Triplane Left Atrial Reservoir Strain in Cardiac Amyloidosis: A Comparative Study with Rhythm-Matched Controls
Marina Leitman, Vladimir Tyomkin, Shmuel Fuchs

TL;DR
This study shows that triplane echocardiography can detect significant atrial dysfunction in cardiac amyloidosis patients, even when they are in normal heart rhythm.
Contribution
The study introduces triplane LA strain as a novel, reproducible method to assess atrial dysfunction in cardiac amyloidosis.
Findings
Triplane LA reservoir strain was significantly lower in cardiac amyloidosis patients compared to controls.
Amyloidosis patients in sinus rhythm showed LA strain values similar to controls with atrial fibrillation.
Triplane and biplane LA strain measurements showed strong correlation and good agreement.
Abstract
Background: Cardiac amyloidosis is characterized by progressive myocardial and atrial infiltration, leading to atrial mechanical dysfunction, atrial fibrillation, and thromboembolic complications. Left atrial (LA) strain is an established marker of atrial function; however, data on triplane LA strain in cardiac amyloidosis are limited. Methods: We evaluated transthoracic echocardiographic examinations of 24 patients with cardiac amyloidosis and 24 age-, sex-, rhythm-, and ejection fraction-matched control subjects (9 with atrial fibrillation in each group). Among amyloidosis patients, 21 had transthyretin and 3 had light-chain cardiac amyloidosis. All examinations were performed during 2025. Triplane and biplane LA reservoir strain were assessed using speckle-tracking echocardiography. Two-way analysis of variance tested the effects of disease (amyloidosis vs. control) and rhythm (sinus…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
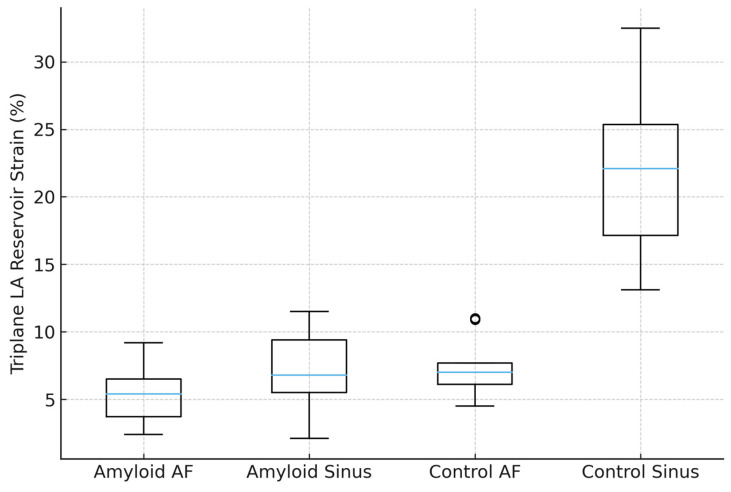 Figure 1
Figure 1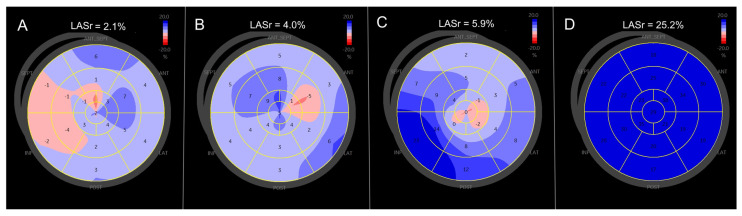 Figure 2
Figure 2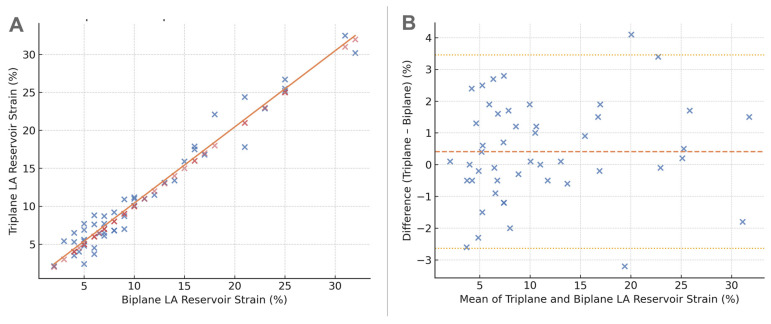 Figure 3
Figure 3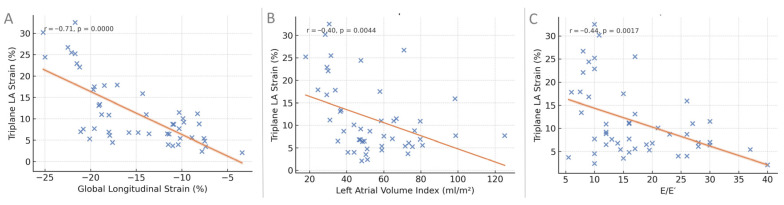 Figure 4
Figure 4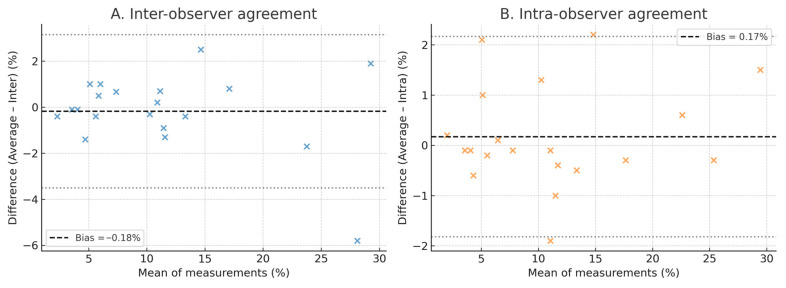 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Cardiovascular Function and Risk Factors · Takotsubo Cardiomyopathy and Associated Phenomena
1. Introduction
The development and increasing availability of disease-modifying therapies for transthyretin cardiac amyloidosis (ATTR-CA) have stimulated intensive research efforts and improved recognition of the disease and its associated clinical risks. Nevertheless, despite the establishment of multimodality diagnostic algorithms aimed at enhancing diagnostic accuracy, cardiac amyloidosis remains frequently underdiagnosed. In a Japanese cohort, the prevalence of cardiac amyloidosis increased markedly with advancing age, reaching 30–40% among patients with left ventricular hypertrophy, low atrial voltage, or both, detected during atrial fibrillation ablation procedures [1].
