Combinatorial Analysis of CD4+Tregs, CD8+Teffs, and Inflammatory Indices Predict Response to ICI in ES-SCLC Patients
Anastasia Xagara, Konstantinos Tsapakidis, Vassileios Papadopoulos, Alexandros Kokkalis, Evangelia Chantzara, Chryssovalantis Aidarinis, Alexandros Lazarou, George Christodoulopoulos, Matina Perifanou-Sotiri, Dimitris Verveniotis, Vasiliki Rammou, Maria Smaragdi Vlachou

TL;DR
This study shows that a blood-based immune profile can predict which lung cancer patients are more likely to benefit from immunotherapy.
Contribution
A novel blood-based immune signature combining T cell ratios and inflammation markers is proposed to predict immunotherapy response in SCLC.
Findings
Higher CD8+ T effector cells and lower Treg/Teff ratios correlate with longer survival in SCLC patients.
Low Treg/Teff ratios are associated with low NLR and eosinophil levels before treatment.
The immune profile is easily obtainable and could guide therapy decisions in clinical practice.
Abstract
Small-cell lung cancer is a very aggressive form of lung cancer, and only a portion of patients benefit from new treatments that activate the immune system. Doctors currently lack simple tests that can show in advance which patients are more likely to respond. In this study, we examined routine blood measurements and specific immune cells circulating in the blood. We found that patients with a lower balance of certain regulatory immune cells compared with active immune cells, along with lower levels of inflammation markers, tended to live longer after starting immunotherapy. Our results suggest that a simple blood-based profile may help identify which patients are more likely to benefit from treatment, offering a practical tool for guiding therapy decisions and improving patient care. Background: Small-cell lung cancer (SCLC) is an aggressive type of lung cancer, and several factors…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
