Patient Concerns Inventory for Arabic Patients with Head and Neck Cancer: A Cross-Cultural Adaptation and Preliminary Validation
Abdullah M. Alsoghier, Bader A. Alwhaibi, Abdullah F. Alnuwaybit, Simon N. Rogers, Saif A. Aljabab

TL;DR
This paper adapts and validates a patient concern inventory for head and neck cancer patients in Arabic, aiming to better understand their unique needs and experiences.
Contribution
The study provides a cross-culturally adapted and preliminary validated Arabic version of the Patient Concerns Inventory for head and neck cancer.
Findings
The Arabic PCI-HN showed good internal consistency (α = 0.723) but fair test–retest agreement (κ = 0.22).
Cultural adaptations were made to items related to social and religious welfare in the Arabic version.
The instrument is recommended for further validation in larger, multi-center studies.
Abstract
Individuals with head and neck cancer usually experience many concerns related to their diagnosis and care needs. Examples could include the treatment of undesired effects on physical, psychological and social aspects. There is no available instrument to investigate the problems associated with this condition for Arabic patients. The present study translated a commonly used patient concern inventory tailored to this condition and its treatment. It tested its precision and accuracy to measure individual preferences and needs. There were varying cultural views on topics such as social and religious issues between the original English and its Arabic translation. Recommendations were presented for further testing with large patient populations and multiple hospitals across the Arabic countries. Introduction: Head and neck cancer (HNC) treatments often lead to significant post-treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
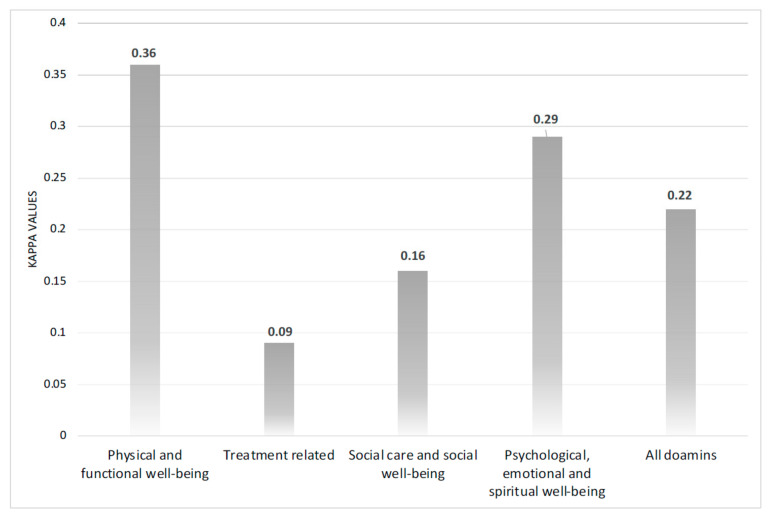 Figure 1
Figure 1- —King Saud University, Riyadh, Saudi Arabia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Head and Neck Cancer Studies · Oral health in cancer treatment
1. Introduction
Head and neck cancers (HNC) constitute a heterogeneous group of malignancies that significantly affect basic human functions, including speech, taste, swallowing, breathing, and appearance. Globally, HNC accounts for more than 890,000 new cases and over 450,000 deaths annually, making it the seventh most common cancer type [1]. The oral and oropharyngeal cancer figures, based on 448 million individuals living in 23 countries of the Middle East and North Africa region, showed an age-standardised incidence rate of 2.6 and 1.1 per 100,000 population for males and females, respectively [2]. Incidence rates for HNCs are increasing and expected to double or increase by 2–4 times by 2040 in the Gulf Cooperation Council countries, including Saudi Arabia, Bahrain, Oman, Kuwait, Qatar, and the United Arab Emirates [3]. It is also notable that variations exist between regions within the same country, where sometimes younger adults and females are unexpectedly at higher risk [3,4].
Survivors of HNC frequently report late and long-term effects and concerns, such as xerostomia, dysphagia, pain, fatigue, anxiety, and body image [5]. These can have a profound impact on physical health, emotional stability, social interactions and overall health-related quality of life [6]. Such concerns are often underreported or missed in routine consultations, as clinical care often focuses on tumour control and survival metrics.
Given the physical and functional impairment combined with the psychosocial impact of HNC and its treatment, a shift toward holistic and patient-centred clinical care has become essential. To help achieve this, patient-clinician consultations benefit from tailored information based on patients’ concerns. This can enhance patient satisfaction and potentially improve care outcomes [7]. Previous work on patients with oral precancerous lesions demonstrated that a somewhat discordance concerning patient-clinician agreement on important topics is essential to identify what exactly a patient would like to know about their disease, address their concerns (e.g., fear of cancer recurrence or progression) and determine which aspects of their disease they prioritise over others [5].
