Neuropsychological Sequelae and Neuroradiological Correlates of Arachnoid Cysts in Adults: A Systematic Review
Odysseas Lorentzos, Panayiotis Patrikelis, Giuliana Lucci, Lambros Messinis, Stefanos Korfias

TL;DR
This review finds that brain cysts in adults can cause subtle cognitive issues, which may improve after surgery, and are linked to changes in nearby brain activity.
Contribution
The study systematically reviews cognitive and neuroimaging effects of arachnoid cysts in adults, highlighting cognitive domains affected and potential reversibility after surgery.
Findings
Arachnoid cysts are associated with impairments in memory, attention, and executive functions.
Functional neuroimaging shows altered cortical activity near cysts.
Some patients show cognitive improvement after surgery.
Abstract
Background/Objectives: Intracranial arachnoid cysts (Acs) are congenital, usually benign lesions that are frequently regarded as clinically silent in adulthood. Nonetheless, growing evidence indicates that Acs may be associated with subtle but measurable cognitive dysfunction. This systematic review synthesizes neuropsychological and functional neuroimaging findings in adults with intracranial Acs, with a focus on cognitive profiles, functional interactions with the adjacent cortex, and postoperative reversibility. Methods: In accordance with PRISMA 2020 guidelines, MEDLINE/PubMed and Scopus