The Role of Imaging Techniques in the Evaluation of Extraglandular Manifestations in Patients with Sjögren’s Syndrome
Marcela Iojiban, Bogdan-Ioan Stanciu, Laura Damian, Lavinia Manuela Lenghel, Carolina Solomon, Monica Lupșor-Platon

TL;DR
This review explores how imaging techniques help evaluate non-gland-related complications in Sjögren’s syndrome, improving early detection and monitoring.
Contribution
The paper systematically reviews the specific roles of various imaging modalities in assessing multisystem involvement in Sjögren’s syndrome.
Findings
Ultrasonography and elastography detect muscular and joint inflammation and tissue changes in Sjögren’s syndrome.
High-resolution CT is most reliable for identifying interstitial lung disease in patients with the condition.
MRI is effective in diagnosing neurological complications and lymphoproliferative disorders associated with Sjögren’s syndrome.
Abstract
Sjögren’s syndrome is a chronic autoimmune disease marked by lymphocytic infiltration of the exocrine glands and the development of sicca symptoms, yet some patients also develop extraglandular involvement. Imaging has become relevant for describing these systemic features and supporting clinical assessment. This review discusses the roles of ultrasonography, elastography, computed tomography, and magnetic resonance imaging in evaluating multisystem disease associated with Sjögren’s syndrome. Ultrasonography and elastography help assess muscular involvement by showing changes in echogenicity and stiffness that reflect inflammation and later tissue remodeling. In joints, ultrasound can detect synovitis, tenosynovitis, and early erosive changes, including abnormalities not yet evident on examination. Pulmonary disease, most often with interstitial lung involvement, is best evaluated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
