Sex Differences in Severity and Recovery Following Mild Traumatic Brain Injury: A Systematic Review
Shanika Arachchi, Ed Daly, Anushree Dwivedi, Lisa Ryan

TL;DR
This review finds that women experience more severe symptoms and slower recovery after mild traumatic brain injury compared to men, suggesting the need for sex-specific approaches in diagnosis and treatment.
Contribution
The study systematically reviews sex differences in mild traumatic brain injury outcomes, highlighting biological and neurochemical factors influencing recovery.
Findings
Female participants reported greater symptom burden, higher pain intensity, and longer recovery times compared to males.
Neuroimaging showed more white matter alterations in females and reduced cerebral blood flow in males.
Females exhibited poorer cognitive performance and higher rates of vestibular-ocular and visual abnormalities.
Abstract
Background: Sex-based variations in brain structure, hormonal balance, and neurochemistry may influence symptom presentation and recovery after mild traumatic brain injury (mTBI). This systematic review investigated sex-related differences in mTBI severity, symptoms, and recovery outcomes across different injury mechanisms. Methods: This review followed PRISMA 2020 guidelines and was registered with PROSPERO (CRD420251011379). Searches were conducted in PubMed, SPORTDiscus, Web of Science, and Scopus for articles published between 2000 and 2024. Eligible studies included adults (≥18 years) diagnosed with mTBI or concussion (Glasgow Coma Scale 13–15) with quantifiable outcome data for both sexes. Data extraction and quality assessment followed the JBI critical appraisal tools. Results: Forty-one studies involving 15,656 participants (8671 males; 6985 females) met the inclusion criteria.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
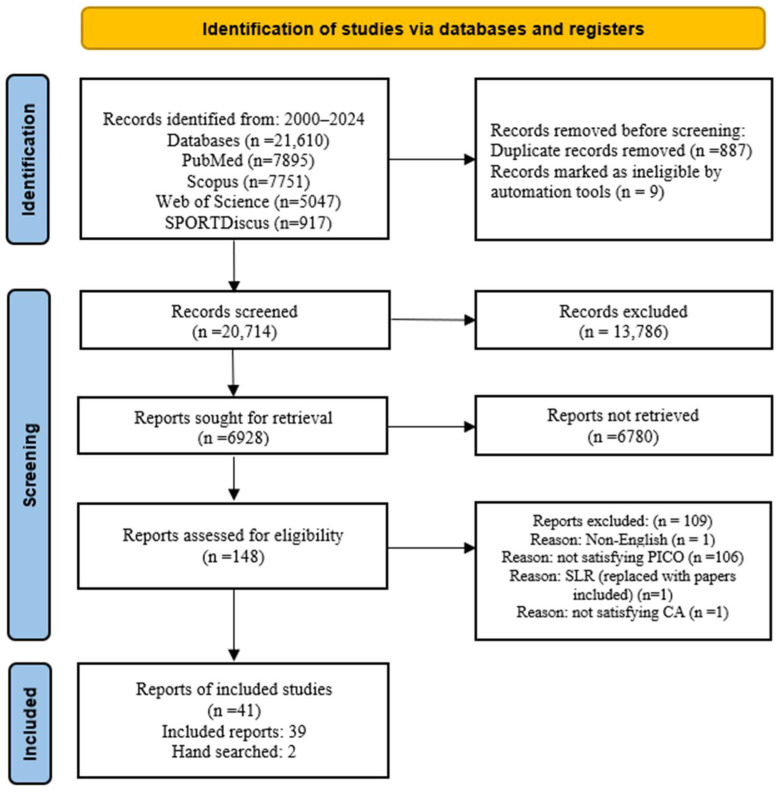 Figure 1
Figure 1- —Government of Ireland
- —European Union
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury Research · Traumatic Brain Injury and Neurovascular Disturbances · S100 Proteins and Annexins
1. Introduction
Approximately 42 million people worldwide annually experience mild traumatic brain injury (mTBI), including concussion [1]. The occurrence of mTBIs is common among the civilian population [2], sports community [3], and military personnel [4]. Sudden lateral or torsional movements of the brain inside the skull due to external force to the head or body may induce biochemical reactions in the brain tissue. This biochemical process causes a massive release of neurotransmitters (like glutamate) and ionic flux (potassium and sodium/calcium). This process causes a surge in energy demand and a subsequent energy crisis, leading to acute and subacute changes in cellular physiology with impaired blood flow and potential long-term cognitive impact [5]. These alterations cause the cognitive [6], sensory [7], electrophysiology [8], and gait and balance [9] functions of the patient. The untreated or not fully recovered mTBI conditions may increase the risk for neurodegenerative diseases in later life.
Clinical signs immediately following an mTBI may include loss of consciousness, altered mental condition, amnesia, incoordination of motor control, seizures; some post-injury symptoms include acute alterations in mental status, headaches, dizziness, balance or vision problems, light or noise sensitivity, mental fog, difficulty concentrating, fatigue, and emotional distress [10]. Cognitive impairments are one of the commonly observed symptoms following an mTBI, and persistent conditions can negatively affect the quality of life of individuals even after full recovery [11]. The axons are the long, slender projections of neurons, which conduct electrical impulses away from the cell body; these axons are more vulnerable to damage during an mTBI. The axonal damage occurs due to the shearing force induced during the injury, resulting in diffuse axonal injury (DAI). DAI plays a major role in cognitive impairments after an mTBI [12]. These cognitive impairments can be seen as cognitive deficits, emotional distress, or somatic complaints [13]. However, most symptoms differ due to person-specific factors such as age, sex, pre-injury conditions, and pre-existing health conditions [14,15].