were searched for English-language studies published up to 2023 that reported neuropsychological assessments and/or functional neuroimaging in adult patients with Acs, including single-case reports, case series, and group studies with pre- and post-operative data. Results: Sixty studies met the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
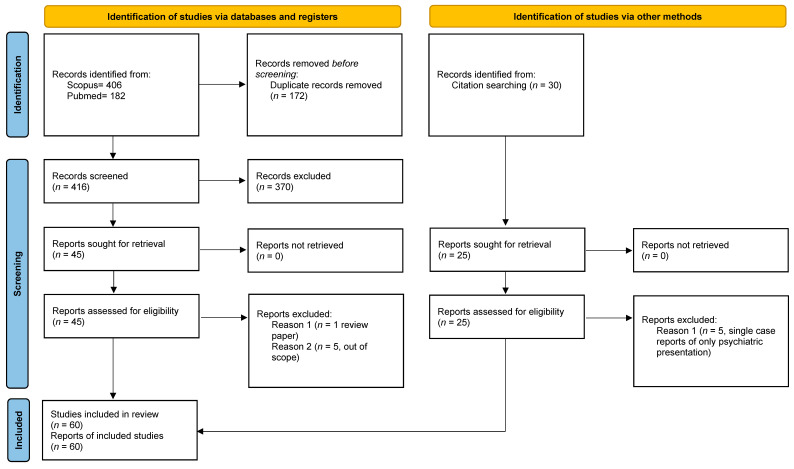 Figure 1
Figure 1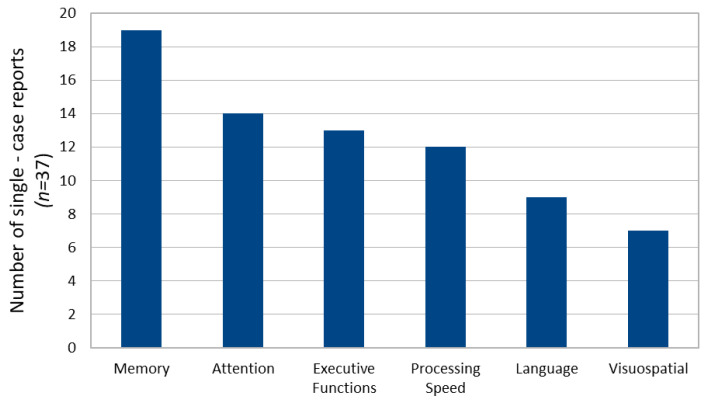 Figure 2
Figure 2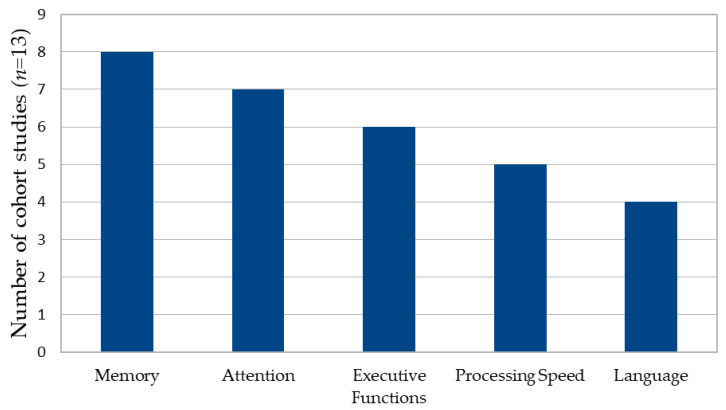 Figure 3
Figure 3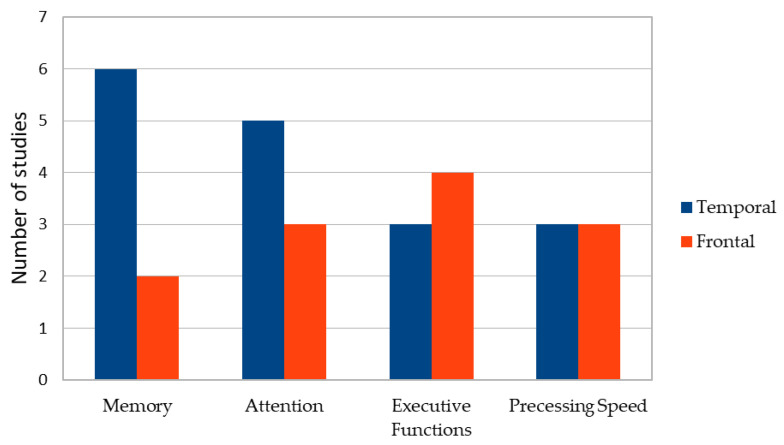 Figure 4
Figure 4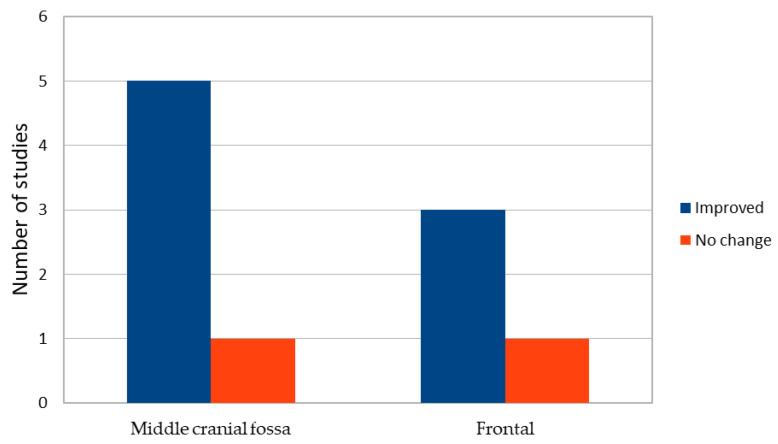 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Spinal Dysraphism and Malformations · Fetal and Pediatric Neurological Disorders
1. Introduction
Intracranial arachnoid cysts (Acs) are congenital, benign malformations characterized by the accumulation of cerebrospinal fluid-like content within the arachnoid membrane [1]. They occur more frequently in males [2] and are most commonly located in the middle cranial fossa, with a predominance in the left hemisphere, while approximately two thirds develop supratentorially [1]. Although Acs may vary considerably in size and location, epidemiological studies estimate their prevalence in adults to range between 1.4% and 2.3% [3,4], with most cases identified incidentally through neuroimaging performed for unrelated reasons [5].
