Efficacy and Safety of HAIC Combined with PD-(L)1 Inhibitors and Bevacizumab Versus HAIC with PD-(L)1 Inhibitors and TKIs in Advanced Hepatocellular Carcinoma: A Retrospective Cohort Study
Zizhuo Wang, Wei Xu, Songlin Song, Yanqiao Ren, Jiacheng Liu, Yiming Liu, Xuefeng Kan, Chuansheng Zheng, Bin Liang

TL;DR
A study found that combining HAIC with PD-(L)1 inhibitors and bevacizumab improved outcomes in advanced liver cancer compared to using tyrosine kinase inhibitors.
Contribution
This study provides real-world evidence comparing two triplet therapies for advanced hepatocellular carcinoma in a clinical setting.
Findings
Bevacizumab-based regimen showed higher objective response rate (83.9%) compared to TKI-based regimen (61.8%).
Median progression-free survival was longer with bevacizumab (10.9 months) than with TKIs (7.4 months).
Both regimens had manageable toxicity but with distinct adverse event profiles.
Abstract
This retrospective study compared the efficacy and safety of two triplet regimens—hepatic arterial infusion chemotherapy (HAIC) plus immune checkpoint inhibitors combined with either bevacizumab or tyrosine kinase inhibitors (TKIs)—in patients with advanced hepatocellular carcinoma (HCC). Among 65 enrolled patients, the bevacizumab-based regimen suggested improved tumor control, with a higher objective response rate (83.9% vs. 61.8%) and longer median progression-free survival (10.9 vs. 7.4 months) compared to the TKI-based regimen. Both regimens exhibited manageable toxicity profiles, but with distinct adverse event profiles. These real-world findings suggest that the triple combination containing bevacizumab may offer a more effective treatment option, warranting further validation in prospective clinical trials. Background: The combination of hepatic arterial infusion chemotherapy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