Clinical studies demonstrate that sex and age are the primary patient-specific factors influencing symptom identification, diagnosis, and post-injury treatments in patients with mTBI [16]. Moreover, female sex is identified as one of the main potential risk factors in addition to pre-concussion history, Glasgow Coma Scale (GCS) of [13,14,15], aetiology of assault, preinjury psychological history, etc. [17]. In addition, female athletes have potentially greater injury burden [18] and higher post-concussion scores [19] compared to their male counterparts. Biologically, females report higher levels of physiological stress compared to males [20]. These sex-based differences may be observed due to the structural variations in the male and female brain tissue, in addition to the biochemical variation with respect to the differences in hormonal and neurochemical levels. Previous studies on mTBI have been based on male participants, and limited studies have included female participants [21,22]. A significant knowledge gap persists regarding the impact of sex differences on mTBI symptom reporting, diagnosis, and treatment interventions, highlighting the need for further research. Therefore, the aim of this systematic literature review (SLR) was to investigate the current state of the art of the sex-based variations in mTBI severity and recovery. Identifying these variations may help to improve the treatment interventions and post-injury recovery.
2. Materials and Methods
2.1. Literature Search
The authors conducted an initial database search in November 2024 using the following keywords with the Boolean terms: “(Concussion OR mTBI OR Mild Traumatic Brain Injury OR sports concussion OR Accidents OR Falls OR Whiplash) AND (Sex OR Gender OR male OR Man OR Men OR Female OR Women OR Woman)”. The search terms, synonyms and related terms are shown in Table 1. The search was conducted in four databases (PubMed, SPORTDiscus, Web of Science, and Scopus) for articles published from 2000 to 2024. This systematic review follows the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines [23]. This systematic review was registered under PROSPERO 2025 CRD420251011379.
2.2. Inclusion and Exclusion Criteria
The inclusion and exclusion criteria of this SLR were based on the PICO (Population, Intervention, Comparator, and Outcome) framework, which was agreed upon by all the authors. The studies were included if they satisfied the PICO inclusion criteria as follows. (1) The population included all the healthy male and female participants ages 18 and over who were diagnosed with mTBI/concussion (GCS of 13–15). (2) The intervention was based on the injury mechanism, which included contact/non-contact sports, trauma, collision, head accelerations (whiplash), or blast-related injuries. (3) The inclusion outcome was based on the concussion/mTBI diagnostic and prognostic outcomes with quantifiable data observed and reviewed for the male and female patients. The outcome measures included the mTBI incident and recovery stage related to cognitive, motor control, visual, and vestibular impacts along with the findings from brain imaging. (4) The inclusion comparator was based on the outcome comparison against the healthy participants in addition to sex-based variations. Furthermore, the biologically defined sex/gender as male or female was considered in this review study.
The studies were excluded if they did not satisfy the inclusion criteria for population, intervention, comparator, and outcome. Studies were excluded if the population was individuals under 18 years old, human or animal cadavers, animals, or cell studies. In addition, if the intervention was moderate to severe TBIs with a GCS index below 12 or inconclusive or unspecified brain injuries those studies were excluded. Furthermore, if the injury mechanism was complicated resulting in severe injuries in addition to a brain injury, those studies were excluded due to the complexity of the injury severity. Studies were excluded if the participants had pre-existing health conditions including neurodegenerative diseases or other drug interventions. Furthermore, studies were excluded if the outcome was based on the validation study for a treatment or protocol intervention. All the non-English and narrative study designs were excluded.
2.3. Selection Process
All search results retrieved were exported into an EndNote 21.3 (Philadelphia, PA, USA) reference management software library for eligibility screening. The initial screening of all the titles and abstracts was conducted to remove the duplicates. Then, the remaining titles were coded according to the inclusion criteria. The ineligible articles were moved to a different library according to the PICO exclusion investigation. The PICO protocol was developed precisely upon the agreement of all the authors prior to the initial literature search. A random selection of 20 reports was shared among all the co-authors to assess the repeatability and the reproducibility of the selection criteria. All the co-authors agreed with the selection criteria. Next, the first author screened the included full-text articles according to the inclusion and exclusion criteria. The inclusion criteria were further refined with the agreement of the co-authors. We decided to exclude the articles focused on model-based outcomes (artificial intelligence or machine learning-based, etc.), complicated traumas, validation studies (including frameworks, drug or nutrition interventions, instruments, etc.), and case reports (due to no comparison).
After that, the first author continued to full-text screening and coding according to the inclusion criteria. Then, the finally selected articles were shared among the co-authors for further assessment of whether they include or exclude the papers. All the co-authors agreed on the selected articles to include in this SLR.
2.4. Data Extraction
The data were extracted by the first author using the Excel work platform. The following information was extracted from the selected articles: title, DOI, author, year of publication, population size, outcome measure, and key findings related to sex-based variations. The data extraction process was verified by co-authors who randomly selected a subset for cross-checking.