The diagnostic evaluation of cardiac amyloidosis typically begins with assessment of left ventricular structure and function, as echocardiography remains the first-line imaging modality. However, amyloid atriopathy—reflecting left atrial involvement—is increasingly recognized as a major contributor to disease burden. Amyloid infiltration of the atrial myocardium leads to electrical and mechanical dysfunction, predisposing patients to atrial fibrillation, loss of atrial contractile function, and worsening heart failure due to impaired atrioventricular coupling. The left atrium is affected both by direct amyloid deposition within the atrial wall and by secondary remodeling resulting from advanced left ventricular diastolic dysfunction [2,3]. These processes result in elevated left atrial pressures and severe impairment of atrial mechanical function, a condition commonly referred to as amyloid atriopathy.
Over the past decade, several studies have sought to characterize amyloid atriopathy using speckle-tracking echocardiography of the left atrium, most commonly through monoplane or biplane reservoir strain analysis [4,5,6,7]. More recently, the feasibility of triplane left atrial strain imaging has been demonstrated. Although triplane and biplane strain measurements show strong correlation, triplane analysis allows a more comprehensive visualization of left atrial deformation and regional heterogeneity, providing a more detailed functional “map” of atrial mechanics [8].
Accordingly, in the present study, we evaluated triplane left atrial reservoir strain in patients with cardiac amyloidosis and compared the findings with those of age-, sex-, rhythm-, and ejection fraction–matched control subjects.
2. Materials and Methods
2.1. Study Population
The study population consisted of 48 subjects, including 24 patients with cardiac amyloidosis and 24 age-, sex-, rhythm-, and ejection fraction–matched control subjects with preserved left ventricular function and no evidence of amyloidosis. The amyloidosis cohort included patients with transthyretin or light-chain cardiac amyloidosis diagnosed according to established clinical, imaging, and laboratory criteria. Control subjects were selected from individuals referred for echocardiographic evaluation who demonstrated normal left ventricular function.