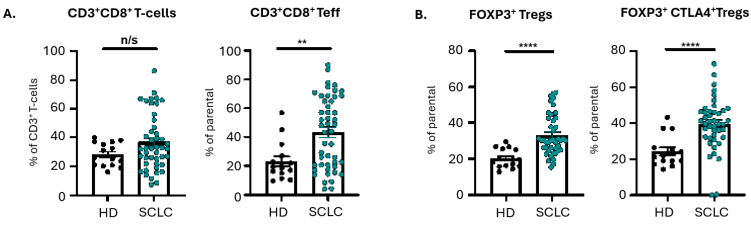 Figure 1
Figure 1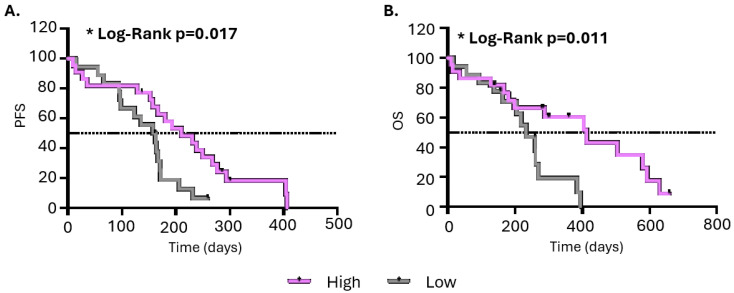 Figure 2
Figure 2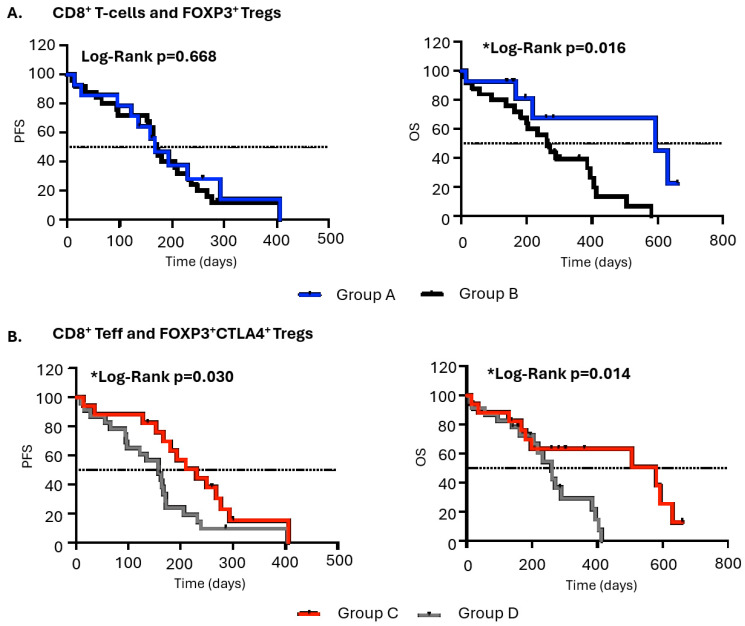 Figure 3
Figure 3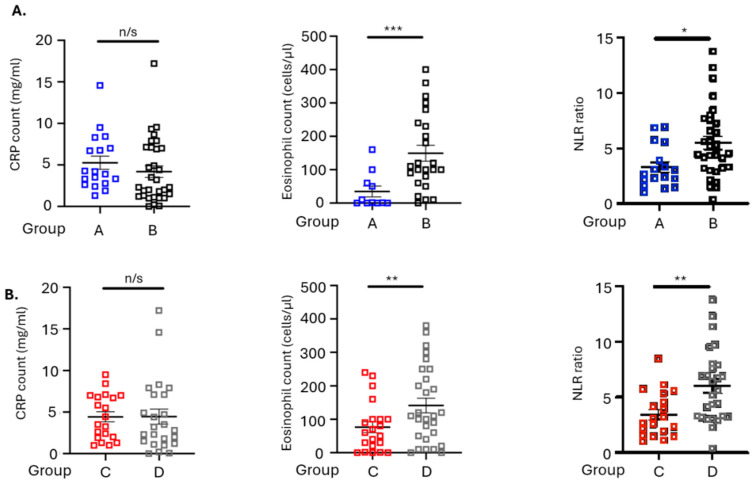 Figure 4
Figure 4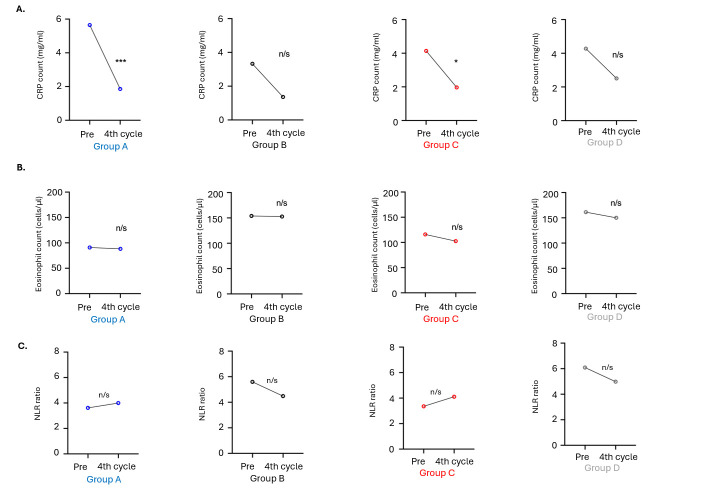 Figure 5
Figure 5- —Society of Clinical and Laboratory Research in Oncology (SCLRO)
- —project SUB3
- —Recovery and Resilience Fund and NextGenerationEU through the General Secretariat for Research and Innovation of the Hellenic Ministry of Development
- —Innovation, Technology Transfer, and Entrepreneurship Unit of the University of Thessaly “One Planet Thessaly”, within the framework of the “University of Thessaly Grants for Scientific Publication Su
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Research Studies · Cancer Immunotherapy and Biomarkers · Inflammatory Biomarkers in Disease Prognosis
1. Introduction
Lung cancer is ranked as the second-most frequently diagnosed cancer and is the leading cause of cancer-related deaths. Small-cell lung cancer (SCLC), which is typically more aggressive, accounts for 14% of all lung cancer cases [1]. Patients diagnosed with limited-stage small-cell lung cancer (SCLC) have a life expectancy of less than 24 months, while the majority of patients with extensive-stage SCLC, despite the available treatments, typically survive for no longer than 12 months [1,2]. There are several factors that can be used to predict a poor outcome, including performance status (PS), extensive-stage disease, male sex, advanced age, and high levels of lactate dehydrogenase (LDH) [2,3,4].
