Prevalence and Outcomes of HER2-Low Versus HER2-0 Status in Patients with Metastatic Breast Cancer
Akshara Singareeka Raghavendra, Diane D. Liu, Senthil Damodaran, Sarah Pasyar, Yu Shen, Jason A. Mouabbi, Carlos H. Barcenas, Kelly K. Hunt, Debu Tripathy

TL;DR
HER2-low breast cancer is common in metastatic cases and is linked to better survival than HER2-0, with changes in HER2 status between primary and metastatic tumors showing the need for reassessment.
Contribution
This study provides real-world evidence on the prevalence and outcomes of HER2-low metastatic breast cancer and highlights the importance of reassessing HER2 status due to tumor heterogeneity.
Findings
HER2-low disease was common in both de novo and recurrent metastatic breast cancer.
HER2-low status was associated with longer overall survival compared to HER2-0 disease.
HER2 status often changed between primary tumors and metastatic sites, especially in recurrent disease.
Abstract
Breast cancers with low levels of HER2 expression (HER2-low) represent a large proportion of tumors traditionally classified as HER2-negative and have recently become clinically relevant with the availability of effective HER2-targeted antibody–drug conjugates. In this large, real-world cohort of patients with metastatic breast cancer, we found that HER2-low disease was common in both de novo and recurrent metastatic settings and was associated with longer overall survival compared with HER2-0 disease. We also observed frequent changes in HER2 status between primary tumors and metastatic sites, particularly in recurrent disease, highlighting tumor heterogeneity and the dynamic nature of HER2 expression over time. These findings support routine reassessment of HER2 status in metastatic breast cancer prior to changing therapy when feasible and underscore the need for more accurate and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
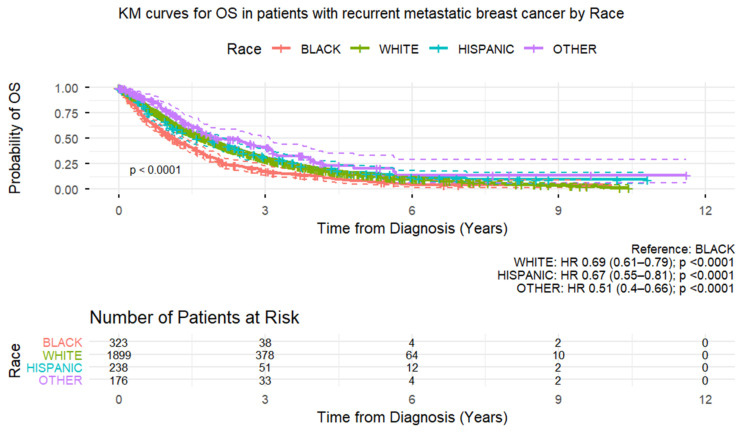 Figure 1
Figure 1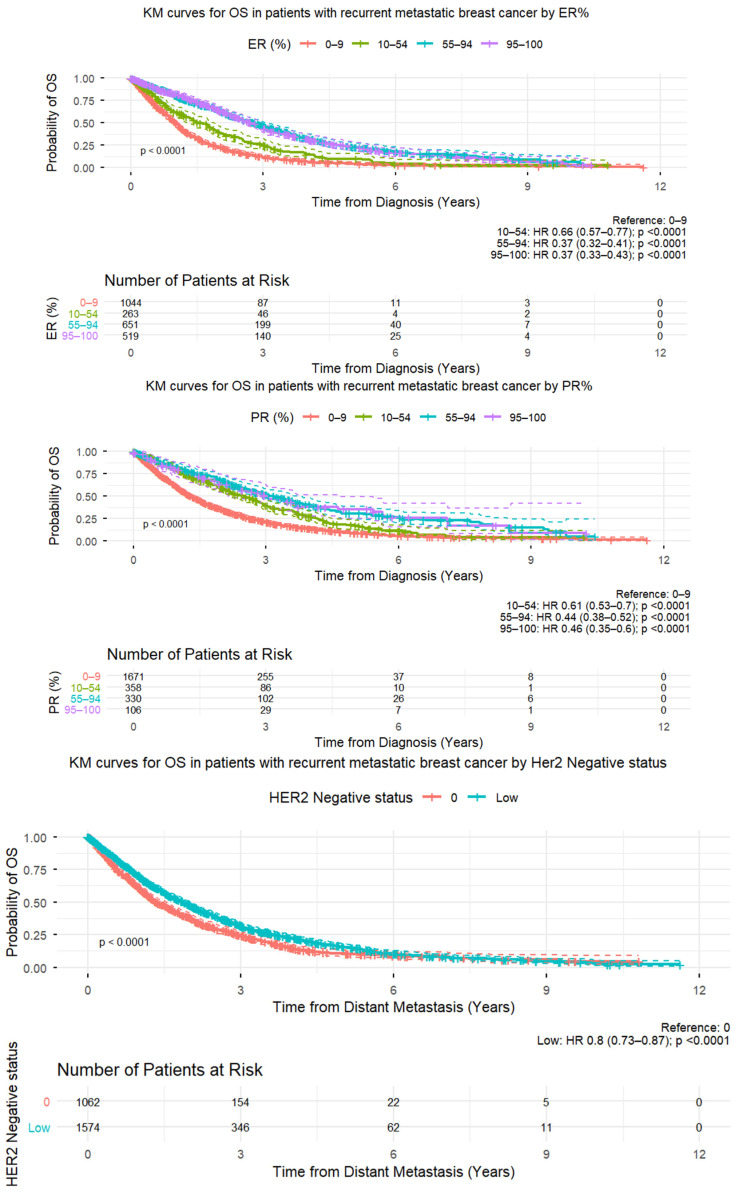 Figure 2
Figure 2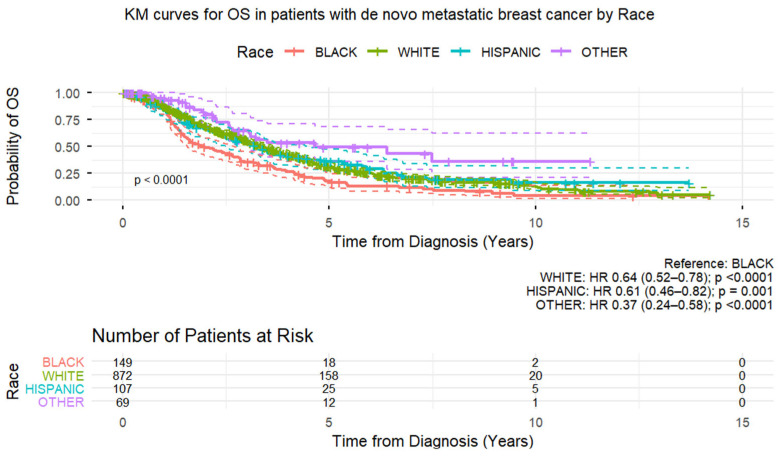 Figure 3
Figure 3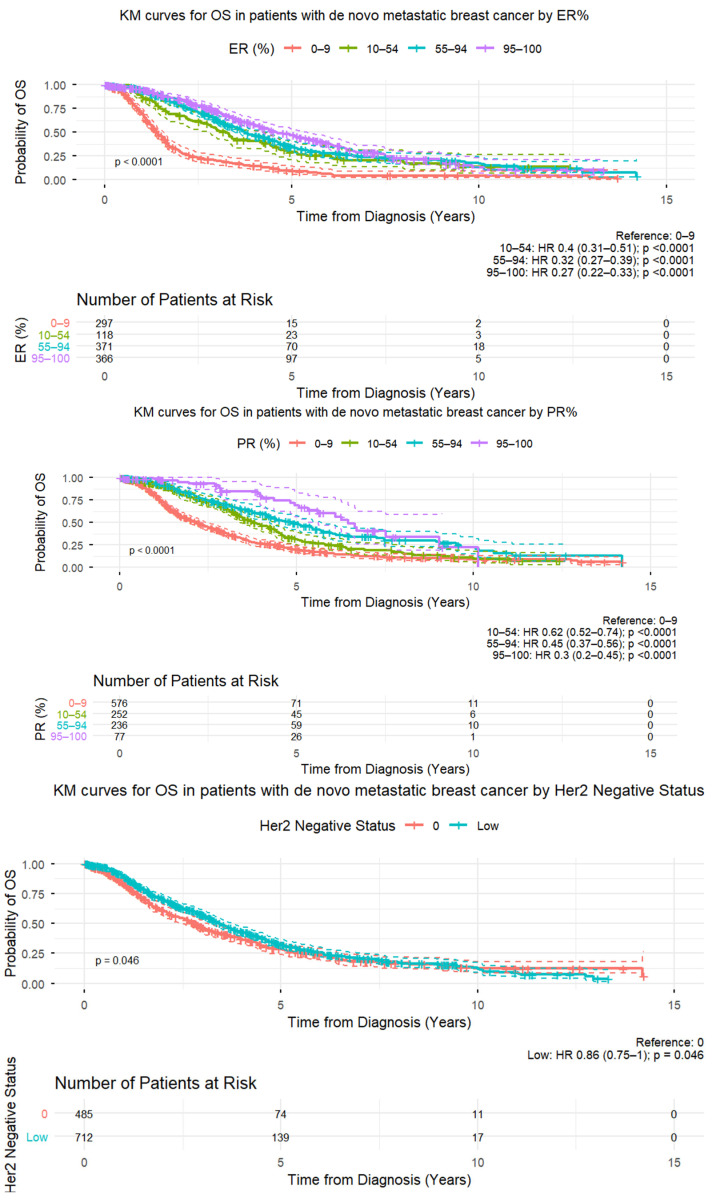 Figure 4