The pathogenesis of Acs is generally attributed to aberrant development of the subarachnoid space during embryogenesis [6], although alternative mechanisms, including abnormalities of the meninx primitive and early disturbances of brain development, have been proposed [6]. These hypotheses have been invoked to explain the frequent association of Acs with structural alterations such as temporal lobe hypoplasia or corpus callosum anomalies, particularly in intrahemispheric cysts [6]. Nevertheless, current evidence suggests that such associations are more likely coincidental than causally related [6]. Despite their often-considerable size and the marked displacement of adjacent cortical and subcortical structures, Acs are traditionally regarded as clinically silent throughout adult life [6,7]. When symptoms occur, they most commonly include headache, dizziness, seizures, or nonspecific neurological complaints [1,8], whereas cognitive symptoms are rarely reported as primary reasons for clinical referral. However, several studies have shown that subtle cognitive alterations may emerge during systematic neuropsychological evaluation, even in patients considered neurologically asymptomatic [9,10,11].
Over the past four decades, the literature addressing the neuropsychological consequences of Acs has progressively expanded. Owing to the relatively low prevalence of these lesions, most available evidence derives from single-case reports and small case series [12,13,14,15,16], although larger cohort studies—particularly those examining pre- and post-operative cognitive outcomes—have also been published [17,18,19,20,21]. Across studies, cognitive deficits have been described in multiple domains, including verbal and visual memory and learning, attention, executive functions, processing speed, and psychomotor performance, with considerable variability depending on cyst location and size [19,20].
The apparent discrepancy between extensive structural displacement and relatively preserved everyday functioning represents one of the most intriguing aspects of Acs. This observation has prompted questions regarding the extent to which cognitive dysfunction reflects direct effects of cortical compression, altered perfusion or metabolism of adjacent tissue, or long-term compensatory and adaptive mechanisms operating during neurodevelopment [22,23,24,25,26,27]. Functional neuroimaging studies have increasingly contributed to this debate by providing evidence of altered activation patterns, metabolic changes, and preserved or displaced functional organization in regions neighboring the cyst [24,25,26,27,28,29,30].
Against this background, the present systematic review aims to identify, synthesize, and critically evaluate neuropsychological and functional neuroimaging evidence in adults with intracranial arachnoid cysts. Emphasis is placed on cognitive profiles associated with different cyst locations, evidence of functional interaction between Acs and adjacent cortex, and the extent to which cognitive deficits may be reversible following surgical intervention.
2. Materials and Methods
2.1. Search Strategy
This systematic review was conducted in accordance with the PRISMA 2020 guidelines for reporting systematic reviews [29]. A comprehensive literature search was performed in the MEDLINE/PubMed(National Library of Medicine, Bethesda, MD, USA) and Scopus (Elsevier, Amsterdam, The Netherlands) databases to identify studies investigating neuropsychological functioning and functional neuroimaging findings in adults with intracranial arachnoid cysts (Acs).
The search strategy included articles published in English between January 1980 and December 2023. The following search terms were used in various combinations: “arachnoid cyst”, “cognition”, “cognitive”, “neuropsychological”, “memory”, “executive functions”, “attention”, “language”, “visuospatial”, “processing speed”, “functional neuroimaging”, and “reorganization”. Database-specific syntax was adapted as necessary. In addition, the reference lists of all included articles were manually screened to identify further relevant studies.
2.2. Eligibility Criteria
Studies were included if they met the following criteria:
(i) involved adult participants (≥18 years) diagnosed with intracranial arachnoid cysts; (ii) reported neuropsychological assessment, either as comprehensive testing or domain-specific evaluation, and/or functional neuroimaging data (e.g., fMRI, PET, and SPECT); (iii) were original peer-reviewed articles, including single-case reports, case series, and observational or interventional group studies; (iv) were published in English.
Studies focusing exclusively on pediatric populations were excluded, given the distinct neurodevelopmental implications in childhood ACs, except for mixed-age studies from which adult data could be clearly extracted. Articles addressing psychiatric manifestations without reporting at least minimal neuropsychological data were excluded. Studies in which ACs were considered secondary findings or consequences of other primary neurological disorders were also excluded.
2.3. Study Selection
Two reviewers (O.L. and P.P.) independently conducted the database search and screened titles and abstracts for eligibility. Duplicate records were removed using Mendeley Reference Manager. Full-text articles were subsequently assessed for inclusion based on the predefined criteria. Any discrepancies between reviewers were resolved through discussion and consensus. The study selection process is summarized in a PRISMA flow diagram (Figure 1).
