Diaphragmatic Ultrasound in Neonates with Transient Tachypnea: Comparison with Healthy Controls and Inter-Operator Reliability
Maria Letizia Patti, Carmela Crapanzano, Rosa Maria Cerbo, Federico Schena, Anna La Rocca, Valeria Cortesi, Giacomo Simeone Amelio, Stefano Ghirardello

TL;DR
This study shows that diaphragmatic ultrasound can detect early functional issues in newborns with transient tachypnea, helping to assess disease severity and guide treatment.
Contribution
The study introduces the use of diaphragmatic ultrasound in combination with lung ultrasound to monitor neonates with transient tachypnea.
Findings
Diaphragmatic excursion increases in healthy neonates during the first 48 hours.
TTN infants show lower diaphragmatic excursion compared to controls on day two.
A negative correlation between diaphragmatic excursion and lung ultrasound score suggests impaired diaphragmatic function in TTN.
Abstract
What are the main findings? •Diaphragmatic excursion increases during the first 48 h in healthy neonates.•On day two, TTN infants show lower diaphragmatic excursion compared with controls, and a negative correlation develops between excursion and LUS, indicating impaired diaphragmatic function in the context of lung disease. Diaphragmatic excursion increases during the first 48 h in healthy neonates. On day two, TTN infants show lower diaphragmatic excursion compared with controls, and a negative correlation develops between excursion and LUS, indicating impaired diaphragmatic function in the context of lung disease. What are the implications of the main findings? •Diaphragmatic ultrasound may help identify early functional impairment in neonates with TTN, complementing lung ultrasound to characterize disease severity.•Integrated lung–diaphragm ultrasound assessment may support…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
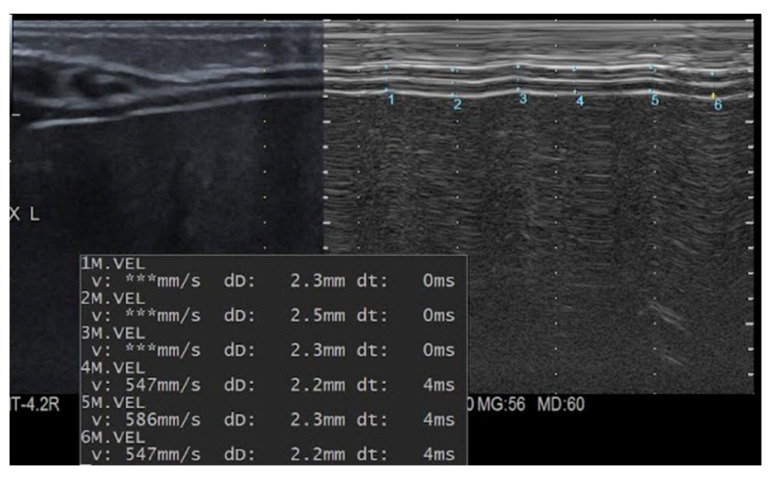 Figure 1
Figure 1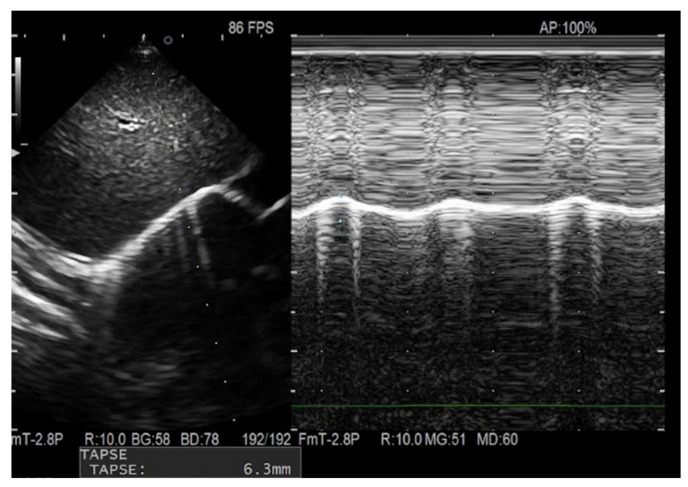 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Neonatal Respiratory Health Research · Congenital Diaphragmatic Hernia Studies
1. Introduction
Recent advances in neonatal imaging have emphasized the importance of diaphragmatic function in respiratory adaptation after birth. Ultrasound assessment of the diaphragm has become a promising, non-invasive method to evaluate diaphragmatic performance in neonates, allowing measurement of parameters such as diaphragmatic thickness, thickening fraction, excursion, and fractional shortening [1,2,3]. Studies in neonates needing mechanical ventilation have shown significant diaphragmatic atrophy and decreased thickening fractions during ventilation [4,5]. Transient tachypnea of the newborn (TTN) remains one of the most common causes of neonatal respiratory distress, especially in late preterm and term infants. It is mainly caused by delayed clearance of fetal lung fluid, leading to impaired gas exchange and increased work of breathing. Although TTN is usually self-limited, resolving within 24–72 h, it can still require respiratory support and may affect respiratory outcomes in early childhood [6,7]. The main goal of this study was to compare diaphragmatic functional parameters (end-inspiratory and end-expiratory thickness, thickening fraction, and diaphragmatic excursion) between neonates requiring non-invasive ventilation (NIV) and healthy term neonates. Additional objectives included assessing how these parameters vary with gestational age and birth weight, and evaluating the reproducibility of diaphragmatic ultrasound measurements.
