Palmitoylethanolamide for Nickel Allergy: Plausible, Untested, and Worth Considering
Irene Palenca, Silvia Basili Franzin, Giovanni Sarnelli, Giuseppe Esposito

TL;DR
This paper suggests palmitoylethanolamide as a potential treatment for nickel allergy, focusing on its anti-inflammatory and gut-protective properties.
Contribution
The paper proposes palmitoylethanolamide as a novel candidate for treating nickel allergy by targeting multiple pathways involved in the condition.
Findings
Palmitoylethanolamide reduces mast cell degranulation and VEGF expression.
It enhances intestinal barrier integrity and may reduce gut hyperpermeability in nickel allergy.
The molecule shows anti-inflammatory, anti-angiogenic, and anti-allergic properties relevant to nickel allergy.
Abstract
Nickel allergy remains the most prevalent cause of allergic contact dermatitis worldwide, imposing a substantial socio-epidemiological and economic burden. Beyond its classical cutaneous presentation, systemic nickel allergy syndrome highlights the systemic dimension of Nickel hypersensitivity, wherein dietary nickel intake may provoke both gastrointestinal and cutaneous symptoms through mechanisms involving gut barrier impairment and mucosal immune priming. Recent evidence highlights the contribution of angiogenesis and lymph-angiogenesis to Nickel-induced allergic contact dermatitis, through crosstalk among keratinocytes, mast cells, endothelial cells, and pro-angiogenic mediators such as vascular endothelial growth factor. Against this background, we propose to revisit palmitoylethanolamide, an endogenous ALIAmide with well-documented anti-inflammatory, anti-angiogenic, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
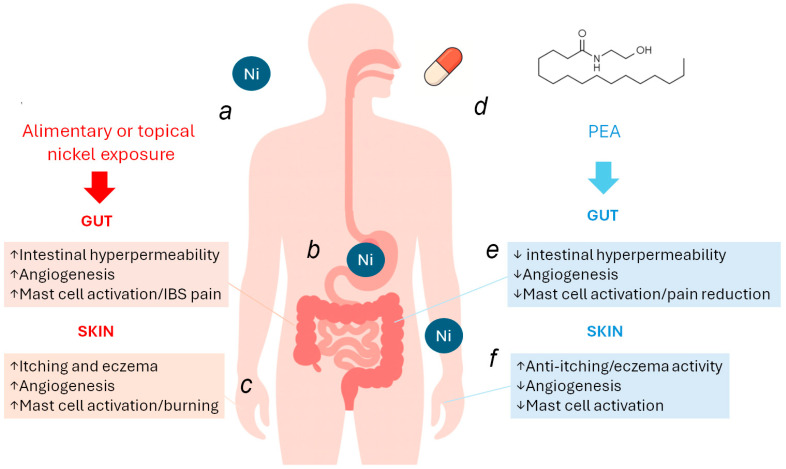 Figure 1
Figure 1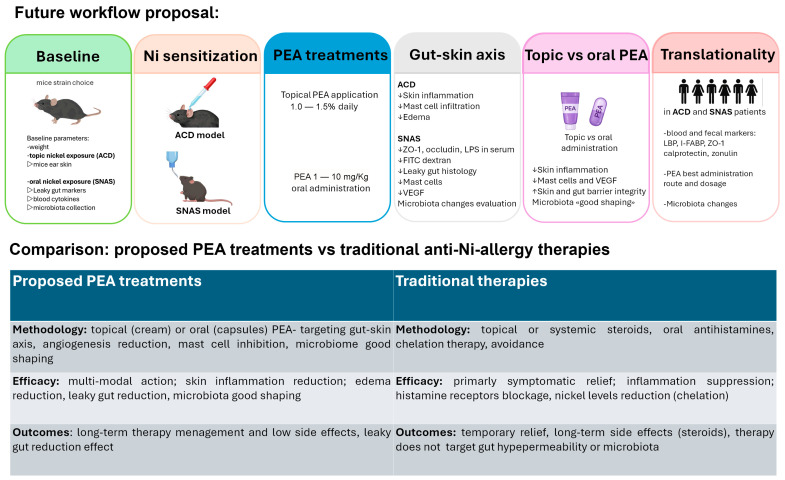 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeavy Metal Exposure and Toxicity · Mast cells and histamine · Trace Elements in Health
1. Basic Aspects of Nickel Allergy: Etiopathogenesis, Clinical Features and Current Management
Nickel (Ni) allergy remains the most common cause of allergic contact dermatitis (ACD), with prevalence rates approaching 20% in the general population [1]. Its socio-epidemiological burden is remarkable: constant exposure through jewelry, clothing fasteners, coins, cosmetics, electronic devices, and even occupational tools leads to recurrent dermatitis, reduced quality of life [2], and significant healthcare expenditures [3]. The chronicity of the condition results in absenteeism, professional impairment, and social stigma, making Ni-allergy a true public health issue rather than a mere dermatological nuisance. Beyond its classical cutaneous presentation, systemic nickel allergy syndrome (SNAS) exemplifies the systemic nature of Ni hypersensitivity, as dietary Ni ingestion can elicit gastrointestinal symptoms, such as nausea, abdominal pain, and diarrhea, alongside cutaneous manifestations like urticaria and eczema [4,5].