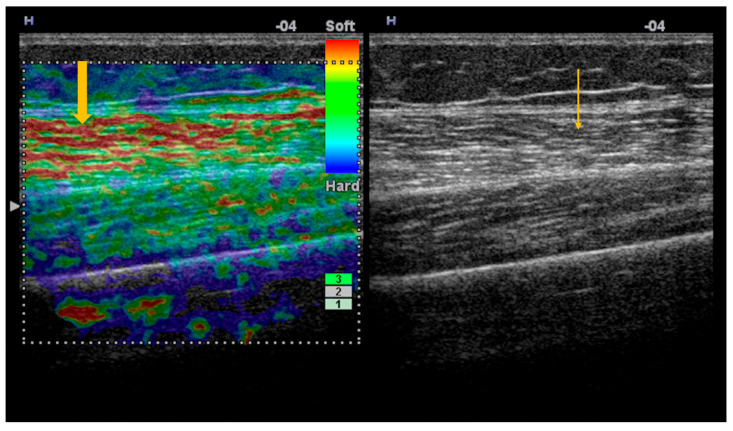 Figure 1
Figure 1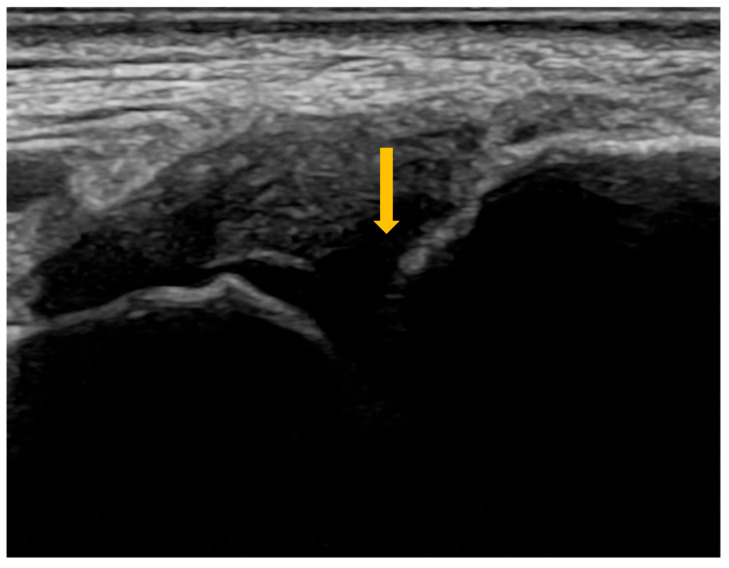 Figure 2
Figure 2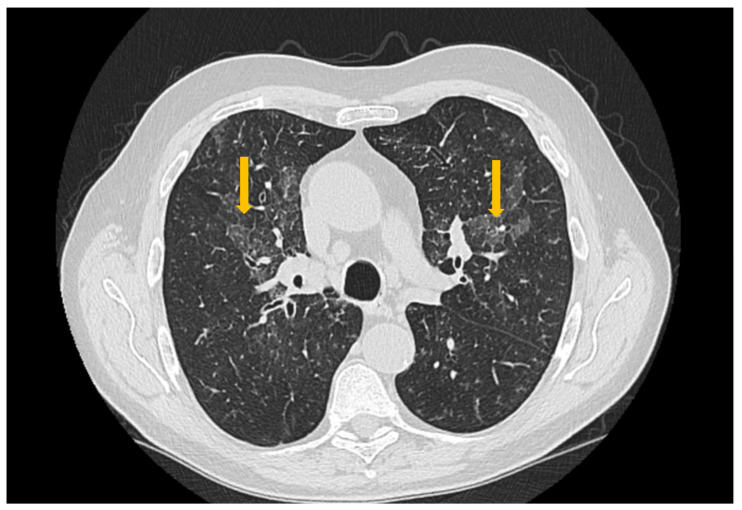 Figure 3
Figure 3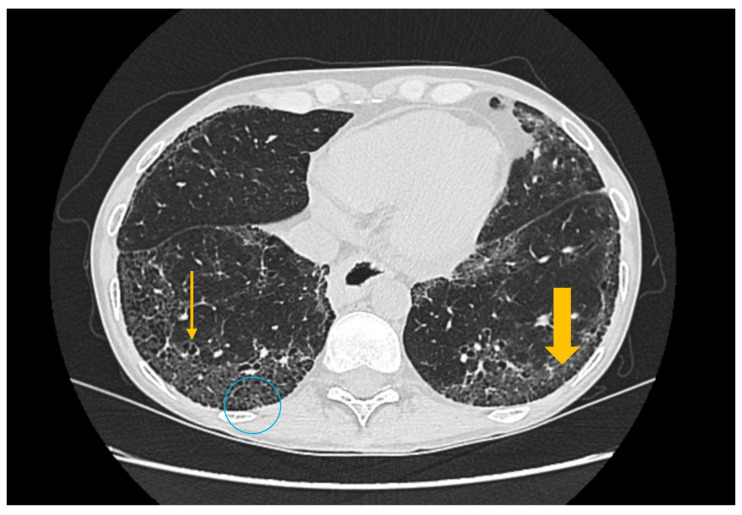 Figure 4
Figure 4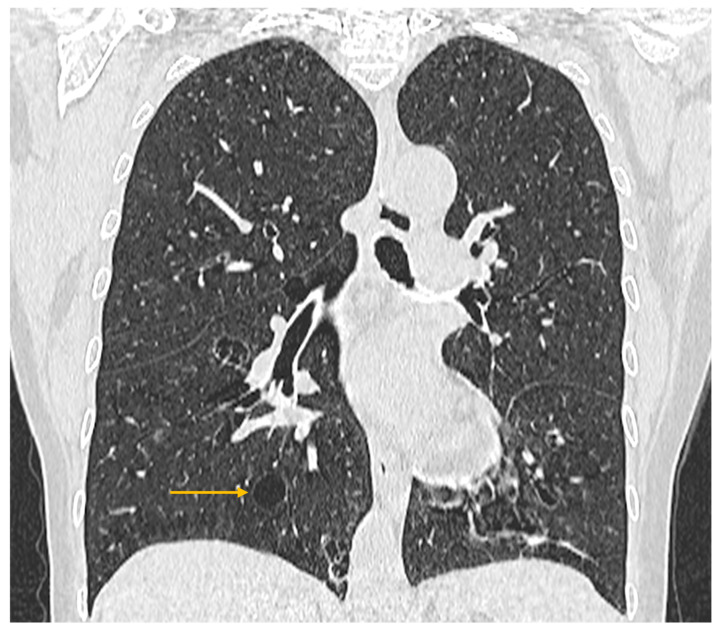 Figure 5
Figure 5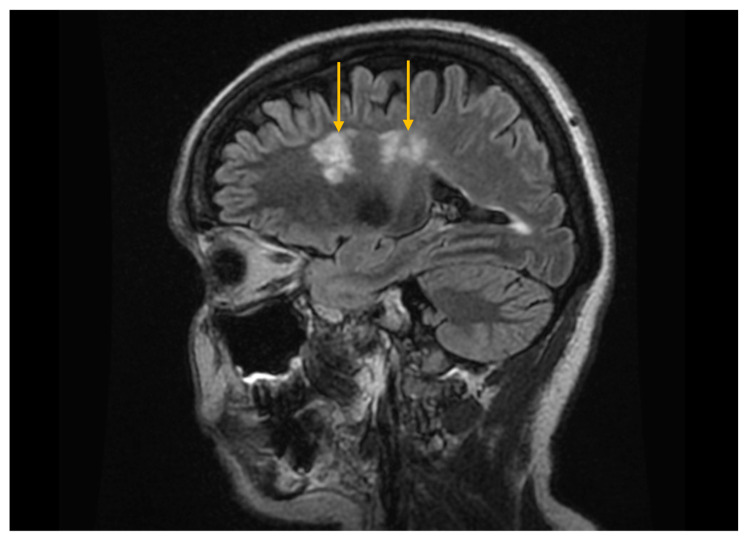 Figure 6
Figure 6 Figure 7
Figure 7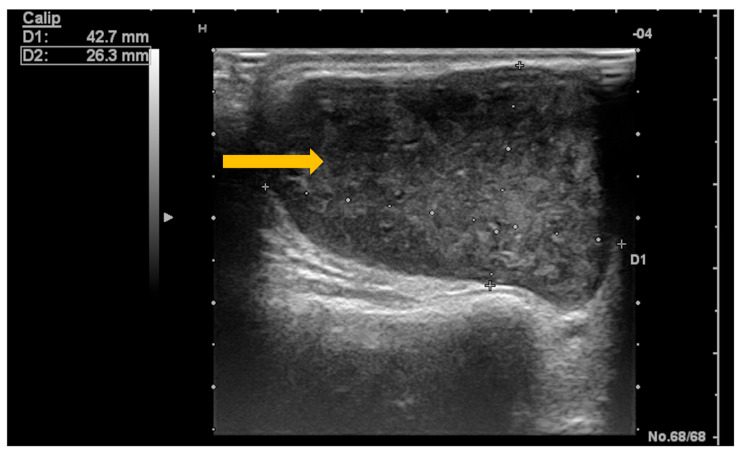 Figure 8
Figure 8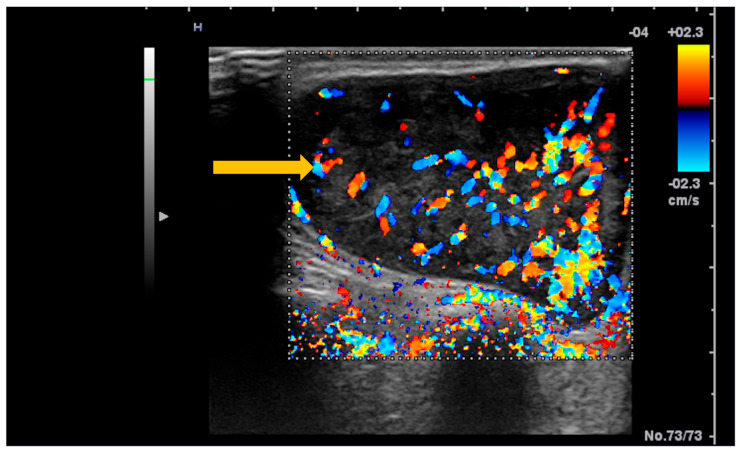 Figure 9
Figure 9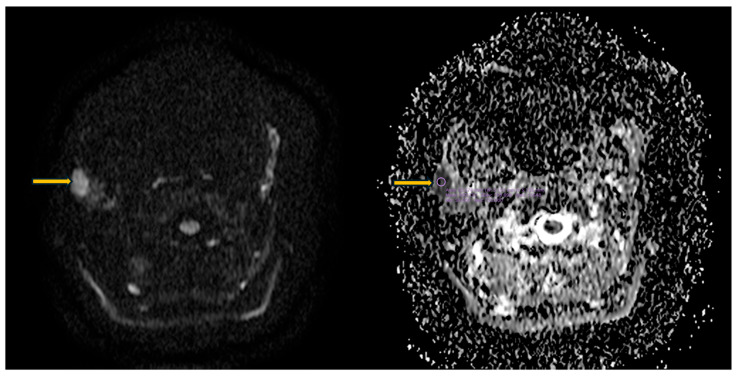 Figure 10
Figure 10| Systemic Manifestations | Prevalence (%) |
|---|---|
| Muscle involvement | <2 |
| Joint involvement | 53 |
| Pulmonary involvement | 23 |
| Central nervous system involvement | 10.8 |
| Systemic Involvement | Findings | Imaging Technique |
|---|---|---|
| Muscular | Myositis | Ultrasonography |
| Articular | Synovitis | Ultrasonography |
| Pulmonary | Interstitial lung disease | High-resolution computed tomography |
| Central nervous system | Demyelinating lesions | Magnetic resonance imaging |
| Lymphoproliferative | Lymphoma | Ultrasonography |
| Grade | Clinical Significance | Ultrasonographic Appearance |
|---|---|---|
| 1 | Normal | Hypoechoic muscle with a clearly visible bone cortex |
| 2 | Mild changes | Mild increase in muscle echogenicity, with a clearly visible bone cortex |
| 3 | Moderate changes | Marked increase in muscle echogenicity, with blurring of the bone cortex |
| 4 | Severe changes | Markedly hyperechoic muscle, with no visualization of the bone cortex |
| Joints | Prevalence (%) |
|---|---|
| Radiocarpal | 30 |
| Metacarpophalangeal | 35 |
| Proximal interphalangeal | 35 |
| Grade | Synovitis | Synovial Hypertrophy on B-Mode US | Power Doppler Signal | Combined Score |
|---|---|---|---|---|
| 0 | Absent | No SH 1, regardless of effusion | No PD 2 | No SH 1 or PD 2 |