2. Materials and Methods
This prospective observational pilot case–control study was conducted at the Neonatology and Neonatal Intensive Care Unit of IRCCS Policlinico San Matteo, Pavia, between February and July 2024. All inborn neonates with a gestational age of ≥34 weeks were considered eligible. Infants who developed respiratory distress after stabilization in the delivery room, requiring non-invasive respiratory support (nasal Continuous Positive Airway Pressure [nCPAP] or Heated Humidified High-Flow Nasal Cannula [HHHFNC]), and with a clinical and ultrasonographic diagnosis of transient tachypnea of the newborn (TTN), were included in the case group. An equal number of healthy neonates with gestational age ≥34 weeks, admitted to the Neonatology or Rooming-in unit, were selected as controls. Parental written informed consent was obtained before enrolment in both groups. Newborns with gestational age below 34 weeks, respiratory distress syndrome (RDS), hemodynamic instability, major congenital malformations, surgical conditions, or known metabolic/genetic syndromes were excluded. TTN was clinically defined as the presence of tachypnoea (respiratory rate > 60 breaths/min) and signs of respiratory distress (including thoracic and abdominal movement, intercostal and xiphoid retraction, nasal flaring, and expiratory grunt, Silverman score > 1) occurring within the first 24 h of life. The diagnosis of TTN was confirmed, as per usual clinical practice in our department, by lung ultrasound, showing a thickened pleural line, multiple B-lines alternating with A-lines, and the presence of the characteristic “double lung point” sign [8]. For both groups, the following clinical data were collected and recorded in a dedicated database: gestational age, gender, mode of delivery, maternal steroid prophylaxis, anthropometric parameters at birth (weight, length, head circumference), parity, Apgar scores at 1 and 5 min, and need for resuscitation at birth. For the TTN group, additional data were collected at each ultrasound assessment, including the mode and duration of non-invasive ventilation, Silverman score, and respiratory rate at the time of examination.
2.1. Ultrasound Equipment and Technique
Both diaphragmatic and lung ultrasound examinations were performed using a Hitachi Aloka Arietta V70™ (Hitachi Aloka Medical America, Inc. 10 Fairfield Boulevard, Wallingford, CT, USA) ultrasound system by two physicians with experience in pulmonary ultrasound, during routine clinical care. All images were reanalyzed for the purpose of the study by a senior neonatologist with expertise in LUS. Diaphragmatic ultrasound measurements included end-inspiratory and end-expiratory thickness (DTi and DTe, respectively), diaphragmatic thickening fraction (DTF), and diaphragmatic excursion (DE), while lung ultrasound was utilized to assess the Lung Ultrasound Score (LUS) [9].
In both groups, ultrasound evaluations were performed by either one of the two operators, at two different time points: T0 (within 6 h after birth) and T1 (second day of life, between 24 h and 36 h after birth), with the neonate in the supine position, during quiet sleep or calm wakefulness.