2.4. Data Extraction and Synthesis
Data were extracted independently by the two reviewers using a standardized extraction form. Extracted variables included authorship, year of publication, study design, sample characteristics, cyst location and size (when reported), neuropsychological assessment tools, functional neuroimaging methods, type of intervention (if any), and cognitive or imaging outcomes. Given the substantial heterogeneity in study design, outcome measures, reporting standards, non-overlapping assessment tools and limited variance data, a qualitative narrative synthesis was adopted rather than a quantitative meta-analysis. To quantify recurrent patterns across cognitive domains, anatomical locations, and postoperative outcomes, descriptive quantitative summaries (frequency counts and proportions at the study level) were carried out in addition to narrative synthesis, without suggesting patient-level prevalence or causal inference.
2.5. Risk of Bias and Methodological Quality Assessment
The methodological quality and risk of bias of included studies were independently assessed by two reviewers (O.L. and P.P.). Case reports and case series were evaluated using the Joanna Briggs Institute (JBI) critical appraisal checklists [30,31], whereas observational group studies were assessed using the Newcastle–Ottawa Scale (NOS) [32]. Disagreements were resolved by consensus. Given the predominance of descriptive and exploratory study designs, risk of bias was considered primarily in the interpretation of findings rather than as a basis for study exclusion.
3. Results
3.1. Study Selection and Characteristics
The literature search identified a total of 59 studies meeting the inclusion criteria. Of these, 37 were single-case reports, 13 were case series or small cohort studies, and 10 were functional neuroimaging studies employing PET, SPECT, or fMRI methodologies (1 study was tabulated in both single-case reports and neuroimaging due to the nature of the study). The study selection process is illustrated in the PRISMA flow diagram (Figure 1).Risk of bias assessments for all included studies are provided in Supplementary Materials.
Across studies, substantial heterogeneity was observed with respect to sample size, cyst location, neuropsychological assessment protocols, and outcome reporting. The extracted study characteristics and key findings are summarized in Table 1, Table 2 and Table 3.
3.2. Single Case Reports
Thirty-seven single-case reports described neuropsychological findings in adults with intracranial arachnoid cysts [3,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,27,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,64,66]. Clinical presentation varied widely and included psychiatric symptoms (e.g., psychosis, mood disorders, and obsessive–compulsive symptoms), neurological complaints (e.g., seizures, headaches, and gait disturbance), cognitive complaints, or incidental findings identified through neuroimaging.
Neuropsychological assessment methods were highly variable. In several cases (24.3%), cognition was assessed only through brief screening instruments such as the Mini-Mental State Examination (MMSE) [12,35,38,45,49,66]. Other reports (29.7%) employed domain-specific neuropsychological tests or standardized batteries targeting memory, attention, executive functions, language, or visuospatial abilities [14,34,37,40,43,51,68]. A subset of studies (45.9%) reported comprehensive neuropsychological evaluations covering multiple cognitive domains [10,11,16,27,36,42,44,50,52].
Across reports, cognitive deficits were most frequently documented in verbal, visual or episodic memory (51.4%), attention (37.8%), executive functioning (35.1%), processing speed and psychomotor performance (32.4%) see Figure 2. Language impairments were less consistently reported (24.3%) and were often subtle or task specific. In several cases (21.6%), cognitive dysfunction was observed in the absence of prominent neurological symptoms and was detected only through formal neuropsychological testing [16,27,48,52]. In single case reports descriptive cross tabulation suggested an anatomical pattern, where middle cranial fossa cysts were more often associated with memory and processing speed impairments and posterior fossa with executive and attention deficits. Frontal-only cases were few and showed heterogeneous profiles. Due to variation in reporting and assessments methods the findings are considered descriptive and hypothesis generating.
Post-intervention neuropsychological data were available in a subset of cases (32.4%), primarily following surgical decompression or shunting [9,15,19,21,36,39,41,46,50]. In these reports, partial or domain-specific cognitive improvement was frequently described (75.0%) and 25% remained unchained, although the extent and durability of improvement varied across cases.