Figure 4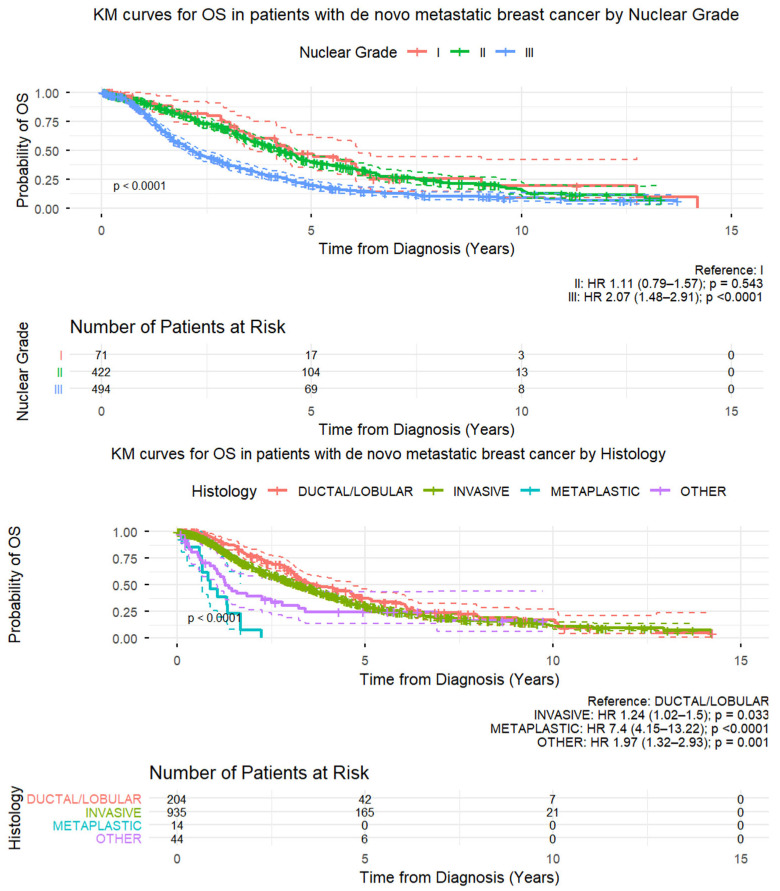 Figure 5
Figure 5- —Department of Defense
- —MD Anderson Cancer Center Support
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Advanced Breast Cancer Therapies · Breast Cancer Treatment Studies
1. Introduction
Breast cancer is a complex and heterogeneous disease with various cell receptor and molecular subtypes that have distinct characteristics and responses to treatment. Human epidermal growth factor receptor 2 (HER2)-low breast cancer, defined by low levels of HER2 protein expression (measured by immunohistochemical [IHC] analysis) in classically HER2-negative tumors, ref. [1] has emerged as an important subtype, challenging the traditional understanding of HER2 status as binary (positive or negative).
Recent multi-omics and real-world studies [2,3] suggest HER2-low tumors comprise ~55–65% of all HER2-negative breast cancers, though classification remains variable due to poor reproducibility between pathologists (with agreement between IHC 0 and 1+ as low as 25–30%).