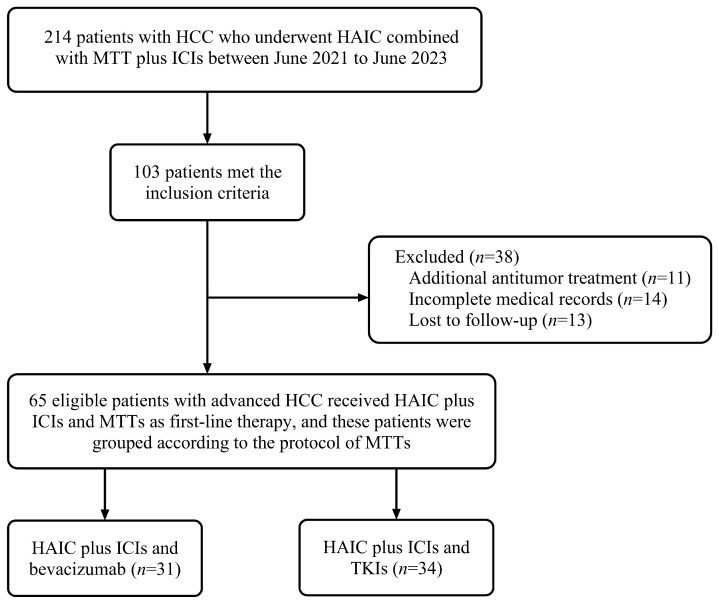 Figure 1
Figure 1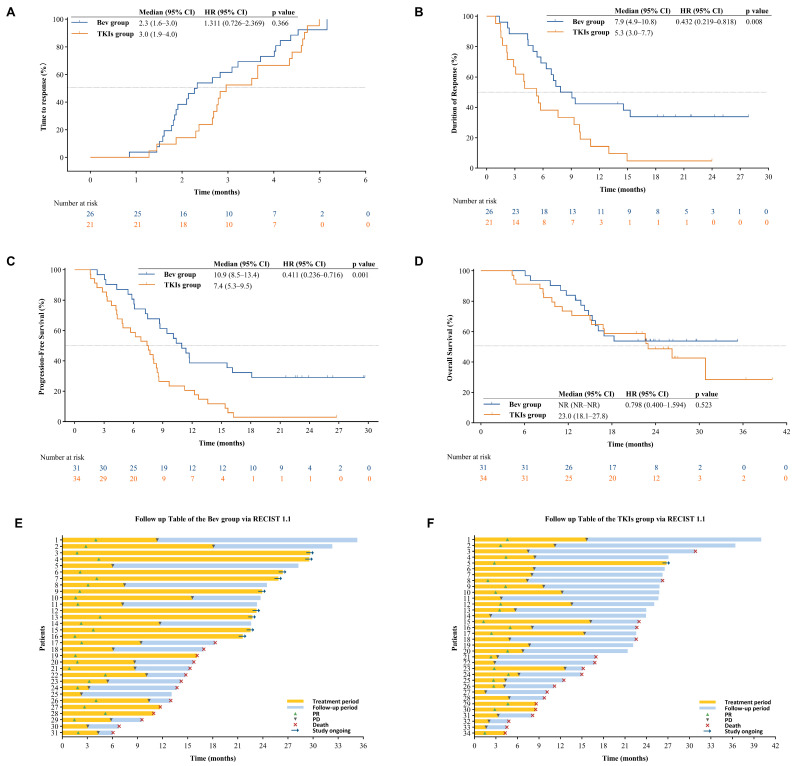 Figure 2
Figure 2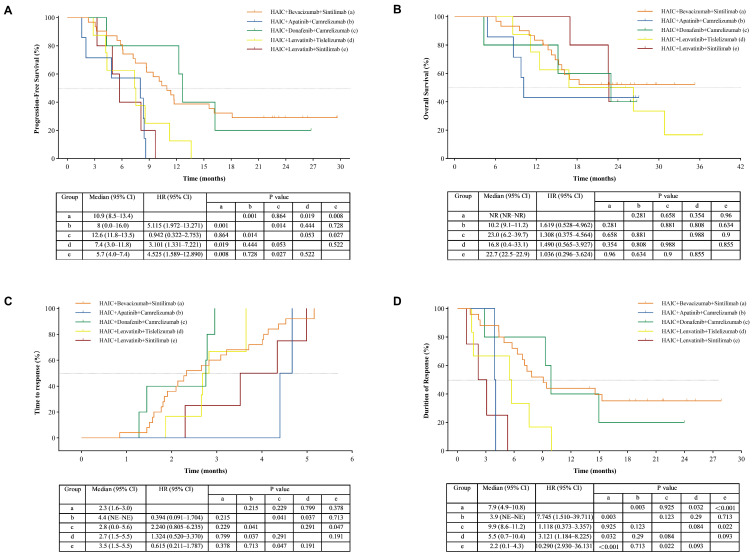 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Cholangiocarcinoma and Gallbladder Cancer Studies · Cancer Immunotherapy and Biomarkers
1. Introduction
Hepatocellular carcinoma (HCC) ranks as the sixth most prevalent malignancy globally and contributes to the third-highest cancer-related mortality, with China bearing a disproportionately high disease burden [1]. Many patients are diagnosed at an advanced stage, for whom curative treatment options are not indicated [2,3]. While current guidelines recommend combinations of immune checkpoint inhibitors (ICIs) and anti-angiogenic therapy as first-line treatment for advanced HCC, particularly those classified as Barcelona Clinic Liver Cancer (BCLC) stage C [3], the clinical outcomes remain suboptimal [3,4]. Established regimens, including atezolizumab plus bevacizumab and pembrolizumab plus lenvatinib, have median OS that seldom surpasses 24 months, highlighting a pressing need for more effective therapeutic strategies.
Hepatic arterial infusion chemotherapy (HAIC), particularly with the FOLFOX regimen, has emerged as a potent locoregional treatment that enhances systemic therapy efficacy in advanced HCC. By delivering high concentrations of chemotherapy directly to the liver, HAIC achieves potent tumor control with limited systemic exposure [5,6,7,8]. Real-world studies demonstrate that FOLFOX-HAIC combined with anti-angiogenic therapy and ICIs can lead to improved therapeutic efficacy [9,10,11,12], with median progression-free survival (PFS) showing significant enhancements over conventional therapy combining ICIs and anti-angiogenic therapy [13,14,15,16]. These findings position HAIC-based combination therapy as a promising advancement in advanced HCC management.
