Technology-Enabled (P)rehabilitation for Patients Undergoing Cancer Surgery: A Systematic Review and Meta-Analysis
Tiffany R. Tsoukalas, Zirong Bai, Claire Jeon, Roy Huynh, Eva Gu, Kate Alexander, Paula R. Beckenkamp, Adrian Boscolo, Kilian Brown, Phyllis Butow, Sharon Carey, Fang Chen, Meredith Cummins, Haryana M. Dhillon, Vesna Dragoje, Kailey Gorman, Matthew Halpin, Abby Haynes

TL;DR
Using technology to support pre- and post-surgery care for cancer patients can reduce hospital stays and improve pain, depression, and fatigue, but more research is needed.
Contribution
This study is the first systematic review and meta-analysis to evaluate the effectiveness of technology-enabled (p)rehabilitation in cancer surgery patients.
Findings
Technology-enabled (p)rehabilitation reduces hospital length of stay by 1.33 days on average.
Improves patient-reported outcomes like pain, depression, fatigue, and distress.
Evidence is limited by small sample sizes and methodological variability.
Abstract
Preoperative and postoperative programs that incorporate exercise, nutritional support, and/or psychological care, collectively known as (p)rehabilitation, have demonstrated efficacy in improving cancer patient outcomes. Access to these programs, however, remains limited. Technology-enabled (p)rehabilitation offers a potential solution to enhance equity and continuity of care. This review evaluated the impact of technology-enabled (p)rehabilitation on perioperative and patient-reported outcomes in individuals undergoing thoracic and/or abdominopelvic cancer surgery. Seventeen randomised controlled trials, involving 1690 participants, were analysed. Findings suggest that technology-enabled (p)rehabilitation significantly reduces hospital length of stay, and improves patient reported outcomes such as pain, depression, fatigue, and distress compared with control groups. Despite these…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