Current HER2 diagnostic tests were designed to identify cancers most sensitive to treatment with trastuzumab, a monoclonal antibody that targets HER2, and thus are optimized for cancers with high levels of HER2 overexpression [4]. However, evidence from a phase 3 study (DESTINY-Breast04) demonstrated the efficacy of the antibody–drug conjugate trastuzumab deruxtecan (T-DXd) in a proportion of patients with tumors classified as HER2-negative, suggesting the need for diagnostics that can identify patients who may benefit from novel HER2-targeted therapies that demonstrate efficacy at levels of HER2 expression lower than those currently defined as HER2 positivity [5]. Findings from the DESTINY-Breast06 trial [6] further validated HER2-low as a therapeutically relevant classification, especially in hormone receptor-positive (HR+) metastatic breast cancer (MBC), [7,8] emphasizing the need for consistent, accurate HER2 IHC interpretation and the development of novel companion diagnostics. Since the US Food and Drug Administration (FDA) granted approval for T-DXd in patients with HR+/HER2-ultralow metastatic breast cancer on 27 January 2025, the distinction between HER2-0 and HER2-ultralow has become clinically relevant.
The HER2 gene, also known as ERBB2, encodes the HER2 receptor protein, a transmembrane tyrosine kinase receptor that plays a crucial role in regulating cell growth, differentiation, and survival. Normal breast epithelial cells typically have one copy of the HER2 gene on each chromosome 17 and express HER2 protein at detectable levels [9]. When amplified or overexpressed, the HER2 gene drives oncogenic signaling that promotes proliferation, survival, and malignant transformation in breast cancer [10]. Historically, HER2-positive breast cancer, representing about 20% of all breast cancer cases, is characterized by high HER2 protein expression [11] and has been associated with aggressive tumor behavior and poorer clinical outcomes.
Breast cancer with low levels of HER2 protein expression below the positivity threshold represents a substantial proportion of cases, estimated to be around 40–50%, [12] and was previously categorized as HER2-negative. However, HER2-low breast cancer exhibits unique molecular characteristics that distinguish it from both HER2-positive and HER2-negative subtypes. Gene expression profiling studies [13,14] have revealed differences in the genomic aberrations like copy number alterations and transcriptomic profiles of HER2-low breast tumors, indicating distinct signaling pathways; however, some studies [15,16] have shown no genomic difference between HER2-0 and HER2-low tumors. This heterogeneity suggests that distinct mechanisms may drive the growth and progression of HER2-low breast cancer, requiring tailored treatment strategies.
The main goals of this study were to measure the prevalence of HER2-low status (IHC 1+ or IHC 2+ and fluorescence in situ hybridization [FISH] negative) in a large cohort of patients with MBC, identify clinicopathological/treatment associations, and compare overall survival (OS) between patients with HER2-0 (IHC 0) and HER2-low MBC. Furthermore, this study characterized the discrepancy in HER2 status between the primary tumor and metastatic lesions, as well as temporal variations in HER2 expression across multiple time points.
2. Patients and Methods
2.1. Patient Population
The Breast Cancer Management System database of the Department of Breast Medical Oncology encompasses a comprehensive record of breast cancer patients referred to The University of Texas MD Anderson Cancer Center since the 1990s. This database was queried to include patients aged 18 or older at diagnosis and evaluated at MD Anderson between January 2006 and January 2019 with a confirmed diagnosis of recurrent or de novo stage IV MBC with HER2-0 or HER2-low expression in the primary breast tumor, regardless of HR status. Patients with recurrent MBC were initially treated for stage I-III breast cancer with later (more than 90 days after diagnosis) development of distant recurrence, while de novo MBC was defined as stage IV breast cancer identified within 90 days of initial diagnosis; these groups were differentiated for the purposes of a sensitivity analysis. The HER2 status was determined using either IHC or gene amplification using fluorescence in situ hybridization (FISH) to assess the presence of HER2 gene amplification and the corresponding protein expression. HER2-0 expression was defined as IHC 0, while HER2-low was defined as either (1) IHC 1+ or (2) IHC 2+ and negative for gene amplification on FISH. HER2-ultralow cases were not called out, as this analysis antedated the results of the DESTINY-Breast06 trial.