However, the optimal anti-angiogenic agent to combine with HAIC and ICIs remains unclear. While anti-angiogenic drugs—such as VEGF-targeting monoclonal antibodies (e.g., bevacizumab) and multi-target tyrosine kinase inhibitors (TKIs; e.g., lenvatinib)—form a cornerstone of systemic therapy [17,18], their comparative performance in this triplet setting is not well-established [19,20]. Direct comparisons between bevacizumab and TKIs combined with HAIC and ICIs are lacking. This study therefore aims to compare the efficacy and safety of these two anti-angiogenic strategies in the context of HAIC-ICI combination therapy, to inform the selection of anti-angiogenic agents in clinical practice for advanced HCC.
2. Materials and Methods
2.1. Study Design and Participants
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No. 2024-0725). Informed consent requirement was waived by the ethics committee in accordance with national regulations for retrospective analyses.
Consecutive patients with HCC treated at our hospital between June 2021 and June 2023 were retrospectively reviewed. Eligible participants received first-line therapy comprising FOLFOX-HAIC, ICIs and anti-angiogenic therapy. Two comparative cohorts were established based on targeted therapy regimens: the bevacizumab cohort (HAIC combined with ICIs and bevacizumab) and the TKIs cohort (HAIC combined with ICIs and TKIs). The selection of specific PD-(L)1 inhibitors and anti-angiogenic agents was not protocol-defined but reflected real-world clinical practice, influenced by contemporary drug availability, reimbursement policies, and clinical judgment.
Inclusion criteria encompassed (1) age ≥ 18 years; (2) HCC diagnosis confirmed histologically or clinically per European Association for the Study of the Liver (EASL) criteria; (3) BCLC stage C classification; (4) Eastern Cooperative Oncology Group (ECOG) performance status 0–1; and (5) completion of ≥2 treatment cycles with the FOLFOX-HAIC/ICI/anti-angiogenic therapy combination. Exclusion criteria included (1) concurrent HCC-directed therapies (e.g., transarterial chemoembolization [TACE] or radiotherapy) during the study period; (2) history of other malignancies; (3) incomplete essential clinical/imaging datasets; and (4) loss to follow-up (>3 months).
2.2. FOLFOX-HAIC Procedure
All patients underwent a standardized HAIC procedure performed by two experienced interventional radiologists (Songlin Song and Bin Liang, with >10 years of expertise). Prior to treatment, patients underwent a comprehensive evaluation, including medical history, physical examination, laboratory tests (complete blood count, hepatic and renal function, coagulation profile, and tumor markers), and contrast-enhanced cross-sectional imaging (CT or MRI) [21].
The procedure was performed via femoral artery access using the Seldinger technique. Initial diagnostic angiography of the hepatic vasculature was conducted with a 5-Fr catheter. Subsequently, a 2.7-Fr microcatheter was advanced superselectively into the tumor-feeding artery. When superselective catheterization was not feasible for entire tumor coverage, the catheter tip was positioned in the right or left hepatic artery. Prophylactic embolization of non-target arteries was performed as needed to optimize drug delivery [22,23,24].
All patients received the same modified FOLFOX6 chemotherapy regimen: oxaliplatin (85 mg/m^2^ infused over 2 h), leucovorin (200 mg/m^2^ over 1 h), followed by fluorouracil (400 mg/m^2^ bolus then 2400 mg/m^2^ continuous infusion over 46 h). Treatment cycles were repeated every 3 weeks until disease progression or unacceptable toxicity. Dose adjustments in subsequent cycles were permitted based on predefined criteria for hepatic function and treatment tolerance [25,26]. Any procedure-related complications were documented within the overall assessment of adverse events.
2.3. Immunotherapy Protocol
PD-(L)1 inhibitors (sintilimab 200 mg, tislelizumab 200 mg, camrelizumab 200–250 mg, atezolizumab 1200 mg, or triplimab 240 mg) were administered intravenously every 3 weeks. Each infusion was given 3 days after HAIC completion. Treatment was continued until disease progression or the occurrence of grade ≥ 3 treatment-related adverse events. Dose reductions were not permitted; however, treatment could be temporarily interrupted or permanently discontinued for unresolved toxicities, consistent with CTCAE v5.0 guidelines.