In certain forms of cancer, there are pre-existing inflammatory conditions before the development of malignancy [5]. On the other hand, in other types of cancer, the presence of oncogenic changes triggers an inflammatory environment that supports tumor growth [6]. Irrespective of its cause, persistent inflammation in the tumor microenvironment has various effects that promote tumor growth [6]. Further evidence suggests that heightened systemic inflammation correlates with a less favorable prognosis across multiple solid tumor types [7]. Several markers, like C-reactive protein (CRP), Glasgow Prognostic Score, neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR), are linked with poor prognosis [8,9,10,11]. These markers have also been associated with immunotherapy, which has been approved as a highly effective treatment option for various types of cancers [12].
There are numerous predictive biomarkers used to predict which tumors are more likely to respond to ICIs, like programmed death ligand 1 (PD-L1) expression and tumor mutational burden (TMB) [13]. In this context, various types of cells play a crucial role in regulating the immune response. One such cell type is regulatory T cells (Tregs), which possess the ability to suppress immune responses and exert influence on immunotherapy [14]. Finally, there is a medical need for predictive biomarkers that can be easily obtained, like CRP and neutrophil-to-lymphocyte ratio (NLR), as the absolute counts of neutrophils and lymphocytes could potentially serve as indicators of the balance between pro-tumoral inflammation and anti-tumoral immune responses [15,16].
In this study, we explored the role of Tregs in predicting immunotherapy in untreated ES-SCLC. Moreover, we evaluated the potential of inflammatory hematological indices, such as NLR and CRP levels, to predict responders.
2. Materials and Methods
2.1. Patients and Blood Collection
Fifty-one therapy-naïve patients diagnosed with extensive SCLC and fifteen matched healthy donors (HDs) were enrolled in this study. The eligibility criteria were (i) age > 18 years, (ii) histologically confirmed diagnosis of SCLC, (iii) extensive clinical stage, and (iv) no prior line of therapy. The median age of the patients was 70 years old (44–84 years). All of them were treated with first-line ICI therapy combined with carboplatin and etoposide according to NCCN guidelines. Of these patients, 35.3% had liver metastases, while 29.4% had lung metastases (Table 1). Response Evaluation Criteria in Solid Tumors (RECISTs) were used to assess response to therapy.
Peripheral blood was collected in K2 ethylenediaminetetraacetic acid (EDTA; BD Biosciences, Heidelberg, Germany) from all patients at baseline, before any treatment. Levels of CRP and NLR were recorded before treatment and before the fourth cycle of therapy. The study was conducted in line with the Ethical Principles for Medical Research Involving Human Subjects, according to the World Medical Association Declaration of Helsinki. All patients provided written informed consent in order to participate in the study, which was approved by the local ethics and scientific committees of the University General Hospital of Larissa, 41334 Larissa, Greece (32710/3-8-20, approval on 25 August 2020).
2.2. Lymphocyte Isolation and Flow Cytometry Analysis
Peripheral blood mononuclear cells (PBMCs) were isolated from all patients and healthy donors with Hypaque-1077 (Sigma-Aldich, St. Louis, MO, USA). Isolated PBMCs were then re-suspended in RPMI-1640 medium (Biosera, Nuaille, France), that was supplemented with heat-inactivated fetal bovine serum (10%) (Gibco, Grand Island, NY, USA) and penicillin and streptomycin (1%) (Solarbio, Beijing, China). Freezing of PBMCs was performed in a freezing mix containing RPMI-1640 supplemented with 20% FBS and 10% DMSO (Sigma-Aldrich, UK), and the cells were stored at −80 °C until flow cytometric analysis.