| 1 | Minimal | SH 1 not extending beyond the horizontal line connecting the bony surfaces, regardless of effusion | ≤3 isolated spots | SH 1 Grade 1 and PD 2 ≤ Grade 1 |
| 2 | Moderate | SH 1 extending beyond the joint line, with a linear or concave surface, regardless of effusion | >Grade 1, with PD 2 spots < 50% of the SH 1 area | SH 1 Grade 2 and PD 2 ≤ Grade 2 |
| 3 | Severe | SH 1 extending beyond the joint line, with a convex surface, regardless of effusion | >Grade 2, with PD 2 spots > 50% of the SH 1 area | SH 1 Grade 3 and PD 2 ≤ Grade 3 |
| Articular Involvement | Se 4 (%) | Sp 5 (%) |
|---|---|---|
| Synovitis | ||
| RC 1 joint | 73 | 78 |
| MCP 2 joint | 64 | 93 |
| PIP 3 joint | 71 | 94 |
| Tenosynovitis | 86.5 | 100 |
| Erosive arthritis | 67.2 | 97.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Systemic Sclerosis and Related Diseases · Systemic Lupus Erythematosus Research
1. Introduction
Sjögren’s syndrome is a multisystem autoimmune disease with a chronic course, characterized by lymphocytic infiltration of the exocrine glands, particularly the salivary and lacrimal glands, and clinically reflected by the development of sicca syndrome [1,2,3,4,5,6]. In addition to salivary gland involvement, several organ systems may also be affected in Sjögren’s syndrome [3,4,5].
Sjögren’s syndrome affects approximately 0.5–1% of the general population and shows a marked predilection for the female sex, with an estimated female-to-male ratio of nine to one. The average age at diagnosis is around 50 years [2].
The diagnosis of Sjögren’s syndrome is made according to the classification criteria established by ACR/EULAR (American College of Rheumatology/European League Against Rheumatism, currently renamed the European Alliance of Associations for Rheumatology), published in 2016 [7,8].
