Shaken Adult Syndrome: Defining a New Traumatic Entity with an Evidence-Based Approach
Fabio Del Duca, Gianpietro Volonnino, Biancamaria Treves, Alessandra De Matteis, Nicola Di Fazio, Raffaele La Russa, Paola Frati, Aniello Maiese

TL;DR
This paper introduces Shaken Adult Syndrome, a new traumatic condition defined by specific injuries from rapid flexion-extension movements in adults.
Contribution
The paper proposes a diagnostic framework for Shaken Adult Syndrome using a validated diagnostic triad and a flowchart for clinical and forensic use.
Findings
The diagnostic triad for Shaken Adult Syndrome includes subdural hemorrhages, retinal hemorrhages, and encephalopathy.
A diagnostic flowchart is proposed to identify SAS in both live patients and post-mortem cases.
Microscopic brain and ocular examinations using immunomarkers can confirm SAS pathognomonic features.
Abstract
Major traumas result from the application of multiple force components that, in adulthood, can lead to high mortality and morbidity. In forensic practice, pathological consequences arising from the rapid flexion–extension of an adult victim’s soma are observed, with typical intracranial and ophthalmological findings. The totality of these findings allows for a contribution to the definition of the Shaken Adult Syndrome (SAS). A comprehensive review, employing the PRISMA