Functional neuroimaging data reported in single-case studies included evidence of reduced regional cerebral metabolism, hypoperfusion, or electrophysiological slowing in cortical areas adjacent to the cyst [17,37,42,47,64]. These findings were observed both in surgically treated and conservatively managed cases. This synthesis consisted of heterogenous single-case studies. RoB was moderate to high due to descriptive designs, the lack of a control group and limited generalizability; however, the detailed presentation offered domain-specific insights.
3.3. Case Series and Group Studies
Thirteen studies employed case series or group-based designs to investigate neuropsychological functioning in adults with Acs [18,21,22,23,24,25,26,28,64,67,68,69,70]. Sample sizes ranged from small cohorts to larger observational studies, with most including pre- and post-operative assessments. Because cognitive outcomes were evaluated using a variety of instruments and domain definitions, cross-study aggregation of individual outcomes was methodologically incorrect, hence patient-level pooling across trials was not carried out.
Across studies, cognitive deficits were most consistently reported in memory (61.5%), attention (53.8%), executive functions (46.2%), processing speed (38.5%) and language (30.8%), with patterns varying according to cyst location and hemispheric dominance [22,23,24,25,26,64,70]. These patterns are illustrated in Figure 3. A descriptive contingency analysis at the study level demonstrated anatomical patterning of cognitive deficits (see Figure 4). Middle cranial fossa cysts (predominantly temporal) were frequently associated with memory (75%) and attentional impairments 62.5%, whereas frontal cysts were more commonly linked to deficits in executive functioning 80% and psychomotor speed 60%.
Most studies (77.8%) documented postoperative cognitive improvement, particularly in memory, attention, executive functioning, and language-related tasks [18,22,25,26,28,64,67,69]. However, not all studies reported significant postoperative changes, and some (22.2%) failed to detect measurable cognitive differences between patients and healthy controls either before or after surgery [21,68] (see Figure 5).
Language-related outcomes were specifically investigated in dichotic listening and lateralization paradigms, with findings indicating altered auditory–verbal processing preoperatively and normalization following surgical intervention in some patients [24,67].
The case series and group study synthesis included small series and observational cohorts, mostly with pre- and post-operative neuropsychological data. The overall RoB was moderate, due to the sample size and non-randomization as well as heterogeneity in the outcome. Potential sources of heterogeneity among included studies were descriptively explored, by the grouping through cyst localization, cognitive domains, and surgical status, as presented above.
3.4. Functional Neuroimaging Studies
Ten studies employed functional neuroimaging techniques to investigate brain function in adults with intracranial Acs [22,23,24,25,26,27,28,68,69,70]. Imaging modalities included PET, SPECT, and fMRI, and study designs comprised both single cases and small case series.
Functional imaging findings most commonly demonstrated altered cortical activity, metabolism, or perfusion in regions adjacent to the cyst [22,23,24,25,26,70]. Reduced regional cerebral blood flow or glucose metabolism was frequently observed in frontal or temporal cortices neighboring the lesion, particularly in symptomatic patients [25,26,70].
Language and motor paradigms investigated through fMRI generally revealed preserved functional lateralization, despite marked displacement of cortical structures [23,24,68]. In some cases, evidence of bilateral activation or intrahemispheric reorganization was reported, particularly in motor and somatosensory networks [27,69].
Overall, functional neuroimaging studies indicated that Acs may be associated with localized functional alterations in adjacent cortex, while large-scale interhemispheric reorganization appeared to be uncommon.
The overall certainty in the presented evidence across domains was estimated as low to moderate. There was higher confidence for domains that were more consistently represented (e.g., memory, attention, executive functions). Conversely there was a lower degree of certainty for less consistently reported domains (language, processing speed). Functional neuroimaging data outcomes were moderate in certainty, since imaging findings were in accordance with neuropsychological evidence, despite the small sample size. RoB was moderate due to sample size and exploratory designs, alleviated, however, partly by the imaging outcome.
4. Discussion
The present systematic review synthesizes neuropsychological and functional neuroimaging evidence on adults with intracranial arachnoid cysts (Acs), challenging the long-standing view of these lesions as uniformly benign and clinically silent. Across a heterogeneous body of literature, the findings consistently indicate that Acs may be associated with subtle but measurable cognitive dysfunction, particularly when systematic neuropsychological assessment is employed.