Management remains largely focused on restrictive low-Ni diets, which may offer symptomatic relief [6] but are often difficult to follow, nutritionally unbalanced, and socially limiting. This unmet therapeutic need emphasizes the importance of novel interventions able to act on the immunological and angiogenic mechanisms underpinning Ni hypersensitivity, improving both patient outcomes and quality of life. Mechanistically, the systemic features of SNAS have been linked to increased gastrointestinal permeability (“leaky gut”), mucosal mast cell activation, and immune sensitization occurring at the gut barrier level [7], contributing to low-grade systemic inflammation and the amplification of both GI and cutaneous symptoms in sensitized individuals.
2. Pathophysiological Mechanisms of Nickel Allergy: Angiogenesis, Mast Cells and the Gut–Skin Axis
It should be emphasized that Ni allergy is characterized not only by classical immune activation but also by marked cutaneous angiogenesis, which underlies and amplifies chronic inflammatory dermatoses. At the cutaneous level, Ni directly activates innate immunity by binding to human toll like receptor—4 (TLR4)/myeloid differentiation factor—2 (MD-2), initiating nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB)–dependent transcription of inflammatory cytokines even before antigen-specific T cell activation [8]. Keratinocytes exposed to Ni upregulate pro-angiogenic factors, such as vascular endothelial growth factor (VEGF), VEGF-C, and VEGF-D, produced by keratinocytes, fibroblasts, and resident immune cells [8,9]. These factors, in turn, stimulate endothelial proliferation, vascular permeability, and lymphangiogenesis [9,10]. Consistently, elevated VEGF levels have been documented in serum and lesional skin of ACD patients, correlating with clinical severity [11]. Moreover, mast cells, abundant in allergic infiltrates, amplify this process by releasing histamine, tryptase, and VEGF, sustaining both inflammation and vascular remodeling [12]. In parallel, Ni ingestion in SNAS promotes mucosal immune priming in the GI tract, where mast cell infiltration and barrier dysfunction trigger low-grade inflammation, epithelial permeability, and systemic sensitization [13]. The so-called “gut–skin axis” thus represents a key pathogenic bridge: local angiogenesis in cutaneous lesions mirrors mucosal vascular responses in the gut, both perpetuating the allergic phenotype and explaining why Ni allergy manifests as a combined dermatological and gastrointestinal disorder [4,7]. The “leaky gut” allows greater antigen translocation and promoting systemic sensitization. Within this inflammatory environment, pro-angiogenic mediators such as VEGF are upregulated, supporting microvascular expansion and increased vascular permeability in the intestinal wall. These vascular changes amplify immune cell recruitment and sustain chronic mucosal inflammation, helping explain the frequent overlap with irritable bowel syndrome (IBS) -like GI symptoms [5]. Clinically, a low-Ni diet has been shown to reduce these symptoms, and emerging evidence indicates that combining dietary restriction with probiotics may further modulate the gut microbiota and dampen inflammatory and angiogenic signaling [4]. Recent studies identifying structural and functional defects in the duodenal mucosal barrier reinforce the concept that Ni-driven immune activation, barrier impairment, and angiogenesis are interconnected processes [5,14]. Overall, the GI angiogenic response