methodology, was conducted on international works pertaining to SAS. This resulted in the identification of six scientific papers, which were analyzed separately. It emerged that, for the diagnosis of SAS, the same diagnostic triad as Shaken Baby Syndrome is valid, comprising subdural hemorrhages, retinal hemorrhages, and encephalopathy. This syndrome appears to encompass a broad spectrum of pathological conditions,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
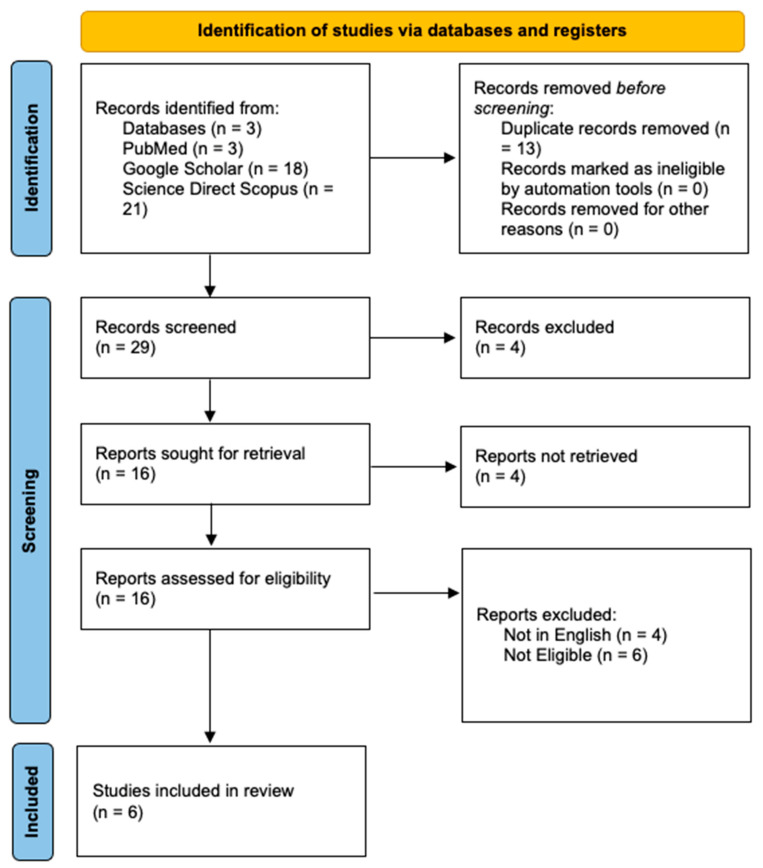 Figure 1
Figure 1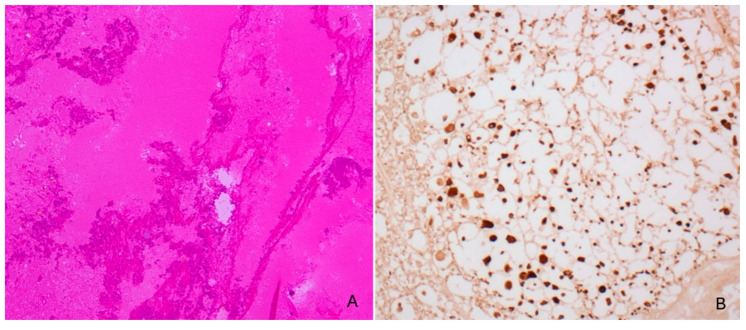 Figure 2
Figure 2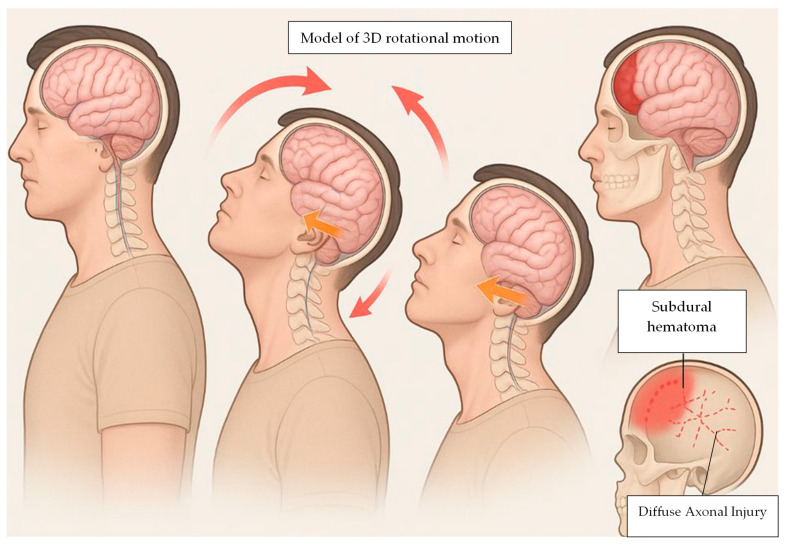 Figure 3
Figure 3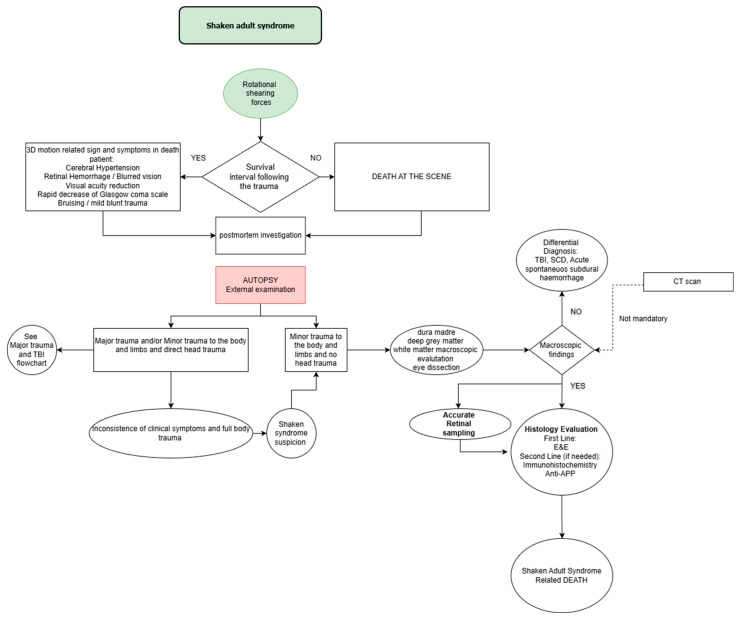 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Abuse and Related Trauma · Traumatic Ocular and Foreign Body Injuries · Trauma and Emergency Care Studies
1. Introduction
Shaken Adult Syndrome (SAS), known as inflicted head injury by shaken trauma (IHI-ST), represents a severe form of non-accidental traumatic brain injury, resulting from the transmission of mechanical forces, frequently external, to the body of an adult victim. This condition typically arises when an individual is subjected to violent shaking, producing a constellation of neurological injuries reminiscent of those observed in infants, such as subdural hematomas and retinal hemorrhages [1].
