lateral neck lymph node metastases. Methods: This retrospective study analyzed 254 patients with histologically confirmed PTMC treated at the Institute for Oncology and Radiology of Serbia between 2004 and 2016. All patients underwent total thyroidectomy with central and, when indicated, lateral neck dissection. Associations between multifocality, bilaterality, and cervical LNM were evaluated using appropriate statistical tests. A p-value < 0.05 was considered statistically significant. Results: Multifocal tumors were present…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
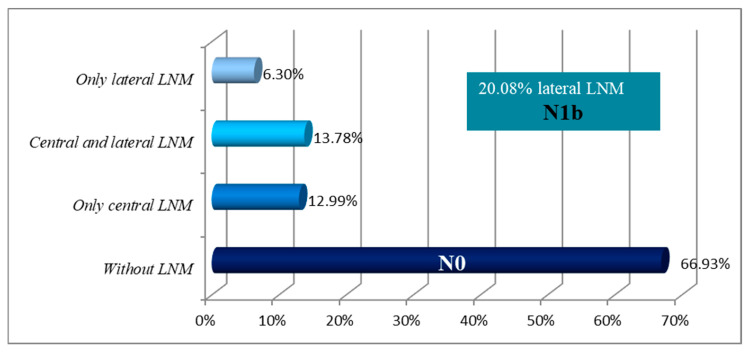 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid and Parathyroid Surgery · Head and Neck Cancer Studies
1. Introduction
According to the World Health Organization (WHO), papillary thyroid microcarcinomas (PTMCs) are papillary thyroid carcinomas (PTCs) measuring ≤ 10 mm in greatest dimension [1]. It is estimated that PTMCs comprise up to 50% of all PTCs. The rising incidence of these tumors likely reflects improved ultrasound diagnostics, expanded surgical indications, and more detailed histopathological processing using thinner tissue sections [2,3]. Despite the increasing incidence, overall mortality from PTMC has remained stable, as these tumors are typically indolent and associated with an excellent prognosis [4].
Multifocality is a common feature of PTMC with its etiology remaining insufficiently understood. Some studies suggest multicentric malignant transformation of follicular cells, supported by evidence of distinct clonal origins among multiple tumor foci [5,6]. Other studies suggest intraglandular spread of a primary tumor through the thyroid’s rich lymphatic network, supported by evidence of identical clonal origin among tumor foci [7]. Bansal et al. found that unilateral multifocal tumors often share the same mutation, while bilateral tumors typically show different mutational profiles [8]. Some authors therefore consider unilateral multifocal and bilateral tumors to be separate entities, with differing clinical behavior, biology, and outcomes, as supported by their divergent mutation statuses [9].
Lymph node metastases (LNMs) indicate regional dissemination of disease to the cervical lymph nodes. This most commonly involves the central neck compartment, level VI, but may also affect the lateral compartments, including levels II through V [10]. Their presence indicates more aggressive tumor behavior, particularly when evident preoperatively, when metastases are larger, or when multiple lymph nodes are involved [11]. During the 2000s, the optimal extent of surgery for PTMC was still under discussion. Many tertiary centers performed total thyroidectomy with prophylactic central neck dissection (CND) to improve pathological staging and guide adjuvant therapy, particularly in multifocal or bilateral disease. Sentinel lymph node biopsy (SLNB) was also explored as a technique to detect occult lateral neck metastases in clinically node-negative patients, enabling a more accurate assessment of disease spread and potential aggressiveness. Although these procedures were not universally adopted, several studies have demonstrated their diagnostic and prognostic value in refining surgical planning and risk stratification for PTMC [12,13,14,15]. However, despite numerous studies addressing the clinicopathological features of PTMC, data on the association between multifocality, bilaterality, and the pattern of cervical lymph node involvement, particularly in cohorts where both central and lateral neck regions were surgically assessed through standardized procedures such as central neck dissection and sentinel lymph node biopsy, remain limited. Further clarification of these relationships may contribute to a better understanding of disease behavior and support future refinements in risk stratification and management strategies.
