Germline BRCA1/2 Variants in Polish Patients with Family History of Breast and Ovarian Cancer: Prevalence, CNV Detection, and Identification of a Novel Loss-of-Function Mutation
Sebastian Skoczylas, Tomasz Płoszaj, Izabela Dróżdż, Hanna Moczulska, Marcin Serafin, Katarzyna Piekarska, Olga Wojtyczka, Karolina Żeżawska, Agnieszka Zmysłowska

TL;DR
The study examines BRCA1/2 gene variants in Polish individuals with a family history of breast and ovarian cancer, identifying a new mutation and highlighting challenges in genetic diagnosis.
Contribution
A novel loss-of-function mutation in the BRCA1 gene and a deletion in exon 21 were identified in Polish patients.
Findings
16 unique pathogenic or likely pathogenic BRCA1/2 variants were identified in 22 patients.
A deletion in exon 21 of the BRCA1 gene was found in two patients.
Only 4.89% of the cohort had detectable genetic predisposition to cancer.
Abstract
Among the Polish population, around 4% of breast cancer patients and 10% of ovarian cancer patients have pathogenic variants of the BRCA1 gene, whereas variants of the BRCA2 gene are uncommon. Short-read sequencing provides a comprehensive range of data, including the detection of CNVs (copy number variants), but it still poses challenges when using standard NGS workflows. In this study, we investigated genetic variants in a cohort of 450 unaffected individuals with a family history of breast and/or ovarian cancer, involving at least one first-degree relative, with particular emphasis on CNV detection. In our study, the detection accuracy was just 4.89%, indicating that the genetic predisposition to cancer could not be demonstrated in the majority of patients. Background/Objectives: Pathogenic and likely pathogenic variants in the BRCA1 and BRCA2 genes are associated with a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
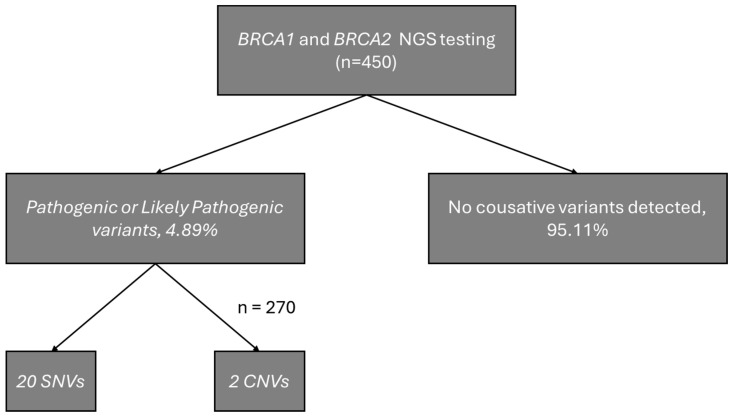 Figure 1
Figure 1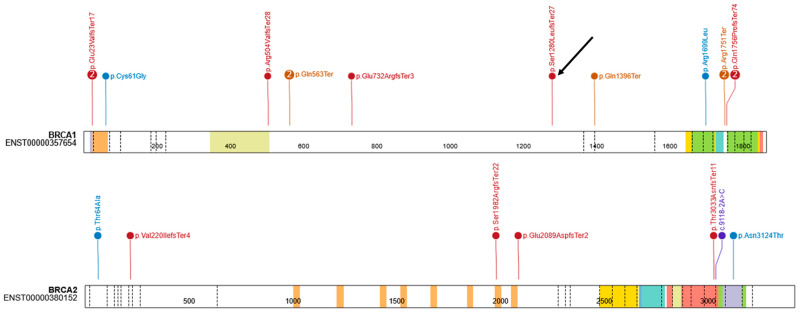 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Genomic variations and chromosomal abnormalities · Genetic factors in colorectal cancer
1. Introduction
The role of predisposition to breast and ovarian cancer caused by germline pathogenic variants in BRCA1 and BRCA2 is well documented in the literature. Pathogenic variants in the BRCA1 gene increase the risk of developing breast cancer to 55–72%, whereas variants in BRCA2 increase the risk to 45–69% [1]. In the Polish population, about 4% of breast cancer patients and 10% of ovarian cancer patients carry pathogenic variants in the BRCA1 gene [2,3,4]. According to the Szwiec et. al. paper, Polish women diagnosed with breast cancer below the age of 50 should be screened with a panel of six founder mutations in BRCA1: NM_007294.4:c.181T>G, NM_007294.4:c.4035del, NM_007294.4:c.5266dup, NM_007294.4:c.3700_3704del, NM_007294.4:c.68_69del and NM_007294.4:c.5251C>T (C61G, 4153delA, 5382insC, 3819del5, 185delAG and 5370C>T) 4) [4]. The screening used to include these variants, but now the standard testing includes targeted NGS of BRCA1/2 genes.