plays a central role in maintaining inflammation and facilitating the gut–skin axis that characterizes SNAS. Nickel-TLR4 signaling initiates inflammation-driven angiogenesis, while VEGF-dependent lymphatic remodeling facilitates antigen presentation and cellular trafficking between skin, lymph nodes, and gut. This bidirectional skin–gut axis explains why Ni allergy often presents with both dermatological and GI symptoms and suggests that targeting angiogenic pathways, alongside dietary and microbiome-based approaches, may provide therapeutic benefit. Molecules acting both at the gut and dermatological side could disrupt this pathogenic communication between the gut–skin axis and pave the way for new approaches in the treatment of SNAS. Although the gut–skin axis in nickel allergy has been clinically supported by dietary challenge studies in SNAS patients showing parallel gastrointestinal and cutaneous symptom modulation, mechanistic causality remains only partially defined [4,5,12,14]. Human evidence derives mainly from low-nickel diet intervention studies and clinical observational cohorts, while experimental data link nickel exposure to mast cell activation, barrier dysfunction, and angiogenic signaling. However, fully integrated animal models combining dietary nickel challenge with quantitative gut permeability endpoints are still limited.
3. Palmitoylethanolamide (PEA) in Current Clinical Practice: Mechanisms and Evidence Across Indications
Autacoid Local Injury Antagonists-amides, abbreviated with the acronym ALIAmides, are endogenous bioactive lipids of the N-acylethanolamine family, synthesized “on demand” in response to injury, inflammation, or cellular stress to maintain local homeostasis and prevent excessive immune activation [15]. They are produced from membrane phospholipids and converted into free NAEs such as palmitoylethanolamide (PEA) and oleoylethanolamide (OEA), while their degradation by specific enzymes (FAAH and NAAA) tightly regulates their levels and duration of action in tissues [16,17]. Among ALIAmides, PEA is the best characterized by its anti-inflammatory, analgesic, and mast-cell-modulating properties [16,17,18]. Notably, the mast cell-modulating properties of PEA are further supported by experimental evidence in ACD, where PEA levels increase locally at sites of skin inflammation and exogenous administration significantly reduces edema, inflammatory cell infiltration, and cytokine release, as demonstrated by Petrosino et al. in a well-established murine model [19]. PEA acts through Peroxisome Proliferator-Activated Receptor-alpha (PPAR-α) activation, suppressing NF-κB-driven transcription of pro-inflammatory genes, reducing VEGF/VEGFR2 signaling, and inhibiting Akt/mTOR phosphorylation, thereby exerting anti-angiogenic effects [16,20]. In addition, it stabilizes epithelial tight-junctions, counteracts oxidative stress, and restores intestinal barrier integrity, which is crucial in conditions characterized by leaky gut [13]. Clinically, PEA has shown benefits in neuropathic pain, fibromyalgia, irritable bowel syndrome, eczema, and atopic dermatitis, with an excellent safety profile supported by multiple human clinical trials and veterinary dermatology studies [21,22,23,24,25].