The aim of this study was to investigate multifocality and bilaterality patterns in PTMCs and their association with the presence of cervical LNMs.
2. Materials and Methods
2.1. Patients and Data
This retrospective study included patients treated at the Institute for Oncology and Radiology of Serbia (IORS) between January 2004 and December 2016. The study included all patients with histopathologically confirmed PTMC and who underwent surgical evaluation of both central and lateral neck lymph nodes. Patients were excluded if they had tumors larger than 10 mm or incomplete lymph node assessment (only central, only lateral or none). Routine preoperative evaluation for all patients included neck and abdominal ultrasound, chest and neck X-rays (to assess tracheal deviation or compression), laryngoscopy to assess vocal cord function, thyroid function testing, and anesthesiologic assessment. Treatment decisions were made by a multidisciplinary thyroid tumor board. Preoperative, operative, and follow-up data were extracted from the institutional database.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Institute for Oncology and Radiology of Serbia (protocol code 01-1/2025/3280; 20 October 2025). The study was conducted using de-identified clinical data collected during routine care, with no patient contact or access to identifiable information. In accordance with institutional and national regulations, the ethics committee granted a waiver of informed consent.
2.2. Treatment
The treatment strategy for patients with preoperatively cytologically or intraoperatively frozen section–proven PTMC involved total or near-total thyroidectomy. In all patients without clinical evidence of central lymph node metastasis, prophylactic CND was performed, whereas those with clinically positive central lymph nodes underwent therapeutic CND. Sentinel lymph node biopsy (SLNB) was performed in patients without clinical or radiological evidence of lateral cervical lymph node metastases (cN0). The procedure was carried out on the affected side, or bilaterally in cases of bilateral PTMC, following the technique described by Džodić et al. [16]. After thyroid exposure and before gland mobilization, approximately 0.2 mL of 1% methylene blue dye was injected peritumorally using a fine needle to identify stained lymphatic vessels and sentinel nodes. The excised sentinel lymph nodes were sent for intraoperative frozen section analysis, and the results guided further surgical management. In cN0 patients with negative SLNB no additional lateral neck dissection was undertaken and patients were subjected to standard follow-up. If lateral lymph node metastases were clinically evident (cN1b) or confirmed by sentinel lymph node biopsy, a modified radical neck dissection (MRND) of the affected side was performed during the same procedure. In most patients who underwent MRND, it included lymph node levels II through IV, while level V was dissected only in cases with clinically or intraoperatively evident metastases. The spinal accessory nerve, internal jugular vein, and sternocleidomastoid muscle were preserved in all cases.
All cases were histopathologically confirmed as PTMC following standard processing of thyroidectomy specimens. Both thyroid lobes were examined in detail to assess tumor focality, bilaterality, and capsular invasion. All tissue samples, including thyroid, CND, SLNB, and MRND specimens, were examined by experienced endocrine pathologists using standardized protocols to determine the presence and extent of lymph node metastases.
2.3. Statistical Analysis
Categorical variables were described using frequencies (percentages), while mean, median, standard deviation (SD), and range were used for numeric variables. Multifocality and bilaterality were analyzed in relation to patient demographics, tumor characteristics, and the presence of cervical LNMs in order to assess potential associations. The normality of distribution for continuous variables was assessed using visual methods (Normal Q-Q plots and histograms) and statistical tests (Kolmogorov–Smirnov and Shapiro–Wilk tests). To compare differences between groups, the Pearson’s χ^2^ test, Fisher’s exact test, or the Wilcoxon rank-sum test were applied, depending on the type and distribution of the variables. A p-value of <0.05 was considered statistically significant. In cases of multiple testing on the same dataset, Bonferroni correction was applied to adjust the significance threshold. Statistical analyses were performed using R version 3.3.2 (2016-10-31)—“Sincere Pumpkin Patch”; Copyright (C) 2016 The R Foundation for Statistical Computing; Platform: x86_64-w64-mingw32/x64 (64-bit) (available at: www.r-project.org; downloaded: 21 January 2017).