Another important aspect is the care of relatives of individuals with a history of breast and/or ovarian cancer, which may improve predictive accuracy in the case of hereditary variants present in the family [1]. While BRCA1 and BRCA2 are the primary genes associated with hereditary breast and ovarian cancer, several other high-penetrance genes (e.g., TP53, PTEN, CDH1) and moderate-risk genes (e.g., ATM, CHEK2, BARD1, etc.) also contribute to cancer susceptibility [1,5,6,7].
Why is testing for variants in the BRCA1/2 genes so crucial? Individuals who carry germline pathogenic variants in these genes are sensitive to poly(ADP-ribose) polymerase (PARP) inhibitors and DNA-damaging agents, including platinum-based chemotherapies. Therefore, recognizing them is important, as this influences both therapeutic and preventive strategies. This information is used to determine eligibility for targeted therapies, which have been shown to provide this group with significant clinical benefits [8]. In addition to their therapeutic value, BRCA1/2 tests play a key role in preventing cancer and managing family risk. This allows for the implementation of personalized surveillance programs, including earlier and more frequent screening tests, such as magnetic resonance imaging, ultrasound and mammography. Importantly, testing is beneficial not only in families with a high risk of cancer, but also in those with a moderate or unclear family history of breast and ovarian cancer [1]. Some carriers may not meet the classic criteria [9]. They can still benefit from preventive interventions once identified. Furthermore, relatives can be tested to help identify those who are unaware of their hereditary predisposition to cancer [10]. This enables early intervention before the disease develops, before any symptoms appear [11]. In this context, genetic testing is becoming the basis for personalized medicine and cancer prevention at a population level. It also facilitates cascade testing of relatives, promoting early detection in asymptomatic carriers and enabling timely medical interventions, even in families without a strong cancer history [9].
Given the large number of variants in the BRCA1/2 genes, molecular diagnostics in breast cancer patients should be performed using next-generation sequencing (NGS) [1,5,6,7]. Despite the fact that short read sequencing offers a comprehensive range of data from sequencing, even for deep intronic variants or CNVs (copy number variants), it still poses a challenge when using standard NGS workflows [12]. Despite the widespread use of NGS in clinical practice, the prevalence and spectrum of BRCA1/2 variants, particularly CNVs, in Polish families with unaffected individuals and a family history of breast and/or ovarian cancer involving at least one first-degree relative, remain limited.
This study aimed to expand current knowledge of germline BRCA1/2 variants in the Polish population by analyzing patients with a family history of breast and/or ovarian cancer, with particular focus on the detection of copy number variants (CNVs).
2. Materials and Methods
A total of 450 unaffected individuals (9.11% male and 90.89% female) with a family history of breast and/or ovarian cancer were recruited between 2021 and 2024 at the Clinical Genetics Outpatient Clinic of the Department of Clinical Genetics at the Medical University of Lodz, Poland. In 2021, within the Polish Ministry of Health program, 12,277 individuals underwent BRCA1 and BRCA2 genetic testing, including 1873 analysis using NGS [13]. All participants underwent pedigree analysis and medical examination. The criterion for inclusion in the study group was the presence of at least one first-degree relative with breast or ovarian cancer. Participants who had already been diagnosed with either of these cancers or who had undergone further genetic testing since the initial BRCA1/2 analysis and obtained a positive result were excluded. Thus, the analyzed cohort consisted exclusively of unaffected individuals at increased familial risk. Peripheral blood was collected from participants in the study group after they had given their informed written consent to genetic testing.
