Primary Uterine NUT Carcinoma: A Case Report and Literature Review
Tetsuro Shiraishi, Iori Kisu, Naomi Kaneko, Takaaki Fukuda, Jun Watanabe, Ryoma Hayashi, Akihisa Ueno, Katsura Emoto, Kanako Nakamura, Yuya Nogami, Kosuke Tsuji, Kenta Masuda, Wataru Yamagami

TL;DR
This paper reports the first case of primary uterine NUT carcinoma, a rare and aggressive cancer, highlighting diagnostic challenges and the importance of specific testing.
Contribution
The first documented case of primary uterine NUT carcinoma is presented, expanding the known locations of this rare cancer.
Findings
Primary uterine NUT carcinoma was confirmed through IHC and molecular testing in a postmenopausal woman.
The tumor recurred rapidly and was fatal within nine months of diagnosis.
Diagnostic challenges led to an initial misdiagnosis as undifferentiated endometrial sarcoma.
Abstract
Background: Nuclear protein in testis (NUT) carcinoma is a rare, aggressive, and poorly differentiated epithelial malignancy characterized by the rearrangement of NUTM1 (NUT midline carcinoma family member 1) on 15q14. It primarily originates along the midline structures, including the head, neck, thorax, and mediastinum. Although NUT carcinoma of the pelvic gynecological organs is exceedingly rare, reported cases have been limited to primary or metastatic ovarian tumors. Here, we present the first documented case of primary uterine NUT carcinoma. Case presentation: A 53-year-old postmenopausal woman presented with abnormal uterine bleeding and a uterine mass. She underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy. The initial postoperative histopathological evaluation suggested undifferentiated endometrial sarcoma; however, subsequent immunohistochemical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
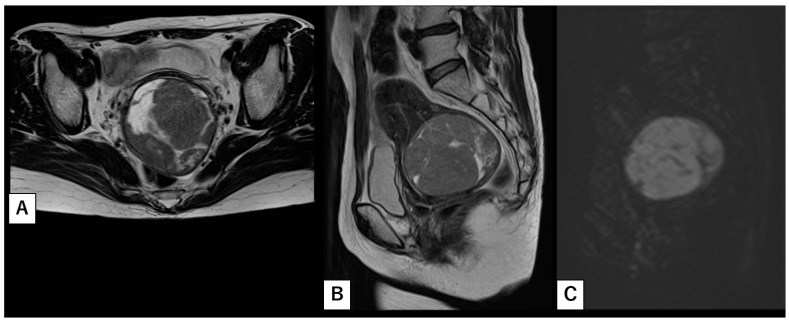 Figure 1
Figure 1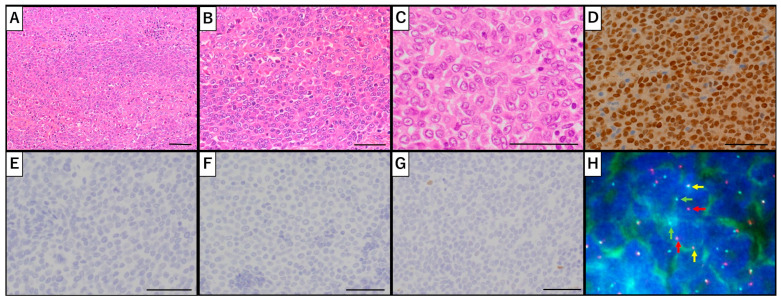 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProtein Degradation and Inhibitors · Chromatin Remodeling and Cancer · FOXO transcription factor regulation
1. Introduction
Nuclear protein in testis (NUT) carcinoma is a rare, highly aggressive, and poorly differentiated epithelial malignancy characterized by the rearrangement of NUTM1 (NUT midline carcinoma family member 1) on 15q14 [1]. It was first described in 1991 as a thymic carcinoma in young adults with a t(15;19)(q15;p13) translocation [2]. Since its initial identification, NUT carcinoma has been increasingly recognized through numerous case reports. Although it primarily arises along the midline of the body, most commonly in the head and neck, thorax, and mediastinum, it has also been reported in extramidline sites, including the lung, salivary glands, pancreas, bladder, kidney, adrenal glands, ovary, and bone [1,3,4]. Although NUT carcinoma predominantly affects adolescents and young adults, it can occur at any age, ranging from infancy to the eighth decade of life [5]. The prognosis remains extremely poor, with a median overall survival of only 6.7 months in the absence of a standardized effective therapy [6].
Only a few cases of NUT carcinoma involving pelvic gynecological organs have been reported, all of which were either primary or metastatic ovarian NUT carcinomas [4,7,8,9,10]. To the best of our knowledge, this study presents the first reported case of primary uterine NUT carcinoma.