The underlying biomechanical mechanisms involve rapid acceleration–deceleration forces, capable of inflicting significant cerebral trauma. Despite anatomical and physiological differences between adults and infants, the hypothesis is that adults remain susceptible to serious injury through similar violent mechanisms [2,3].
Evidence from clinical literature indicates that the presentation of shaking-related injuries in adults may parallel that seen in pediatric cases [4,5,6,7]. Neurological signs such as confusion, hemiplegia, and diplopia may be present, though they may be misattributed to other etiologies. As a result, SAS in adults might be underdiagnosed, leading to an underappreciation of the broader implications of interpersonal and domestic violence.
In geriatric populations, particularly among frail individuals with multiple comorbidities, intracranial hemorrhages and parenchymal injuries due to shaken forces may occur in the absence of overt external trauma [8,9,10,11], complicating forensic recognition and clinical assessment [12].
Beyond the immediate physical injuries, long-term pathological consequences may include cognitive decline, psychological trauma, and persistent neurological deficits [13,14,15,16,17,18]. Research underscores that, similar to the pediatric population, the structural and functional vulnerabilities of the adult brain can result in profound internal damage when exposed to high-velocity shaking [19,20,21,22,23,24].
Although episodes of adult shaking may occur in a variety of settings, the social and preventive implications mirror those associated with Shaken Baby Syndrome [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. Educational initiatives aimed at increasing public and professional awareness of the dangers of violent shaking and at promoting non-violent conflict resolution have been advocated as essential measures to reduce the incidence of such trauma. This includes informing both potential victims and perpetrators about the risks and long-term consequences of violent behavior [41]. Despite the clinical symptoms being clearly depicted in the current literature, autopsy findings are less well-known by the scientific community. In fact, the literature on Shaken Adult Syndrome is almost exclusively composed of case series. There is a need for a work to collect and synthesize the evidence from the individual contributions in the literature.
To date, the pathophysiological mechanism of shaking in infants, which results in a syndrome known as shaken baby syndrome, is well established. This condition is often associated with episodes of child abuse; for this reason, shaken baby syndrome has been the subject of numerous studies in the literature, and diagnostic pathways have been developed to enable its early identification. Similar shaking of the head can produce, through the same pathogenic mechanism, a comparable clinical picture in adults; however, this entity has not yet been investigated to the same extent in the literature, despite its relevance.
In conclusion, while Shaken Adult Syndrome shares key pathological features with its pediatric counterpart, awareness and recognition remain critically insufficient. Greater clinical vigilance, improved identification protocols, and a societal shift toward prevention through education and support are essential to addressing this under-recognized form of domestic violence and safeguarding vulnerable populations. The aim of the study is to provide a comprehensive overview of the forensic diagnostic challenges in shaken-related trauma, focusing on the key clinical, radiological, and pathological findings, the main differential diagnoses, and the medico-legal implications for accurate case assessment.
2. Materials and Methods
A comprehensive review of the updated literature was carried out according to the Preferred Reporting Items for comprehensive Review (PRISMA) standards [42], as previously reported in previous studies [43,44,45,46,47]. The review protocol was developed a priori to ensure transparency and reproducibility, and all methodological steps were performed in compliance with PRISMA standards.
Although the protocol was not registered in PROSPERO, the methodological framework strictly followed the PRISMA 2020 checklist and flow diagram, ensuring standardized reporting of identification, screening, eligibility, and inclusion stages.