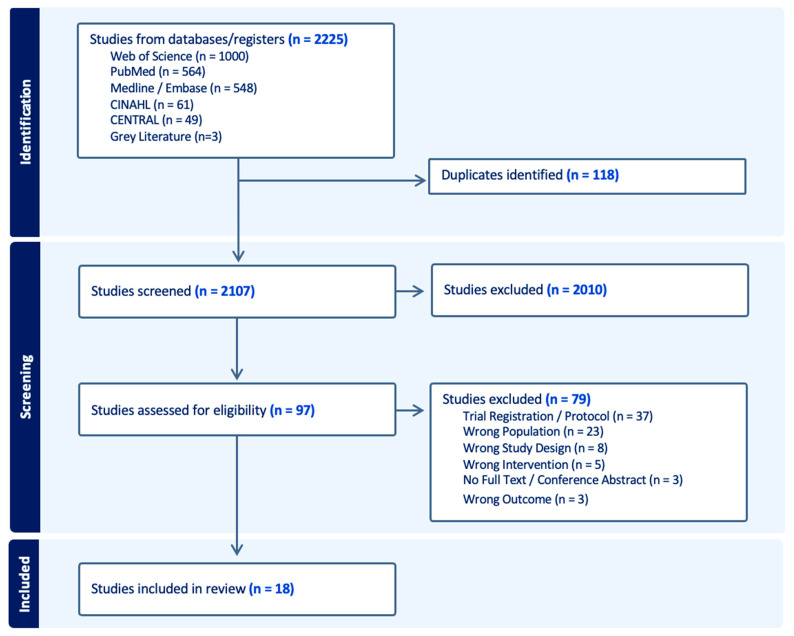 Figure 1
Figure 1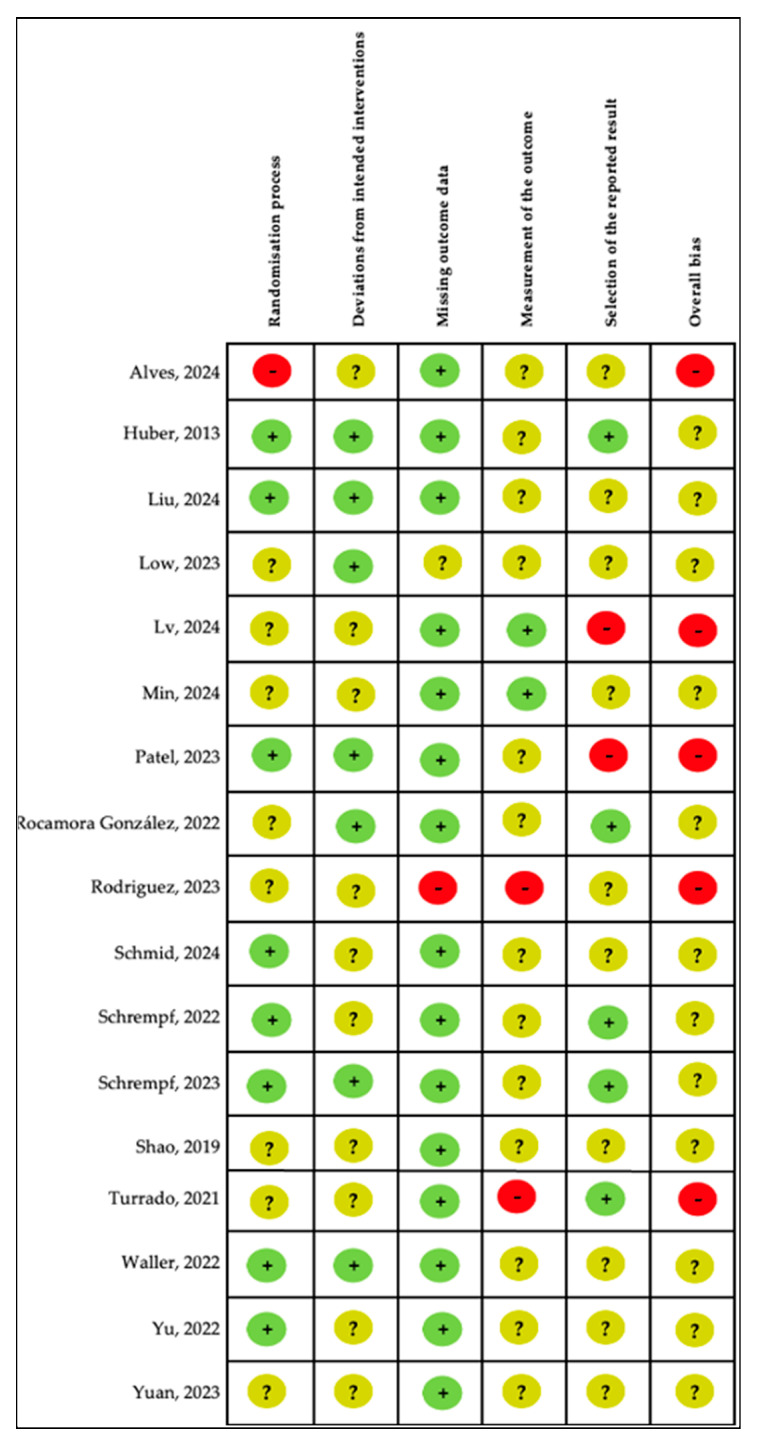 Figure 2
Figure 2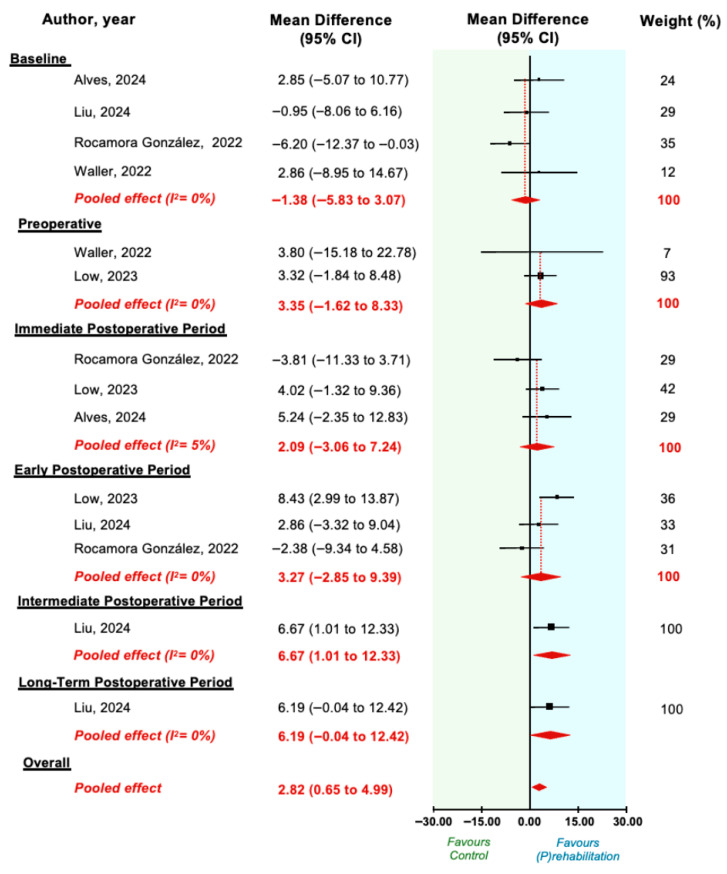 Figure 3
Figure 3- —University of Sydney Postgraduate Award (The University of Sydney)
- —Cancer Institute NSW Career Development Fellowship (Cancer Institute NSW)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Enhanced Recovery After Surgery · Frailty in Older Adults
1. Introduction
Cancer is the leading cause of death worldwide, accounting for nearly 10 million deaths in 2020 [1,2]. By 2050, its global burden is expected to rise substantially, with annual diagnosis and mortality exceeding 35 million and 18 million respectively [1,3,4].
For patients with localised disease, surgical resection, with or without adjuvant therapy, remains the cornerstone of curative treatment. However, major oncologic surgery imposes a significant physiological and psychological burden on patients. Physiologically, surgery triggers inflammatory and catabolic responses that exacerbate sarcopenia and functional decline. Psychologically, patients may experience anxiety, depression and/or emotional distress related to diagnostic uncertainty, symptom burden and prognostic concerns. Even with modern perioperative strategies, these burdens predispose patients to postoperative complications, prolonged hospitalisation, delayed functional recovery, and increased risk of hospital readmission. Collectively, these sequelae contribute to cycles of deconditioning, malnutrition, and psychological distress, adversely impacting patient outcomes, healthcare utilisation, timely access to postoperative adjuvant therapy, and long-term survivorship.