2. Case Report
A 53-year-old postmenopausal female (para 2) presented with abnormal uterine bleeding and was referred to our institution with a suspected uterine fibroid or sarcoma. Her past medical history was unremarkable except for a previous surgical abortion. Pelvic magnetic resonance imaging (MRI) revealed a 7.4-cm mass located within the posterior wall of the lower uterine body (Figure 1A,B). Diffusion-weighted imaging (DWI) demonstrated a high signal within a cystic component, suggestive of degenerative, necrotic, or malignant tissue (Figure 1C). Given the well-defined borders of the mass and the absence of overt invasion or metastasis, our initial differential diagnosis included cellular leiomyoma and low-grade endometrial stromal sarcoma. Laboratory tests, including tumor markers (LDH 173 U/L, CEA 1.3 ng/mL, CA 19-9 13 U/mL, and CA-125 7 U/mL), were within normal limits, and both endocervical and endometrial smears were negative. Endometrial biopsy did not indicate malignancy.
Approximately 3 months after the initial referral, the patient underwent an abdominal total hysterectomy with bilateral salpingo-oophorectomy. Intraoperatively, the uterine mass was mobile and free of adhesions, extrauterine invasion, or metastasis. Histopathological evaluation revealed uniformly round tumor cells with moderate amounts of amphophilic cytoplasm and centrally located, enlarged nuclei with prominent nucleoli arranged in a loosely cohesive pattern (Figure 2A,B). Although the tumor invaded deeply into the myometrium, no evidence of extrauterine extension was observed. A broad IHC panel was performed to evaluate various uterine tumors; however, the findings remained inconclusive, with undifferentiated carcinoma, high-grade endometrial stromal sarcoma, and undifferentiated uterine sarcoma all being considered (Table 1). Subsequent review in collaboration with the pathology team revealed focal squamous differentiation (Figure 2C), prompting additional immunostaining for NUT, which demonstrated diffuse positivity (Figure 2D). Moreover, NUTM1-break-apart signals were confirmed by fluorescence in situ hybridization (FISH), which genetically proved NUTM1-rearrangement of the tumor (Figure 2H). Given the possibility that the NUT carcinoma might have originated from other sites (e.g., head and neck or thorax), a fluorodeoxyglucose positron emission tomography (FDG-PET) scan was performed; however, no abnormal FDG uptake suggestive of a primary or residual tumor was identified. Thus, a final diagnosis of primary uterine corpus NUT carcinoma was established. Ascites cytology was negative.
Considering the lack of effective postoperative treatments for NUT carcinoma, the patient was closely monitored with follow-up visits every 2 months. Six months postoperatively, small nodules were detected on the vaginal wall and pelvic floor; pathological analysis confirmed recurrent NUT carcinoma. FDG-PET further revealed disseminated nodules in the abdominal and retroperitoneal cavities, pleural metastases with associated effusions, and multiple mediastinal and cervical lymph node metastases. A computed tomography scan of the brain did not reveal any metastatic lesions. Comprehensive genomic profiling was proposed to identify potential therapeutic options; however, acknowledging the grim prognosis, the patient declined further invasive diagnostics and opted to focus solely on palliative care. Following a unilateral percutaneous nephrostomy performed for ureteral stricture secondary to pelvic seeding, she was transferred to a palliative care unit at another institution. The patient ultimately succumbed to her disease 15 months after the initial surgery.
3. Discussion
NUT carcinoma is well recognized in head and neck surgery; however, its occurrence in gynecology remains exceptionally rare. We conducted a literature review for NUT carcinoma cases in pelvic gynecological organs, including case reports, systematic reviews, meta-analyses, randomized controlled trials, and clinical trials. Various databases were consulted: all cases from Web of Science overlapped with those from PubMed, and no cases were identified from Cochrane Library (Supplementary Figure S1). Currently, only six cases of primary or metastatic ovarian NUT carcinoma have been documented (Table 2) [4,7,8,9,10,11]. To the best of our knowledge, this report represents the first case of primary uterine NUT carcinoma.
A preoperative suspicion of NUT carcinoma was Impossible. In our patient, a non-contrast MRI, performed owing to her history of asthma, suggested cellular leiomyoma or low-grade endometrial stromal sarcoma. Although gadolinium-enhanced imaging might have accentuated necrotic features within the mass, such findings could nonetheless have been interpreted as benign. In addition, normal blood tests and negative results from cytology and endometrial biopsy contributed little to clinical suspicion, leaving only intermittent uterine bleeding and a high signal on DWI as indicators of an underlying malignancy. In the absence of distant metastasis or lymphadenopathy, diagnostic surgery became the sole method to establish a definitive diagnosis.