Diaphragmatic ultrasound was performed using a high-frequency linear transducer (15–8 MHz) positioned perpendicularly to the chest wall between the 8th and 10th intercostal spaces, along the right anterior to mid-axillary line. In B-mode, the diaphragm was identified as a hypoechoic structure bordered by two echogenic lines corresponding to the pleura (superiorly) and the peritoneum (inferiorly).
End-inspiratory and end-expiratory diaphragm thicknesses were measured in M-mode by calculating the maximal and minimal distance between the pleural and peritoneal layers (Figure 1). To ensure measurement accuracy and reproducibility, three measurements were obtained over three consecutive respiratory cycles, and the mean value was used for analysis.
The diaphragmatic thickening fraction (DTF) was calculated using the following formula:
Diaphragmatic excursion was assessed in M-mode using a low-frequency phased-array transducer (14–3 MHz) placed in the subcostal area between the right midclavicular and anterior axillary lines, with the confluence of the hepatic veins as an anatomical landmark. Excursion was measured as the distance between the baseline at end-expiration and the point of maximal inspiration (Figure 2).
Simultaneously, lung ultrasound was performed using a high-frequency linear transducer (15–8 MHz). The LUS score was assigned by evaluating six lung regions: upper anterior, lower anterior, and lateral regions on both sides of the chest. In detail, the LUS score was assigned as follows, according to Brat R. et al. [9]: 0 indicates an A-pattern, characterized by the exclusive presence of A-lines; 1 corresponds to a B-pattern, defined by the appearance of three or more well-separated B-lines; 2 refers to a severe B-pattern, in which B-lines are densely packed and merging, possibly accompanied by small subpleural consolidations; 3 is used when larger, more extensive consolidations are present. For each lung area, a 0- to 3-point score was given (total score ranging from 0–18).
2.2. Assessment of Reproducibility
To assess the reproducibility of the diaphragmatic ultrasound, measurements were independently carried out by two different operators (C.C. and A.L.R.) on a subgroup of 31 neonates (independently cases or controls), with a total of 62 scans and a 5-min gap between assessments.
2.3. Statistical Analysis
Statistical analysis was performed using DATAtab software (DATAtab e.U., Graz, Austria). The Shapiro–Wilk test was used to assess the normality of data distribution [10] (Supplementary Table S1). Variables with normal distribution (p > 0.05) were analyzed using parametric tests. Homogeneity of variances was assessed using Levene’s test [11]. When the assumption of equal variances was violated (p < 0.05), Welch’s correction was applied [12,13]. The independent-sample Student’s t-test was applied to compare continuous parametric variables between groups. In contrast, the paired-samples t-test was used to compare numerical variables within the same group. The Mann–Whitney U test was applied for non-parametric continuous variables. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Clinical and ultrasound data were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR), depending on distribution. Categorical variables were presented as absolute numbers and percentages. Pearson’s correlation coefficient was used for correlations between normally distributed variables, and Spearman’s rank correlation coefficient for non-normally distributed variables. A point-biserial correlation was used to assess the association between diaphragmatic excursion and the type of ventilation. A p-value < 0.05 was considered statistically significant. Given the pilot nature of the study and the limited number of predefined outcomes, no correction for multiple comparisons was applied, and effect size calculations were not included in the analysis plan. Inter-operator agreement was evaluated using Bland–Altman plots and the coefficient of variation (CV), while reliability was assessed with the intraclass correlation coefficient (ICC) from a two-way random-effects analysis of variance [14,15].
3. Results
Of the 65 neonates initially considered eligible, 44 were enrolled, and 40 of them (20 cases and 20 controls) completed the study protocol. Demographic and prenatal characteristics of the two groups are presented in Table 1.
Data analysis revealed no significant differences in diaphragmatic parameters between cases and controls on the first day of life (Table 2, T0). On the second day (Table 2, T1), diaphragmatic excursion was significantly greater in healthy neonates than in those with TTN (p = 0.03). Healthy newborns, unlike the TTN group, also exhibited a significant increase in diaphragmatic excursion from the first to the second day (p = 0.04) (Table 3). No correlation between diaphragmatic excursion measured on T1 and Silverman score, or type and duration of respiratory support, was found. Instead, a negative correlation between diaphragmatic excursion and LUS score was found at the threshold of statistical significance (r = −0.44; p = 0.05) (Supplement, Table S2).