The collected demographic, clinical, and pathological characteristics encompassed age, race/ethnicity, disease stage, clinical nodal status, sites of metastasis, history of neoadjuvant and/or adjuvant treatments, prior lines of systemic treatments in the metastatic setting, and disease status at the time of last contact or death. The clinical stages, evaluated at the initial diagnosis or at the time of distant recurrence, were determined in accordance with the American Joint Committee on Cancer guidelines that were current at the time of diagnosis. Biopsy of metastatic sites was performed based on clinical indication criteria, which included site accessibility, diagnostic confirmation, and suspected clinical progression. In addition to HER2 status, HR positivity was defined based on the expression of estrogen receptor (ER) or progesterone receptor (PR), as determined by standard IHC using institutional cutoffs that adhered to the guidelines set by the American Society of Clinical Oncology and the College of American Pathologists (ASCO/CAP) [11].
2.2. Statistical Analysis
Data were summarized using descriptive statistics such as mean, standard deviation, median, and range for continuous variables and frequency and proportion for categorical variables. The association between categorical variables was examined by the chi-squared test or Fisher exact test when appropriate. The Wilcoxon rank sum test was used to examine the differences in continuous variables between two groups. A logistic regression model was used to estimate the association between demographic and clinicopathological characteristics and HER2-negative status. OS time was defined as the duration from the date of diagnosis of metastatic disease until death from any cause. A patient was censored if alive at the time of the last follow-up. OS times were estimated using the Kaplan–Meier method and compared between patient-characteristic groups by the log-rank test. A multivariate Cox proportional hazards regression model was applied to assess the effect of covariates of interest on OS. McNemar’s test was used to assess whether the percentages of patients with HER2-low status differed significantly between the primary tumor and the metastasis site, without adjustments for multiple comparisons. All computations were carried out in SAS 9.4.
3. Results
3.1. Patient Characteristics
This study included 3834 patients with HER2-low or HER2-0 MBC, of which 2637 (69%) patients had recurrent disease and 1197 (31%) had de novo MBC. Among these groups, 1575 (60%) and 712 (59%) patients exhibited HER2-low status, respectively. Table 1 presents the demographic and clinicopathological characteristics of the recurrent disease group stratified into HER2-0 (IHC 0) and HER2-low (IHC 1+ or IHC 2+/FISH−) groups. In multivariate logistic regression analysis, HER2-low status was significantly associated with initial clinical stage (III vs. I, odds ratio [OR] = 1.42, p = 0.005), ER-positivity in the primary tumor (OR = 1.96, p < 0.001), and use of adjuvant radiation therapy (OR = 0.79, p = 0.007) (Table 2).
Table 3 shows the demographic and clinicopathological characteristics of the de novo MBC group stratified into HER2-0 and HER2-low groups. In univariate analysis, HER2-low status was associated with post-menopausal status, higher nuclear grade (2 and 3 vs. 1), and HR+ status (indicated by 55–100% of tumor nuclei being ER-positive). In multivariate logistic regression analysis, the only variable significantly associated with HER2-low status was higher nuclear grade (grade 2 [vs. 1], OR = 2.016, p = 0.0068; grade 3 [vs. 1], OR = 1.869, p = 0.0145) (Table 4).
3.2. Overall Survival
With a median follow-up of 5.7 years, 767 (64%) patients died among the de novo MBC patients. For the recurrent MBC group, with a median follow-up of 4.3 years, 1892 (72%) patients died. The median OS was 3.2 years (95% CI: 3.0–3.5 years) in the de novo MBC group and 1.6 years (95% CI: 1.5–1.8 year) in the recurrent MBC group. In the recurrent MBC group, Supplement Table S1 shows landmark survival rates at 2 and 5 years post-diagnosis within each of the demographic and clinicopathological categories. In the recurrent MBC group, significant predictors of shorter OS time were seen only in the 2-year timeframe and included Black race, higher nuclear grade, presence of lymphovascular invasion, hormone receptor-low/negative, and HER2-negative status. In the multivariate Cox proportional hazards regression model for OS in the recurrent MBC group, shorter OS time was significantly associated with Black race (hazard ratio [HR] = 1.210 [95% CI 1.051–1.392], p = 0.0078), lower ER and PR expression (staining percentage) (ER ≥ 95% [vs. 0–9%] HR = 0.439 [95% CI 0.376–0.513], p < 0.0001; PR ≥ 95% [vs. 0–9%] HR = 0.728 [95% CI 0.547–0.969], p = 0.029), and HER2-negative status (HR = 0.890 [95% CI 0.807–0.981], p = 0.0194) (Table 5 and Figure 1).