2.5. Risk of Bias (RoB) Assessment
The selected articles included cohort studies, cross-sectional studies, case–control studies, and systematic reviews. Hence, the quality of the selected articles was assessed using JBI’s critical appraisal tool [24,25]. JBI is an international research organisation based in the Faculty of Health and Medical Sciences at the University of Adelaide, South Australia. JBI tools for cohort studies, cross-sectional studies, case–control studies, and systematic reviews were used to evaluate the quality of the study methodology and the possible bias in the study design, conduct, and analysis. All questions in the JBI’s critical appraisal tools were organized into an Excel spreadsheet for the ease of analysis. For each study design, the appraisal tool checklist was filled out. Reasons for exclusion were clearly tabulated in the same Excel spreadsheet. Each co-author performed a pilot test separately using a copy of the embedded Excel spreadsheet to verify the assessment criteria.
A quality assessment scaling system was defined as follows, “Yes” (1 Point) “No” (0 Points), and “Unclear/NA” (0.5 Points). The total points scored by each study were presented as a percentage for easier comparison. All co-authors reviewed the final Excel spreadsheet and agreed with the reasons for including or excluding each study. If the quality assessment percentage fell below 50%, the article was removed from the selection, resulting in one article being eliminated. In addition, a systematic review article was replaced with two hand-searched articles included in the same paper, which satisfy the inclusion criteria.
3. Results
A total of 21,610 records were screened for eligibility, and the full text of 148 reports was retrieved for detailed evaluation. After a comprehensive review of the full texts, a total of forty-one articles met the inclusion criteria after full text review. However, one of the eligible full-text SLRs was replaced by two hand-searched full text articles included in that specific SLR. The identification, screening, and inclusion of the eligibility criteria are presented in the PRISMA flow diagram [23] shown in Figure 1.
3.1. Characteristics of the Included Studies
The characteristics of the included studies are summarized in Table 2 and Table 3, which include the study design, participants, outcome measures, main findings, whether significant sex-based variation is reported, and the RoBs of the study. A total of 12,382 individuals participated in the selected studies (n = 7021 males; n = 5361 females). The studies consisted of cohort studies (prospective, retrospective, observational, longitudinal), cross-sectional studies, and case–control studies.
The selected studies were categorized under the following subcategories: sports-related concussion (SRC), military-related concussion, domestic violence, (Table 2) and unclassified category (UC) (Table 3). The studies included in the unclassified category represented the patients admitted to the emergency departments due to falls, road accidents, workplace-related accidents, etc. The study outcomes are synthesised below under the following identified areas: brain image variations, cognitive function variations, gait and balance deformities, variations in electrophysiological measures, and neurosensory alterations.
3.2. Sex-Based Variations in Brain Structure Following an mTBI (Neuroimage-Based Findings)
Ten studies investigated sex-based variations in brain images after mTBI. The imaging techniques employed in these studies included Diffusion-Tensor Imaging (DTI), Diffusion-Weighted Magnetic Resonance Imaging (dMRI), MRI (Magnetic Resonance Images), and Resting-state functional Magnetic Resonance Imaging (rs-fMRI). These imaging techniques were utilized to observe the cerebral blood flow (CBF), white matter microstructure, white matter fractional anisotropy (FA), mean diffusivity, cortical thickness, etc. These indices can be examined using imaging techniques. The brain physiology indices of white matter microstructure and CBF demonstrate substantial sex-based differences, where 30% of the white matter regions of interest show absolute sex differences [62], while females are more sensitive to CBF changes [63].
Four out of ten brain image-based studies were under the SRC category representing soccer, ice hockey, hockey, volleyball, football, rugby, basketball, and lacrosse players (Table 2). These studies investigated the sex-based variations in white matter microstructural changes in the brain tissues [31,32,36,37]. Rubin et al.’s study [31] found that women exhibit higher microstructural white matter alteration than men following repetitive sub-concussive head impacts in amateur soccer. Their sample included the players of more than 5 years of amateur-level playing (Table 2). These repetitive head impacts may lead to higher white matter microstructural changes. The reason for these brain microstructural variations between males and females may be observed due to the variations in the heading locations and the biomechanical approaches of force and acceleration experienced during the impact. The heading exposure was associated with lower Fractional Anisotropy (FA) in genu and splenium of the corpus callosum and the pons regions in males, while in females FA-lowering regions include the genu of the corpus callosum; left occipital, right parietal, and right orbitofrontal white matter; left superior longitudinal fasciculus; right cingulum; and right cerebral peduncle [31]. Sollmann et al. [32] also found sex-based differences in structural alterations following exposure to repetitive sub-concussive head impacts in collegiate ice hockey players. Their study observed that increases were observed in pre- vs. post-seasonal absolute difference in FA (0.0268), mean diffusivity (0.0002), axial diffusivity (0.00008), and radial diffusivity (0.00005) in female athletes compared to their male counterparts, showcasing the structural alterations in brain tissue following exposure to repetitive head impacts (Table 2). Churchill et al.’s [36] study, based on university-level athletes (soccer, hockey, volleyball, football, rugby, basketball, and lacrosse players), found that male athletes had greater reductions in occipital-parietal CBF and increases in callosal mean diffusivity, with the greatest effects at one year after the return to play compared to the female athletes. Furthermore, female athletes exhibited reductions in FA of the corona