Eligible studies were selected according to the following inclusion criteria:
- -Articles published in peer-reviewed journals between January 1990 and September 2025;
- -Studies written in English;
- -Studies involving adult human subjects (≥18 years) diagnosed with Shaken Adult Syndrome or adult shaken head trauma;
- -Articles presenting original data (case reports, case series, or observational studies).
Exclusion criteria included:
- -Non-human studies, pediatric populations, reviews, conference abstracts, editorials, and non-English papers;
- -Studies lacking diagnostic, histopathological, or imaging evidence consistent with shaking mechanisms
Three electronic databases were systematically searched: PubMed, Scopus (ScienceDirect), and Google Scholar. The last search was conducted in September 2025. Reference lists of included articles were also manually screened to identify additional relevant studies. The following Boolean search string was used across all databases: (“Shaken Adult Syndrome” OR “Adult Shaken Head Trauma” OR “Shaking Syndrome” OR “Whiplash”) AND (“adult” OR “elder”) AND (“autopsy” OR “post-mortem” OR “postmortem”).
Searches were performed in all fields (title, abstract, and keywords). The results were exported in nbib format and managed using Zotero 6.0.30 for reference organization and deduplication.
Two independent reviewers (F.D.D. and N.D.F.) screened titles and abstracts for eligibility. Full texts of potentially relevant articles were then retrieved and assessed according to the inclusion and exclusion criteria. Disagreements were resolved by consensus or by a third reviewer (G.V.). No article from backward snowballing was retrieved. The selection process is detailed in the PRISMA 2020 flow diagram (Figure 1).
Data were extracted from each included study using a standardized data collection form. Extracted variables included: year and country of publication, study design, patient demographics (age, sex), clinical history, cause and mechanism of trauma, neuroimaging findings, autopsy results, histological and immunohistochemical findings (particularly β-amyloid precursor protein expression), and ocular findings.
Given the qualitative nature of the included studies (mainly case reports and case series), a formal risk-of-bias assessment was not applicable. Nevertheless, methodological quality and internal validity were appraised through careful evaluation of diagnostic consistency, data completeness, and concordance with established neuropathological criteria for traumatic brain injury.
The extracted data were synthesized descriptively. The results were summarized in tables highlighting demographic characteristics, clinical presentation, imaging features, and histopathological findings. A narrative synthesis was then performed to integrate findings and identify recurring diagnostic patterns across studies.
Risk of Bias
This systematic review targets articles published within the last thirty five years, employing specific research methods utilizing a select few keywords.
Given the qualitative nature of the included studies, which consist primarily of case reports and case series, a formal risk-of-bias assessment using traditional tools designed for randomized trials (e.g., RoB 2) was not applicable. Key study limitations include the absence of prospective protocol registration (e.g., in PROSPERO), which should not be applied because this paper is not a systematic review. Additionally, while the review timeframe was consistently defined as January 1990 to September 2025 to encompass foundational and recent literature, this broad span may introduce heterogeneity in diagnostic practices over time. These factors collectively rate the overall certainty of evidence, highlighting the need for higher-quality observational studies to validate SAS diagnostic criteria
3. Results
After the complete database screening, a total of seven cases were retrieved from case reports and case series. All of them regards adult, and only in one case was an old man involved (>65 years old). Mean age was 53.2 years old ± SD 18.89 (s^2^ = 357.2, IQR = 34, IQ_1–3_ = 37–71), which shows no age prevalence (Table 1).
Table 2 shows the different clinical presentations of shaken syndrome in adults, all caused by a single underlying mechanism. In every case, the head was subjected to rapid acceleration–deceleration forces, either indirectly by shaking the shoulders or body (indirect shaking syndrome), or directly by shaking the head itself. Only one individual survived the assault, while six out of seven cases resulted in rapid death (See Table 3).