4.1. Cognitive Profiles and Anatomical Correlates
Across study designs, cognitive impairments were most frequently reported in domains subserved by frontal and temporal networks, including verbal and visual memory, attention, executive functions, processing speed, and psychomotor performance. This pattern aligns with the predominant localization of Acs in the middle cranial fossa and frontal convexity, regions critically involved in higher-order cognitive processing [7,9,10]. Importantly, the observed deficits were often mild and domain-specific, rarely reaching a severity that would unequivocally compromise everyday functioning. This may partly explain why cognitive symptoms are infrequently reported as primary complaints and are instead uncovered during structured neuropsychological evaluation.
Language impairments were less consistently observed and, when present, tended to be task-dependent rather than reflecting overt aphasia. Findings from dichotic listening and functional imaging studies suggest that language lateralization is generally preserved despite substantial displacement of cortical tissue [22,23,67]. These observations argue against large-scale interhemispheric reorganization and instead support the notion of functional displacement or local adaptation within the affected hemisphere.
4.2. Evidence for Reversibility and Surgical Effects
A central question in the clinical management of Acs concerns the extent to which cognitive deficits are reversible. Several case reports and cohort studies documented postoperative cognitive improvement, particularly in memory, attention, executive functioning, and language-related tasks [10,11,18,19,20]. Such findings support a causal relationship between Acs and cognitive dysfunction, consistent with earlier proposals that symptom reversibility following surgical decompression provides indirect evidence of pathogenicity [7].
However, the literature is not uniform. Some studies failed to demonstrate significant cognitive change following surgery or reported comparable neuropsychological performance between patients and controls both pre- and post-operatively [3,21]. These discrepancies likely reflect differences in cyst characteristics, patient selection, baseline cognitive reserve, assessment sensitivity, and follow-up duration. Together, these findings suggest that reversibility is not universal but may depend on whether a critical threshold of functional compromise has been exceeded.
4.3. Functional Neuroimaging and Pathophysiological Mechanisms
Functional neuroimaging studies provide important insights into the mechanisms underlying cognitive alterations in Acs. PET and SPECT investigations frequently revealed reduced regional cerebral metabolism or perfusion in cortical areas adjacent to the cyst, particularly in frontal and temporal regions [25,26,70]. These findings support the hypothesis that cognitive deficits may arise from local hypoperfusion, metabolic disruption, or altered network efficiency, rather than from gross neuronal loss.
fMRI studies further demonstrated that, despite marked anatomical displacement, functional organization is often preserved, especially for language and motor systems [23,24,25]. In some cases, bilateral activation patterns or intrahemispheric reorganization were observed, particularly within motor and somatosensory networks [25,69]. Taken together, these data point to a complex interaction between structural deformation, vascular–metabolic factors, and neuroplastic adaptation.
4.4. Compensation, Cognitive Reserve, and Threshold Effects
One of the most salient themes emerging from this review is the apparent dissociation between structural abnormality and clinical expression. Large Acs may coexist with relatively preserved cognitive functioning, suggesting the operation of long-term compensatory mechanisms. This observation is consistent with a compensation–threshold model, whereby gradual developmental displacement allows adjacent networks to adapt, preserving function until compensatory capacity is saturated [71].
Once this threshold is exceeded—due to factors such as cyst growth, increased intracystic pressure, age-related vulnerability, or comorbid pathology—cognitive symptoms may emerge. This framework may also account for the variability in surgical outcomes, as decompression may restore function only when deficits are driven by reversible physiological mechanisms rather than by entrenched network reorganization.
4.5. Clinical and Research Implications
From a clinical perspective, the findings underscore the importance of systematic neuropsychological assessment in adults with Acs, even in the absence of overt neurological symptoms. Reliance on brief screening measures alone may underestimate subtle cognitive alterations that are nonetheless relevant for quality of life and functional outcomes. Additionally, the functional neuroimaging findings indicate that cyst size alone, does not reliably predict functional compromise or surgical necessity. The more subtle physiological mechanisms proposed may underlie both compromise and recovery of cognitive function and in conjunction with neuropsychological and clinical assessment inform surgical decision making.