Both amyloidosis patients and control subjects were identified retrospectively. The amyloidosis cohort consisted of consecutive eligible patients, whereas control subjects were selected retrospectively from echocardiography referrals and manually matched for age, sex, cardiac rhythm and left ventricular ejection fraction at the time of examination.
The study population was derived from the same institutional cohort previously evaluated for other echocardiographic parameters; however, the present analysis focused on a distinct endpoint (triplane left atrial strain), and one control subject was replaced to ensure matching by cardiac rhythm. No data or results from the present analysis were included in any previous publication. All echocardiographic examinations included in the study were performed between January and June 2025.
Cardiac amyloidosis was diagnosed according to established international criteria. Transthyretin cardiac amyloidosis was confirmed by the presence of typical echocardiographic features in conjunction with positive bone-avid scintigraphy (Perugini grade ≥2) in the absence of monoclonal protein. Light-chain amyloidosis was diagnosed based on histological confirmation of amyloid deposition with immunohistochemical or immunofluorescent typing. In the present cohort, 21 patients had transthyretin amyloidosis and 3 had light-chain amyloidosis.
2.2. Echocardiographic Acquisition and Measurements
All examinations were performed using a Vivid E95 ultrasound system (GE Healthcare, Horten, Norway) equipped with a 1.7–4.0 MHz transducer. Frame rates for speckle-tracking analysis were optimized and maintained at ≥50–90 frames/s whenever feasible. Standard parasternal long- and short-axis views, as well as apical four-, two-, and three-chamber views, were acquired in accordance with current chamber quantification guidelines [9].
Left ventricular diastolic function was assessed according to contemporary recommendations [10], including measurements of mitral E and A velocities, E/A ratio, E-wave deceleration time, septal and lateral tissue Doppler E′ velocities, and the E/E′ ratio.
Left atrial volume was calculated using the biplane area–length method and indexed to body surface area (left atrial volume index, LAVi). Left ventricular mass was calculated using the Devereux formula and indexed to body surface area (left ventricular mass index, LVMi). Relative wall thickness (RWT) was calculated as:
where PW represents posterior wall thickness and LVEDD—left ventricle end-diastolic diameter.
2.3. Speckle-Tracking Analysis
All echocardiographic studies were transferred to EchoPAC software (Version 206; GE Healthcare) for offline analysis. Endocardial borders were initially traced using automated speckle-tracking algorithms and manually adjusted when necessary to optimize tracking quality. End-systole was defined by aortic valve closure identified in the apical long-axis view and verified using aortic Doppler recordings.
2.4. Global Longitudinal Strain
Peak systolic longitudinal strain was measured for each left ventricular segment, and global longitudinal strain (GLS) was calculated as the average value obtained from the apical four-, two-, and three-chamber views.
2.5. Biplane Left Atrial Strain
Biplane left atrial reservoir strain was obtained from the apical four- and two-chamber views using automated software, in accordance with current recommendations [11,12,13].
2.6. Triplane Left Atrial Strain
Triplane left atrial strain was assessed using ventricular-dedicated two-dimensional speckle-tracking software (EchoPAC, Version 206; GE Healthcare). Left atrial longitudinal strain was measured separately from apical four-chamber, two-chamber, and three-chamber views by manual tracing of the left atrial endocardial border on high-quality two-dimensional images acquired at frame rates of 50–90 frames/s. Peak left atrial reservoir strain was obtained for each view, and the average of the three values was reported as triplane left atrial reservoir strain. This multi-view two-dimensional approach has been previously described and applied for the assessment of regional left atrial strain heterogeneity [8].
2.7. Reproducibility Analysis
To evaluate measurement reproducibility, left atrial reservoir strain was re-measured in 20 randomly selected studies (10 patients with cardiac amyloidosis and 10 control subjects). Inter-observer variability was assessed by two independent observers (M.L. and V.T.) blinded to each other’s results. Intra-observer variability was evaluated by one observer (M.L.) who repeated the measurements at least two weeks later, blinded to the initial results.
Reproducibility was quantified using the two-way random-effects intraclass correlation coefficient for absolute agreement [ICC (2,1)], Bland–Altman analysis (mean bias and 95% limits of agreement), within-subject standard deviation (Sw = SD of differences/√2), and coefficient of variation (CV% = 100 × Sw/mean).