2.4. Vascular Targeted Therapy Protocol
The anti-angiogenic therapies in this study comprised tyrosine kinase inhibitors (TKIs: apatinib 250 mg, donafenib 200 mg, or lenvatinib 8 mg, all administered orally once daily) and the monoclonal antibody bevacizumab (7.5 mg/kg intravenously every 3 weeks). To mitigate peri-procedural risks, oral TKIs were withheld from 48 h before to 72 h after each HAIC session, while bevacizumab infusion was scheduled for at least 72 h after HAIC. Treatment modifications, including dose reduction, dose interruption, or treatment discontinuation, were implemented to manage treatment-related adverse events, in accordance with institutional guidelines and the approved prescribing information.
2.5. Efficacy and Safety Assessment
Baseline and clinical data were retrospectively collected from electronic medical records. Systematic radiological surveillance incorporating contrast-enhanced abdominal CT/MRI and chest CT was conducted at baseline, q6w during the initial 12-month therapeutic phase, followed by q12w intervals until disease progression or mortality. Dual-blinded independent radiographic evaluation was conducted by two board-certified radiologists (Bin Liang and Songlin Song) with >10 years of hepatobiliary imaging experience.
The efficacy evaluation indices included PFS, OS, 1-year OS rate, ORR, disease control rate (DCR), time to response (TTR), and duration of response (DOR). PFS was defined as the interval from treatment initiation to radiologically confirmed progression or all-cause mortality (whichever occurred first). ORR was defined as the proportion of patients with a complete response (CR) or partial response (PR). DCR was defined as the proportion of patients with a CR, PR, or stable disease (SD). TTR was defined as the time from treatment initiation to the first recorded CR or PR for patients with CR or PR. DOR was defined as the time from the first recorded CR or PR to disease progression or death for patients with CR or PR. The assessment of PFS, ORR, DCR, TTR, and DOR was based on RECIST 1.1. OS was defined as the time from treatment initiation to death from any cause.
Safety monitoring encompassed comprehensive documentation of TRAEs during therapeutic cycles and surveillance periods. All AEs were graded according to CTCAE v5.0, with protocol-defined allowances for dose reduction, dose interruption, or treatment discontinuation.
2.6. Statistical Analysis
Categorical variables were summarized as frequencies and percentages. Continuous variables, after assessment for normality, are presented as mean ± standard deviation or median (range), as appropriate. Group comparisons were performed using Student’s t test, Wilcoxon rank-sum test, Chi-square test, or Fisher’s exact test, depending on the variable type and distribution. Time-to-event endpoints, including PFS, OS, TTR, and DOR, were estimated by the Kaplan–Meier method and compared with the log-rank test. Hazard ratios (HRs) with 95% CIs were calculated using univariate Cox models, with patients censored at their last valid imaging assessment. Variables with p ≤ 0.05 in univariate analysis were considered for inclusion in a multivariable Cox proportional hazards model to identify independent prognostic factors. A two-sided p-value < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS 27.0 (SPSS, Chicago, IL, USA) and GraphPad Prism 10.0 (GraphPad Software, La Jolla, CA, USA).
3. Results
3.1. Patient Characteristics
Between June 2021 and June 2023, 214 consecutive hepatocellular carcinoma (HCC) patients were screened for HAIC in combination with ICIs and anti-angiogenic therapy. Following eligibility assessment, 65 patients were enrolled, including 31 assigned to HAIC plus ICIs and bevacizumab and 34 to HAIC plus ICIs and TKIs (Figure 1). In the TKIs group, the specific agents used were lenvatinib (n = 15, 44.1%), donafenib (n = 12, 35.3%), and apatinib (n = 7, 20.6%). The study population exhibited advanced disease burden. In the bevacizumab cohort, 67.7% (21/31) had tumors ≥ 10 cm in maximal diameter, 87.1% (27/31) demonstrated portal vein invasion, and 32.3% (10/31) presented with extrahepatic metastases. The corresponding figures in the TKIs group were 76.5%, 79.4%, and 55.9%, respectively. The other baseline characteristics are presented in Table 1. No statistically significant differences were observed between the two groups for all other baseline characteristics (p > 0.05).