Descriptive Review of the Study’s Methodology
In the study by Carrigan et al. [1], a case is described involving a 34-year-old woman who presented to the emergency department claiming she had fallen down the stairs. Upon arrival, she exhibited the triad of subdural hematoma, retinal hemorrhages, and fingertip-shaped bruising. The woman had also ingested alcohol. Only after 48 h and following repeated questioning did she admit that she had, in fact, been the victim of domestic violence rather than a simple fall. At admission, her Glasgow Coma Scale score was 13/15 due to a confused mental state, but it rose to 15/15 within the following 24 h. She experienced post-concussion symptoms for around two weeks, reported episodes of vomiting, and complained of persistent blurred vision. Her visual acuity was reduced to hand movements in the right eye and finger counting in the left. Clinical examination revealed fingertip bruising over her back, buttocks, and arms, as well as scalp hematoma, a frontal abrasion, periorbital bruising, and epistaxis. Although radiographic skull and facial bone examinations were unremarkable, CT imaging revealed a small left temporal subdural hemorrhage with associated edema. Ophthalmological evaluation demonstrated bilateral retinal and preretinal hemorrhages along with macular bleeding.
The case reported by Jennian F. Geddes [48] involves a Palestinian man who died after three days of interrogation and assault by Shin Bet officers. External examination revealed bruising over the anterior thorax bilaterally, while the face, neck, and scalp showed no external trauma. Upon craniotomy, cerebral edema and subdural hemorrhage were identified. Microscopic brain analysis showed edema, subdural bleeding, and diffuse axonal injury (DAI), confirmed via amyloid precursor protein (APP) immunohistochemistry. Histological slides described “shrinkage beads of nerve fibers”, particularly within the corpus callosum. Microscopic eye examination revealed retinal hemorrhage.
Amir A. Azari [49] presented two reports. The first was of a man in his fifties found dead after an assault in which, according to an eyewitness, he was grabbed from behind and shaken back and forth three to four times. External examination revealed no head trauma. Craniotomy revealed a unilateral right subdural hemorrhage and cerebral edema without signs of herniation. Blood toxicology showed alcohol. Standard histology confirmed subdural bleeding. Immunohistochemical staining for APP showed bilateral positivity within the centrum semiovale and dorsal midbrain white matter. Ocular microscopy demonstrated retinal hemorrhages, vitreous hemorrhage, macular folds, extraocular muscle hemorrhages, and pathological alterations of the optic nerve, including edema and subdural/subarachnoid hemorrhage of the nerve sheath.
The second case described a man in his sixties found unconscious at home; two friends attempted resuscitation by repeatedly shaking him. External examination showed various bruises on the chest and lower limbs, likely self-inflicted, with no cranial injuries or fractures. Craniotomy revealed bilateral subdural hemorrhage, cerebral edema, Duret midbrain hemorrhages, and transtentorial herniation. Microscopy confirmed subdural and focal subarachnoid hemorrhages with areas of tissue necrosis. APP staining showed nonspecific positivity. Toxicology showed alcohol. Ocular microscopy showed retinal hemorrhages, vitreous hemorrhage, macular folds, and hemorrhages of the extraocular muscles and optic nerve sheath.
Kenji Ninomiya [51] reported an apparent drowning case involving a ~40-year-old man swept away while fishing on a rocky shore. His body was recovered adrift hours later. Postmortem CT showed subarachnoid hemorrhage (SAH). External examination revealed no head injuries. Lungs were overinflated, weighing 820 g and 1040 g, with massive frothing in airways and pleural effusion of 60 mL left and 100 mL right. Craniotomy showed brain edema and SAH within the interhemispheric fissure and parieto-occipital convexity, as well as small caudate nucleus hemorrhages. Conventional microscopy showed multiple mesencephalic foci; APP staining was negative. Toxicology was negative. The traumatic midline SAH and DAI indicated rotational shearing forces from the whirlpools rather than direct impact with rocks.