2.8. Statistical Analysis
Continuous variables are presented as mean ± standard deviation, and categorical variables as number (percentage). Normality was evaluated using the Shapiro–Wilk test and visual inspection of Q–Q plots. Between-group comparisons were performed using independent-samples t tests or Mann–Whitney U tests, as appropriate. Categorical variables were compared using χ^2^ or Fisher’s exact tests. Associations were evaluated using Pearson or Spearman correlation coefficients. Statistical significance was defined as a two-sided p value < 0.05. All analyses were performed using IBM SPSS Statistics version 28.0 (IBM, Armonk, NY, USA).
2.9. Ethics
The study was approved by the Helsinki Ethics Committee of Shamir (Assaf Harofeh) Medical Center (Approval No. 137744; 0122-25-ASF(V1), 28 July 2025). Data extraction and analysis began on 1 August 2025, following receipt of this approval. All images were fully de-identified. The study complied with institutional policies and the principles of the Declaration of Helsinki. Given the retrospective and anonymized design, the requirement for written informed consent was waived.
3. Results
3.1. Baseline Characteristics
Baseline characteristics of the study population are summarized in Table 1.
Patients with cardiac amyloidosis and matched control subjects were comparable in age, sex distribution, body size, and major cardiovascular comorbidities. Atrial fibrillation during echocardiographic acquisition was present in 9 patients (37.5%) in each group, ensuring balanced rhythm distribution. The prevalence of hypertension, diabetes mellitus, chronic kidney disease, ischemic heart disease, chronic pulmonary disease, and prior atrial fibrillation did not differ significantly between groups. Functional status, as reflected by New York Heart Association (NYHA) class, was modestly worse in the amyloidosis group (2.8 ± 0.5 vs. 2.3 ± 0.9; p < 0.04). Among patients with cardiac amyloidosis, 21 had transthyretin amyloidosis and 3 had light-chain amyloidosis.
Echocardiographic Characteristics
Echocardiographic findings are presented in Table 2.
Left ventricular wall thicknesses and mass index were significantly higher in patients with cardiac amyloidosis compared with controls, consistent with myocardial infiltration. Although left ventricular ejection fraction was preserved in both groups, global longitudinal strain was markedly reduced in amyloidosis (−10.2 ± 2.6% vs. −20.1 ± 2.4%, p < 0.0001), indicating severe impairment of longitudinal myocardial mechanics. Left ventricular end-diastolic diameter was modestly smaller in amyloidosis, while diastolic filling indices demonstrated higher E/E′ ratios, consistent with elevated filling pressures.
Left atrial reservoir strain was markedly impaired in patients with amyloidosis using both biplane and triplane assessments (6.4 ± 2.5% and 6.7 ± 2.7%, respectively), compared with control subjects (15–16%; p = 0.0001 for both). Tricuspid annular peak systolic velocity was also significantly lower in amyloidosis, reflecting impaired right ventricular longitudinal function, whereas estimated pulmonary artery pressures and left atrial volume index were similar between groups. Age was not significantly correlated with triplane left atrial reservoir strain in the overall cohort, indicating that observed differences in atrial strain were not driven by age.
3.2. Effect of Disease Status and Cardiac Rhythm on Triplane LA Strain
Triplane left atrial reservoir strain demonstrated a graded distribution across the four disease–rhythm subgroups (Table 3, Figure 1).
The lowest strain values were observed in patients with cardiac amyloidosis and atrial fibrillation (5.5 ± 2.2%), followed by amyloidosis patients in sinus rhythm (7.4 ± 2.7%) and control subjects with atrial fibrillation (7.4 ± 2.1%). Control subjects in sinus rhythm exhibited preserved LA strain (21.5 ± 5.8%).
Two-way analysis of variance confirmed significant main effects of disease (F = 68.9, p < 0.0001) and rhythm (F = 45.0, p < 0.0001), as well as a significant disease-by-rhythm interaction (F = 26.5, p < 0.0001; Table 4), indicating that the impact of atrial fibrillation on LA strain was more pronounced in patients with cardiac amyloidosis.