radiata. These variations were observed mainly due to the sex-based differences in white matter microstructure alterations and CBF distribution. Similarly to Rubin’s et al. [31] study on soccer players, Sollmann et al.’s [32] study on ice hockey players also exhibited alterations in the FA in female athletes compared to their male counterparts (Table 2). However, Wright et al.’s [37] study also showed that male concussed athletes (amateur footballers) exhibited significantly greater white matter disruption compared to female concussed athletes following 48 h and two weeks post-injury. Their study on whole-brain voxel analyses found that male athletes demonstrate an increased fibre density in the cingulum compared to their female counterparts following an SRC at 40 h and 2 weeks’ time intervals. Cognitive performance is associated with white matter microstructure and fibre density in the cingulum; therefore, disruptions in these parameters may be linked to early-stage neurodegenerative disorders (Table 2). In addition, Valera et al. [43] investigated brain-imaging-based variations in repetitive mTBIs in the context of domestic violence, finding they may lead to measurable white matter abnormalities especially in posterior and superior corona radiate regions of the affected women’s brain. Both posterior and superior regions of corona radiate serve as major convergence points for long fibre tracts in cerebral cortex to subcortical areas. The damage caused to these regions may impact the working memory, learning attention, and visuospatial and linguistic abilities of the affected person (Table 2). These image-based results indicate that microstructural variations in male and female brain tissue exhibit differences after a head impact, especially with respect to FA variations in white matter and CBF variations. These differences may have a correlation to the structural and anatomical differences in the male and female brains as discussed above, in addition to the level of sex hormones, resulting in differences in cognitive, neurosensory, electrophysiological, and gait and balance deformities. To understand these alterations in treatment interventions, it is essential to understand the sex-based variations in brain tissue microstructures in detail.
In the unclassified category (Table 3), Fakhran et al. [48] found that female patients with mTBI have more extensive white matter abnormalities than male patients, where male patients had significantly decreased fractional anisotropy values in the uncinate fasciculus, which connects the temporal lobe with the frontal lobe with a white matter pathway (mean FA, for males 0.425; 95% confidence interval: 0.375, 0.476 for females 0.443; 95% confidence interval: 0.393, 0.493 with a p value > 0.05, (compared with male patients with mTBI) and the Cohen d effect size of 0.720) (Table 3). This detail can be a promising predictor for the persistence of post-concussion symptoms. Shao et al. [50] examined the MRI-based cortical thickness and compared it with neurocognitive outcomes after an mTBI. Females had thicker cortical thickness in the left caudal anterior cingulate cortex than their male counterparts (p = 0.004) and higher scores for neurocognitive assessments. These findings can relate to the management strategies for male and female mTBI patients differently (Table 3). Wang et al. [51] examined the influence of sex differences in abnormal intrinsic functional connectivity after acute mTBI, with distinct patterns observed in females compared to males, especially in the right middle frontal gyrus and its connectivity with other brain regions (Table 3). Another Chinese study [53] found that gender and time following the injury significantly affect cognitive performance. An increased CBF was observed in the male patients compared to the females at the acute phase. In addition, male patients showed a reduced CBF in the left inferior frontal cortex at the subacute phase (one month) following the injury. In contrast, no impairments on neuropsychological performance were observed in female patients in their study. These findings suggested that the regional CBF variations could serve as a potential biomarker to investigate the gender variations in the mTBI pathology and the recovery phase [53].
Hsu et al. [49] conducted a study on working memory functional MRI of patients with mTBI one month and two-and-a-half months after the head injury reported at the emergency departments of three selective hospitals. They investigated that female patients with mTBI demonstrate worse working memory activation patterns (with functional MRIs) compared with male patients, and these differences persist over time (Table 3) These decreases in working memory circuits may result from persistent hypoactivation observed in the females post-injury, and it may play a role in poor working memory post-injury and the delayed recovery phase.
By concluding the above brain-imaging-based variations, the following findings were highlighted: females showed smaller disturbances to the CBF compared to their male counterparts. However, sex-based differences in white matter alterations were observed in different regions across the brain. These differences were mainly attributed to the structural and anatomical variations between male and female brains. Moreover, the variations in sex hormones, especially estrogens, progesterone and testosterone levels, may also contribute to the neuroprotective mechanism following an mTBI. Hence, it is important to consider the individual sex hormonal levels, especially for female patients during their menstrual cycle or menopause period.
3.3. Sex-Based Variations in Cognitive Function Alterations Following an mTBI
Twenty-four studies discussed the sex-based variations in cognitive functions after mTBI. The assessment tools employed were Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT), Sport Concussion Assessment Tool (SCAT), Standardized Assessment of Concussion (SAC), Post-Concussion Symptom (PCS) scores, Neurobehavioral Symptom Inventory (NSI), Posttraumatic Stress Disorder Checklist (PTSD) checklist, Rivermead Post-Concussion Symptoms Questionnaire (RPQ), computerized Concussion Resolution Indices (CRI) Cambridge Neuropsychological Test Automated Battery, Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), Conversational discourse: Canadian Adult Achievement Test (CAAT), Glasgow Outcome Scale Extended (GOSE), and the Test de Rendement pour Francophones (TRF).