Zhengdong Li et al. [50] described a detainee shaken over 20 times within 12 h by fellow prisoners, captured on CCTV (Figure 2). He developed gait instability and entered a coma before CT revealed cerebral edema, midline shift, and left temporal subdural hemorrhage. Decompressive craniectomy and hematoma evacuation were performed, but he died ten days later. Autopsy confirmed cerebral edema, subdural bleeding, and DAI via APP immunostaining.
Bugelli et al. [12] reported an 82-year-old woman found unresponsive at home with a GCS of 3. CT revealed right parieto-temporal and left parieto-occipital subdural hemorrhages with midline shift, superimposed on chronic ischemic encephalopathy. No thoracic or abdominal injuries were present. She died after four days. External examination showed multiple bruises on upper and lower limbs compatible with forceful grabbing or repeated blows, as well as bruises on the chest, face, head, and neck, with minimal or absent cranial contusions. Craniotomy showed bilateral subdural hemorrhages. Microscopy dated these to 5–7 days due to granulation tissue, erythrocyte breakdown, siderophages, fibroblast infiltration, and capillary neovascularization. Severe edema with large pericellular and perivascular spaces was also observed. Toxicology was negative for alcohol or drugs.
4. Discussion
Based on the available literature, Shaken Adult Syndrome can be identified in both living patients and deceased individuals. It is necessary to define the diagnostic steps required to reach an accurate diagnosis of this syndrome while excluding alternative forensic diagnoses.
In all case studies, where a patient or deceased individual presents with suspicious injuries, it is imperative to conduct a thorough investigation of the medical history and/or circumstantial data to exclude an episode of violence [1,52].
Although during the initial assessment the patient may deny experiencing violence, it is essential to re-evaluate the patient’s history in the subsequent days, as they may later disclose the violence suffered. This aspect is crucial, as it may lead the patient to file a complaint or seek legal or social assistance [53].
Furthermore, in many countries, including several US states and Italy, physicians are legally required to report injuries resulting from assault in any patient presenting to the emergency department. This creates an ethical and legal dilemma for emergency physicians, who are obliged to report suspected domestic violence even in the absence of explicit patient disclosure, which may only occur after several days. Unfortunately, victims of domestic violence are often discharged the same day, resulting in the loss of an important diagnostic window for Shaken Adult Syndrome [54].
Physical, cerebral, and ocular injuries can worsen over time and may be fatal; therefore, a structured emergency-department follow-up can support a more accurate investigation and help uncover violence, preventing further episodes as in pediatric protocols. In deceased cases without a history, scene investigation, circumstantial review, and witness interviews are essential. Typical findings include bruises (sometimes with fingertip marks) and abrasions, and subdural hematomas without external head contusions, suggesting shaking-related acceleration–deceleration and rotational forces rather than direct impact [55].
Neuroimaging, specifically brain CT scans, whether conducted ante-mortem or post-mortem, typically reveals unilateral or bilateral subarachnoid hemorrhages, predominantly located in the temporo-parietal regions. These are often associated with a midline shift secondary to increased intracranial pressure [51].
All autopsy examinations generally revealed characteristic findings, particularly at the cerebral level, such as unilateral or bilateral subdural hemorrhages, often associated with cerebral edema. Additional findings may include small subarachnoid hemorrhages, focal tissue necrosis, and signs of brain herniation.
However, in certain cases, pathological alterations may also involve other organs. For example, in the case report by Kenji Ninomiya [51], the decedent suffered injuries not only from head shaking but also from an asphyxial mechanism due to drowning. The lungs were markedly overinflated, weighing 820 g and 1040 g, respectively, with massive froth present in the upper and lower airways. Pleural effusions of 60 mL (left) and 100 mL (right) were also observed. In such instances, it is crucial to establish the predominant mechanism responsible for death.
The next diagnostic step involves microscopic examination of the brain and ocular structures. Brain histology confirms macroscopic findings of subdural hemorrhage and edema, and enables assessment of diffuse axonal injury (DAI) through sampling of multiple brain regions. Conventional staining techniques reveal “shrinkage beads” of nerve fibers within the white matter. Immunohistochemistry for amyloid precursor protein (APP) is typically positive, confirming axonal damage [56,57].