Modern imaging techniques, such as ultrasonography (US), elastography (SE/SWE), computed tomography (CT), and magnetic resonance imaging (MRI), allow both the characterization of glandular involvement by detecting structural changes in the salivary glands and the evaluation of systemic involvement (muscular and articular, pulmonary, neurological, and lymphoproliferative complications), with the advantage of avoiding the invasive nature of traditional methods and reducing radiation exposure [8,9,10,11,12,13,14,15,16,17].
This paper aims to analyze the role of imaging techniques in evaluating systemic involvement, including the muscular, articular, pulmonary, and neurological systems, as well as lymphoma development, in patients with Sjögren’s syndrome.
2. Methods
This narrative review was based on a focused literature search conducted in PubMed/MEDLINE to identify publications addressing the role of imaging in systemic (extraglandular) manifestations of Sjögren’s syndrome. The search combined Medical Subject Headings (MeSH) and free-text terms related to Sjögren’s syndrome with imaging modalities, including ultrasonography, elastography, computed tomography/high-resolution computed tomography, and magnetic resonance imaging, as well as organ-specific terms referring to musculoskeletal, pulmonary, neurological, and lymphoproliferative involvement. Additional relevant articles were identified through manual screening of reference lists from selected publications. The retrieved evidence was qualitatively analyzed and synthesized, and the results are presented in a narrative format.
All diagnostic imaging figures (ultrasound, elastography, computed tomography, and magnetic resonance imaging) are original and belong to the authors; they were acquired during routine clinical care and fully anonymized before inclusion. The images are presented for illustrative purposes in this narrative review.