3.2. Treatment Exposure and Compliance
The final follow-up was conducted in May 2025. Overall median follow-up duration was 25.8 months (range: 4.3–40.0), with medians of 23.9 months (range: 6.1–35.3) for the bevacizumab cohort and 25.8 months (range: 4.3–34.1) for the TKIs cohort. All participants underwent HAIC procedures with radiologically confirmed technical success, yielding a 100% technical success rate in both groups. The median HAIC cycles in the bevacizumab and TKIs groups were 6 (range: 3–9) and 5 (range: 2–9) cycles, respectively. The median ICIs cycles in the two groups were 11 (range: 3–33) and 7 (range: 2–33) cycles, respectively. The median number of anti-angiogenic therapy cycles was 11 (range: 3–33) in the bevacizumab group and 6 (range: 1–24) in the TKIs group. Complete therapeutic agent profiles, including regimens of ICIs and anti-angiogenic agents and their cycle distributions, are provided in Tables S1 and S2.
3.3. Therapeutic Efficacy
Efficacy outcomes between the bevacizumab and TKIs groups are summarized in Table 2. According to RECIST 1.1, the bevacizumab group demonstrated significantly higher ORR (83.9% vs. 61.8%, p = 0.047) and DOR (7.9 vs. 5.3 months, p = 0.008) compared to the TKIs group (Figure 2A). There were no significant differences between the groups in TTR (2.3 vs. 3.0 months, p = 0.366; Figure 2B) or DCR (96.8% vs. 85.3%, p = 0.243).
At the end of follow-up, PFS events occurred in 71.0% (22/31) patients of bevacizumab group and 97.1% (33/34) patients of TKIs group, respectively. The PFS was markedly prolonged in the bevacizumab group, with a median PFS of 10.9 months (95% CI: 8.5–13.4) versus 7.4 months (95% CI: 5.3–9.5) in the TKIs group (p = 0.001; Figure 2C). At data cut-off, the median OS was not reached in the bevacizumab group (95% CI: NR–NR; 1-year survival rate: 83.9%), compared to 23.0 months (95% CI: 18.1–27.8; 1-year survival rate: 73.5%) in the TKIs group (Figure 2D). The follow-up tables assessed using RECIST 1.1 for both groups are shown in Figure 2E,F.
The multivariable Cox regression model met the proportional hazards assumption. On multivariate analysis, the bevacizumab-containing regimen (HAIC plus ICIs and bevacizumab) remained an independent predictor of prolonged PFS (hazard ratio [HR]: 0.47; 95% CI: 0.26–0.85; p = 0.012) when assessed by RECIST 1.1 (Table 3). Subgroup analyses were also performed for specific drug combinations with ≥5 patients each. The HAIC–sintilimab–bevacizumab subgroup showed a potential efficacy trend compared to other subgroups. However, no significant difference was observed when it was directly compared with the HAIC–camrelizumab–donafenib subgroup (Figure 3). It should be noted that the latter subgroup comprised only 5 patients, which limits the statistical power of this direct comparison and precludes definitive conclusions. These exploratory findings warrant validation in larger cohorts. To further explore potential differences among the three individual TKIs within the TKIs group, we conducted a PFS subgroup analysis stratified by the specific TKI agent (lenvatinib, donafenib, and apatinib). No significant difference in PFS was observed among these three TKI subgroups (Figure S1).
3.4. Safety Profile
All patients in both cohorts experienced at least one TRAE of any grade (Table S3). No grade 5 adverse events occurred. Hematologic toxicities, hypoalbuminemia, hypertension, abdominal pain, fever, fatigue, and weight loss were commonly observed in both groups. However, differences emerged for specific AEs. Gastrointestinal hemorrhage (45.2% vs. 8.8%, p = 0.002) and gastric ulcer (22.6% vs. 2.9%, p = 0.040) were significantly more frequent in the bevacizumab cohort. Among the 14 patients with gastrointestinal hemorrhage in the bevacizumab cohort, 13 (92.9%) were grade 1–2 and 1 (7.1%) was grade 3–4. The majority of these cases were detected through routine fecal tests showing blood cells and typically did not require specific intervention. In contrast, patients in the TKIs cohort more frequently experienced elevated transaminase levels (AST: 67.6% vs. 32.3%, p = 0.003; ALT: 61.8% vs. 19.4%, p = 0.002) and hand-foot syndrome (20.6% vs. 0%, p = 0.018).