The alteration in cognitive functions after an mTBI is one of the commonly observed symptoms in assessing injury severity. Patient-specific factors play a significant role in these symptoms, both immediately after the injury and several months afterward. Sex is considered one of the most important patient-specific factors in the scientific findings, and females show the worst symptoms compared to male patients.
The following findings were highlighted in the SRC subcategory (Table 2). Hutchison et al. [29] found that female university athletes (representing football, soccer, rugby, hockey, basketball, volleyball, lacrosse, and baseball) reported higher baseline SCAT3 symptom scores compared to male athletes (p = 0.009). Hamer et al.’s [3] (Table 2) study suggests that a history of concussion (HOC) may have sex-specific effects on CBF, with only males with HOC showing lower CBF relative to controls, but females with multiple concussions showing lower CBF than those with a single concussion. These findings suggest greater overall variability in the effects of HOC on cerebrovascular function for female athletes compared to their male counterparts resulting in a negative impact on cognitive abilities. A Swedish study by Vedung et al. [35] (Table 2) found that compared to male soccer players, female soccer players had worse initial symptom severity scores. These observations may represent the biological differences in male and female neck muscle strength in addition to the hormonal fluctuations. In addition, a recent SRC study by D’Alonzo et al. [40] (Table 2) found that female athletes (participated in basketball, field hockey, football, ice hockey, lacrosse, rugby, soccer, sprint football, water polo, wrestling, baseball, cheerleading, diving, equestrian, fencing, golf, gymnastics, polo, rowing/crew, sailing, skiing, softball, squash, swimming, tennis, track and field/cross country, and volleyball) may experience a longer symptom duration and recovery to sport compared to male athletes, even after controlling for baseline differences and injury characteristics of symptom resolutions, concussion history and academic accommodations [40]. In addition to the differences in neck muscle strength and hormonal fluctuations, females are more vulnerable for the pre-existing psychological conditions. These factors may play a major role in these observations.
A military-based concussion incidence study by Brickell et al. [4] suggests that female service members report more post-concussive symptoms than male service members after mTBI. Their study investigated the patients using the PTSD checklist and NSI. These symptoms include poor concentration, trouble remembering a stressful event, disturbing memories, thoughts, and images with higher PTSD scores (Table 2). These observations may have a relationship with females’ vulnerability in pre-existing psychological conditions and the psycho-social differences experienced in their workplace.
In the unclassified category, five studies found that female sex is independently associated with worse outcome after mTBI at 3 to 6 months, as evidenced by higher PCS scores compared to their male counterparts [44,45,55,58,59] (Table 3). In addition, these findings further encourage the scientific community to assess the mTBI symptom outcomes such as sleep quality, fatigue, phycological status, etc., together with biological sex to understand the severity and the treatment interventions. Wang et al. [52] study suggests that sex differences influence the patterns of abnormal intrinsic functional connectivity after acute mTBI, with distinct patterns observed in females compared to males, particularly about the right middle frontal gyrus and its connectivity with other brain regions, and this may underpin sex-specific clinical symptoms like BAI and BDI (Table 3). LeBlanc et al.’s [56] study also observed that sex-based variations in mTBI based on conversational discourse and reading comprehension. Females performed better than males on letter-category naming. However, for most other cognitive-communication measures presented, males and females performed similarly in the acute stage after a complicated mTBI. In addition, Levin et al. [16] study on posttraumatic stress disorder in mTBI, women exhibited higher levels of posttraumatic stress, depressive, anxiety, and somatization symptoms across all post-injury time points compared with men (Table 3).
Biologically, females report higher levels of physiological stress compared to males [20]. This could show differences in self-reporting symptoms and the pain levels after an mTBI by male and female individuals. Five out of thirteen studies included in the unclassified mTBI category discussed the sex-based variations in self-reported cognitive complaints, and the following findings were highlighted. Levy et al.’s [2] study observed that female participants reported significantly higher levels of cognitive complaint (CCAMCHI scores) compared to males, even after accounting for psychological distress and greater symptom burden (Table 3). However, Anderson et al. [58] study found that sex did not significantly predict CCAMCHI (subjective cognitive impairment), even though female sex was associated with an increased likelihood of PCS reporting. Wågberg et al.’s [60] study observed a worse GOSE outcome in women compared to men (Table 3). Similarly, Losoi et al. [61] study found sex was not associated with chronic post-concussion symptoms after evaluating many neuropsychological indices (Table 3).
Furthermore, Mondello et al. [34] investigated the impact of total tau, neurofilament light chain, glial fibrillary acidic protein, and ubiquitin C-terminal hydrolase-L1 on blood biomarkers after an mTBI (Table 2). Plasma tau levels were significantly higher in females 6 h and 3 days after a concussive event compared to males (10.78 vs. 5.42 pg/mL, p = 0.017, and 6.78 vs. 3.49 pg/mL, p = 0.0006, respectively), and the relationship between biomarker levels and behavioural outcomes is more evident in females than males.