3. Results
A total of 254 patients met the inclusion criteria for this study. The study population included a predominance of female patients (84.65%). Average age of patients was 47.7 years (Table 1). Metastases in the cervical lymph nodes were histopathologically confirmed in 84 (33.07%) patients. Metastases limited to the central neck compartment (N1a) were found in 33 patients (12.99%). Skip metastases, involving only the lateral compartment without central lymph node involvement, were identified in 16 patients (6.30%), while both central and lateral metastases were present in 35 patients (13.78%). These two groups were collectively classified as N1b (Table 1, Figure 1). Multifocal disease was present in 103 patients (40.55%). Notably, among patients with multifocal tumors, the number of those with bilateral involvement was 69 (66.99%) compared with 34 (33.01%) in those with unilateral multifocal disease. Capsular invasion was detected in 20.87% of patients, and vascular invasion was observed in only one patient (Table 2).
The association between the number of PTMC foci and patient and tumor characteristics is presented in Table 3. A statistically significant difference in sex distribution was observed between patients with unifocal and multifocal tumors, with the proportion of male patients being 11.26% in unifocal group compared to 21.36% in the multifocal group. Multifocal tumors were also associated with larger average tumor size compared to unifocal tumors. Additionally, the prevalence of capsular invasion and the incidence of cervical lymph node metastases (central, lateral, or both) were significantly higher among patients with multifocal tumors.
The association between the number of PTMC foci and the presence of cervical LNM is presented in Table 4. Patients with cervical LNM (central, lateral, or both) had, on average, a greater number of PTMC foci compared to those without metastases. Furthermore, an increasing number of PTMC foci were associated with a higher likelihood of central and overall LNM. A similar trend was observed for lateral LNM, although it did not reach statistical significance.
The association between laterality and patient and tumor characteristics in subgroup of patients with multifocal PTMC is presented in Table 5. Patients with bilateral tumors had larger average tumor size and a greater number of tumor foci compared to those with unilateral multifocal disease. Capsular invasion was also more frequently observed in the bilateral group. No significant difference was observed in the presence of LNM between patients with unilateral and bilateral multifocal PTMC.
Two patients experienced recurrent laryngeal nerve (RLN) injury during surgery. In one case, the RLN was accidentally transected intraoperatively, promptly recognized, and repaired with direct perineurial suturing. The second patient developed transient RLN palsy, which resolved spontaneously within six months. No cases of permanent hypoparathyroidism or other major thyroid or neck dissection-related complications were reported. Local recurrence occurred in two female patients and distant recurrence occurring in one male patient with occult PTMC diagnosed via biopsy of an enlarged cervical lymph node.
4. Discussion
The reported prevalence of multifocality in papillary thyroid carcinomas varies widely, ranging from 18% to 87.5%, largely due to differences in histopathological tissue processing [4,17]. In our study, multifocal tumors were identified in 40.55% of patients, consistent with findings from other studies [18,19]. The prevalence of bilaterality in PTMC typically ranges from 10–30%, though rates up to 68.1% have been reported, largely reflecting differences in histopathological techniques [18,20]. In our cohort, bilateral tumors were present in 27% of patients, while 13% showed unilateral multifocality. Comparable rates of bilaterality were observed by Varshney et al. (28.8%) and Karatzas et al. (24.1%) [18,19].
The mean number of tumor foci per patient was 1.97 in our cohort, compared with 1.6 in a similar series. In multifocal tumors, secondary foci were generally smaller than the dominant lesion, averaging 1.8 mm in our study versus 3.2 mm reported by So YK et al. [21]. In our study, total number of tumor foci was significantly higher in patients with LNM compared to those without (2.79 vs. 1.56, p = 0.0009). Similarly, Al Afif reported an association between tumor focus number and central LNM in PTC [22]. In the study by Lee HS et al., the incidence of LNM in multifocal PTMC ≤ 5 mm was 42.3%, and multifocality was identified as the sole predictor of LNM in small PTMC [23].