Postoperative pathological evaluation further underscored the diagnostic challenges. NUT carcinoma typically exhibits nests and sheets of primitive round cells with prominent nucleoli, enlarged nuclei, frequent mitoses, and areas of necrosis, features that were present in our case [5]. Regarding IHC in typical NUT carcinoma, cytokeratins (AE1/AE3, CK7, CK20) are expressed in 75% of the cases, whereas p63 or p40 are observed in nearly 50%, consistent with squamous cell carcinoma. However, this indicates that cytokeratins and p40/p63 can be negative, as observed in our case. Moreover, in some cases, neuroendocrine markers (e.g., S100, synaptophysin, chromogranin A) are reported to be positive [12]. In our case, an extensive panel of IHC stains initially suggested a diagnosis of undifferentiated carcinoma, high-grade endometrial stromal sarcoma, or undifferentiated uterine sarcoma, yet none yielded a definitive diagnosis. It was only after obtaining a second pathological opinion from a specialist oncology center—where abrupt squamous differentiation, a hallmark of NUT carcinoma, was identified—that additional NUT staining was performed, revealing diffuse positivity. The NUT test is an important basis for diagnosis, showing 87% sensitivity, nearly 100% specificity, a negative predictive value of 99%, and a positive predictive value of 100% [12]. Given that squamous differentiation is observed in only about 30% of NUT carcinoma cases [13], routine NUT IHC staining is crucial when evaluating poorly differentiated malignant uterine neoplasms. Based on our experience, it is possible that some tumors previously classified as undifferentiated or dedifferentiated carcinoma, high-grade endometrial stromal sarcoma, or undifferentiated uterine sarcoma may indeed represent NUT carcinoma. Although no established treatment exists, the dismal prognosis associated with NUT carcinoma mandates prompt treatment decisions grounded in accurate diagnosis.
At the molecular level, NUT carcinoma is characterized by rearrangements of the NUTM1 gene. Recent genomic profiling has revealed that most NUTM1 fusions involve BRD4 (bromodomain-containing protein 4) on 19p13.1 (70–80%), with less frequent associations observed with BRD3 (bromodomain-containing protein 3) (15%), NSD3 (nuclear receptor binding SET domain protein 3) (6%), ZNF532/ZNF592 (Z4 zinc-finger protein family) (2%), and unidentified partners (7%) [14,15,16,17]. However, diffuse positivity on NUT IHC staining does not automatically confirm NUT carcinoma, as CIC::NUTM1 sarcoma cases have also been reported since 2018 [18]. To further confirm the diagnosis, we performed FISH to analyze the CIC::NUTM1-rearrangement, which yielded negative results (Supplementary Figure S2). The differential diagnosis of CIC::NUTM1 sarcoma relies on certain key features: (1) younger age of onset, (2) higher likelihood of central nervous system involvement, (3) absence of abrupt squamous differentiation, and (4) immunohistochemical expression of ETS variant transcription factor 4 (ETV4) as well as vimentin with negative p63 and p40 [19]. In our case, these criteria also support the diagnosis of NUT carcinoma.
Primary uterine NUT carcinoma can be misdiagnosed as other undifferentiated uterine tumors owing to its rarity and histological overlap. Considering the diagnostic challenge, NUT IHC staining and molecular testing for NUTM1 rearrangement should be considered in undifferentiated uterine tumors with ambiguous histopathological features.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1French C.A. Pathogenesis of NUT midline carcinoma Annu. Rev. Pathol.2012724726510.1146/annurev-pathol-011811-13243822017582 · doi ↗ · pubmed ↗
- 2Kubonishi I. Takehara N. Iwata J. Sonobe H. Ohtsuki Y. Abe T. Miyoshi I. Novel T. Novel t(15;19)(q 15;p 13) chromosome abnormality in a thymic carcinoma Cancer Res.199151332733282040007 · pubmed ↗
- 3French C. NUT midline carcinoma Nat. Rev. Cancer 20141414915010.1038/nrc 365925688404 · doi ↗ · pubmed ↗
- 4Jung M. Kim S.I. Kim J.W. Jeon Y.K. Lee C. NUT carcinoma in the pelvic cavity with unusual pathologic features Int. J. Gynecol. Pathol.20224129229710.1097/PGP.000000000000080134166280 · doi ↗ · pubmed ↗
- 5Moreno V. Saluja K. Pina-Oviedo S. NUT Carcinoma: Clinicopathologic features, Molecular Genetics and epigenetics Front. Oncol.20221286083010.3389/fonc.2022.86083035372003 PMC 8966081 · doi ↗ · pubmed ↗
- 6Bauer D.E. Mitchell C.M. Strait K.M. Lathan C.S. Stelow E.B. Lüer S.C. Muhammed S. Evans A.G. Sholl L.M. Rosai J. Clinicopathologic features and long-term outcomes of NUT midline carcinoma Clin. Cancer Res.2012185773577910.1158/1078-0432.CCR-12-115322896655 PMC 3473162 · doi ↗ · pubmed ↗
- 7Jiang H. Wang C. Hou Z. Wang Y. Qiao J. Li H. Case report: NUT carcinoma with MXI 1::NUTM 1 fusion characterized by abdominopelvic lesions and ovarian masses in a middle-aged female Front. Oncol.202212109187710.3389/fonc.2022.109187736741693 PMC 9890191 · doi ↗ · pubmed ↗
- 8Stevens T.M. Morlote D. Xiu J. Swensen J. Brandwein-Weber M. Miettinen M.M. Gatalica Z. Bridge J.A. NUTM 1-rearranged neoplasia: A multi-institution experience yields novel fusion partners and expands the histologic spectrum Mod. Pathol.20193276477310.1038/s 41379-019-0206-z 30723300 PMC 8194366 · doi ↗ · pubmed ↗