Microscopic examination of ocular tissues demonstrates retinal hemorrhages and macular folds. Retinal hemorrhages [1] are generally bilateral, symmetrical, and may be intraretinal, preretinal, or subretinal. The most affected regions are those with maximum vitreoretinal adhesion, including the ora serrata, posterior pole, and perivascular areas.
Additionally, the optic nerve is frequently involved, with findings such as papilledema and subdural or subarachnoid hemorrhages. The extraocular muscles are often affected as well, frequently presenting with hemorrhages [49].
A crucial differential diagnosis is Terson Syndrome [58], which is defined as a vitreous hemorrhage associated with subarachnoid hemorrhage. However, its current clinical application encompasses any coexistence of intraocular and intracranial hemorrhage. In contrast, Shaken Adult Syndrome is characterized by the additional presence of hemorrhages within the extraocular muscles, sclera/episclera, and retina at the ora serrata, as well as macular folds and retinal hemorrhages—findings absent in Terson Syndrome.
Reported cases are heterogeneous but share a common acceleration–deceleration mechanism, namely shaking. This mechanism is responsible for the development of cerebral edema and subdural hemorrhage, leading to increased intracranial pressure and subsequent brain herniation.
A critical aspect of this pathophysiology is the frequent absence of direct cranial trauma. Shaking does not depend on impact with an external object. Indeed, the main hypothesis is that it alone generates the forces necessary to cause subdural hemorrhage. The shaking may be performed by gripping either the shoulders or the head directly.
When describing the pathogenetic mechanism, the predominant feature is rapid flexion–extension and rotational movement of the head, while the torso remains relatively stationary (Figure 3). In some cases, the torso acts as a pivot, whereas in others the head is shaken directly [59].
This mechanism can result from another individual’s mechanical action or from natural forces, such as wave motion, as described in the aforementioned case report. Identified risk factors include alcohol ingestion and significant physical differences between the victim and aggressor in terms of height, age, or muscular strength.
These forces produce diffuse axonal injury in the white matter and hemorrhages within midline brain structures.
It is important to emphasize that all the literature sources considered in this article showed overall agreement both on the macroscopic and microscopic autopsy findings and on the shaking mechanism that produces such injuries, which appears to be pathognomonic of Shaken Adult Syndrome.
In conclusion, a diagnostic proposal is needed to facilitate the early and accurate diagnosis of Shaken Adult Syndrome in both living patients and post-mortem examinations.
5. Conclusions
The diagnosis of Shaken Adult Syndrome (SAS) represents a still little-known yet distinct and clinically significant condition, characterized by the triad of subdural hemorrhage, retinal hemorrhages, and optic nerve sheath hemorrhages. Those findings are often associated with diffuse axonal injury (DAI). The triad described above is, however, too often underestimated. In adult individuals, this type of lesion may occur in various contexts—such as domestic violence, physical assault, or sudden accidental movements—and can develop even in the absence of any clear cranial trauma. In this study, we propose a diagnostic flowchart aimed at guiding both clinicians and forensic pathologists towards the recognition of a syndrome that is at once subtle and severe. Starting with the assessment of an individual exposed to rotational forces to the head, it is necessary to investigate possible pre-mortem symptoms. Regardless of whether the person survives, a proper external examination must be carried out to exclude major external trauma. Subsequently, an appropriate autopsy examination (see Figure 4) and histological confirmation are necessary to arrive at a diagnosis of Shaken Adult Syndrome.