Lannsjö et al.’s [47] study investigated the computer tomography outcome of an mTBI after 3 months, together with the (RPQ) and GOSE, and reported that female sex is associated with poor outcome, reporting more post-injury symptoms (Table 3). They further emphasized the importance of incorporating sensitive imaging technologies to identify brain pathology together with symptoms, thereby facilitating effective treatment interventions. However, three studies out of 24 included in the cognitive function category have reported no significant sex-based differences (p < 0.05) in SAC scores [26], SCAT5 symptom scores [38], computerised CRI [26], and ImPACT battery [42] based on their study populations [26,38]. Even though, Walton et al.’s [41] study on athletes who participated in basketball, baseball/softball, cheer/dance, cross country/track and field, swimming and diving, gymnastics, lacrosse, soccer, squash, and tennis found that no significant sex-based differences in times to reaching any clinical milestone such as time to diagnosis, symptom resolution and RTP (Table 2) Similarly, Sicard et al. [27] analysed sex-based variations in four core cognitive domains: processing speed (Detection Task), attention/vigilance (Identification Task), visual learning (One Card Learning Task) and executive function (1-Back condition of the N-back), where they found no significant sex differences in cognitive tasks except N-back Task (Executive Functions). In the N-back Task, female athletes with a history of concussion responded significantly slower than their male counterparts. The N-back task is more cognitively challenging than the 1-back task; hence, these observations could indicate the persistent cognitive challenges that females exhibit during the chronic phase of the injury. In contrast, females scored significantly higher (p = 0.048) on a visual memory test based on pattern recognition compared to their male counterparts [46]. This finding is different from the other cognitive functional variations observed between males and females. Better processing speed in female participants may be linked to their higher education level compared to the male participants in the study cohort.
3.4. Sex Based Variations in Gait and Balance Deformities Following an mTBI
Three of the included studies investigated sex-based variations in gait and balance deformities after an mTBI. Females tended to have longer recovery times for gait deformities and return to play/work compared to the male. The following findings were highlighted in the SRC subcategory; Messerschmidt et al. [28] presented their findings based on dual-task cost (DTC) of gait speed, cadence, step length, and step width of the collegiate athletes (Table 2). Their findings show that females demonstrated significantly higher DTC of gait speed cadence, percentage of swing phase, and double-support phase. Howell et al. [33] found that female collegiate athletes (participated in soccer, field hockey, rugby, basketball, ice hockey, softball, and volleyball) take longer to recover objective gait measures of single-task, dual-task, and height-adjusted gait speed after concussion compared to male collegiate athletes (participated in football, baseball, wrestling, ice hockey, lacrosse, sailing) (Table 2).
In the unclassified subcategory, Studenka et al.’s [54] study found that concussed females may be more susceptible to lasting alterations in visual-motor performance than males, especially with increasing numbers of concussion (p = 0.031) (Table 3).
3.5. Sex-Based Variations in Electrophysiological Measures Following an mTBI
Two studies, by Pauhl et al. [57] and Carrier-Toutant et al. [30], in the included articles discussed the sex-based variations in electrophysiological measures after an mTBI. Pauhl et al. [57] found no significant differences in motor-evoked potential amplitude or cortical silent period duration between males and females following concussion, indicating a lack of differences in these neurophysiological measures between sexes after concussion (Table 3). Carrier-Toutant et al.’s [30] study investigated the early event-related brain potentials measures of P1 and N1 (Table 2). They observed that males exhibited significantly smaller P1 (p = 0.08) responses to Emotional Facial Expression stimuli than females. Also, male athletes showed smaller amplitude in N1 component following a concussion compared to female athletes. These findings help to understand the differences in neurophysiological mechanisms related to emotional stimuli for male and female patients with mTBI.
3.6. Sex-Based Variations in Neurosensory Alterations Following an mTBI
Lumba-Brown et al. [7] was one of the two included studies that discussed the sex-based variations in neurosensory alterations after mTBI (Table 2). Their study investigated the neurosensory measures of oculomotor impairment, auditory changes, and vestibular impairment. They found that females have a higher incidence of abnormalities in smooth pursuit, convergence, and visual motion sensitivity. Furthermore, males reported higher rates of light sensitivity, while females reported higher rates of noise sensitivity, but these differences were not statistically significant. Caccese et al.’s [39] study reported that female participants scored higher vestibular ocular motor screen total symptom scores at 24–48 h post-injury (p = 0.005) compared to their male counterparts (Table 2). Neurosensory variations are widely observed in the post-concussion stage. Understanding the sex-based variations in the neurosensory changes can be incorporated to improve the rehabilitation outcomes.
4. Discussion
This systematic review synthesised current evidence on sex-related differences in mild traumatic brain injury (mTBI) severity and recovery across sports, military, domestic violence, and civilian settings. Overall, females consistently showed a higher symptom burden, longer recovery times, and greater cognitive and neurosensory impairments compared with males. These findings emphasise the need to consider sex as a biological variable in both research and clinical practice for mTBI management.
Male and female brains differ in total volume, cortical thickness, and white-to-grey matter ratios, which may influence injury biomechanics and post-injury physiology [64]. When controlling the total brain volume, females show greater total cortical grey matter volumes, while males show greater total white matter volumes [65]. Also, females have a greater volume in the corpus callosum, bilateral parietal lobes, left anterior cingulate gyrus, and left caudate nucleus compared to males, while males have a greater volume in the left superior temporal gyrus [65]. These anatomical variations play a key role in responding to mTBI, as they induce structural and physiological disruption in the white matter regions, especially causing DAI [66]. The external mechanical force experienced by the head during an mTBI includes a mechanical deformation across the brain tissues. Wright et al. [37] observed changes in white matter microstructure within 48 h post-injury, showing striking differences in fibre density. While some studies highlight more white matter alterations in females, which correlate with worse symptom outcomes [31,48,51], others focus on repetitive mild traumatic brain injuries (mTBI) due to domestic violence affecting women [43]. Sollmann et al. [32] also note significant structural changes in collegiate ice hockey players after repeated head impacts. These findings emphasize the vital need for tailored approaches in incorporating sex-based structural differences in mTBI injury management and care.