The Patient Concerns Inventory for Head and Neck (PCI-HN) is a patient-reported outcome measure tool that facilitates patient-focused consultations for various diseases, including HNC [5]. This tool simply asks the patient to choose one or more of the 56 topics they wish to discuss during clinical consultations across four domains: physical and functional well-being; social care and social well-being; psychological, emotional, and spiritual well-being; and treatment-related issues [5]. This enables patients to identify issues they wish to discuss with the clinician during routine clinical consultations.
Furthermore, PCI-HN demonstrated excellent content validity compared to other instruments addressing HNC-related unmet needs, including physical and psychological needs, daily activities, and other needs related to information, social, spiritual, dental, communication, sexual, financial aspects, and access to care [8]. Furthermore, its contribution to value-based healthcare for patients with HNC has been demonstrated through a randomised clinical trial in the UK, showing it to be a low-cost intervention that can improve patient satisfaction, multidisciplinary referrals, and the detection of otherwise overlooked issues [7]. The University of Washington Quality of Life questionnaire (UW-QOL) was used in conjunction with PCI to measure various aspects of health-related quality of life over the past week [9,10]. The UW-QOL has been translated and validated across several languages, including Turkish, Chinese, and Portuguese, demonstrating its adaptability and cross-cultural relevance [11,12,13]. Also, its Arabic version demonstrated adequate reliability (test–retest and internal consistency) and construct validity among a cohort of HNC patients in Morocco [9].
There remains little known about patient-reported needs and concerns in Arabic-speaking patients with HNC. PCI-HN was previously translated into Chinese, Dutch, French, German, Greek, Hindi, Malay, Mandarin, Serbian, Spanish, Polish, Portuguese, Tamil, and Urdu. However, no valid Arabic translation is currently available. Addressing cultural and linguistic differences among patient populations globally can improve the understanding of how patients perceive symptoms and express their concerns [14]. It is also mandatory to maintain personalised patient-clinician communication and education [7,14]. The present work aimed to translate and assess the reliability (test–retest and internal consistency) and validity (content, face, and construct) of the Arabic versions of the PCI for patients with HNC.
2. Materials and Methods
Patients attending the outpatient oncology clinics at King Saud University Medical City between March 2022 and January 2024 were enrolled in the study. A convenience non-random sampling method was used to identify potential participants aged 18 years or older with pathologically confirmed HNC diagnoses, who had received HNC treatment, and who were native Arabic-speaking patients [15,16]. Exclusion criteria included those younger than 18 years of age and who did not receive HNC treatment, had severely debilitating diseases, and could not read and understand the Arabic language.
The study investigators included an oral medicine consultant involved in the multidisciplinary HNC team (A.M.A.), a medical oncologist with a focus on head and neck cancers and provided care for these patients (S.A.F), two medical interns who were involved in oncology rotations (A.F.A. and B.A.A.) and a maxillofacial surgeon who had experience in patient concerns related to HNC (S.N.R.). Each participant was recruited after their routine care visits to a medical oncology clinic. At the end of the consultation, two study investigators (A.F.A. and B.A.A.) provided the patients with written information about the study. Those who agreed were recruited in the same or next care visit per their wishes. Potential participants received information about completing the electronic version of the questionnaires. After signing the informed consent form, the recruited participants completed the tablet-based information independently and reported no difficulties or technical issues.
2.1. Translation and Cross-Cultural Adaptation
The Arabic PCI (Ar-PCI-HN) was adapted from the original English versions using the forward-backwards translation method, in line with the principles of good practice for translating and culturally adapting patient-reported outcome measures (PROMs) [13,17]. Two bilingual study investigators conducted forward translation, two performed translation reconciliation, two addressed synthesis and modifications, and then two independent translators performed back translation into English. A panel of study investigators reviewed all versions for conceptual equivalence, harmonisation, and cultural appropriateness, as well as proofreading (Table 1) [17,18].
2.2. Content and Face Validity
The content validity was assessed by six clinicians, comprising three oral medicine specialists and three medical oncologists, all with more than 10 years of relevant experience in HNC care. Questions to ensure that all Ar-PCI-HN items are relevant to the patient population, the area of interest [e.g., the concerns of patients that they would like to discuss during their consultation], the context of interest [e.g., to address a wide variety of problems, assist direct outpatient appointments, and advance interdisciplinary therapy], and whether each response option is appropriate. Clinicians were also asked about comprehensiveness by asking, ‘Are all key concepts related to patient concerns included?’ (Supplementary File S1) [19,20,21]. All six clinicians viewed the items as comprehensive, appropriate, and relevant to the patient population and the area/context of interest. However, they had demonstrated specific comments and suggestions for the initial version (Table 2).