DNA was extracted from peripheral blood using the Maxwell^®^ RSC Instrument (Maxwell^®^ RSC Blood DNA Kit, Promega, Madison, WI, USA). Libraries were prepared using the Devyser BRCA NGS kit (Devyser, Stockholm, Sweden) according to the manufacturer’s instructions. Paired-end sequencing (2 × 149 bp) was performed on a MiSeq System (Illumina). The sequencing quality was assessed using the manufacturer’s software. The mean sequencing coverage was 930x for both BRCA1 and BRCA2. Samples that did not pass quality control were sequenced to obtain the required parameters. Supplementary Figure S1 provides a detailed visualization of exon-by-exon coverage (minimal, mean and maximal) for both BRCA1 and BRCA2.
CNV confirmation was performed using MLPA (Multiplex Ligation-dependent Probe Amplification (SALSA^®^ MLPA^®^ Probemix P002 BRCA1, MRC Holland, Amsterdam, The Netherlands) according to the manufacturer’s instructions. Only CNVs confirmed by MLPA were reported.
The FASTQ file was analyzed using Amplicon Suite 3.7.0 (SmartSeq), and for additional variant annotation and variant selection, we used local ANNOVAR (2019Oct24) [9]. The variants to be analyzed were prioritized according to the ClinVar prediction, the loss-of-function character, and finally the frequency in the GnomAD v4.1 reference population [14], which is below 0.01. For the analysis of CNVs from the BRCA1 and BRCA2 genes, dedicated software was applied. All statistical analyses were performed using Python (version 3.11) and the libraries NumPy [10] and SciPy [11]. The odds ratio (OR), 95% confidence intervals and p-values were calculated using a two-sided Fisher’s exact test based on 2 × 2 contingency tables.
3. Results
A total of 450 (n = 409 female, n = 41 male) unaffected individuals were included in the study group. CNV analysis was possible in only 270 patients due to data quality constraints. Detailed characteristics are shown in Table 1.
A total of 22 individuals (4.89%) were identified as carriers of pathogenic or likely pathogenic variants, including 16 carriers of BRCA1 variants (10 unique variants) and 6 carriers of BRCA2 variants (6 unique variants). Among the identified variants, 14 were classified as pathogenic by the ClinGen Expert Panel and 3 as pathogenic or likely pathogenic according to ClinVar (one of our records). The carrier frequency of BRCA1 was significantly higher in the study group than in gnomAD v4.1 (OR = 23.17; 95% CI: 13.99–38.40; p = 1.07 × 10^−16^), whereas no significant difference was observed for BRCA2 (OR = 1.88; 95% CI: 0.84–4.20; p = 0.15). Odds ratios were calculated relative to the gnomAD v4.1 European (non-Finnish) population. Figure 1 presents a schematic diagram of the obtained results. Founder mutations were observed in 7 patients, and 4 unique variants were identified. The distribution of single-nucleotide variants in the study cohort is shown in Figure 2, visualized using ProteinPaint (https://proteinpaint.stjude.org, accessed on 17 December 2025) [15].
Table 2 presents the selected variants with HGVS nomenclature, their classification and study group frequency, and the predicted protein changes.
One novel variant was identified in the BRCA1 gene (NM_007294.4:c.3837del; NP_009225.1:p.(Ser1280LeufsTer27), classified as likely pathogenic and submitted to ClinVar (VCV003384156.1). Additionally, twelve missense variants were identified, all of which had a minor allele frequency of less than 0.01 in gnomAD v4.1. Ten of these variants have conflicting interpretations in ClinVar. One variant had a VUS classification (NM_007294.4: c.1844C>A; p.(Ser615Tyr); VCV002811842.2), and the remaining variant without classification was NM_000059.4:c.190A>G p.(Thr64Ala). They were both evaluated according to the ACMG [16] and ClinGen BRCA1/2 VCEP classifications [17], and were classified as likely benign. According to the AlphaMissense [18], NM_007294.4:c.1844C>A was classified as likely benign (score: 0.119), while BRCA2:c.190A>G was classified as ambiguous (score: 0.38). Additionally, the lack of segregation was another aspect of the final decision.