Alterations in cognitive functions following a mild traumatic brain injury (mTBI) are frequently observed and can serve as key indicators for assessing the severity of the injury. Cognitive functions are altered following an mTBI mainly because axons are damaged or destroyed by acceleration/deceleration forces acting upon the axonal bundles and intracranial blood vessels, resulting in white matter damage. Understanding patient-specific factors is essential, as they significantly impact the symptoms experienced and self-reporting both immediately after the injury and for post-injury assessments. Among these factors, sex has been identified as particularly influential, with research indicating that females may experience more pronounced symptoms and longer recovery time compared to their male counterparts in SRC [35,36,40], military-related mTBI [4] and unclassified mTBI reported at the emergency departments [44,45,55,58,59]. Biologically, females report higher levels of physiological stress compared to males [20]. This could show differences in self-reporting symptoms and the pain levels after an mTBI by male and female individuals. This insight underscores the importance of tailored assessment and intervention strategies based on sex differences in post-injury management following an mTBI.
Impairment in balance and gait is another concerning symptom associated with mTBI [9]. mTBI may alter the gait cycle with slowed walking velocity, greater time in double-leg stance support, and less time in single-leg stance support [67]. These gait deformities are the outcomes of underlying pathophysiological processes due to the concussion, resulting in alterations in neurocognitive functions [5]. This SLR also revealed that females tend to have longer recovery times for gait deformities and return to play/work compared to males [28,33,54].
An mTBI has the potential to alter the electrophysiological measures of the brain. Event-related potentials are one of the most used techniques to observe the cerebral/cognitive consequences that occur due to an mTBI. Only two of the studies [30,57] included in this SLR discuss the electrophysiological observations after an mTBI. The event-related brain potentials (P1, N1) of emotional facial expressions study by Carrier-Toutant et al. [30] identified that males exhibited significantly smaller P1 responses to Emotional Facial Expression stimuli and an amplification in the N1 component than their female counterparts. These observations highlighted the sex-based differences in neurophysiological mechanisms after an mTBI incidence. Hence, it is vital to investigate the event-related electrophysiological potentials to understand the underlying cerebral dysfunctions to address the post-concussive symptoms while addressing the sex-based variations for effective management. Sometimes, conventional imaging assessment may fail to diagnose the underlying impact; in such situations, electrophysiological measures can be used as a promising biomarker to further investigate the injury incident to detect the underlying changes in brain function that are responsible for a patient’s symptoms related to cognition, brain function, and neurological conditions. This indicates that incorporating the sex differences in these interventions may improve the outcome of injury management.
Neurosensory alterations are common after a head trauma due to the extreme damage to the brain tissue, diminished metabolism, and the regulation of cerebral blood flow [68]. Female participants experienced more symptoms related to neurosensory alterations; they exhibited worse ImPACT Visual Memory, slower clinical reaction times, and longer King–Devick Total Time across the timelines of 24–48 h post-injury compared to their male counterparts [39]. Also, females had a higher incidence of abnormalities in smooth pursuit, convergence, and visual motion sensitivity [7]. The sex differences in hormonal fluctuations, especially during the menstrual cycle, and the level of neurochemistry (which are crucial for brain repair and regeneration) may contribute to the injury severity and the symptom outcomes. A tailored assessment may be important when the standard clinical assessments fail to identify the neurosensory symptoms related to the injury, especially for women, as they are more vulnerable to physiological stress compared to males.
Research shows that an mTBI experience during the lifetime may have a positive correlation with neurodegenerative incidents in the later stages of life [69,70,71]. Hence, diagnosis of the incident, proper treatment interventions, and recovery play key roles in reducing the future risk of neurodegenerative diseases. According to the research, sex and age are the primary factors influencing symptom identification, diagnosis and post-injury treatments in patients with mTBI [16]. Therefore, understanding the sex-based factors can guide effective treatment interventions and post-injury management. This will eventually reduce the incidence of neurodegenerative diseases among the impacted population. Additionally, understanding the biochemical changes resulting from head impacts and how they correlate with symptom levels is vital for accurate mTBI diagnosis. This knowledge will significantly enhance treatment outcomes.
People become exposed to various accidents/incidents possibly causing head traumas throughout their lives. These head traumas may be neglected at the point of the incident, mainly due to the severity of the other accident-related injuries. The undiagnosed or untreated head traumas may have a positive correlation with the neurodegenerative diseases in their late life. Understanding the patient-specific factors, like sex, will enhance the effective diagnostic or prognostic interventions by reducing the risk factors and healthcare burdens. This SLR concludes that sex difference plays a vital role in symptom reporting, diagnosis, and recovery phase following a mTBI, mainly due to the biological differences in male and female brain structures, in addition to the sex related biochemical variations, especially in hormones and neurochemistry. Thus, incorporating sex-based variations plays a key role in effective diagnostic and treatment interventions and recovery outcomes. Ultimately, this will contribute to achieving sustainable developmental goals (SDG 3.4) by reducing mortality from non-communicable diseases and promoting mental health.