Tumor size is another factor linked to increased aggressiveness, with larger tumors being more likely to metastasize to lymph nodes. In PTMC, tumors > 5 mm are considered more aggressive due to a higher risk of LNM [24,25]. In our study, multifocal tumors were significantly larger than solitary tumors (5.17 mm vs. 4.8 mm, p = 0.0134). Multifocality was more common in tumors measuring 6–10 mm compared to those ≤ 5 mm, although without statistical significance, consistent with findings by So YK et al. [21], while Kaliszewski and Kim reported statistically significant associations [26,27]. Bilaterality was also more common in larger tumors, consistent with findings by Kaliszewski [26]. In our study, capsular invasion was more frequent in multifocal and bilateral tumors. Karatzas et al. and Cupisti reported associations between multifocality, bilaterality, and capsular invasion, consistent with our findings [18,28].
LNMs were present in 33.07% of patients, in our study, with central compartment metastases identified in 26.77% and lateral metastases in 20.08%. Similar results were reported by Cheng F and Luo Y, but with the frequency of lateral LNMs being notably higher in our cohort [29,30]. LNMs occurred more frequently in multifocal tumors, supporting the view that multifocality reflects more aggressive behavior. Although bilateral tumors also showed a trend toward increased LNMs, the difference was not statistically significant. Similarly, Zheng et al. found a strong association between multifocality and central LNM, but not with bilaterality [31]. However, some studies have reported no independent association between multifocality and central LNM in multivariate analyses [32,33].
A meta-analysis by Pyo et al. showed significantly higher recurrence rate in multifocal tumors [34], while Kuo et al. reported worse survival in multifocal compared to solitary tumors, although no difference was found between multifocal PTMC and larger multifocal carcinomas [35]. Incomplete surgical treatment is a recognized cause of recurrence in multifocal disease, supporting total thyroidectomy as the optimal approach for PTC, including PTMC, particularly when multifocality is confirmed preoperatively. In our cases, recurrence likely resulted from additional aggressive tumor features or incomplete lateral neck dissection (levels II–V), as both recurrences arose in previously dissected regions. Kaliszewski reported a higher incidence of distant metastases in multifocal and bilateral PTMC, with rates of 0.9% in solitary, 14.6% in multifocal, and 13.3% in bilateral tumors [26]. In contrast, only one patient in our study developed distant metastases, originating from an occult solitary PTMC.
In recent years, active surveillance has emerged as a viable and evidence-based management option for carefully selected patients with low-risk PTMC. Large prospective and multicenter studies have demonstrated that, in the absence of high-risk features, active surveillance can safely replace immediate surgery without compromising oncologic outcomes [36,37,38]. Adequate patient selection remains the cornerstone of this approach, requiring careful assessment of clinical, radiological, and pathological factors that may predict disease progression. Recent reviews have emphasized that features such as multifocality, extrathyroidal extension, and lymph node metastases should prompt caution when considering active surveillance [39,40]. The results of our study contribute to this evolving body of evidence by identifying multifocality as a marker associated with more aggressive disease behavior and an increased risk of nodal metastasis, suggesting that this feature can be incorporated into comprehensive decision-making algorithms when selecting patients for active surveillance. Although bilaterality was not significantly associated with lymph node metastasis in our cohort, it correlated with other markers of aggressiveness, including larger tumor size, capsular invasion, and multifocality. Therefore, bilaterality may also represent a relative risk factor when evaluating patients for active surveillance, and its presence should encourage a more individualized, cautious approach
This study comes with several limitations inherent to its retrospective design. The analysis was based on data collected from a single tertiary institution, which may limit the generalizability of the findings to broader populations. While efforts were made to ensure data accuracy, the retrospective nature introduces potential for selection and information bias. Molecular profiling was not performed, precluding evaluation of potential genetic differences between multifocal and bilateral tumors. Additionally, multivariate analysis was not conducted, limiting the ability to control for confounding variables This approach was not pursued due to the interrelation among several key variables, such as multifocality, bilaterality, and number of tumor foci, which could introduce collinearity and compromise model stability and interpretability; moreover, such analysis would require a larger, prospectively designed study specifically powered for predictive modeling. The absence of long-term outcome analysis limits conclusions regarding recurrence and overall survival.