3.3. Post Hoc Group Comparisons
Post hoc pairwise comparisons (Table 5) demonstrated a progressive decline in triplane LA reservoir strain from control subjects in sinus rhythm to patients with cardiac amyloidosis and atrial fibrillation.
All pairwise comparisons between amyloidosis and control groups, as well as between sinus rhythm and atrial fibrillation within each disease category, remained significant after Holm correction, with the exception of the comparison between amyloidosis patients in sinus rhythm and control subjects with atrial fibrillation (adjusted p = 0.12).
3.4. Representative Triplane LA Strain Patterns
Representative examples of triplane left atrial reservoir strain maps are shown in Figure 2.
Patients with cardiac amyloidosis and atrial fibrillation exhibited markedly reduced and heterogeneous LA strain, whereas amyloidosis patients in sinus rhythm showed modestly higher but still substantially impaired and heterogeneous deformation. Control subjects with atrial fibrillation demonstrated reduced strain with a visual appearance similar to that observed in amyloidosis patients in sinus rhythm. In contrast, control subjects in sinus rhythm displayed normal, uniform LA reservoir strain. These qualitative examples correspond closely with the quantitative group-level findings, particularly the similar mean strain values observed in amyloidosis patients in sinus rhythm and control subjects with atrial fibrillation.
3.5. Agreement Between Triplane and Biplane LA Strain
Triplane and biplane LA reservoir strain measurements showed a strong linear relationship (Pearson r = 0.94, p < 0.0001; 95% CI, 0.88–0.97). The correlation scatterplot (Figure 3A) demonstrated a near one-to-one relationship with minimal dispersion around the regression line. Bland–Altman analysis (Figure 3B) revealed a small mean bias of −0.5%, with 95% limits of agreement from −4.2% to +3.2%, indicating minimal systematic differences and no proportional bias across the measurement range.
3.6. Correlations with Ventricular Function and Filling Parameters
Triplane LA reservoir strain demonstrated a strong inverse correlation with left ventricular global longitudinal strain (r = −0.71, p < 0.0001), indicating that worsening ventricular deformation was associated with impaired atrial reservoir function (Table 6, Figure 4). Moderate negative correlations were also observed with left atrial volume index (r = −0.40, p = 0.004) and E/E′ ratio (r = −0.44, p = 0.002), suggesting that reduced atrial strain accompanies both atrial dilatation and elevated filling pressures.
3.7. Reproducibility Analysis
Inter-observer and intra-observer reproducibility results are presented in Table 7 and Figure 5. Inter-observer reproducibility was excellent (ICC = 0.98, CV ≈ 10.6%), and intra-observer reproducibility was near-perfect (ICC = 0.99, CV ≈ 6.5%). Similar reproducibility metrics were observed when amyloidosis and control subgroups were analyzed separately. Bland–Altman analyses demonstrated negligible systematic bias and narrow limits of agreement across the full range of strain values.
4. Discussion
In this study, we evaluated triplane left atrial reservoir strain in patients with cardiac amyloidosis compared with age-, sex-, and rhythm-matched control subjects. The principal finding is that triplane LA reservoir strain is markedly reduced in amyloidosis patients even when they are in sinus rhythm, with strain values similar to those observed in control subjects with atrial fibrillation. These findings indicate the presence of a severe atrial cardiomyopathy in cardiac amyloidosis that is largely independent of rhythm status.
4.1. Relation to Previous Studies
Our findings build upon and extend prior investigations using monoplane or biplane LA strain assessment in cardiac amyloidosis. Previous studies have consistently demonstrated that LA reservoir, conduit, and contractile strain components are significantly impaired in amyloidosis and correlate with left ventricular dysfunction, disease severity, prognosis, and thromboembolic risk [4,7,14].
In particular, Inoue et al. [15] showed that among patients with left ventricular hypertrophy, LA reservoir strain provided diagnostic utility in differentiating cardiac amyloidosis from other causes of hypertrophy (area under the curve ≈0.81). Reduced LA strain has also been reported in cardiac amyloidosis compared with Fabry disease [16] and hypertensive heart disease [17].