Additionally, cognitive debriefing and face validity were initially assessed through semi-structured interviews with six patients to evaluate relevance, comprehensiveness, and comprehensibility [17,20,21]. After reading the electronic version of Ar-PCI-HN using touch-screen technology [22], all noted that items were related and comprehensive. Although five of them noted a low understanding of the meaning of physical and functional well-being, attractiveness to a romantic partner, and were unsure about the roles of social workers and financial counsellors. After revisions, another group of eight patients found all revised items were indeed relevant and easy to comprehend (Table 3).
2.3. Construct Validity
Construct validity was examined using Spearman’s rank correlation coefficient (ρ) to assess associations between Ar-PCI-HN and the Ar-UW-QOL questionnaire (v 4.0) [9]. Based 4 or 5-point scale, this version included (1) items related to activity, anxiety, appearance, chewing, mood, speech, shoulder, recreation, saliva, swallowing, taste and pain; (2) a question to indicate up to 3 important symptoms to the patient of the previous items; and (3) global questions to rate the health-related quality of life over the past month, past week and overall [23]. Its Arabic translation was validated in a head and neck cancer patient cohort and demonstrated a good internal consistency (Cronbach’s α = 0.82) and excellent test–retest reliability (Intraclass correlation coefficient = 0.098) [22].
2.4. Statistical Analysis
Data were analysed using IBM SPSS (v.25). Internal consistency, which measures the interrelatedness within a multi-item instrument, was assessed using Cronbach’s alpha (α), with values ≥0.70 indicating acceptable reliability [19,24]. Assessments by Cohen’s Kappa (κ) for nominal variables were performed to assess the test–retest reliability of Ar-PCI-HN between the first and second completions by participants over 7–14 days [19]. These were interpreted based on the level of agreement as slight (<0.20), fair (<0.40), moderate (<0.60), substantial (<0.80), and almost perfect (>0.80) [25].
For the ordinal variables, the intraclass correlation coefficients (ICCs) were used to assess the test–retest reliability of the Ar-UW-QOL [19]. ICCs were interpreted as poor (<0.5–0.75), moderate (<0.75), or good-excellent (>0.75) [26]. Statistical significance was set at a p-value of 0.05 or less.
Ethical approval was prospectively approved by the Institutional Review Board of King Saud University [Ref: 23/0221/IRB, date: 14 February 2023]. All study participants read the study information sheet and signed the informed consent form, indicating their participation and consent for publication.
3. Results
The records of 113 patients were initially screened for eligibility. After excluding 75 records for patients awaiting HNC treatment and those in palliative care, 38 patients (males = 19, females = 19) with a mean age of 50 ± 16.13 years (range, 18–90 years) were invited and agreed to participate following their routine clinical care visits. Regarding their educational attainment, 22 had a high school education or less, 14 had a bachelor’s degree, and 2 had postgraduate degrees. They were mainly retired or unemployed (n = 24), with the remaining being either employed (n = 12) or students (n = 2). Regarding tobacco use and alcohol drinking, 29 of them (76%) indicated that they never smoked, 9 were previous tobacco users, and none indicated present or previous alcohol drinking.
The Ar-PCI-HN demonstrated acceptable internal consistency, with a Cronbach’s α of 0.723; all items exceeded the cut-off for acceptable internal consistency reliability (α = 0.71). These included physical and functional well-being (α = 0.72), treatment-related (α = 0.72), social care and social well-being (α = 0.72), and psychological, emotional, and spiritual well-being (α = 0.72). Its test–retest reliability between the first and second completions by 31 of the 38 patients was fair (average κ = 0.22). Notably, the highest and lowest agreement was observed for physical and functional well-being (κ = 0.36) and treatment-related items (κ = 0.09), respectively (Figure 1).
The Ar-UW-QOL demonstrated strong internal consistency, with a Cronbach’s alpha of 0.753 and good test–retest reliability, as indicated by an ICC of 0.753. Domain-level analysis revealed that the most affected areas were saliva, swallowing, and appearance. Approximately 48% of participants reported dysfunction in at least one UW-QOL domain, 24% in two or more domains, and 9% in four or more. Mean composite UW-QOL scores indicated moderate impairment across most domains. Construct validity analysis revealed a weak, non-significant positive correlation between Ar-PCI-HN and Ar-UW-QOL total scores (ρ = 0.296, p = 0.119), suggesting these instruments capture overlapping but distinct constructs. The final version of the Ar-PCI-HN is available online (Supplementary File S2).