A multidisciplinary clinical and medico-legal approach will therefore be necessary. To this end, a thorough examination of the brain is essential, involving a cranial CT scan in the living patient to detect subdural hemorrhages or signs of cerebral edema, followed by macroscopic and microscopic examination with immunohistochemical analysis in the deceased, in order to highlight diffuse axonal injuries and vascular damage consistent with shaking mechanisms. At the same time, examination of the retinal structures is mandatory. This can be performed through a fundus oculi examination in living patients or by microscopic evaluation of the retina, optic nerve, and extraocular muscles in the cadaver. Retinal and optic nerve sheath hemorrhages, particularly when bilateral and symmetrical, represent highly suggestive findings of SAS and may serve as discriminating elements in differential diagnosis, especially in distinguishing SAS from Terson’s syndrome. For these reasons, and with a view to future developments, it would be necessary to implement ocular diagnostic tools comparable in diagnostic value to immunohistochemical staining techniques used for cerebral analysis. The recognition of SAS has significant clinical, forensic, and legal implications. Identifying the underlying traumatic mechanism through a rigorous diagnostic process carries considerable social importance, as it enables the protection of vulnerable individuals who are victims of violence. For this reason, future research should promote interdisciplinary collaboration among clinicians, neurologists, ophthalmologists, radiologists, forensic pathologists, and biomechanical engineers. Specifically, in the future, it would be advisable to collect additional data and to disseminate a diagnostic algorithm that enables proper diagnostic and therapeutic management of the syndrome. The consolidation of Shaken Adult Syndrome within the pathophysiological framework of traumatic brain injuries will contribute to preventing further episodes of abuse and to strengthening both diagnostic awareness and medico-legal protection [18,19].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Carrigan T.D. Domestic Violence: The Shaken Adult Syndrome Emerg. Med. J.20001713813910.1136/emj.17.2.138PMC 172533010718242 · doi ↗ · pubmed ↗
- 2BauerováA. NoskováP. Bláha J. Shaken Adult Syndrome or a Neurological Complication of Epidural Anesthesia?Anest. Intenziv. Med.202132525410.36290/aim.2021.002 · doi ↗
- 3Chia J.K.K. Goh K.Y.C. Chan C. An Unusual Case of Traumatic Intracranial Hemorrhage Caused by Wakeboarding Pediatr. Neurosurg.20003229129410.1159/00002895710971190 · doi ↗ · pubmed ↗
- 4Arneitz C. Schmitz J. Szilagyi I. Kienesberger B. Schalamon G. Senica S.O. Schalamon J. Abusive Head Trauma and Crying Infant-Public Awareness of Newborn and Infant Trauma Acta Paediatr.20241131569157810.1111/apa.1724338634613 · doi ↗ · pubmed ↗
- 5Feld K. Feld D. Karger B. Helmus J. Schwimmer-Okike N. Pfeiffer H. Banaschak S. Wittschieber D. Abusive Head Trauma in Court: A Multi-Center Study on Criminal Proceedings in Germany Int. J. Leg. Med.202113523524410.1007/s 00414-020-02435-533030617 PMC 7782463 · doi ↗ · pubmed ↗
- 6Goethals L. Prokofieva Nelson V. Fenouillet F. Chevreul K. Bergerat M. Lebreton C. Refes Y. Blangis F. Chalumeau M. Le Roux E. Characteristics and Popularity of Videos of Abusive Head Trauma Prevention: Systematic Appraisal J. Med. Internet Res.202426 e 6053010.2196/6053039657172 PMC 11668989 · doi ↗ · pubmed ↗
- 7Oates A.J. Sidpra J. Mankad K. Parenchymal Brain Injuries in Abusive Head Trauma Pediatr. Radiol.20215189891010.1007/s 00247-021-04981-533638693 · doi ↗ · pubmed ↗
- 8Drommi M. Barranco R. Ventura F. Molinelli A. Elder Abuse in Europe’s “Most Elderly” City: An Update of the Phenomenon Based on the Cases Reported to the Penal Court of Genoa from 2020 to 2023 and Literature Review Aging Clin. Exp. Res.20253724210.1007/s 40520-025-03153-x 40778972 PMC 12334366 · doi ↗ · pubmed ↗