5. Conclusions
Multifocality in PTMC is a common finding and was significantly associated with male sex, larger tumor size, capsular invasion, and higher rates of lymph node metastases. Bilateral tumors also showed more aggressive features but without a statistically significant association with lymph node involvement. Although local recurrence was rare, it occurred exclusively in patients with multifocal disease, suggesting a trend toward more aggressive behavior. While active surveillance remains appropriate for carefully selected low-risk patients, the presence of multifocality, especially when combined with other high-risk features, should prompt a more cautious and individualized approach. These findings indicate that multifocal PTMC may represent a biologically distinct subtype, although confirmation requires studies incorporating long-term survival data and molecular profiling (BRAF, RAS, TERT, RET/PTC). Further research should define the independent prognostic role of multifocality and its potential inclusion in future risk stratification models for PTMC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Christofer Juhlin C. Mete O. Baloch Z.W. The 2022 WHO classification of thyroid tumors: Novel concepts in nomenclature and grading Endocr.-Relat. Cancer 202330 e 22029310.1530/ERC-22-029336445235 · doi ↗ · pubmed ↗
- 2Kaliszewski K. Diakowska D. Miciak M. Jurkiewicz K. Kisiel M. Makles S. Dziekiewicz A. Biernat S. Ludwig M. Ludwig B. The Incidence Trend and Management of Thyroid Cancer—What Has Changed in the Past Years: Own Experience and Literature Review Cancers 202315494110.3390/cancers 1520494137894308 PMC 10605595 · doi ↗ · pubmed ↗
- 3Weller S. Chu C. Lam A.K. Assessing the Rise in Papillary Thyroid Cancer Incidence: A 38-Year Australian Study Investigating WHO Classification Influence J. Epidemiol. Glob. Health 202515910.1007/s 44197-025-00354-539869269 PMC 11772643 · doi ↗ · pubmed ↗
- 4Bashir A.A. El-Zaheri M.M. Bashir A.A. Fayyad L. Obed A.H. Alkam D. Bashir A.Y. Papillary Thyroid Microcarcinoma in Thyroid Surgical Practice: Incidental vs. Non-Incidental: A Ten-Year Comparative Study Cancers 202517202910.3390/cancers 1712202940563679 PMC 12190977 · doi ↗ · pubmed ↗
- 5Giannini R. Ugolini C. Lupi C. Proietti A. Elisei R. Salvatore G. Berti P. Materazzi G. Miccoli P. Santoro M. The heterogeneous distribution of BRAF mutation supports the independent clonal origin of distinct tumor foci in multifocal papillary thyroid carcinoma J. Clin. Endocrinol. Metab.2007923511351610.1210/jc.2007-059417535994 · doi ↗ · pubmed ↗
- 6Park S.Y. Park Y.J. Lee Y.J. Lee H.S. Choi S.H. Choe G. Jang H. Park S.H. Park D.J. Cho B.Y. Analysis of differential BRAFV 600E mutational status in multifocal papillary thyroid carcinoma Cancer 20061071831183810.1002/cncr.2221816983703 · doi ↗ · pubmed ↗
- 7Fang H. Si Y. Wang C. Gong Q. Liu C. Wang S. Diffuse intrathyroidal dissemination of papillary thyroid carcinoma with no stromal fibrosis at presentation: A pattern of aggressive differentiated thyroid carcinoma Pathol.-Res. Pract.202122415351010.1016/j.prp.2021.15351034329840 · doi ↗ · pubmed ↗
- 8Bansal M. Gandhi M. Ferris R.L. Nikiforova M.N. Yip L. Carty S.E. Nikiforov Y.E. Molecular and Histopathologic Characteristics of Multifocal Papillary Thyroid Carcinoma Am. J. Surg. Pathol.2013371586159110.1097/PAS.0b 013e 318292 b 78023797723 · doi ↗ · pubmed ↗