4. Discussion
This study represents the first attempt to translate, culturally adapt, and preliminarily test the internal consistency of Ar-PCI-HN in a cohort of patients with HNC. The results demonstrated that Ar-PCI-HN is a helpful tool for Arabic-speaking HNC populations. The internal consistency of the Ar-PCI-HN (α = 0.723) aligns with its English version (α = 0.76) [5], while the Brazilian Portuguese version demonstrated an alpha of 0.78 [6]. Similarly, the Ar-UW-QOL’s internal consistency (α = 0.753) is comparable to other versions, including the Turkish (α = 0.74) [13], Chinese (α = 0.79) [12], and Hindi (α = 0.75) [27], confirming its acceptable psychometric properties across different patient populations. Furthermore, the overall fair agreement between both completions by participants might be explained by the over-time changes in perceived needs and concerns in cancer care.
Clinically, the Ar-UW-QOL revealed that saliva, swallowing, and appearance were the most affected domains, as observed in another clinical cohort of post-radiotherapy HNC survivors [28]. Similar findings were noted in a Brazilian patient cohort, emphasising the tool’s sensitivity in detecting common treatment-related sequelae [29].
The relatively weak correlation between Ar-PCI-HN and Ar-UW-QOL (ρ = 0.296) confirms their complementary roles. While the UW-QOL quantifies functional impairment, the PCI identifies broader and more subjective concerns, such as emotional distress and family impact. A large UK randomised trial demonstrated that routine use of the PCI in outpatient consultations enhanced communication and identified concerns not typically captured by structured instruments [7]. Similarly, a study in Brazil confirmed that the PCI identified unmet psychosocial and practical needs in patients that would have otherwise gone unaddressed.
A significant negative correlation was found between the Ar-UW-QOL and the Xerostomia Inventory (ρ = –0.434), underscoring the burden of xerostomia on post-treatment quality of life. These findings are consistent with validation work in China and Turkey, where xerostomia and swallowing dysfunction were among the top concerns affecting quality of life (QOL) [12,13].
The results underscore the importance of implementing culturally adapted PROMs in Arabic-speaking clinical settings. In the Middle Eastern countries, where cancer incidence is projected to increase substantially [2,3], the need for patient-centred, culturally competent care is urgent. It also highlights the importance of considering diverse cultural and social interpretations across different patient populations (e.g., items related to social and religious welfare and financial counselling). The perceived importance of such topics might be less desirable to discuss with clinicians in a Western population but rather considered essential among those in the Arabic world [30,31]. For instance, decisions to own health in cancer care (e.g., palliative and end-of-life care) in Arabic countries are often affected by religious beliefs where a disease might be seen as a natural fate or indeed faith/patience testing and penance for sins [32]. Therefore, addressing these spiritual/cultural underpinnings with appropriate counselling might facilitate HNC diagnosis acceptance and early management [32,33]. This also explains why the related AR-PCI-HN followed cultural and religious views compared to its original version, while the measured construct in both versions remains similar (e.g., ‘Spiritual/religious aspects’ was adapted as ‘religion’).
PROMs, such as the PCI and UW-QOL, support early symptom detection, improved multidisciplinary referrals, and patient empowerment, all of which contribute to better treatment experiences and outcomes. Furthermore, integrating the PCI into routine care supports multidisciplinary communication, enhances psychological screening, and improves consultation quality without extending visit time [7,21]. The PCI has also been shown to enhance the quality of life when used consistently across follow-ups.
There remain little known related to access healthcare services in the Arabic countries due to sometime limited resources, increased out-of-pocket healthcare cost and insufficient expenditure for clinical services concerning cancer screening, surgical and chemoradiotherapy interventions and rehabilitation [34,35]. The is also a notable lack of clinical research that ascertaining the patient experiences and needs through the cancer journey, including what they wish to discuss with their care providers in short and perhaps overwhelming cancer services [36,37,38]. The cultural, religious, and social underpinnings are profound determinants of patient concerns in the Middle East and North Africa, where around half a billion Arabic speakers live [39]. Thus, Ar-PCI can be incorporated as a web-based tool as a hospital visit diary to help patients determine what they wish to address during their clinical visits with relevance. This can be available as a pre-visit checklist sent via phone text or email along with the appointment reminder. Then responses could be linked to the patient’s electronic medical records to support informed decisions about their care and to maintain tailored, patient-centred discussions. The Ar-PCI may also support an accurate referral process and resource allocation that addresses the patient’s care needs and maintains value-based healthcare services [5].