PEA is the most well-known ALIAmide with a well-documented high safety profile [26]. Because it is produced physiologically PEA acts as a pro-homeostatic modulator rather than as a conventional anti-inflammatory drug, and does not induce immunosuppression. Clinical and preclinical data show very low toxicity, good tolerability, and no evidence of dependency or withdrawal [25]. From a pharmacokinetic perspective, PEA is mainly degraded by NAAA and FAAH, and clinically relevant CYP-mediated drug–drug or drug-nutrients interactions have not been convincingly documented [16,25,26]. At the molecular level, PEA constitutes a heterogeneous family of endogenous lipid mediators with specific biochemical targets and therapeutic potential (Table 1). Along this line, PEA exemplifies a broad spectrum, immune regulation, mast cell modulation, barrier protection, angiogenesis inhibition, metabolic control, and satiety signaling, making it an attractive tool for chronic inflammatory and metabolic conditions, including Ni allergy, where mast cell activation, vascular remodeling, and gut–skin crosstalk converge.
Current Clinical Use of PEA: Topical and Systemic Indications
PEA is currently used in clinical practice in both topical and oral formulations across a range of inflammatory and pain-related conditions, supported by an overall favorable safety profile [25,26]. Topical PEA preparations, including creams and emollients, have been mainly evaluated in dermatological conditions characterized by inflammation, pruritus, and barrier dysfunction, such as eczema and atopic dermatitis, where they exert predominantly local effects with good tolerability [21,22,24,29]. Oral PEA, typically administered in micronized or ultramicronized formulations, has been investigated primarily in chronic and neuropathic pain conditions, with additional evidence supporting effects on gastrointestinal barrier function and inflammation-related endpoints [13,23,25]. Table 2 summarizes the current clinical indications for PEA, distinguishing topical and systemic formulations based on available evidence.
4. Rationale for the Use of PEA in Ni Allergy: Skin and Gut Target Engagement
Since PEA is an endogenous fatty acid amide that regulates inflammatory and pain signaling primarily through PPAR-α activation and mast cell down-modulation [25], its application in dermatology is particularly relevant. The skin expresses components of the endocannabinoid-related system, including PEA, which contributes to epidermal barrier homeostasis and local immune control [16]. Clinically, a randomized, double-blind, vehicle-controlled trial demonstrated that a PEA-containing emollient significantly reduced pruritus and improved clinical severity in eczema with excellent tolerability [33]. In parallel, PEA has also been shown to strengthen epithelial tight-junctions and reduce mast cell-driven mucosal inflammation in GI models relevant to SNAS [27,37], supporting a gut–skin axis mechanism in SNAS and Ni-related dermatoses (Figure 1). Current clinical investigation further reflects this therapeutic interest: NCT05003453 is evaluating a 1.5% topical PEA cream for atopic dermatitis; NCT05877170 is assessing PEA in inflammatory skin conditions [24,38]. While early data consistently indicate benefits in barrier repair, pruritus control, and neuro-immune modulation, larger, longer-duration dermatology-focused trials are needed to fully define optimal formulations and treatment algorithms. Consistent with these observations, PEA’s ability to stabilize both the skin barrier and the intestinal barrier positions it as a dual-acting mediator within the gut–skin axis, capable of addressing the dermatological manifestations of ACD and the mucosal immune dysregulation driving systemic Ni hypersensitivity. Thus, both topical and oral PEA can be conceptually integrated into therapeutic strategies aimed at protecting barrier function, modulating mast cell activity, and mitigating the cutaneous and GI consequences of Ni allergy.
5. Advantages, Limitations and Future Directions for PEA in Ni Allergy
Current standard-of-care for Ni allergy, including ACD and, in selected cases, SNAS, relies primarily on strict Ni avoidance, together with topical corticosteroids for acute flares and topical calcineurin inhibitors as steroid-sparing options. Severe or refractory cases may require short courses of systemic corticosteroids or other immunosuppressive approaches, while low-Ni diet and oral Ni hyposensitization/immunotherapy have been explored for systemic forms of the disease [1,4]. However, these strategies present important limitations: avoidance is often impractical and does not modify the underlying disease mechanisms; corticosteroids are effective in the short term but unsuitable for long-term use due to local adverse effects and, when systemic, broader toxicities; and oral Ni immunotherapy shows variable efficacy and tolerability and remains applicable only to selected patients [1,4,6].