3. Imaging Evaluation of Systemic Manifestations in Sjögren’s Syndrome
Sjögren’s syndrome may present with either glandular manifestations (sicca syndrome) or systemic, extraglandular manifestations (Table 1) [18,19]. In a multicenter study, Seror and colleagues reported that, among 395 patients with primary Sjögren’s syndrome, 30% presented systemic manifestations at the time of evaluation, and 39% had previously experienced extraglandular symptoms [20].
EULAR developed the ESSDAI score (EULAR Sjögren’s Syndrome Disease Activity Index) to quantify systemic involvement in Sjögren’s syndrome, and it serves as a standardized tool for assessing disease activity across 12 domains: constitutional (non-specific symptoms such as fever, night sweats, and unintentional weight loss), glandular, articular, muscular, pulmonary, renal, central and peripheral neurological, lymphoma/lymphadenopathy, cutaneous, hematological, and biological [19]. Several of these domains, such as the articular, muscular, pulmonary, neurological, and lymphoma domains, can be assessed by imaging, providing additional information to evaluate the severity of systemic involvement (Table 2).
3.1. Imaging Evaluation of Muscle Involvement in Sjögren’s Syndrome
Histopathologically confirmed myositis is a rare manifestation in Sjögren’s syndrome (<2%) [21,22], characterized by various histological patterns within the spectrum of idiopathic inflammatory myopathies, such as inclusion body myositis, polymyositis, and dermatomyositis [26]. Espitia-Thibault et al. identified a non-specific form of myositis associated with Sjögren’s syndrome, characterized by follicular organization of the lymphocytic infiltrate, suggesting a shared pathogenesis between muscular and glandular involvement in the context of the autoimmune disease [27].
Inclusion body myositis is the most frequent form of myositis associated with Sjögren’s syndrome [26,28]. Imaging techniques are commonly used in clinical practice for patients presenting with muscle weakness, as in idiopathic inflammatory myopathies [29,30,31].
Ultrasonography is a valuable tool for evaluating structural changes in myositis and can be used both for diagnostic purposes and for monitoring disease progression [31]. Ultrasonographic examination shows increased muscle echogenicity in the myositis subtypes mentioned above, along with reduced muscle thickness, the reduction being significantly greater in inclusion body myositis than in other idiopathic inflammatory myopathies or in healthy subjects [29]. The increase in echogenicity results from inflammatory infiltration in the acute phase, during which the bone cortex remains well visualized, while in the chronic phase, it is predominantly due to fatty infiltration, fibrosis, and muscle atrophy [32]. Ultrasonography has a sensitivity and specificity of 82% and 98%, respectively, for the diagnosis of inclusion body myositis [33]. Muscle echogenicity can be assessed ultrasonographically either quantitatively, by placing a region of interest within the examined muscle and measuring its gray-scale value, or semi-quantitatively using the Heckmatt scale (Table 3) [34].
Elastography, both strain and shear-wave, provides additional information to conventional ultrasonography, demonstrating increased stiffness in the acute phase of myositis and reduced stiffness during disease progression, in the context of fatty infiltration (Figure 1) [35]. Because standardized reference values for normal muscle stiffness are not available in the literature, studies rely on comparisons between patients with Sjögren’s syndrome and healthy subjects. In patients with inclusion body myositis, muscle stiffness measured by shear-wave elastography (m/s) is lower compared with normal muscle: vastus lateralis (1.35 ± 0.32 vs. 1.68 ± 0.23), rectus femoris (1.52 ± 0.33 vs. 1.81 ± 0.23), vastus medialis (1.36 ± 0.16 vs. 1.60 ± 0.21) vastus intermedius (1.62 ± 0.49 vs. 1.86 ± 0.22), biceps femoris (1.30 ± 0.14 vs. 1.67 ± 0.20), semitendinosus (1.33 ± 0.31 vs. 1.66 ± 0.23), semimembranosus (1.36 ± 0.28 vs. 1.71 ± 0.18) (p < 0.05) [36].
Strain elastography and corresponding gray-scale imaging of myositis with fatty infiltration. Strain elastography of the thigh skeletal muscle demonstrates reduced tissue stiffness, as indicated by red color coding on the elastography map (thick arrow), indicating softening of the affected muscle. The corresponding gray-scale ultrasound image shows hyperechoic muscle texture (thin arrow), consistent with fatty infiltration.
3.2. Imaging Evaluation of Joint Involvement in Sjögren’s Syndrome
The joints are frequently involved in the systemic inflammatory process of Sjögren’s syndrome, being affected in approximately 53% of patients [23]. Clinical manifestations range from arthralgia without objective inflammatory signs in the joints to inflammatory arthritis (16%)—most often non-erosive, or more rarely erosive, similar to that observed in rheumatoid arthritis (5%) [37,38]. Articular involvement is usually symmetric and affects the radiocarpal (RC), metacarpophalangeal (MCP), and proximal interphalangeal (PIP) joints (Table 4) [37].