4. Discussion
Our study yielded a positive result in 4.89% of cases, of which 20 were SNV variants and two were CNV mutations. This result is slightly lower than the results of other studies conducted in Poland, in which individuals underwent BRCA1/2 testing [2,3,4,19]. However, unlike previous studies that focused on affected patients, our cohort consisted entirely of unaffected individuals with a positive family history of breast and/or ovarian cancer.
Unlike BRCA1 (p = 1.07 × 10^−16^), no significant difference in carrier frequency was observed for BRCA2 (p = 0.15) when compared with gnomAD v4.1. This finding is consistent with a study by Cybulski et al., which found that variants in BRCA2 are relatively rare in familial breast cancer in Poland [20]. Consequently, the absence of statistical significance of variants for the BRCA2 gene in our dataset should be interpreted with caution, particularly in the context of population structure, penetrance differences and cohort selection. Furthermore, the insignificant p-value for BRCA2 can partly be explained by the small number of observed carriers, which reduces the accuracy of the odds ratio estimate. This limitation is inherent in analyses of rare variants, emphasizing the importance of larger sample sizes for reliably detecting moderate enrichment signals.
Furthermore, the NM_007294.4:c.5266dup variant, which is most strongly associated with breast and/or ovarian cancer in Poland, was not the most frequently observed variant in our cohort [2,3,4,19]. Nevertheless, several studies have discussed pathogenic variants in the BRCA1 and BRCA2 genes associated with reduced penetrance [21,22,23]. Finally, the inclusion of unaffected individuals in our cohort may explain the observed frequency deviation, as many of the most severely affected families were likely diagnosed earlier in other clinical centers. Thus, despite the relatively small size of the study group, our study provides additional data on a new loss-of-function variant in the BRCA1 gene (NM_007294.4:c.3837del; p.(Ser1280Leufs*27); ACMG: PVS1, PM2) and other described variants. The NM_007294.4:c.3837del variant is located in exon 10 of the BRCA1 gene. This variant was absent from the gnomAD v4.1 database. The serine cluster domain spans amino acids 1280–1524, and the variant is in position 1800 aa. Mutation of these serine residues has clinical implications and may affect the localization of BRCA1 to sites of DNA damage and the function of the DNA damage response [24].
It is worth noting that the process of detecting CNVs can be a difficult undertaking [12,25,26]. Identifying even a single CNV can have a significant impact on the further care of the patient and their family. Therefore, it is extremely important to accurately determine the exact diagnosis. Several technical challenges were encountered during CNV assessment using the Devyser BRCA NGS kit (NGS amplicon-based) in our study. Although the DNA quality and sequencing metrics (including coverage depth and Q30) were within acceptable ranges, a subset of the samples generated could not be analyzed for CNVs. We attempted to analyze DNA isolate purity parameters based on the A260/A280 spectrophotometric parameters, but this did not show a correlation with the success rate of CNV analysis from NGS data. Neither DNA concentration alone nor different reagent batches from different manufacturers had a significant impact on the success rate of CNV analysis. Consequently, it was not possible to evaluate certain samples for CNVs with confidence, which highlights the need for MLPA validation for negative samples. NGS kits based on probe enrichment may yield more reliable and reproducible CNV analysis results than those based on amplicon technology.
Given the growing number of available genetic test results, it is crucial to collect data on rare genetic variants across multiple families. These efforts could potentially lead to more reliable classification of variants, as demonstrated in the article by Caputo et al. [27]. In this context, the systematic collection of data from cohorts of unaffected individuals with a positive family history, as in the present study, can contribute to the future development of reference datasets for interpreting BRCA1/2 variants in the Polish population. However, several methodological limitations should be taken into consideration. First of all, this study did not analyze deep intronic sequences, meaning that pathogenic variants in these locations of the genome could not be detected. Furthermore, not all patients had CNVs analyzed. Secondly, the analysis only considered two genes and did not involve a broader genetic assessment (e.g., PALB2, CHEK2, ATM, RAD51C and RAD51D). This reflects the clinical and financial constraints of the testing strategy used during the study period, when BRCA1/2 testing was the only approach to screening that was reimbursed in Poland.