While the concept of amyloid-related LA myopathy is therefore well established, the present study adds incremental value by applying a triplane imaging approach. Triplane LA strain enables not only quantitative assessment of atrial reservoir function but also visualization of regional heterogeneity in atrial deformation and mechanics. As illustrated in Figure 2, this qualitative visualization provides insight into the pathophysiologic mechanisms linking amyloid infiltration, atrial dysfunction, atrial fibrillation, and thromboembolic vulnerability.
4.2. Pathophysiologic Implications
The marked reduction in triplane LA reservoir strain observed in amyloidosis patients—even in sinus rhythm—supports the concept that the left atrium is affected early and profoundly in the disease course. This impairment likely reflects a combination of direct amyloid infiltration of the atrial wall, elevated left atrial pressure secondary to restrictive ventricular physiology, and loss of atrial compliance and contractile reserve. These observations are consistent with histopathologic evidence of atrial amyloid deposition and imaging studies demonstrating increased atrial stiffness and mechanical dispersion in ATTR-CA [2,3].
Notably, amyloidosis patients in sinus rhythm exhibited triplane LA strain values similar to those of control subjects with atrial fibrillation, underscoring the severity of atrial mechanical dysfunction in amyloid cardiomyopathy. This finding may help explain the high prevalence of atrial fibrillation, atrial enlargement, thromboembolic events, and progressive heart failure in this population [18,19,20]. Although some post hoc pairwise comparisons did not reach statistical significance, the strong disease–rhythm interaction demonstrated by two-way ANOVA highlights the disproportionate adverse impact of atrial fibrillation on LA mechanics in amyloidosis compared with controls.
The regional heterogeneity observed on triplane LA strain maps may reflect patchy amyloid infiltration, fibrotic remodeling, and intra-atrial mechanical dispersion—features that constitute established substrates for atrial arrhythmias and intracavitary thrombus formation (Figure 2).
4.3. Clinical and Diagnostic Implications
From a clinical perspective, our findings suggest that triplane LA strain may serve as an additional imaging biomarker for assessing the burden of atrial involvement in cardiac amyloidosis. While echocardiographic evaluation has traditionally focused on left ventricular wall thickness and strain, atrial strain provides complementary information regarding atrial remodeling, mechanical dysfunction, and potential arrhythmic and thromboembolic risk.
Incorporating triplane LA strain into the diagnostic work-up of cardiac amyloidosis may improve sensitivity for detecting early atrial involvement, particularly in patients who remain in sinus rhythm and do not yet exhibit overt atrial enlargement. In the present cohort, triplane LA reservoir strain values below approximately 8% were predominantly observed in amyloidosis patients, whereas values exceeding 15–20% were typical of control subjects in sinus rhythm. These thresholds should be considered exploratory and require validation in larger prospective studies.
Although biplane LA strain reduction in amyloidosis has been consistently reported, the principal contribution of the present study lies in demonstrating the utility of triplane LA strain for visualizing regional heterogeneity of atrial mechanics. By integrating deformation data from three orthogonal apical views, the triplane approach provides an intuitive representation of atrial mechanical dispersion and patchy dysfunction that may be less apparent with conventional mono- or biplane techniques.
4.4. Reproducibility and Feasibility
An important strength of this study is the excellent reproducibility of triplane LA strain measurements. Both inter- and intra-observer analyses demonstrated high intraclass correlation coefficients, low coefficients of variation, and narrow Bland–Altman limits of agreement, indicating robust measurement reliability. Importantly, reproducibility was maintained in both sinus rhythm and atrial fibrillation, supporting the feasibility of triplane LA strain assessment across different rhythm states. These findings are consistent with prior reproducibility studies of LA strain [12,21] and support the potential applicability of triplane LA strain in clinical practice, longitudinal follow-up, and multicenter research settings.
4.5. Strengths and Limitations
The strengths of our study include the use of a carefully matched control group (age, sex, rhythm, and ejection fraction) and the application of a triplane imaging approach that enables comprehensive atrial assessment with both quantitative and qualitative components.
Several limitations should be acknowledged. First, this was a single-center, cross-sectional observational study, precluding causal inference and outcome assessment. Second, although rhythm matching was performed, subgroup sizes were modest. Third, clinical outcomes such as incident atrial fibrillation, thromboembolic events, and mortality were not evaluated. Given the small number of patients with light-chain amyloidosis, meaningful subgroup analyses by amyloid subtype were not feasible. Finally, evaluation of the independent effects of medical therapy or biomarker levels on triplane LA strain was beyond the scope of this study.