Unlike conventional long-term therapies, particularly corticosteroids or systemic immunosuppressants, which are often limited by cumulative toxicity and tolerability issues, PEA may allow sustained symptom control with fewer safety constraints, supporting its suitability as a candidate adjunctive strategy for chronic allergic conditions such as Ni allergy, pending dedicated clinical validation [16,24,25,26].
Among ALIAmides, PEA was prioritized in this viewpoint because it is the most extensively characterized compound in this class, with direct preclinical evidence in ACD, established clinical use in inflammatory conditions, and commercially available oral and topical formulations, making it the most mature candidate for Ni allergy and SNAS. The potential use of PEA in Ni allergy rests on a strong mechanistic rationale but faces important translational challenges. On the positive side, PEA has an excellent safety profile, supported by decades of use in humans and veterinary medicine, and is generally well tolerated [21,22,23,25]. Its multimodal action, mast cell modulation [16,18], angiogenesis inhibition via PPAR-α/mTOR signaling [39], and gut barrier protection [13], aligns closely with the central mechanisms of both ACD and SNAS. Although anti-angiogenic strategies may raise concerns in specific clinical contexts such as pregnancy or active wound healing, PEA should not be considered a classical anti-angiogenic agent but rather a context-dependent modulator of inflammation-associated angiogenic signaling. Nevertheless, future studies should explicitly consider these conditions as exclusion criteria and include basic safety monitoring, such as wound healing assessment and circulating VEGF levels, when evaluating PEA in SNAS. The availability of multiple formulations represents another advantage: oral micronized and ultra-micronized preparations improve absorption [23], topical creams and gels are effective in eczema and atopic dermatitis [24], and novel carriers such as nano-formulations are under active investigation. Moreover, its dual intestinal and cutaneous efficacy positions PEA as an ideal candidate for targeting the gut–skin axis in systemic Ni allergy (Table 1). Importantly, PEA is not proposed as a direct microbiome- or strain-specific modulator. Rather, its potential relevance to microbiome-related processes in SNAS is framed in terms of host-directed mechanisms, including intestinal barrier restoration and immune modulation, which may secondarily influence microbiome-associated functional outputs. The proposed combined topical and oral use of PEA is based on compartment-specific mechanisms along the gut–skin axis, whereby topical formulations primarily exert local cutaneous effects, while oral micronized formulations provide intestinal and systemic availability sufficient for mucosal immune and barrier modulation. On the other hand, major limitations must be acknowledged. To date, no clinical trial has directly evaluated PEA in Ni-induced ACD or SNAS, meaning its efficacy remains hypothetical. The heterogeneity of Ni allergy phenotypes, ranging from localized dermatitis to systemic syndromes, complicates trial design and patient stratification [4,5,6]. Oral bioavailability, though improved, remains variable, and inter-individual differences in metabolism may limit efficacy [23]. From a regulatory perspective, PEA is classified mainly as a nutraceutical or cosmetic; thus, therapeutic claims would require robust randomized controlled trials, which are costly and time-consuming. Finally, the proposed additive role of PEA requires careful evaluation, since current standard management, primarily low-Ni diets, already provides clinical benefit, and it remains to be demonstrated whether PEA can offer meaningful incremental efficacy. Within this context of phenotypic heterogeneity and translational uncertainty, a mechanistically informed stratification framework becomes essential for any future evaluation of PEA in SNAS. To enable mechanistic validation and translational consistency, future studies evaluating PEA in SNAS should integrate functional measures of intestinal permeability with circulating and tissue-level biomarkers of epithelial integrity and immune activation. Table 3 summarizes candidate biomarkers and assays applicable across preclinical and clinical settings. A proposed mechanistic research workflow integrating preclinical and clinical validation steps is summarized in Figure 2.