5. Conclusions
In conclusion, our study expands the spectrum of known genetic variants with a newly identified loss-of-function variant of BRCA1, which highlights the importance of including CNV analysis in routine BRCA1/2 screening. Identifying this variant shows that clinically relevant changes can be missed in families with no obvious history of the condition. Furthermore, failing to incorporate reliable CNV analysis into standard workflows in amplicon arrays can result in false-negative results. In such cases, diagnostics should be extended to include additional tests, such as MLPA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Petrucelli N. Daly M.B. Pal T. BRCA 1- and BRCA 2-Associated Hereditary Breast and Ovarian Cancer Gene Reviews® Adam M.P. Feldman J. Mirzaa G.M. Pagon R.A. Wallace S.E. Amemiya A. University of Washington Seattle, WA, USA 199320301425 · pubmed ↗
- 2Gronwald J. Cybulski C. Huzarski T. Jakubowska A. Debniak T. Lener M. Narod S.A. Lubinski J. Genetic Testing for Hereditary Breast Cancer in Poland: 1998–2022 Hered. Cancer Clin. Pract.202321910.1186/s 13053-023-00252-637312208 PMC 10262348 · doi ↗ · pubmed ↗
- 3Łukomska A. Menkiszak J. Gronwald J. Tomiczek-Szwiec J. Szwiec M. Jasiówka M. Blecharz P. Kluz T. Stawicka-Niełacna M. Mądry R. Recurrent Mutations in BRCA 1, BRCA 2, RAD 51C, PALB 2 and CHEK 2 in Polish Patients with Ovarian Cancer Cancers 20211384910.3390/cancers 1304084933670479 PMC 7921976 · doi ↗ · pubmed ↗
- 4Szwiec M. Jakubowska A. Górski B. Huzarski T. Tomiczek-Szwiec J. Gronwald J. Dębniak T. Byrski T. Kluźniak W. Wokołorczyk D. Recurrent Mutations of BRCA 1 and BRCA 2 in Poland: An Update Clin. Genet.20158728829210.1111/cge.1236024528374 · doi ↗ · pubmed ↗
- 5Hanson H. Astiazaran-Symonds E. Amendola L.M. Balmaña J. Foulkes W.D. James P. Klugman S. Ngeow J. Schmutzler R. Voian N. Management of Individuals with Germline Pathogenic/Likely Pathogenic Variants in CHEK 2: A Clinical Practice Resource of the American College of Medical Genetics and Genomics (ACMG)Genet. Med.20232510087010.1016/j.gim.2023.10087037490054 PMC 10623578 · doi ↗ · pubmed ↗
- 6Reiner A.S. Robson M.E. Mellemkjær L. Tischkowitz M. John E.M. Lynch C.F. Brooks J.D. Boice J.D. Knight J.A. Teraoka S.N. Radiation Treatment, ATM, BRCA 1/2, and CHEK 2 *1100 del C Pathogenic Variants and Risk of Contralateral Breast Cancer JNCI J. Natl. Cancer Inst.20201121275127910.1093/jnci/djaa 03132119081 PMC 7735763 · doi ↗ · pubmed ↗
- 7Yadav S. Boddicker N.J. Na J. Polley E.C. Hu C. Hart S.N. Gnanaolivu R.D. Larson N. Holtegaard S. Huang H. Contralateral Breast Cancer Risk Among Carriers of Germline Pathogenic Variants in ATM, BRCA 1, BRCA 2, CHEK 2, and PALB 2J. Clin. Oncol.2023411703171310.1200/JCO.22.0123936623243 PMC 10022863 · doi ↗ · pubmed ↗
- 8Arun B. Couch F.J. Abraham J. Tung N. Fasching P.A. BRCA-Mutated Breast Cancer: The Unmet Need, Challenges and Therapeutic Benefits of Genetic Testing Br. J. Cancer 20241311400141410.1038/s 41416-024-02827-z 39215191 PMC 11519381 · doi ↗ · pubmed ↗