Limitations and Future Directions
There are a number of limitations to acknowledge. One of the important limitations was that some of the included studies relied on self-reported concussion/mTBI assessments, which may have introduced bias into the overall findings of these studies. This bias could have influenced the pain severity assessments and the reporting. The selected studies included participants aged 18 years old. However, age is one of the main factors that impact the injury severity and the recovery. Hence, incorporating the younger-aged participants could improve the study’s findings. Heterogeneity of the studies is one of the key limitations of this SLR. It challenges the results synthesis process, especially in interventions, outcome measures, and settings. Furthermore, publication lag could be another limitation, as we conducted the search in November 2024, and since then, some new findings could have been published relevant to this SLR.
The differences in the severity and recovery of mTBI based on sex highlight the need for further research in this area. It is essential to gain a clearer understanding of how brain injuries affect males and females differently. Future studies should concentrate on investigating the structural and biochemical transformations that occur following an mTBI in relation to sex, based on neurobiological differences, while incorporating both neuroimaging and neuropsychological biomarkers. In addition, future studies should focus on female patients during their menstrual cycle or menopause period, as the sex hormone fluctuations vary differently during these periods of their lives. Moreover, the identification and incorporation of the influences of sex chromosome-linked genes may be crucial in injury severity and recovery; therefore, it is vital to explore these gene influences in future research. The inclusion of vulnerable populations such as geriatric, pediatric (children and adolescents), and athletes in the study cohort is crucial when tailoring the early treatment interventions, as it creates a provision to address the variations in individual anatomical and hormonal levels. As stress levels can highly influence the mTBI injury severity and recovery, incorporating the lifestyle and pre-existing mental conditions into the diagnostic stage could improve the treatment outcome. In addition to male and female genders, more research should be focused on understanding the anatomical and biochemical variations in individuals in the nonbinary category. Furthermore, the clinical research should include larger, diverse samples with longitudinal studies to map the symptom trajectories with combined clinical, anatomical (images), genetic, and hormonal data to obtain a clear picture of the mTBI symptoms and recovery stages. This information could be further implemented into risk prediction models to incorporate personalized treatment interventions and better recovery outcomes.
5. Conclusions
Mild traumatic brain injuries contribute to more than 90% of reported traumatic brain injuries, which leads to the injury-related long-term consequences, causing higher healthcare costs. This SLR concludes that sex difference plays a vital role in symptom reporting, diagnosis, and the recovery phase following an mTBI. These differences are primarily due to the distinct biological characteristics of male and female brain structures, along with the variations in sex-related biochemistry, especially regarding hormones and neurochemistry. Thus, incorporating sex-based variations plays a key role in effective diagnostic and treatment interventions and recovery outcomes. Therefore, further research should focus more on gaining a clearer understanding of how brain injuries affect males and females differently, especially concerning structural and biochemical variations that result from mTBI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gardner R.C. Yaffe K. Epidemiology of mild traumatic brain injury and neurodegenerative disease Mol. Cell. Neurosci.201566758010.1016/j.mcn.2015.03.00125748121 PMC 4461453 · doi ↗ · pubmed ↗
- 2Levy A.M. Saling M.M. Anderson J.F. Psychological distress and gender predict cognitive complaint after adult civilian mild traumatic brain injury in pre-morbidly healthy adults Neuropsychol. Rehabil.20243472174110.1080/09602011.2023.223634837493086 · doi ↗ · pubmed ↗
- 3Hamer J. Churchill N.W. Hutchison M.G. Graham S.J. Schweizer T.A. Sex differences in cerebral blood flow associated with a history of concussion J. Neurotrauma 2020371197120310.1089/neu.2019.680031650894 · doi ↗ · pubmed ↗
- 4Brickell T.A. Lippa S.M. French L.M. Kennedy J.E. Bailie J.M. Lange R.T. Female service members and symptom reporting after combat and non-combat-related mild traumatic brain injury J. Neurotrauma 20173430031210.1089/neu.2016.440327368356 · doi ↗ · pubmed ↗
- 5Giza C.C. Hovda D.A. The neurometabolic cascade of concussion J. Athl. Train.20013622810.1227/NEU.000000000000050512937489 PMC 155411 · doi ↗ · pubmed ↗
- 6Naumenko Y. Yuryshinetz I. Zabenko Y. Pivneva T. Mild traumatic brain injury as a pathological process Heliyon 20239 e 1834210.1016/j.heliyon.2023.e 1834237519712 PMC 10372741 · doi ↗ · pubmed ↗
- 7Lumba-Brown A. Niknam K. Cornwell J. Meyer C. Ghajar J. Sex-related differences in neurosensory alterations following blunt head injury Front. Neurol.202011105110.3389/fneur.2020.0105133041988 PMC 7522405 · doi ↗ · pubmed ↗
- 8Gosselin N. Bottari C. Chen J.K. Huntgeburth S.C. De Beaumont L. Petrides M. Cheung B. Ptito A. Evaluating the cognitive consequences of mild traumatic brain injury and concussion by using electrophysiology Neurosurg. Focus 201233 E 710.3171/2012.10.FOCUS 1225323199430 · doi ↗ · pubmed ↗