Structured prehabilitation and rehabilitation programs represent key strategies to support surgical recovery. Prehabilitation is a preoperative intervention aimed at optimising patients’ resilience, while rehabilitation is a postoperative intervention designed to support recovery and restore functional capacity. Such interventions are typically delivered as comprehensive programs combining exercise, nutritional optimisation, and psychological support. Conventional face-to-face (p)rehabilitation programs have demonstrated efficacy in improving surgical and functional outcomes across the cancer care continuum [5,6,7]. However, their implementation is often constrained by logistical barriers, including limited availability of specialised services, scheduling challenges, and geographic inaccessibility [8,9,10], which limit scalability and exacerbate inequities in access and uptake.
Technology-enabled (p)rehabilitation has emerged as a promising, scalable approach to address these implementation barriers [11]. These programs leverage digital health platforms, including synchronous telehealth consultations, asynchronous mobile applications, wearable activity monitors and biosensors, and immersive virtual reality environments, to deliver structured, multimodal care across the surgical treatment pathway. Key distinguishing features include real-time remote monitoring of physiological parameters and activity levels, automated delivery of educational content and exercise prescriptions, bidirectional communication between patients and healthcare providers, and adaptive program tailoring based on individual progress and feedback. By decentralising care delivery, technology-enabled interventions have the potential to overcome geographic barriers, reduce travel burden, enhance program adherence through convenience and personalisation, and enable continuous patient engagement throughout the perioperative period. Despite growing clinical interest, evidence for the efficacy of such programs is limited, with existing reviews primarily examining conventional, non-technology based programs [6,12] or broad cancer cohorts [6,13,14].
To address this, we conducted a systematic review and meta-analysis using the PICO framework. The population included adults undergoing elective thoracic and/or abdominopelvic cancer surgery. The intervention comprised technology-enabled prehabilitation and/or rehabilitation programs. The comparator was standard care, usual care, or non-technology-enabled (p)rehabilitation interventions. The outcomes assessed included postoperative complications, hospital length of stay, readmission rates, patient-reported outcome measures (PROMs), and patient-reported experience measures (PREMs).
2. Methods
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement [15] (Supplementary Table S1). The protocol was prospectively registered on PROSPERO (CRD42024601602).
2.1. Search Strategy
The search strategy was developed in consultation with a senior University of Sydney Librarian. Six electronic databases (PubMed, MEDLINE/EMBASE, Web of Science, CENTRAL, and CINAHL) were searched from database inception to October 2024. Forward and backward citation tracking was also performed to identify any additional eligible studies. The complete search strategy is provided in Supplementary Table S2.
2.2. Eligibility Criteria
The eligibility criteria was defined using the Population, Intervention, Comparator, Outcomes, and Study Design (PICOS) framework [16]. The target population comprised adults (≥18 years) undergoing thoracic and/or abdominopelvic cancer surgery. Interventions of interest included technology-enabled (p)rehabilitation programs. Interventions could be unimodal (exercise, nutrition, or psychosocial training/support) or multimodal (any combination). Interventions were considered technology-enabled if delivered via mobile application, web-based platform, video game, or virtual reality. For the purpose of this study (p)rehabilitation programs included interventions delivered prior to surgery (prehabilitation), and/or interventions initiated within 30 days post-index surgery (rehabilitation). No restrictions were placed on program duration or location. Eligible comparators included no intervention, placebo, minimal intervention, or non-technology-based controls. Outcomes of interest were postoperative complications, hospital readmission rates, hospital length of stay, health-related quality of life, pain, anxiety, depression, fatigue, distress, patient satisfaction. Only randomised controlled trials (RCTs) were eligible. Trials reported solely as scientific conference abstracts were excluded. No restrictions were applied on language or publication date.
2.3. Study Selection
All retrieved publications were imported into Covidence for deduplication and screening. Two reviewers independently screened titles and abstracts, followed by full-text review. Discrepancies were resolved through discussion, with a third reviewer consulted if consensus could not be reached.
2.4. Data Extraction
A piloted extraction form was used to record study characteristics (publication year, sample characteristics, target population), intervention and comparator details, and outcome measures. Where multiple publications of the same trial existed, data was consolidated to maximise completeness. Where multiple intervention groups were included, only the technology-enabled (p)rehabilitation intervention group and the control group, were included in the analysis. Non-technology-enabled intervention groups were excluded [17].
For dichotomous outcomes (e.g., postoperative complications, hospital readmissions), the number of events and participants per arm were extracted. For continuous outcomes (e.g., hospital length of stay, patient-reported outcome measures), means and standard deviations were preferentially extracted, along with the number of patients analysed in each arm.
Where medians and ranges (interquartile or minimum-maximum) were reported, data were converted to means and standard deviations using the method of Wan et al. [18]. Other data formats were transformed as necessary [17,19]. Patient-reported outcome measures were scaled to 0–100 (when required). Details of outcome transformation and standardisation are provided in Supplementary Table S3. Higher scores indicated better health-related quality of life or worse symptom severity (pain, anxiety, depression, fatigue, distress).