4.6. Future Directions
Future studies should investigate the prognostic value of triplane LA strain in larger prospective cohorts, including endpoints such as atrial fibrillation onset, thromboembolic events, heart failure hospitalization, and mortality. Comparative analyses of mono-, bi-, and triplane LA strain may further clarify the incremental value of each technique. Integration of atrial functional imaging with structural modalities such as cardiac MRI or PET may provide additional mechanistic insight. Longitudinal assessment of triplane LA strain during disease-modifying therapy (e.g., tafamidis) may also help determine whether atrial mechanical dysfunction is reversible and clinically meaningful [22,23,24,25].
5. Conclusions
In conclusion, triplane LA reservoir strain is profoundly reduced in patients with cardiac amyloidosis even in sinus rhythm, reaching values comparable to those observed in control subjects with atrial fibrillation—findings consistent with severe atrial cardiomyopathy. The ability of triplane imaging to visualize regional atrial mechanical heterogeneity offers additional pathophysiologic insight and may enhance risk stratification in cardiac amyloidosis. Further studies are warranted to define its prognostic and therapeutic implications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shinzato K. Takahashi Y. Yamaguchi T. Otsubo T. Nakashima K. Yoshioka G. Yokoi K. Tsuruta K. Osako R. Shichida S. Atrial amyloidosis identified by biopsy in atrial fibrillation: Prevalence and clinical presentation Eur. Heart J.2025463437344910.1093/eurheartj/ehaf 33240392565 PMC 12448450 · doi ↗ · pubmed ↗
- 2Vergaro G. Aimo A. Rapezzi C. Castiglione V. Fabiani I. Pucci A. Buda G. Passino C. Lupón J. Bayes-Genis A. Atrial amyloidosis: Mechanisms and clinical manifestations Eur. J. Heart Fail.2022242019202810.1002/ejhf.265035920110 PMC 10087817 · doi ↗ · pubmed ↗
- 3Bandera F. Martone R. Chacko L. Ganesananthan S. Gilbertson J.A. Ponticos M. Lane T. Martinez-Naharro A. Whelan C. Quarta C. Clinical Importance of Left Atrial Infiltration in Cardiac Transthyretin Amyloidosis JACC Cardiovasc. Imaging 202215172910.1016/j.jcmg.2021.06.02234419399 PMC 8724534 · doi ↗ · pubmed ↗
- 4Nochioka K. Quarta C.C. Claggett B. Roca G.Q. Rapezzi C. Falk R.H. Solomon S.D. Left atrial structure and function in cardiac amyloidosis Eur. Heart J. Cardiovasc. Imaging 2017181128113710.1093/ehjci/jex 09728637305 · doi ↗ · pubmed ↗
- 5Rapezzi C. Pavasini R. Serenelli M. The left atrium in cardiac amyloidosis: A valuable but still underused observation window on the overall disease process Eur. J. Heart Fail.2021231296129910.1002/ejhf.225734050585 PMC 8453979 · doi ↗ · pubmed ↗
- 6Aimo A. Fabiani I. Spini V. Chubuchny V. Pasanisi E.M. Petersen C. Poggianti E. Taddei C. Cameli M. Mandoli G.E. Left atrial strain in cardiac amyloidosis Eur. Heart J.202142 ehab 724.179410.1093/eurheartj/ehab 724.1794 · doi ↗
- 7Ferkh A. Geenty P. Stefani L. Emerson P. Pham J. Byth K. Boyd A.C. Richards D. Taylor M.S. Kwok F. Diagnostic and prognostic value of the left atrial myopathy evaluation in cardiac amyloidosis using echocardiography ESC Heart Fail.2024114139414710.1002/ehf 2.1501339129371 PMC 11631228 · doi ↗ · pubmed ↗
- 8Leitman M. Tyomkin V. Inhomogeneity of the Left Atrial Strain Medicina 20256194410.3390/medicina 6106094440572632 PMC 12195444 · doi ↗ · pubmed ↗