Ultrasonography is a valuable imaging tool for identifying articular changes in Sjögren’s syndrome, such as synovitis, tenosynovitis, or bone erosions, including in cases with subclinical involvement that cannot be detected on physical examination [38,39]. Ultrasound of the small joints of the hand (RC, MCP, and PIP) has a sensitivity of 73%, 64%, and 71%, and a specificity of 78%, 93%, and 94% for the diagnosis of synovitis, with an area under the curve of 0.81, 0.91, and 0.91, respectively [40].
On ultrasound, synovitis is characterized by synovial hypertrophy (Figure 2) and joint effusion, with an increased-color Doppler signal suggestive of vascular congestion [38]. The severity of synovitis is assessed using a semi-quantitative scoring system developed by the OMERACT group (Outcome Measures in Rheumatology), which allows classification of patients into different categories of inflammatory activity (Table 5) [41].
B-mode ultrasound of the right radiocarpal joint demonstrating synovial hypertrophy. Gray-scale (B-mode) ultrasound of the right radiocarpal joint shows synovial hypertrophy, appearing as thickened hypoechoic synovial tissue within the joint recess (arrow), consistent with active inflammation.
Tenosynovitis represents an inflammation of the synovial sheath of the tendons, which may lead to reduced joint mobility [42]. Ultrasound has a sensitivity of 86.5%, specificity of 100%, positive predictive value of 100%, negative predictive value of 92.3%, and an accuracy of 94.8% in identifying peritendinous inflammatory processes [43]. On ultrasound, tenosynovitis is characterized by peritendinous fluid accumulation and the presence of a Doppler signal within the synovial sheath [44].
Erosive arthritis was long considered a rare systemic manifestation of Sjögren’s syndrome, being more frequently attributed to rheumatoid arthritis [37]. The use of ultrasonography to evaluate structural changes in the small joints of the hand in patients with Sjögren’s syndrome allows the detection of bone erosions, which develop in the context of persistent intra-articular inflammation [39,45], with a higher prevalence. Ultrasonography has a sensitivity of 67.2%, specificity of 97.5%, positive predictive value of 84.8%, negative predictive value of 90.5%, and an accuracy of 91.5% for identifying cortical bone defects [43]. The coexistence of Sjögren’s syndrome increases the severity of erosive changes in rheumatoid arthritis [46].
The diagnostic performance of ultrasound in the evaluation of articular involvement in primary Sjögren’s syndrome is summarized in Table 6.
3.3. Imaging Evaluation of Pulmonary Involvement in Sjögren’s Syndrome
Pulmonary involvement in patients with Sjögren’s syndrome manifests with symptoms such as persistent cough and dyspnea, associated with abnormal findings on diagnostic tests (pulmonary function tests and high-resolution computed tomography—HRCT) [37]. Pulmonary manifestations result from diffuse interstitial pathologies that develop in these patients, the most frequent histologic subtype being non-specific interstitial pneumonia (NSIP) [47], followed by usual interstitial pneumonia (UIP), lymphoid interstitial pneumonia (LIP), and organizing pneumonia (OP) [24]. The prevalence of interstitial lung disease among patients with Sjögren’s syndrome is 23% [24].
High-resolution computed tomography represents the gold standard for evaluating pulmonary changes in diffuse interstitial lung diseases [48]. This imaging technique has a sensitivity of 100%, specificity of 82%, positive predictive value of 97%, and negative predictive value of 100% for the diagnosis of diffuse interstitial disease [49]. The imaging features vary according to the histologic subtype of involvement (Figure 3, Figure 4 and Figure 5) [50].
High-resolution computed tomography (HRCT) of the chest in non-specific interstitial pneumonia (NSIP). Axial HRCT image demonstrates bilateral, diffuse ground-glass opacities (arrows), associated with interlobular septal thickening and traction bronchiectasis, findings characteristic of fibrotic NSIP.
High-resolution computed tomography (HRCT) of the chest in usual interstitial pneumonia (UIP). Axial HRCT image demonstrates subpleural reticulations (thick arrow), traction bronchiectasis (thin arrow), and honeycombing (circle), with an asymmetric distribution and basal predominance, findings characteristic of UIP.
High-resolution computed tomography (HRCT) of the chest in lymphocytic interstitial pneumonia (LIP). Coronal HRCT image demonstrates thin-walled pulmonary cysts (arrow), a characteristic imaging feature of LIP.