Analysis of the entire cohort showed a significant correlation between diaphragmatic thicknesses, gestational age, and birth weight (p < 0.01) (Table 4). Bland–Altman plots showed low bias values (0.18 for end-inspiratory thickness, 0.15 for end-expiratory thickness, 0.3 for diaphragmatic excursion) and acceptable limits of agreement between ultrasound measurements performed by the two operators (95% CI: −1.19 to 0.83 for end-inspiratory thickness; −0.98 to 0.68 for end-expiratory thickness; −2.74 to 2.15 for diaphragmatic excursion) (Supplement Figures S1–S3). ICC showed good reliability for end-expiratory thickness (ICC = 0.66), moderate reliability for end-inspiratory thickness (ICC = 0.52), and discrete reliability for diaphragmatic excursion (ICC = 0.32) (Table 5).
4. Discussion
Diaphragmatic ultrasound has been widely used in adult and pediatric populations to assess diaphragmatic dysfunction in patients undergoing invasive mechanical ventilation, particularly in relation to the duration of ventilatory support and extubation outcomes [2]. However, studies evaluating diaphragmatic function in association with underlying lung disease remain limited, especially in neonates.
Our pilot study compared diaphragmatic parameters in healthy neonates and those with TTN requiring non-invasive ventilation during the first 48 h of life. Diaphragmatic thickness and excursion measured within the first 24 h were similar between groups, suggesting that early diaphragmatic function may not be significantly influenced by underlying pulmonary disease during the initial transition to extrauterine life.
However, diaphragmatic excursion was the only parameter that showed a significant increase from the first to the second day of life in healthy neonates. This progressive increase may be related to the gradual maturation of respiratory muscles over time. Furthermore, diaphragmatic excursion was significantly greater in healthy infants compared with those with TTN after the first 24 h of life, suggesting partial diaphragmatic impairment possibly related to reduced lung compliance due to respiratory disease.
This hypothesis is further supported by our finding of a negative correlation—at the threshold of statistical significance (p = 0.05)—between diaphragmatic excursion on the second day of life and the LUS score, indicating that lower excursion values are associated with higher LUS scores, which reflect increased interstitial fluid content.
In contrast, analysis of our data revealed no significant differences in diaphragmatic excursion based on the type or duration of non-invasive ventilation, likely due to the small sample size and short duration of non-invasive ventilation in our cohort, though consistent with the expected clinical course of TTN. Similarly, a recent study showed that diaphragmatic function parameters, including excursion, were not predictive of successful CPAP weaning, whereas the LUS score demonstrated good sensitivity and specificity for this purpose [16]. Moreover, El-Mogy et al. reported no significant differences in diaphragmatic parameters between infants receiving nCPAP and those on HHHFNC [17]. Conversely, Gupta et al. found that in preterm neonates, diaphragmatic excursion decreased, and thickening fraction increased, among infants who failed nCPAP transition [18].
Consistent with existing literature, diaphragmatic thickness increased proportionally with gestational age and birth weight, while this was not observed for thickening fraction or diaphragmatic excursion. Rehan et al. examined diaphragmatic ultrasound parameters in 34 preterm infants and demonstrated that diaphragmatic thickness was directly proportional to anthropometric measures (birth weight, length, and head circumference) and post-conceptional age, while diaphragmatic excursion decreased with advancing post-conceptional age due to reduced chest wall compliance [19]. Similar findings were reported in a recent study of 107 preterm neonates [20]. Likewise, El-Halaby et al. observed a positive correlation between diaphragmatic thickness and excursion and anthropometric parameters in a pediatric population aged one month to two years [3]. Our findings align with these results, demonstrating a positive correlation between gestational age, birth weight, and diaphragmatic thickness. Previous studies in neonatal [3], pediatric [21], and adult [22] populations have also shown that diaphragmatic excursion tends to increase with body weight. However, in our cohort, this relationship did not reach statistical significance.
A study involving 66 healthy neonates (33 term and 33 preterm) reported that term infants exhibited greater diaphragmatic thickness compared with preterm infants, while thickening fraction was similar between groups [23].