6. Conclusions
Ni allergy and SNAS represent complex inflammatory conditions in which immune activation, mast cell signaling, angiogenesis, and intestinal barrier dysfunction converge along a gut–skin axis. Despite their high prevalence, current management strategies remain largely based on avoidance measures and dietary restriction, underscoring the need for adjunctive, mechanism-based approaches. Within this framework, PEA emerges as a biologically plausible and translationally accessible candidate. Its established safety profile, combined with documented anti-inflammatory, mast cell–modulating, anti-angiogenic, and barrier-protective properties, supports its consideration as an adjunct strategy for both cutaneous and gastrointestinal manifestations of Ni hypersensitivity. At the same time, the absence of direct clinical trials in Ni allergy or SNAS represents a critical gap. Future research should prioritize well-designed preclinical models and randomized controlled trials specifically addressing Ni-induced disease, incorporating objective biomarkers of barrier integrity and endotoxin-driven inflammation, together with standardized dermatological and gastrointestinal outcomes. Such studies will be essential to determine whether the mechanistic promise of palmitoylethanolamide translates into meaningful clinical benefit for patients with Ni allergy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahlström M.G. Thyssen J.P. Wennervaldt M. MennéT. Johansen J.D. Nickel Allergy and Allergic Contact Dermatitis: A Clinical Review of Immunology, Epidemiology, Exposure, and Treatment Contact Dermat.20198122724110.1111/cod.1332731140194 · doi ↗ · pubmed ↗
- 2Torres F. das Graças M. Melo M. Tosti A. Management of Contact Dermatitis Due to Nickel Allergy: An Update Clin. Cosmet. Investig. Dermatol.20092394810.2147/ccid.s 369321436967 PMC 3047925 · doi ↗ · pubmed ↗
- 3Silverberg N.B. Pelletier J.L. Jacob S.E. Schneider L.C. Section on Dermatology, Section on Allergy and Immunology Nickel Allergic Contact Dermatitis: Identification, Treatment, and Prevention Pediatrics 2020145 e 2020062810.1542/peds.2020-062832341178 · doi ↗ · pubmed ↗
- 4Lombardi F. Fiasca F. Minelli M. Maio D. Mattei A. Vergallo I. Cifone M.G. Cinque B. Minelli M. The Effects of Low-Nickel Diet Combined with Oral Administration of Selected Probiotics on Patients with Systemic Nickel Allergy Syndrome (SNAS) and Gut Dysbiosis Nutrients 202012104010.3390/nu 1204104032283870 PMC 7230804 · doi ↗ · pubmed ↗
- 5Rizzi A. Nucera E. Laterza L. Gaetani E. Valenza V. Corbo G.M. Inchingolo R. Buonomo A. Schiavino D. Gasbarrini A. Irritable Bowel Syndrome and Nickel Allergy: What Is the Role of the Low Nickel Diet?J. Neurogastroenterol. Motil.20172310110810.5056/jnm 1602728049864 PMC 5216640 · doi ↗ · pubmed ↗
- 6Antico A. Soana R. Nickel Sensitization and Dietary Nickel Are a Substantial Cause of Symptoms Provocation in Patients with Chronic Allergic-like Dermatitis Syndromes Allergy Rhinol.20156 e 56e 6310.2500/ar.2015.6.0109 PMC 438887825747857 · doi ↗ · pubmed ↗
- 7De Graaf N.P.J. Roffel S. Gibbs S. Kleverlaan C.J. Lopez Gonzalez M. Rustemeyer T. Feilzer A.J. Bontkes H.J. Nickel Allergy Is Associated with a Broad Spectrum Cytokine Response Contact Dermat.202388101710.1111/cod.14199 PMC 1008788036082421 · doi ↗ · pubmed ↗
- 8Schmidt M. Raghavan B. Müller V. Vogl T. Fejer G. Tchaptchet S. Keck S. Kalis C. Nielsen P.J. Galanos C. Crucial Role for Human Toll-like Receptor 4 in the Development of Contact Allergy to Nickel Nat. Immunol.20101181481910.1038/ni.191920711192 · doi ↗ · pubmed ↗