This study addresses a key gap in global oncology literature: the underrepresentation of Arabic-speaking patients in PROM validation. By offering validated instruments in a language patients can understand, this work provides a foundation for inclusive, high-quality care, enabling cross-cultural comparisons in survivorship research [40]. Additionally, using touch-screen/computerised questionnaires may be burdensome for individuals with low digital literacy or visual limitations [22]. However, this was not observed in the present study, which employed standardised settings and training for the study investigators (e.g., a quiet clinical waiting area, sufficient explanation of the study activities, appropriate timing for completing the questionnaires, and clarification of any unclear items). The relatively small sample size and single-centre design may limit the generalizability of the findings.
Further multicentre studies with larger and more diverse patient populations and clinical settings are needed to assess the over-time changes in perceived needs further to ensure that the presently limited test–retest (κ = 0.22) of Arabic PCI-HN is rather a reflection of clinical changes during the 7–14-day period of perceived needs than a structural limitation of the instrument. Additionally, further assessments are necessary to determine the criterion/construct validity (comparisons with the gold standard/instruments using similar constructs), responsiveness, and clinical interpretability of Ar-PCI-HN in different Arabic-speaking countries.
5. Conclusions
The Ar-PCI-HN is a culturally appropriate instrument with acceptable content and face validity, as well as internal consistency reliability, for assessing the multifaceted experiences of HNC survivors in Arabic-speaking countries. These assessments highlighted the essence and practical value of cross-cultural adjustments. There is, however, a need for further testing of other measurement properties to ensure their suitability for clinical practice, including identifying unmet needs, guiding individualised care, and enhancing survivorship outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Alsharif A. Alsharif M.T. Samman M. Binmadi N. Kassim S. Mourad S. Warnakulasuriya S. Forecasting Head and Neck Cancer Trends in GCC Countries: Implications for Public Health Policy and Strategy Risk Manag. Healthc. Policy 2023162943295210.2147/RMHP.S 44516238164292 PMC 10758177 · doi ↗ · pubmed ↗
- 3Alqahtani W.S. Almufareh N.A. Al-Johani H.A. Alotaibi R.K. Juliana C.I. Aljarba N.H. Alqahtani A.S. Almarshedy B. Elasbali A.M. Ahmed H.G. Oral and oropharyngeal cancers and possible risk factors across Gulf Cooperation Council countries: A systematic review World J. Oncol.20201117310.14740/wjon 128332849958 PMC 7430852 · doi ↗ · pubmed ↗
- 4Alhazzazi T.Y. Alghamdi F.T. Head and Neck Cancer in Saudi Arabia: A Systematic Review Asian Pac. J. Cancer Prev.2016174043404810.7314/APJCP.2016.17.3.113527644659 · doi ↗ · pubmed ↗
- 5Rogers S.N. El-Sheikha J. Lowe D. The development of a Patients Concerns Inventory (PCI) to help reveal patients concerns in the head and neck clinic Oral. Oncol.20094555556110.1016/j.oraloncology.2008.09.00419028135 · doi ↗ · pubmed ↗
- 6Jungerman I. Toyota J. Montoni N.P. Azevedo E.H.M. Guedes R.L.V. Damascena A. Lowe D. Vartanian J.G. Rogers S.N. Kowalski L.P. Patient Concerns Inventory for head and neck cancer: Brazilian cultural adaptation Rev. Assoc. Médica Bras.20176331131910.1590/1806-9282.63.04.31128614532 · doi ↗ · pubmed ↗
- 7Rogers S.N. Allmark C. Bekiroglu F. Edwards R.T. Fabbroni G. Flavel R. Highet V. Ho M.W.S. Humphris G.M. Jones T.M. Improving quality of life through the routine use of the patient concerns inventory for head and neck cancer patients: Main results of a cluster preference randomised controlled trial Eur. Arch. Oto-Rhino-Laryngol.20212783435344910.1007/s 00405-020-06533-3PMC 775126333346856 · doi ↗ · pubmed ↗
- 8Shunmugasundaram C. Rutherford C. Butow P.N. Sundaresan P. Dhillon H.M. Content comparison of unmet needs self-report measures used in patients with head and neck cancer: A systematic review Psychooncology 2019282295230610.1002/pon.525731654540 · doi ↗ · pubmed ↗