Staining of PBMCs for the detection of surface markers was performed as previously described [17]. Briefly, the following anti-human fluorochrome-conjugated monoclonal antibodies were used: anti-CD3 PE-Cy7; anti-CD4 BV510; anti-CD8 APC-Cy7; anti-CD45RA PE; anti-CD45RO APC; anti-CCR7 FITC for T lymphocytes; and anti-CD3 PE-Cy7; anti-CD4 BV510; anti-FoxP3 FITC; anti-CD25 PerCpCy5.5; anti-CD127 BV421; anti-CTLA-4 APC for Tregs (all antibodies were purchased from Biolegend, San Diego, CA, USA). Staining buffer consisted of PBS supplemented with 1% BSA, and staining was performed for 30 min on ice in the dark. BD FACSChorus v3.0 Software on a Melody flow cytometer (BD Biosciences, Heidelberg, Germany) was used for acquisition of the different T-cell populations. For each measurement, 10^6^ single-cell events were counted. Negative controls consisted of unstained cells, and FMO-stained cells were used for setting the gates (Supplementary Figure S1).
2.3. Statistical Analysis
For statistical analysis, GraphPad Prism version 10 (GraphPad Institute Inc., San Diego, CA, USA) was used. To corelate immune cell phenotypes with patients’ clinical outcomes, Kaplan–Meier analysis was performed together with the log-rank test. For this type of analysis, percentages of different T-cell types were divided into high and low groups according to receiver operating characteristic (ROC) curves cut-offs (Supplementary Figure S2). Overall survival (OS) was calculated as the number of days from patient enrollment until death or last follow-up, while progression-free survival (PFS) was defined as the number of days from patient enrolment to disease relapse or death, whichever occurred first. The nonparametric Mann–Whitney U test was used to determine differences between groups. Moreover, Pearson’s chi-square test and Fisher’s exact test were used to analyze changes in inflammatory signatures between patient groups. Differences and associations were considered significant when p < 0.05. All p-values were two-sided.
3. Results
3.1. CD8+ T Effectors and CD4+ Tregs in the Peripheral Blood of SCLC Patients
PBMCs from fifty-one treatment-naïve SCLC patients having ES-SCLC and fifteen healthy donors were analyzed by multicolor flow cytometry. SCLC patients had significantly higher percentages of CD8^+^ T effectors (p = 0.005), but not CD8^+^ T cells (p = 0.189), compared with healthy individuals. Additionally, SCLC patients had higher percentages of FOXP3^+^ Tregs (p < 0.0001) and FOXP3^+^ Tregs expressing CTLA-4 (p < 0.0001) compared with healthy donors (Figure 1).
3.2. Correlation of CD8+ T Effectors and CD4+ Tregs with Clinical Outcome
To investigate if any of the T-cell populations were correlated with clinical outcome, patients were separated into two groups bearing high or low cell populations using the cut-offs defined by ROC curves. Results indicated that high levels of CD3^+^CD8^+^ T effectors in the circulation of SCLC patients before therapy were associated with longer PFS (median: 210 vs. 161 days; p = 0.018) and longer OS (median: 412 vs. 232 days; p = 0.012) compared with patients bearing low levels. Other subtypes of CD8^+^ T cells and CD4^+^ Tregs were not found to be correlated with PFS or OS (Table 2 and Figure 2).