Data presented solely in figures were estimated to two decimal places using WebPlotDigitizer (version 5.2). Studies that reported outcomes using multivariable models (e.g., Generalised Estimating Equations) and/or presented between-group differences without effect size estimates, were excluded from pooled analysis. Excluded outcomes are detailed in Supplementary Table S4.
Outcome data were categorised into six predefined timepoints: baseline (prior to intervention), preoperative (prior to surgery), immediate postoperative (surgery day—postoperative day seven), early postoperative (one week–one month), intermediate postoperative (one–three months), and long-term postoperative (>three months) (Supplementary Table S5A,B). When multiple tools assessed the same outcome at a given timepoint, or when multiple assessments occurred within the same predefined timepoint, a prespecified prioritisation hierarchy was applied (Supplementary Table S6A,B).
2.5. Risk of Bias and Certainty of Evidence
Two reviewers (TT, ZB) independently assessed the risk of bias of included studies using Version 2 of the Cochrane Risk-of-Bias Tool for Randomised Trials (RoB2) [20]. Bias was assessed across five domains (randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results), and trials were classified as “low”, “some concerns”, or “high” risk of bias. Disagreements were resolved by discussion, with a third reviewer consulted if consensus could not be reached.
The quality and certainty of the evidence was rated accordingly to the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) [21]. Evidence was downgraded by one level according to the following criteria: (1) risk of bias (classification of one or more domain as ‘high risk’ in ≥25% of included trials); (2) inconsistency (statistically significant heterogeneity [I^2^ > 50%] or ≤75% of trials reporting results in the same direction); (3) imprecision (sample size <300 participants for dichotomous outcomes or <400 for continuous outcomes); and (4) publication bias (identified by visual assessment of funnel plots if >10 trials were included) [12]. The indirectness criterion was not considered since all studies involved thoracic and/or abdominopelvic populations, with direct comparisons and relevant outcomes. For single trials with <400 participants, inconsistency and imprecision (i.e., sparse data) were both downgraded, and the quality of evidence was rated as ‘low’ [12]. If additional risk of bias limitation were identified, the quality of the evidence could be further downgraded to ‘very low’ [12].
2.6. Data Synthesis and Analysis
All analyses were conducted using the Comprehensive Meta-Analysis software (version 4). A random effects model was applied. For dichotomous outcomes, pooled relative risks (RRs) and 95% confidence intervals (CI) were calculated. An RR < 1 indicated benefit of the intervention. For continuous outcomes, pooled mean differences (MDs) with 95% CIs were calculated. Mean differences were coded so that positive values favoured (p)rehabilitation interventions, with scores inverted for outcomes where higher values represent improved outcomes (i.e., quality of life). Statistical heterogeneity was assessed using the χ^2^ test (p < 0.10) and quantified with the I^2^ statistic, with I^2^ > 50% considered substantial heterogeneity. Where meta-analysis was not appropriate, results were reported descriptively.
3. Results
Of the 2225 publications identified, a total of 2107 were screened, with 97 undergoing full-text review. Of these, 18 publications (reporting findings from 17 unique trials) met the eligibility criteria (Figure 1). The primary reason for full-text exclusion is detailed in Supplementary Table S7.
3.1. Characteristics of Included Publications
Of the 17 included trials (n = 1690 participants), eight evaluated prehabilitation interventions exclusively [22,23,24,25,26,27,28,29], five focused solely on rehabilitation [30,31,32,33,34,35], and four incorporated both prehabilitation and rehabilitation components [36,37,38,39]. The majority of trials included patients undergoing surgery for gastrointestinal cancer. Of these, five focused on upper gastrointestinal cancer (n = 567 participants) [25,27,30,31,35,37], five on lower gastrointestinal cancer (n = 328 participants) [24,28,29,34,38], and one on metastatic gastrointestinal cancer broadly (n = 26 participants) [36]. This was followed by thoracic cancer (three trials; n = 431 participants) [23,33,39], genitourinary cancer (single trial; n = 203 participants) [22], gynaecological cancer (single trial; n = 67 participants) [26], and hepatobiliary cancer (single trial; n = 68 participants) [32]. Sample sizes ranged from 22 to 203. Detailed information of the included trials is included in Table 1, Table 2 and Table 3.
Intervention delivery modalities varied across the included trials. Application-based platforms were most frequent (n = 8), followed by virtual reality (n = 4). Web-based platforms, telehealth, videogame-based, wearable technology, and a multimedia video were each used in a single study. Across all trials, 10 incorporated psychological support, 10 physical activity, and 7 nutritional support.
3.2. Risk of Bias
The risk of bias assessment for the included trials is presented in Figure 2. Most trials presented some risk of bias. Bias due to ‘measurement of the outcomes’ and ‘selection of the reported result’ were most frequently judged to be at high risk, while ‘deviations from intended interventions’ was least commonly rated as a high risk of bias.
3.3. Certainty of Evidence
The quality and certainty of the evidence, according to the Grading of Recommendations, Assessment, Development, and Evaluations, is presented in Table 4.