From a research standpoint, the literature remains limited by methodological heterogeneity and a predominance of descriptive designs. Future studies would benefit from prospective, longitudinal approaches, standardized neuropsychological batteries, and multimodal neuroimaging protocols capable of capturing both functional and structural network changes over time. In particular, the role of white matter connectivity and large-scale network dynamics remains largely unexplored and represents a critical avenue for future investigation.
4.6. Limitations
Several limitations can be identified in the scope of the present review. Firstly, there was considerable variability in the methodologies of the included studies. The assessment protocol was not consistent among studies, with some being more thorough, while others were narrower in scope. Heterogeneity was also observed regarding sample sizes and study type, with many single-case reports or small cohorts limiting the overall generalization of the findings. The same holds for the type of intervention, if any, as well as the lack of consistent reporting of outcomes or follow-ups in some instances.
Additionally, the interpretation of improvement albeit comparable in terms of cognition in most small cohort studies was not always apparent between single-case studies, thus affecting comparability and practical significance of findings. The aforementioned factors constitute the reasons that a narrative review was adopted, since data heterogeneity could not allow for a quantitative comparison amongst most studies.
5. Conclusions
The majority of neuropsychological evidence on adults presenting with ACs points to aberrant cognitive functioning. The emerging pattern of cognitive impairment varies as a function of a cyst’s anatomical location. The reported deficits are varied, ranging from verbal and visual memory and learning, attention, executive functions, speed of information processing, expressive language, and psychomotor speed. Though traditionally viewed as silent, ACs and their presumed rapport with the adjacent cortex have been subject to careful neuropsychological scrutiny. Deficit reversibility following surgery further corroborates the above “interaction” hypothesis. A compensation–threshold mechanism is alluded to since cognitive changes are subtle and likely occur without being transferred to the other hemisphere. This review highlights the need for further research to understand the relationship between ACs and cognitive functions, considering the potential for brain adaptation and functional compensation over time. While ACs are often considered benign, their impact on cognitive functions warrants careful neuropsychological assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cincu R. Agrawal A. Eiras J. Intracranial arachnoid cysts: Current concepts and treatment alternatives Clin. Neurol. Neurosurg.200710983784310.1016/j.clineuro.2007.07.01317764831 · doi ↗ · pubmed ↗
- 2Wester K. Intracranial arachnoid cysts—Do they impair mental functions?J. Neurol.20082551113112010.1007/s 00415-008-0011-y 18677648 · doi ↗ · pubmed ↗
- 3Rabiei K. Jaraj D. Marlow T. Jensen C. Skoog I. WikkelsøC. Prevalence and symptoms of intracranial arachnoid cysts: A population-based study J. Neurol.201626368969410.1007/s 00415-016-8035-126860092 · doi ↗ · pubmed ↗
- 4Al-Holou W.N. Terman S. Kilburg C. Garton H.J.L. Muraszko K.M. Maher C.O. Prevalence and natural history of arachnoid cysts in adults J. Neurosurg.201311822223110.3171/2012.10.JNS 1254823140149 · doi ↗ · pubmed ↗
- 5Weber F. Knopf H. Incidental findings in magnetic resonance imaging of the brains of healthy young men J. Neurol. Sci.2006240818410.1016/j.jns.2005.09.00816256141 · doi ↗ · pubmed ↗
- 6Massimi L. Caldarelli M. Di Rocco C. Intracranial congenital arachnoid cysts Textbook of Pediatric Neurosurgery Springer Cham, Switzerland 2020
- 7Wester K. Hugdahl K. Intracranial arachnoid cysts and mental functions Arachnoid Cysts Clinical and Surgical Management Wester K. Springer Cham, Switzerland 2018
- 8Arai H. Sato K. Wachi A. Okuda O. Takeda N. Arachnoid cysts of the middle cranial fossa: Experience with 77 patients Neurosurgery 1996391108111310.1097/00006123-199612000-000078938764 · doi ↗ · pubmed ↗