Additionally, correlation analysis was performed between CD8^+^ or CD8^+^ T effectors and different subtypes of CD4^+^ Tregs. CD8^+^ T cells were negatively correlated with FOXP3^+^ Tregs (Spearman r: −0.363, p = 0.018) but not with CTLA-4^+^ Tregs (Spearman r: −0.067, p = 0.684). Moreover, correlation analysis between CD8^+^T effectors and CD4^+^ Tregs indicated a significant negative correlation between CD8^+^T effectors and CTLA-4^+^ Tregs (Spearman r: −0.365, p = 0.021), but not with FOXP3^+^ Tregs (Spearman r: −0.086, p = 0.597) (Table 3).
As CD8^+^ T cells were found to be negatively correlated with FOXP3^+^ Tregs and CD8^+^T effectors with CTLA-4^+^ Tregs, patients were separated into groups as follows: for CD8^+^ T cells, group A consisted of patients with high CD8^+^ T cells (ROC cut-off) and low FOXP3^+^ Tregs (ROC cut-off) (n = 18), and group B included the rest of the patients (n = 33); for CD8^+^T effectors, group C consisted of patients with high CD8^+^ T effectors (ROC cut-off) and low CTLA-4^+^ Tregs (ROC cut-off) (n = 21), and group D included the rest of the patients (n = 30). Regarding CD8^+^ T cells, patients in group A were not correlated with PFS (p = 0.668; med: 167 days vs. 171 days; HR 0.85) but had significant longer OS (p = 0.016; med: 592 days vs. 261 days; HR 0.35) compared with group B. Additionally, patients harboring high levels of CD8^+^T effectors and low levels of CTLA-4^+^ Tregs (group C) indicated significantly longer OS (p = 0.014; med: 580 days vs. 260 days; HR 0.42) and longer PFS (p = 0.030; med: 230 days vs. 158 days; HR 0.49) compared with patients in group D (Figure 3).
3.3. Correlation of Inflammatory Signatures with Immunotherapy Response in SCLC Patients
As high percentages of CD8^+^T cells and low percentages of Tregs (group A), and high percentages of CD8^+^ Teffs with low percentages of CTLA4^+^ Tregs (group C), in circulation found to be predictive for survival under first-line ICI therapy, we next proceeded to analyze patients’ inflammatory status. Levels of inflammatory markers, including neutrophil-to-lymphocyte ratio (NLR), CRP, and eosinophils, were counted before treatment initiation and after the third therapy cycle. Kaplan–Mayer analysis of PFS and OS in patients bearing high or low baseline levels of inflammatory markers did not reveal any significant differences (Supplementary Figure S3). At baseline, patients in in group A had significantly lower levels of NLR (p = 0.0101) and eosinophil counts (p = 0.0006) compared with patients in group B, whereas CRP levels (p = 0.1406) did not differ between the two groups (Figure 4A). Moreover, patients in group C had significantly lower levels of NLR (p = 0.0398) and eosinophil counts (p = 0.0006), while CRP levels did not differ (p = 0.6033), compared with patients in group D (Figure 4B).
Changes in inflammatory markers from baseline (pretreatment) to end of the third cycle were also examined in a total of 29 patients (11 patients in group A/C and 18 patients in group B/D) for whom data were available at both time points. The results indicated a significant reduction in CRP levels from baseline to the end of the third cycle in patients in group A (p = 0.0005) and group C (p = 0.0244), but not in patients in group B (p = 0.086) and group D (p = 0.188). Levels of eosinophils and NLR were not found to have significant changes during immunotherapy in any of the four groups tested (Figure 5, Supplementary Figure S4).
4. Discussion
SCLC patients comprise a population with significant morbidity and mortality. For many years, treatment options were limited. Recently, immunotherapy has been approved for extensive-stage disease in the first-line setting. However, important questions remain regarding which category of patients benefits the most, highlighting the need for predictive biomarkers. Additionally, the role of assessing peripheral T-cell phenotypes and inflammatory indices in predicting overall survival (OS) after ICI treatment in SCLC is unclear.