3.4. Efficacy of (P)rehabilitation Programs
3.4.1. Postoperative Complications
Six trials (n = 552 participants) evaluated the impact of technology-enabled (p)rehabilitation on postoperative complications. Intervention timing varied: two trials focused on rehabilitation only, two on prehabilitation only and two combined both. Intervention components were heterogenous: two trials delivered multimodal programs incorporating physical activity, nutritional support and psychological support; two delivered a unimodal exercise program; and two delivered psychological support.
Reporting methods varied: three trials (50%) used the Clavien–Dindo classification system [33,34,38], two (33%) reported complications without formal grading [28,37], and one (17%) used the Modified Accordion Grading System [25]. Three trials solely reported ‘major complications’, defined as either Clavien–Dindo Grade ≥III (n = 2) [34,38] or ≥IIIb (n = 1) [33]. Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Table 2 and Table 3).
Four trials (67%) [28,33,34,37] reported equivalent or reduced postoperative complication events in the intervention group, compared to the control group. However, pooled analysis found no statistically significant difference between groups (RR = 0.95; 95% CI = 0.69 to 1.32; I2 = 0) (Supplementary Figure S1). The quality of evidence for this outcome was rated as low.
3.4.2. Hospital Readmission
Two trials (n = 162 participants) [33,36] investigated the effect of (p)rehabilitation interventions on 30-day hospital readmission rates. One trial delivered rehabilitation as a multimodal program incorporating physical activity, nutritional support and psychological support, while the other evaluated a combined prehabilitation and rehabilitation program focused on physical activity. Pooled analysis demonstrated no statistically significant difference between intervention and control groups (RR = 1.46; 95% CI = 0.57 to 3.76; I2 = 0) (Supplementary Figure S1). The quality of evidence for this outcome was rated as low.
3.4.3. Hospital Length of Stay
The efficacy of technology-enabled (p)rehabilitation on hospital length of stay was reported across seven trials (n = 707 participants) [23,28,30,31,34,37,38,39]. Intervention timing varied: three combined both prehabilitation and rehabilitation, two focused on rehabilitation, and two on prehabilitation. Intervention components were heterogenous: two trials delivered a unimodal exercise program, two provided psychological support, two combined physical activity with nutritional support, and one delivered a multimodal program incorporating physical activity, nutritional support and psychological support.
Pooled estimates demonstrated moderate quality evidence of a significant effect favouring (p)rehabilitation over standard care (MD = 1.33 days; 95% CI = 0.59 to 2.07; I^2^ = 4.1) (Supplementary Figure S2).
3.4.4. Health-Related Quality of Life (QoL)
Six trials (n = 501 participants) evaluated the effect of technology-enabled (p)rehabilitation on health-related quality of life. Intervention timing varied: three trials evaluated rehabilitation only, two prehabilitation only and one combined both. Intervention components ranged from unimodal programs targeting physical activity or psychological support, to combined interventions integrating nutritional support with either physical activity or psychological support.
Reporting methods varied, with each trial using a different measure. These included the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire—Core 30 (EORTC QLQ-C30; Global Health Status [32] and Summary Score [35]), EuroQol 5-Dimension 5-Level (EQ-5D-5L; Overall Health Component [23] and Index Score [34]), World Health Organisation Quality of Life (WHO QLQ; Physical Health component [24]), and the Functional Assessment of Cancer Therapy [36] (FACT). Scores were standardised to a 0–100 range to enable comparability across measures (Supplementary Table S3). Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Table 2 and Supplementary Table S4).
Overall pooled analysis demonstrated no significant effect between the control and intervention groups (MD = −0.05; 95% CI = −0.81 to 0.72). When stratified by timepoint, a significant improvement favouring (p)rehabilitation was observed at intermediate (single trial [32]; MD = 7.50; 95% CI = 0.65 to 14.35) and long-term follow-up (n = 2 trials [32,35]; MD = 9.93; 95% CI = 4.34 to 15.51) (Supplementary Figure S3).
3.4.5. Pain
Four randomised controlled trials (n = 469 participants) [23,30,33,35] evaluated the effect of technology-enabled (p)rehabilitation on postoperative pain. Three trials focused on rehabilitation, and one on prehabilitation. Across these studies, intervention components ranged from unimodal programs targeting physical activity, to combined strategies integrating nutritional support with either physical activity or psychological support. One trial delivered a multimodal program including physical activity, nutritional support and psychological support.
Reporting methods also varied, with each trial using a different measure. These included the Numeric Rating Scale, EORTC QLQ-C30 pain subscale, MD Anderson Symptom Inventory for Lung Cancer pain score, and the EQ-5D-5L pain/discomfort component. Scores were standardised to a 0–100 range to enable comparability across measures (Supplementary Table S3). Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Supplementary Table S4).
Overall pooled estimates demonstrated a significant difference between (p)rehabilitation and control groups (MD = 6.12, 95% CI = 3.40 to 8.84). When stratified by timepoint, a significant improvement favouring (p)rehabilitation was observed at immediate (n = 3 trials [23,30,33]; MD = 12.18, 95% CI = 7.19 to 17.17) and long-term follow-up (single trial [35]; MD = 8.10, 95% CI = 2.71 to 13.49). No data was available for preoperative or intermediate postoperative periods (Supplementary Figure S4).