3.4. Imaging Evaluation of Central Nervous System Involvement in Sjögren’s Syndrome
Central nervous system involvement is reported in approximately 10.8% of patients with Sjögren’s syndrome, manifesting as headache, as well as sensory–motor syndromes and visual disturbances [25,51]. Magnetic resonance imaging plays an essential role in detecting structural changes within the central nervous system in the context of Sjögren’s syndrome [16,52].
Headache, usually of a migrainous character, is frequently associated with anti-SSA antibodies and Raynaud’s phenomenon. This association supports the hypothesis of vascular endothelial dysfunction or immune-mediated inflammatory injury affecting the cerebral microcirculation [51]. Imaging reveals ischemic lacunar lesions in the basal ganglia, without a statistically significant association with atherosclerotic plaques identified on color Doppler ultrasound [51].
In patients with Sjögren’s syndrome and neurological involvement, MRI may reveal cerebral demyelinating lesions with a distribution and appearance similar to those observed in multiple sclerosis (Figure 6) [25]. However, the published data regarding their significance are contradictory; some studies report a higher prevalence of demyelinating changes in Sjögren’s syndrome compared with control groups, while others do not demonstrate significant differences, suggesting that these lesions may instead reflect changes associated with normal physiological aging [53,54].
Magnetic resonance imaging (MRI) of the brain using the fluid-attenuated inversion recovery (FLAIR) sequence. Sagittal FLAIR MRI image demonstrates hyperintense cerebral demyelinating lesions (arrows), with a distribution pattern similar to that seen in multiple sclerosis.
In some patients with Sjögren’s syndrome and neurological manifestations, MRI may reveal lesions with features characteristic of neuromyelitis optica or disorders within the neuromyelitis optica spectrum, suggesting a possible association between the conditions (Figure 7) [16,25,52].
Magnetic resonance imaging (MRI) of the brain and orbits, axial T2-weighted short tau inversion recovery (STIR) sequence. The image demonstrates hyperintensity of the left optic nerve (arrow), consistent with optic neuritis.
More rarely, pseudotumoral brain lesions may occur, characterized by mass effect, perilesional edema, absence of diffusion restriction, and peripheral contrast enhancement [55,56,57,58,59]. In some reported cases, histopathologic examination reveals changes consistent with gliosis or vasculitis, and treatment is based on corticosteroid therapy, which leads to improvement of focal symptoms and regression of the lesions on imaging [55,56].
3.5. Imaging Evaluation of Lymphoproliferative Complications in Sjögren’s Syndrome
B lymphocytes play a central role in the pathogenesis of Sjögren’s syndrome through a process of chronic activation that contributes to immune system dysfunction [10]. This sustained stimulation is reflected in the increased risk of developing non-Hodgkin lymphoma, particularly the mucosa-associated lymphoid tissue (MALT) subtype [60,61,62]. Modern imaging techniques—ultrasonography and magnetic resonance imaging—are valuable for monitoring patients with Sjögren’s syndrome to enable early detection of lymphoma [63].
Ultrasonography is the imaging tool most frequently used in clinical practice due to its non-invasive nature, low cost, and wide availability [64]. Dynamic ultrasonographic evaluation of the salivary glands can identify a newly developed hypervascular, oval, relatively well-defined, hypoechoic nodular lesion with intrinsic hyperechoic septa and posterior acoustic enhancement (Figure 8 and Figure 9) [64,65]. At the same time, ultrasonography can be used to guide biopsies of lesions with suspicious imaging characteristics [63].
B-mode ultrasound of the parotid gland in a patient with Sjögren’s syndrome. Gray-scale (B-mode) ultrasound demonstrates a newly developed hypoechoic nodular lesion within the parotid gland (arrow), a finding suspicious for salivary gland lymphoma in the clinical context of Sjögren’s syndrome.
Color Doppler ultrasound of the parotid gland in a patient with Sjögren’s syndrome. Color Doppler imaging demonstrates a newly developed hypervascular nodular lesion within the parotid gland (arrow), a finding suspicious for salivary gland lymphoma in the clinical context of Sjögren’s syndrome.