In the present study, we explored the predictive value of inflammatory cells and indices in the circulation of extensive-stage SCLC patients receiving first-line immunotherapy. The results indicated higher levels of circulated T effectors and Tregs in extensive-stage SCLC patients than in healthy controls, as has been described previously [18]. A significant negative correlation between T effectors and FOXP3^+^CTLA-4^+^ Tregs, and between CD8^+^ T cells and FOXP3^+^ Tregs, in circulation before treatment initiation was observed and was further correlated with OS. Furthermore, in patients with longer OS during immunotherapy, we detected significantly lower levels of NLR and eosinophil counts before treatment initiation. CRP levels were significantly decreased during immunotherapy treatment only in the group of patients with longer OS.
Tregs are subsets of CD4^+^ T cells that express the transcription factor FoxP3 and favor tumorigenesis [19,20]. Their immunosuppressive activity is mediated by various mechanisms, thereby affecting a wide range of different immune cell types [21]. Tregs can both reduce the number and function of Teffs by secreting granzyme B, perforin, and cytokines such as IL-10 [22]. Additionally, they express high levels of inhibitory receptors such as PD-1 and CTLA-4, thereby affecting antigen presentation and reducing APC function [23]. In this study, we detected elevated levels of FOXP-3 Tregs and CTLA-4^+^FOXP-3^+^ expressing Tregs in the circulation of treatment-naïve ES-SCLC patients. Elevated levels of Tregs in circulation have been detected in various tumor types and have been correlated with worse clinical outcomes [24,25]. In SCLC, Treg levels were not predictive of ICI response. FOXP-3^+^ Tregs were also not predictive for ES-SCLC patients receiving chemotherapy, as described previously by others [18]. To our knowledge, this has not been previously described for ES-SCLC patients receiving first-line immunotherapy.
The role of CD8 T cells in targeting and eliminating cancer cells is indispensable. Teffs comprise a category of differentiated antigen-specific T cells that express perforin and are cytotoxic [26,27]. They also express ICI inhibitors such as PD-1 and CTLA-4 in response to persistent stimulus by tumor cells, which reduces their cytotoxic activity, a state called T-cell exhaustion [28]. In this study, we observed high levels of CD8^+^ Teffs in the circulation of SCLC patients compared with healthy individuals. These high levels were predictive of response to ICI regarding PFS and OS. However, further studies are needed to validate the predictive value of circulating Teffs in ICI response in SCLC patients.
Significantly, we observed a strong negative correlation between CD8^+^ Teffs and CTLA-4^+^ Tregs in circulation, which was reflected in longer OS for the subgroup of patients harboring high levels of CD8^+^ Teffs and low levels of CTLA-4^+^ Tregs. This was also the case for patients harboring high percentages of CD8^+^ T cells and low levels of FOXP3^+^ Tregs. The Treg/Teff ratio has previously been shown indicate the balance between immunosuppression and immunoactivation in cancer [29]. It has also been mentioned as a marker for disease staging in SCLC, as patients with limited-stage disease (LS-SCLC) seem to harbor a lower Treg/Teff ratio compared with ES-SCLC patients [30]. Mechanistically, it remains unclear how the balance between these two immune cell populations is regulated; however, multiple biological events play pivotal roles in their interaction [31]. Tregs direct regulate Teff cells by suppressing their function in the TME through the secretion of inhibitory cytokines (e.g., TGF-β) or by reducing their population through cytotoxic molecules (e.g., perforin) [32]. Teff metabolism is also regulated by antagonistic consumption of IL-2 by Tregs [33]. In addition, direct cell–cell interactions, mediated mainly by checkpoint inhibitors expressed on Tregs (e.g., CTLA-4), reduce the activation and activity of Teff cells [33]. Currently, the rationale for the prognostic use of this ratio is weak, as it indicates a favorable outcome in some cancer types and an unfavorable one in others [34]. To our knowledge, this study is the first to describe that a low Treg/Teff ratio is a favorable predictive factor for ES-SCLC receiving first-line ICI therapy.