3.4.6. Anxiety
The effect of technology-enabled (p)rehabilitation on anxiety was evaluated in seven trials (n = 640 participants) [22,24,26,27,29,30,32]. Most trials focused on prehabilitation (n = 5), with two evaluating rehabilitation. Intervention components varied: unimodal programs targeted psychological support (n = 4 trials) or physical activity (single trial), while a combined program integrated physical activity with nutritional support (single trial), and a multimodal program included physical, nutritional and psychological components (single trial).
Reporting methods also varied: four trials (n = 242 participants) used the anxiety subscale of the Hospital Anxiety and Depression Scale (HADS-A), two (n = 331 participants) used the Spielberger State-Trait Anxiety Inventory (STAI) questionnaire, and one (n = 67 participants) used a novel six-tier Visual Facial Anxiety Scale. Scores were standardised to a 0–100 range to enable comparability across measures (Supplementary Table S3). Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Table 1 and Table 2 and Supplementary Table S4).
Pooled estimates demonstrated no significant difference in anxiety between (p)rehabilitation and control groups (MD = 2.19; 95% CI = −0.08 to 4.46). Timepoint-stratified analysis indicated statistically significant reductions in anxiety at intermediate (single trial [32]; MD = 5.20; 95% CI = 0.22 to 10.18) and long-term (single trial [32]; MD = 7.62; 95% CI = 2.64 to 12.60) postoperative assessments (Supplementary Figure S5).
3.4.7. Depression
Five randomised controlled trials (n = 268) [24,29,30,32,36] assessed the impact of technology-enabled (p)rehabilitation on depression. Intervention timing varied: two trials evaluated rehabilitation only, two prehabilitation only and one combined both. Intervention components were heterogenous, comprising unimodal programs targeting either physical activity (n = 2 trials) or psychological support (n = 2 trials). One trial implemented a multimodal program including physical, nutritional and psychological components.
Four trials (n = 242) used the depression subscale of the Hospital Anxiety and Depression Scale (HADS-D), and one (n = 26) used the Centre for Epidemiological Studies Depression Scale (CES-D). Scores were standardised to a 0–100 range to enable comparability across measures (Supplementary Table S3). Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Table 2 and Supplementary Table S4).
Pooled analysis showed a statistically significant reduction in depression favouring (p)rehabilitation (MD = 2.82; 95% CI = 0.65 to 4.99). Timepoint-stratified analyses revealed no significant between-group differences at baseline, preoperative, immediate, early, or long-term postoperative timepoints. A statistically significant reduction was observed at the intermediate postoperative timepoint (single trial [32]; MD = 6.67; 95% CI = 1.01 to 12.33) (Figure 3).
3.4.8. Fatigue
Three trials (n = 374 participants) [30,33,35] evaluated the efficacy of technology-enabled (p)rehabilitation on fatigue. All trials delivered a rehabilitation program: one was a unimodal program targeting physical activity, another was a combined program integrating nutritional and psychological support, and the third was a multimodal program encompassing physical, nutritional, and psychological components.
Across included trials, reporting instruments included the Fatigue Assessment Scale, MD Anderson Symptom Inventory for Lung Cancer fatigue score and the EORTC QLQ-C30 fatigue subscale. Scores were standardised to a 0–100 range to enable comparability across measures (Supplementary Table S3). Additional instruments were reported in the included trials, but these were not included in the pooled analysis (Supplementary Table S4).
Pooled estimates demonstrated a significant reduction in fatigue favouring (p)rehabilitation over standard care (MD = 10.10; 95% CI = 6.97 to 13.23). Timepoint-stratified analyses revealed no significant between-group differences at baseline, immediate, and early postoperative periods. A statistically significant reduction in fatigue favouring (p)rehabilitation was reported at the long-term follow-up (single trial [35]; MD = 18.57; 95% CI = 13.77 to 23.37). No data were reported for the preoperative or intermediate postoperative periods (Supplementary Figure S6).
3.4.9. Distress
The efficacy of technology-enabled (p)rehabilitation on distress was evaluated in a single trial (n = 200 participants) [39], using the Huaxi Emotional-Distress Index (scored on a 0–36 scale). The trial evaluated a combined prehabilitation and rehabilitation program incorporating both physical activity and nutritional support. Statistically significant differences were reported (MD = 1.23; 95% CI = 0.30 to 2.16) (Supplementary Figure S7).
3.4.10. Patient Satisfaction
Nine of the included trials (53%) reported patient satisfaction, most commonly using brief self-reported questionnaires. Across intervention groups, satisfaction was consistently high. Five studies reported mean satisfaction scores ≥ 85% [22,24,35,36,39], one reported that 95.5% of participants rated their overall satisfaction as ≥3 on a five-point scale [33], and another reported that all participants rated the overall program as “good” or “excellent” [29]. No studies reported low satisfaction (Supplementary Table S8).
4. Discussion
This review synthesised the current evidence base on digital (p)rehabilitation in thoracic and abdominopelvic surgical oncology. Pooled analyses identified statistically significant reduction in length of hospital stay, pain, depression, fatigue and distress, but no consistent improvements were observed for postoperative complications, hospital readmissions, health-related quality of life, or anxiety. Timepoint-stratified analyses suggested improvements in health-related quality of life, pain, anxiety, depression, and fatigue mainly at later follow-up timepoints (>one month postoperatively), although these findings were largely derived from single trials.