In the bevacizumab cohort, 29.0% (9/31) of patients required dose interruption, with treatment discontinuation occurring in 3.2% (1/31). No dose reductions were implemented. Conversely, in the TKIs cohort, dose reduction was required in 26.5% (9/34) of patients, while 2.9% (1/34) required dose interruption and 2.9% (1/34) underwent treatment discontinuation. Detailed information on treatment adjustments for both groups is presented in Table S4.
4. Discussion
This retrospective study suggests that the combination of HAIC and ICIs with bevacizumab is associated with significantly better key efficacy outcomes—including ORR, PFS, and DOR—compared with TKI-based triple therapy in advanced HCC. Multivariate analysis further identified the bevacizumab-containing regimen as an independent predictor of prolonged PFS.
Specifically, the bevacizumab group achieved a higher ORR (83.9% vs. 61.8%, p = 0.047) and a longer median PFS (10.9 vs. 7.4 months, p = 0.001). These findings are consistent with most previous studies on HAIC-based triplet therapies, which reported median PFS ranging from 6.6 to 13.8 months [27,28,29,30]. In contrast, He et al. reported superior efficacy for a TKI-based regimen [31], which might be attributable to the inclusion of stage B patients and greater heterogeneity in systemic agents. Additionally, the bevacizumab group showed a significantly longer median DOR (7.9 vs. 5.3 months, p = 0.008). Subgroup analysis suggested a potential efficacy advantage for the HAIC–sintilimab–bevacizumab combination, although no significant difference was found in a direct comparison with the HAIC–camrelizumab–donafenib subgroup; these results require cautious interpretation due to the limited sample size. Interestingly, although the early survival signals (6-month OS rate: 100% vs. 91.2%; 12- month OS rate: 83.9% vs. 73.5%) favored the bevacizumab-containing triplet regimen, the 18-month landmark data (57.1% vs. 58.8%) suggest that the long-term overall survival rates between the two groups may become comparable. This underscores that the current data analysis remains at a relatively early stage, and longer follow-up is essential to determine whether any initial survival benefit can be sustained.
Both regimens demonstrated no grade 5 TRAEs and had low rates of permanent treatment discontinuation (bevacizumab: 3.2%; TKIs: 2.9%). The toxicity profiles, however, differed. The bevacizumab group exhibited higher rates of gastrointestinal events, including hemorrhage (45.2% vs. 8.8%; 3.2% grade 3–4) and ulcers (22.6% vs. 2.9%; 9.7% grade 3–4), consistent with its anti-VEGF mechanism. In contrast, the TKIs group showed increased hepatic toxicity (AST elevation: 67.6% vs. 32.3%; ALT elevation: 61.8% vs. 19.4%) and higher incidences of proteinuria (29.4%), diarrhea (26.5%), hand-foot syndrome (20.6%), and RCCEP (11.8%), mirroring established TKIs toxicity patterns.
These distinct profiles required distinct management approaches. For bevacizumab, management primarily involved dose interruption (29.0%) rather than dose reduction, allowing maintenance of therapeutic intensity despite bleeding risks. For TKIs, dose reduction (26.5%) was more commonly required to manage toxicities such as hand-foot syndrome and transaminitis. These findings are consistent with landmark trials (e.g., IMbrave150 bleeding risks [13], REFLECT hepatotoxicity [32]) while extending evidence to triplet therapy contexts. Notably, the incidence of gastrointestinal hemorrhage in our bevacizumab cohort was higher than that reported in pivotal trials. This difference may stem from several study-specific factors. Patients in our cohort had advanced disease with frequent portal vein tumor thrombosis, suggesting a significant background of portal hypertension. Additionally, the fluorouracil component of FOLFOX-HAIC can cause mucositis, potentially acting synergistically with bevacizumab to increase gastrointestinal mucosal vulnerability. It should be noted that all hemorrhagic events occurred in patients who were considered appropriate candidates for bevacizumab therapy following thorough clinical evaluation, and most events were low-grad. However, in the context of portal hypertension, even low-grade bleeding warrants clinical attention, as it may signal a risk of more severe hemorrhage. This incidence rate should be regarded as a significant safety warning for this treatment regimen in HCC patients with portal vein tumor thrombosis. It is emphasized that in future clinical practice, for patients considered for bevacizumab-containing combination therapy who have risk factors for portal hypertension, baseline endoscopic screening and necessary preventive measures (such as ligation) are crucial and indispensable.