In line with previous studies, in our cohort, the thickening fraction did not vary with gestational age. This parameter, which reflects diaphragmatic contractility, tended to be higher in neonates with TTN compared with controls on both days of life, although the difference was not statistically significant. This trend may reflect increased respiratory effort in infants with respiratory disease, as previously described in neonates with bronchopulmonary dysplasia (BPD) [24] or may be related to altered chest wall compliance and/or increased lung stiffness associated with TTN. In adults with chronic obstructive pulmonary disease (COPD), a similar diaphragmatic excursion reduction has also been reported [25,26]. However, none of these studies involve newborns.
Assessment of inter-operator agreement demonstrated good reliability for diaphragmatic thickness measurements, despite their millimetric precision. Discrete reliability was observed for diaphragmatic excursion. Inter-operator variability for this measurement may depend on the infant’s condition at the time of examination, as excursion is influenced by respiratory rate and comfort state. Overall, our results are consistent with previous pediatric and adult studies evaluating the reproducibility of this technique [22].
We are aware that the differences in diaphragmatic thickness and diaphragmatic excursion between the two groups are minimal. However, our study highlights the potential role of diaphragmatic activity during perinatal respiratory transition and how reduced lung compliance, due to an underlying disease (such as transient tachypnea in our cohort), may affect diaphragmatic function. A study with an ad hoc design (for example, with an initial assessment of diaphragmatic excursion a few hours after birth) and a larger population would be required to confirm our findings. Moreover, as our study population included only term and late preterm infants, diaphragmatic function in other pulmonary conditions, such as respiratory distress syndrome, could not be evaluated, as these are more prevalent in infants of lower gestational age.
5. Conclusions
Respiratory disease may negatively affect diaphragmatic function after neonatal adaptation. In healthy neonates, diaphragmatic function, particularly excursion, improves over the first hours of life, whereas this increase does not occur in infants with TTN. Diaphragmatic ultrasound is a non-invasive, bedside-applicable, and radiation-free tool that, combined with lung ultrasound, provides clinically relevant information in neonates with respiratory distress. Integrated assessment may help monitor lung disease progression and guide respiratory support weaning. Further studies are needed to improve interpretation and support routine use in neonatal intensive care units.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alonso-Ojembarrena A. Estepa-Pedregosa L. Can Diaphragmatic Ultrasound Become a New Application for Point-of-Care Ultrasound in Preterm Infants?Chest 202316326626710.1016/j.chest.2022.09.01136759111 · doi ↗ · pubmed ↗
- 2Weber M.D. Lim J.K.B. Glau C. A narrative review of diaphragmatic ultrasound in pediatric critical care Pediatr. Pulmonol.2021562471248310.1002/ppul.2551834081825 · doi ↗ · pubmed ↗
- 3El-Halaby H. Abdel-Hady H. Sonographic Evaluation of Diaphragmatic Excursion and Thickness in Healthy Infants and Children J. Ultrasound Med.20163516717510.7863/ultra.15.0108226679203 · doi ↗ · pubmed ↗
- 4Hoshino Y. Arai J. Ventilator-induced diaphragmatic dysfunction in extremely preterm infants: A pilot ultrasound study Eur. J. Pediatr.20231821555155910.1007/s 00431-023-04846-z 36719478 · doi ↗ · pubmed ↗
- 5Nobile S. Sbordone A. Diaphragm atrophy during invasive mechanical ventilation is related to extubation failure in preterm infants: An ultrasound study Pediatr. Pulmonol.20245985586210.1002/ppul.2681838353403 · doi ↗ · pubmed ↗
- 6Alhassen Z. Vali P. Recent Advances in Pathophysiology and Management of Transient Tachypnea of Newborn J. Perinatol.20214161610.1038/s 41372-020-0757-332753712 PMC 11867197 · doi ↗ · pubmed ↗
- 7Neri C. Sartorius V. Transient tachypnoea: New concepts on the commonest neonatal respiratory disorder Eur. Respir. Rev.20253424011210.1183/16000617.0112-202439909500 PMC 11795285 · doi ↗ · pubmed ↗
- 8Copetti R. Cattarossi L. The ‘double lung point’: An ultrasound sign diagnostic of transient tachypnea of the newborn Neonatology 20079120320910.1159/00009745417377407 · doi ↗ · pubmed ↗