Magnetic resonance imaging is frequently used for the diagnosis and local staging of lymphoma arising within the salivary glands in Sjögren’s syndrome. Owing to their increased cellularity, lymphomatous lesions show diffusion restriction, with low apparent diffusion coefficient (ADC) values (approximately 0.64 × 10^−3^ mm^2^/s) (Figure 10) [66]. On dynamic contrast-enhanced MRI, lymphoma typically demonstrates a type III enhancement curve, characterized by rapid gadolinium uptake and washout [67]. The time-to-peak (TTP) is the most sensitive parameter for distinguishing MALT lymphoma from benign lymphoepithelial lesions. Using a cut-off value of 79.65 s, TTP has an overall diagnostic accuracy of 94.7%, with a sensitivity of 94.1% and specificity of 95.2%. TTP values below this threshold are strongly associated with malignancy, whereas longer TTP values are indicative of benign lesions, reflecting differences in tumor vascularity and contrast kinetics [67].
MRI diffusion-weighted imaging (DWI) and ADC map of the parotid gland. Axial images show a right parotid nodular lesion with restricted diffusion (arrows). The purple circle indicates the region of interest (ROI) used for calculation of the apparent diffusion coefficient (ADC), which is markedly reduced (0.460 × 10−3 mm2/s), a pattern suspicious for salivary gland lymphoma in the context of Sjögren’s syndrome.
In recent years, MRI radiomics (textural analysis on STIR/T2 and ADC sequences) has shown potential for risk stratification of lymphoma in patients with Sjögren’s syndrome and for differentiating benign from malignant parotid tumors, demonstrating high performance (AUC~0.931) in internal validation models [68], representing a promising direction for future research.
4. Conclusions
Modern imaging techniques play a central role in the multisystem evaluation of patients with Sjögren’s syndrome. Ultrasonography is a non-invasive, accessible, and reproducible imaging method, frequently used in clinical practice to identify and characterize changes within the muscular and articular systems, such as myopathies, synovitis, tenosynovitis, joint effusion, and bone erosions. High-resolution computed tomography accurately detects pulmonary abnormalities, particularly diffuse interstitial disease. Magnetic resonance imaging provides higher resolution than ultrasound and is valuable for diagnosing lymphoproliferative complications and assessing articular and neurological involvement.
Integrating these imaging modalities with clinical and paraclinical data enables a comprehensive approach to patients with Sjögren’s syndrome, facilitating early diagnosis, differentiation from other pathologies, monitoring disease progression, and detection of extraglandular complications arising in the context of immune dysregulation and persistent systemic inflammation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AndréF. Böckle B.C. Sjögren’s syndrome J. Dtsch. Dermatol. Ges.202220980100210.1111/ddg.14823 PMC 953988135775593 · doi ↗ · pubmed ↗
- 2Baldini C. Talarico R. Tzioufas A.G. Bombardieri S. Primary Sjogren Syndrome Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 431049/(accessed on 19 September 2025)
- 3Negrini S. Emmi G. Greco M. Borro M. Sardanelli F. Murdaca G. Indiveri F. Puppo F. Sjögren’s syndrome: A systemic autoimmune disease Clin. Exp. Med.20222292510.1007/s 10238-021-00728-634100160 PMC 8863725 · doi ↗ · pubmed ↗
- 4Maleki-Fischbach M. Kastsianok L. Koslow M. Chan E.D. Manifestations and management of Sjögren’s disease Arthritis Res. Ther.2024264310.1186/s 13075-024-03262-438331820 PMC 10851604 · doi ↗ · pubmed ↗
- 5Lodba A. Ancuta C. Tatarciuc D. Ghiorghe A. Lodba L.O. Iordache C. Comparative Analysis of Glandular and Extraglandular Manifestations in Primary and Secondary Sjögren’s Syndrome: A Study in Two Academic Centers in North-East Romania Diagnostics 202414236710.3390/diagnostics 1421236739518335 PMC 11545017 · doi ↗ · pubmed ↗
- 6Zabotti A. Zandonella Callegher S. Tullio A. Vukicevic A. Hocevar A. Milic V. Cafaro G. Carotti M. Delli K. De Lucia O. Salivary Gland Ultrasonography in Sjögren’s Syndrome: A European Multicenter Reliability Exercise for the Harmonic SS Project Front. Med.2020758124810.3389/fmed.2020.581248 PMC 771981933330537 · doi ↗ · pubmed ↗
- 7Shiboski C.H. Shiboski S.C. Seror R. Criswell L.A. Labetoulle M. Lietman T.M. Rasmussen A. Scofield H. Vitali C. Bowman S.J. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts Arthritis Rheumatol.201769354510.1002/art.3985927785888 PMC 5650478 · doi ↗ · pubmed ↗
- 8Horai Y. Shimizu T. Nakamura H. Kawakami A. Recent Advances in Pathogenesis, Diagnostic Imaging, and Treatment of Sjögren’s Syndrome J. Clin. Med.202413668810.3390/jcm 1322668839597832 PMC 11595189 · doi ↗ · pubmed ↗