In the present review, the absence of consistent effects on postoperative complications likely reflects the complex interplay between intervention timing and mechanistic pathways. Current evidence suggests that prehabilitation may reduce perioperative and in-hospital complications [6,11,40,41,42,43], whereas rehabilitation is primarily associated with improvements in recovery beyond the immediate postoperative period [44,45]. Aggregating prehabilitation and rehabilitation interventions under a single “(p)rehabilitation” framework may therefore obscure clinically meaningful effects. Findings from this review, particularly regarding postoperative complications, should therefore be interpreted with caution.
Findings in the present review align with prior evidence indicating that digital health interventions can enhance psychosocial outcomes. Telehealth programs for breast cancer survivors, for instance, have been associated with improved quality of life, reduced depression, lower distress, and perceived stress [46]. Similarly, digital pulmonary rehabilitation programs for lung cancer survivors have been associated with improvements in depression and anxiety [47], and digital prehabilitation programs for esophagogastric cancer cohorts have been associated with improvements in anxiety and emotional wellbeing [48]. As intervention modality is a key determinant of success [14], the accessibility and continuity of support inherent in digital programs likely underpin the observed benefits. However, interpretation of current findings is limited by the modest sample sizes and heterogeneity of included interventions. Findings from this review should therefore be interpreted with caution and further well-designed, adequately powered trials are needed to establish the most effective digital (p)rehabilitation models.
Previous systematic reviews in surgical oncology cohorts have primarily focused on conventional multimodal (p)rehabilitation (i.e., without the routine use of digital technology), with reported clinically meaningful improvements in functional recovery and reductions in complications. Notably, a large network meta-analysis by McIsaac et al. demonstrated significant benefits of multimodal prehabilitation [6]. Similarly, previous reviews of structured, in-person programs in lung cancer cohorts have reported reductions in major complications [12]. By contrast, the present review identified limited effect of (p)rehabilitation on clinical endpoints, with only a statistically significant improvement reported for length of hospital stay. This discrepancy may reflect the inherent constraints of digital interventions, particularly their inability to address postoperative complications that require in-person clinical assessment or intervention [49]. However, given the low overall certainty of evidence and high risk of bias across many included trials, further high-quality studies are needed to determine whether digital interventions can achieve comparable effects to conventional, in-person models.
Improvements in functional and exercise capacity in the present review were predominately observed at intermediate and long-term follow-up. This temporal pattern is consistent with findings from a recent meta-analysis which reported statistically significant improvements in exercise capacity at four to eight weeks postoperatively among patients receiving prehabilitation, compared with usual care [50]. Consistent with this pattern, a pilot study by Van Rooijen et al. reported that at four weeks postoperatively, 86% of patients in the prehabilitation group had returned to or exceeded their baseline functional capacity, compared with 40% of controls [51]. Collectively, these findings underscore the importance of assessing outcomes beyond the immediate postoperative period and suggest that future research should explore the optimal timing and duration of digital interventions to maximise recovery.
Despite growing evidence supporting (p)rehabilitation interventions, interpreting trial findings remains challenging due to variability in design, reporting, and outcome assessment. A persistent issue is the lack of standardisation in intervention protocols and outcome measures [11,52,53,54,55]; methodological limitations contributing to the substantial heterogeneity observed in the present review. Further complicating analysis, patient-reported outcome measures (PROMs) and patient-reported experience measures (PREMs), which are increasingly valued for capturing recovery trajectories and long-term well-being, are often underappreciated in traditional grading frameworks [56]. Such frameworks tend to prioritise objective or blinded measures, inadvertently penalising patient-centred research. As a result, studies using PROMs and PREMs were often rated as “some concerns” or “high risk” for outcome measurement, despite their established prognostic relevance in oncology research. Future studies should therefore focus on improving methodological rigour while refining grading systems to ensure that clinically meaningful outcomes, including PROMs and PREMs, are appropriately recognised and appraised.
4.1. Strengths and Limitations
This review has several methodological strengths. The protocol was pre-registered, and the review adhered to Cochrane Handbook standards. A comprehensive search strategy—developed in conjunction with a senior librarian at the University of Sydney—was applied without language restrictions. Inclusion was limited to randomised controlled trials, and risk of bias and certainty of evidence were assessed using RoB 2 and GRADE, respectively.
Nonetheless, several limitations that may affect the robustness and generalisability of the findings warrant consideration. First, the relatively small number of trials, modest sample sizes and predominance of gastrointestinal cancer trials (67%) limited statistical power and generalisability of the findings. Specifically, the small number of eligible studies precluded subgroup analyses stratified by intervention timing, modality or components, limiting the ability to discern conclusions regarding their differential effects. Second, although predefined hierarchies and published data transformations (including rescaling ordinal scale to a continuous 0 to 100 scale) were applied, these assumptions may have influenced effect estimates and introduced additional measurement error. Finally, although analyses were guided by a predefined analysis plan, time point-stratified analyses were introduced post hoc to support interpretation of outcome trajectories. To enhance transparency and methodological rigour, future studies should pre-specify all analyses.