This study has several limitations. Its retrospective, single-center nature introduces inherent selection bias and limits generalizability. Clinically relevant baseline imbalances, particularly in the rates of extrahepatic metastasis and cirrhosis, were present between the groups. Although baseline characteristics were balanced, the modest sample size reduced statistical power and hindered comprehensive subgroup analyses, particularly in the heterogeneous TKIs group, where the influence of specific agents on toxicity could not be adequately assessed. Furthermore, the follow-up duration remains insufficient for mature OS analysis, and the emerging survival advantage in the bevacizumab group may become more pronounced with extended observation. These limitations highlight the need for future multicenter, prospective studies with larger cohorts to validate our findings.
5. Conclusions
This retrospective study suggests that the triplet therapy combining HAIC, ICIs, and anti-angiogenic therapy is a promising approach for advanced HCC, and the bevacizumab-based regimen was associated with better efficacy outcomes than TKI-based regimens. Both regimens demonstrated manageable, yet distinct, toxicity profiles, supporting their clinical viability with appropriate monitoring. This study observed a relatively high incidence of bleeding events with the bevacizumab-containing regimen. Therefore, we strongly recommend that the future clinical application of such regimens must be combined with mandatory baseline endoscopic risk assessment and appropriate secondary preventive measures to minimize patient bleeding risk. These preliminary findings, tempered by the study’s retrospective design, modest sample size, and heterogeneity within the TKIs group, highlight the potential of HAIC-based triplet therapy. Prospective, randomized trials with larger cohorts are warranted to validate these results, establish mature overall survival benefits, and optimize patient selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Reig M. Forner A. Rimola J. Ferrer-Fàbrega J. Burrel M. Garcia-CriadoÁ. Kelley R.K. Galle P.R. Mazzaferro V. Salem R. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update J. Hepatol.20227668169310.1016/j.jhep.2021.11.01834801630 PMC 8866082 · doi ↗ · pubmed ↗
- 3Gordan J.D. Kennedy E.B. Abou-Alfa G.K. Beal E. Finn R.S. Gade T.P. Goff L. Gupta S. Guy J. Hoang H.T. Systemic Therapy for Advanced Hepatocellular Carcinoma: ASCO Guideline Update J. Clin. Oncol.2024421830185010.1200/JCO.23.0274538502889 · doi ↗ · pubmed ↗
- 4Killock D. Novel ICI-TKI combination improves HCC outcomes Nat. Rev. Clin. Oncol.20232073310.1038/s 41571-023-00812-837563429 · doi ↗ · pubmed ↗
- 5Lyu N. Wang X. Li J.-B. Lai J.-F. Chen Q.-F. Li S.-L. Deng H.-J. He M. Mu L.-W. Zhao M. Arterial Chemotherapy of Oxaliplatin Plus Fluorouracil Versus Sorafenib in Advanced Hepatocellular Carcinoma: A Biomolecular Exploratory, Randomized, Phase III Trial (FOHAIC-1)J. Clin. Oncol.20224046848010.1200/JCO.21.0196334905388 · doi ↗ · pubmed ↗
- 6Lyu N. Lin Y. Kong Y. Zhang Z. Liu L. Zheng L. Mu L. Wang J. Li X. Pan T. FOXAI: A phase II trial evaluating the efficacy and safety of hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin for advanced hepatocellular carcinoma Gut 20186739539610.1136/gutjnl-2017-31413828592441 · doi ↗ · pubmed ↗
- 7Chisthi M.M. Current Research Status and Future Directions of Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma World J. Gastrointest. Oncol.2025179906810.4251/wjgo.v 17.i 3.9906840092943 PMC 11866237 · doi ↗ · pubmed ↗
- 8Zheng K. Zhu X. Fu S. Cao G. Li W.-Q. Xu L. Chen H. Wu D. Yang R. Wang K. Sorafenib Plus Hepatic Arterial Infusion Chemotherapy versus Sorafenib for Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: A Randomized Trial Radiology 202230345546410.1148/radiol.21154535103539 · doi ↗ · pubmed ↗