Chronic inflammation promotes tumor growth and, subsequently, patients’ inflammatory state measured by blood inflammatory markers comprises a promising, easily obtained predictive tool [35]. Such measurable indices with predictive value in different cancer types include levels of the NLR, CRP, and eosinophil count [12]. None of the indices examined in this study were predictive for response to ICI at baseline. In addition, levels of the NLR and eosinophil count were significantly lower in patients in groups A and C, who were shown to have longer OS. Moreover, CRP levels were significantly reduced in both groups during ICI treatment, indicating that early changes in CRP during immunotherapy treatment could be used as a surrogate marker for early monitoring of response. This has recently been shown to be the case for other tumor types, such as NSCLC [36].
5. Conclusions
Ιn this study, we explored the predictive value of various inflammatory signatures for immunotherapy treatment in ES-SCLC patients. The data indicated higher percentages of both Teff and Treg cell populations before treatment in patients compared with healthy individuals. Importantly, a survival benefit in patients harboring a low Treg/Teff ratio, which was further accompanied by low eosinophil levels and a low NLR, a result that probably reflects an immunostimulatory environment. Although significant results are presented in the current exploratory study, several limitations exist, mainly related to the small number of patients. Future studies in larger multicenter cohorts are required to confirm, validate, and strengthen the statistical power of our findings. Moreover, due to the nature of this study, we were not able to exclude the possibility that the reduction in CRP levels during treatment is related to confounders such as infections or tumor burden. Overall, further validation in a larger cohort of ES-SCLC patients, as well as LS-SCLC patients, may offer an easily obtainable tool to select immunotherapy responders in daily clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Cancer Society Cancer Facts & Figures 2024 Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf(accessed on 4 January 2026)
- 2Hong X. Cui B. Wang M. Yang Z. Wang L. Xu Q. Systemic Immune-inflammation Index, Based on Platelet Counts and Neutrophil-Lymphocyte Ratio, Is Useful for Predicting Prognosis in Small Cell Lung Cancer Tohoku J. Exp. Med.201523629730410.1620/tjem.236.29726250537 · doi ↗ · pubmed ↗
- 3Bremnes R.M. Sundstrom S. Aasebo U. Kaasa S. Hatlevoll R. Aamdal S. Norweigian Lung Cancer Study G. The value of prognostic factors in small cell lung cancer: Results from a randomised multicenter study with minimum 5 year follow-up Lung Cancer 20033930331310.1016/S 0169-5002(02)00508-112609569 · doi ↗ · pubmed ↗
- 4Osterlind K. Factors confounding evaluation of treatment effect in lung cancer Lung Cancer 199410 S 97S 10310.1016/0169-5002(94)91672-18087532 · doi ↗ · pubmed ↗
- 5Mantovani A. Allavena P. Sica A. Balkwill F. Cancer-related inflammation Nature 200845443644410.1038/nature 0720518650914 · doi ↗ · pubmed ↗
- 6Liu D. Huang Y. Li L. Song J. Zhang L. Li W. High neutrophil-to-lymphocyte ratios confer poor prognoses in patients with small cell lung cancer BMC Cancer 20171788210.1186/s 12885-017-3893-129268698 PMC 5740933 · doi ↗ · pubmed ↗
- 7Kang M.H. Go S.I. Song H.N. Lee A. Kim S.H. Kang J.H. Jeong B.K. Kang K.M. Ling H. Lee G.W. The prognostic impact of the neutrophil-to-lymphocyte ratio in patients with small-cell lung cancer Br. J. Cancer 201411145246010.1038/bjc.2014.31724921916 PMC 4119986 · doi ↗ · pubmed ↗
- 8Crumley A.B. Mc Millan D.C. Mc Kernan M. Mc Donald A.C. Stuart R.C. Evaluation of an inflammation-based prognostic score in patients with inoperable gastro-oesophageal cancer Br. J. Cancer 20069463764110.1038/sj.bjc.660299816479253 PMC 2361199 · doi ↗ · pubmed ↗