In this review, interpretation of findings was further complicated by the limited reporting of enhanced recovery after surgery (ERAS) protocols, despite their widespread adoption in contemporary surgical care. Heterogeneity in the timing of intervention delivery, with both preoperative and postoperative interventions analysed under a single “(p)rehabilitation” construct, further complicated assessment of outcomes such as postoperative complications and readmissions. In addition, participant adherence, engagement, and digital literacy were not assessed, despite their potential role as important moderators of intervention effectiveness.
4.2. Implications for Practice and Research
Technology-enabled (p)rehabilitation appears effective in reducing hospital length of stay and improving some psychosocial outcomes, particularly at later time points. However, benefits across clinical endpoints remain inconclusive. Future research should explore hybrid models that integrate digital and face-to-face delivery, as these approaches may combine the accessibility of technology with the clinical benefits of in-person care. In parallel, studies should investigate which delivery modalities and program characteristics are most effective. Finally, incorporating co-design principles into intervention development may enhance both effectiveness and scalability, as evidence suggests this approach improves adherence, acceptability and patient experience [57,58].
Given the low quality of evidence in this review, appropriately powered RCTs are needed to confirm whether technology-enabled delivery of (p)rehabilitation is effective. To improve evidence quality and reduce heterogeneity across trials, future studies should standardise intervention components. Control groups should consistently follow enhanced recovery after surgery (ERAS) protocols, while intervention groups receive ERAS plus technology-enabled (p)rehabilitation. Trials should also pre-specify primary and secondary outcomes and employ validated outcome measures beyond the immediate perioperative period. Such rigor will enable robust comparisons and strengthen the reliability of future pooled analyses. In addition, future trials should systematically assess and report digital literacy levels of participants, system usability metrics, adherence data (including login frequency and feature utilisation), and technical difficulties encountered. Given the older demographic commonly associated with thoracic and abdominopelvic cancers, understanding these factors is essential for successful implementation and equitable access to digital health interventions. We recommend that standardised reporting frameworks for digital health interventions incorporate these metrics to facilitate meaningful evaluation of intervention feasibility and scalability across diverse populations.
Finally, ensuring equitable access and successful implementation should be integral to future research. Technology-enabled interventions must be accessible across socioeconomic, geographic and cultural contexts to avoid widening disparities. This includes addressing barriers such as language differences and digital literacy. Applying implementation frameworks can support integration into routine practice, promote sustainability and ensure alignment with health system priorities.
5. Conclusions
This review enhances the growing evidence base on technology-enabled perioperative care; a rapidly expanding field following the digital transformation of the healthcare setting. The findings suggest that technology-enabled (p)rehabilitation interventions show promise in reducing hospital length of stay and improving selected patient-reported outcomes and experience measures following thoracic and abdominopelvic cancer surgery. However, benefits across selected outcomes are often reported by single studies. Additionally, the quality of evidence is limited by the small number of studies, modest sample sizes, methodological heterogeneity, and variable intervention designs. Large-scale, adequately powered trials are needed to confirm the efficacy of technology-enabled (p)rehabilitation, identify optimal delivery models, and guide future clinical effectiveness and implementation studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Cancer: World Health Organisation 2025 Available online: https://www.who.int/news-room/fact-sheets/detail/cancer(accessed on 4 January 2026)
- 3Global Cancer Burden growing, Amidst Mounting Need for Services: World Health Organization 2024 Available online: https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services(accessed on 3 September 2025)PMC 1111539738438207 · pubmed ↗
- 4Bizuayehu H.M. Ahmed K.Y. Kibret G.D. Dadi A.F. Belachew S.A. Bagade T. Tegegne T.K. Venchiarutti R.L. Kibret K.T. Hailegebireal A.H. Global Disparities of Cancer and Its Projected Burden in 2050 JAMA Netw. Open 20247 e 244319810.1001/jamanetworkopen.2024.4319839499513 PMC 11539015 · doi ↗ · pubmed ↗
- 5Gennuso D. Baldelli A. Gigli L. Ruotolo I. Galeoto G. Gaburri D. Sellitto G. Efficacy of Prehabilitation in cancer patients: An Rcts systematic review with meta-analysis BMC Cancer 202424130210.1186/s 12885-024-13023-w 39438910 PMC 11494964 · doi ↗ · pubmed ↗
- 6Mc Isaac D.I. Kidd G. Gillis C. Branje K. Al-Bayati M. Baxi A. Grudzinski A.L. Boland L. Veroniki A.-A. Wolfe D. Relative efficacy of prehabilitation interventions and their components: Systematic review with network and component network meta-analyses of randomised controlled trials BMJ 2025388 e 08116410.1136/bmj-2024-08116439843215 PMC 11752451 · doi ↗ · pubmed ↗
- 7Coderre D. Brahmbhatt P. Hunter T.L. Baima J. Cancer Prehabilitation in Practice: The Current Evidence Curr. Oncol. Rep.2022241569157710.1007/s 11912-022-01304-135788874 · doi ↗ · pubmed ↗
- 8Pham G.T. Miegel R. Watson D.I. Bright T. Challenges of a prehabilitation program for oesophageal cancer patients in the Australian setting ANZ J. Surg.20259585285410.1111/ans.7005640040506 PMC 12105562 · doi ↗ · pubmed ↗