In the de novo MBC group, from Supplement Table S2, significant predictors of shorter OS time were seen only in the 1-year timeframe and included Black race, metaplastic histology, higher nuclear grade, presence of lymphovascular invasion, and hormone receptor-negative status. In the multivariate Cox proportional hazards regression model for OS in the de novo MBC group, shorter OS time was significantly associated with Black race (HR = 1.483 [95% CI 1.183–1.859], p = 0.0006), metaplastic histology (HR = 3.146 [95% CI 1.592–6.218], p = 0.0010), higher nuclear grade (grade 3 [vs. 1] HR = 1.673 [95% CI 1.145–2.446], p = 0.0079), lower ER and PR expression (staining percentage) [ER ≥ 95% [vs. 0–9%] HR = 0.413 [95% CI 0.318–0.536], p < 0.0001; PR ≥ 95% [vs. 0–9%] HR = 0.527 [95% CI 0.338–0.822], p = 0.0048), and HER2-negative status (HR = 0.774 [95% CI 0.656–0.913], p = 0.0025) (Table 6 and Figure 2).
3.3. Discordance in HER2 Status Between Primary and Metastatic Tumors
HER2-low status was, in general, more common in primary tumors than in metastases. Among the patients with recurrent MBC after a prior diagnosis of early-stage breast cancer, the proportion with HER2-low status (vs. HER2-0) decreased from 61.4% in the primary tumor to 48.3% in the metastasis site (McNemar’s test p < 0.0001) (Table 7). Similarly, among those with de novo MBC, 54.9% had HER2-low disease at the primary site and 50.0% had HER2-low disease at the site of metastasis (McNemar’s test p = 0.0078) (Table 7). Among the 609 recurrent cases, 236 (38.75%) underwent a change—that is, showed discordance—in HER2 status upon distant recurrence, with 158 gaining and 78 losing HER2 expression. This difference was less pronounced in the de novo MBC group, as among 388 in the de novo group, 51 had a change in the HER2 status in the metastasis (a discordance of 13.14%) (Table 7).
3.4. Types of Metastases and the Discordance in HER2 Status with Primary Tumors
We examined HER2 status by types and locations of metastases among those whose HER2 status changed. Non-visceral metastasis was more frequent than visceral metastasis (62.4% non-visceral vs. 37.6% visceral in recurrent MBC and 70.1% vs. 29.9%, respectively, in de novo MBC), and bone was the most frequent metastasis site (40.6% in recurrent and 55.4% in de novo MBC) (Table 8).
Among the MBC recurrent cases, the prevalence of HER2-low status was not different between visceral and non-visceral metastasis. Among the 229 patients (37.6% of the recurrent MBC group) with visceral metastasis, 143 (62.5%) had HER2-low primary tumors and 108 (47.2%) had HER2-low metastatic tumors (p < 0.0001). Among the 380 (62.39%) with non-visceral metastasis, 231 (60.8%) had a HER2-low primary tumor, and 186 (48.9%) had a HER2-low metastatic tumor (p = 0.0003) (Table 9).
In the de novo MBC group, the 116 (29.9%) patients with visceral metastasis showed notable similarity between primary and metastatic tumors, as 56.0% had HER2-low primary tumors and 51.7% had HER2-low metastatic tumors (p = 0.1655). Among the 272 (70.1%) with non-visceral metastasis, 60.8% had a HER2-low primary tumor and 49.3% had a HER2-low metastatic tumor (p = 0.0231) (Table 10).
4. Discussion
In patients with recurrent MBC and patients with de novo MBC, HER2-low status was significantly associated with a longer OS compared to HER2-0 status. Initial disease stage, ER-positivity, and use of adjuvant radiation therapy were associated with HER2-low status in the recurrent MBC group, while higher nuclear grade was significantly associated with HER2-low status in the de novo MBC group. Also, a notable discrepancy in HER2 status was observed between the primary breast cancers and distant metastases. This correlation suggests a potential link between the biological characteristics of the primary tumor and the development of recurrent metastatic disease in the context of HER2 status in individuals with early-stage or de novo MBC. These differences in phenotypes and outcomes between HER2-0 and HER2-low status could be, in part, due to the association between HER2-0 with ER-positivity; however, these differences persisted in the multivariate analysis that included ER.
The phase 3 DESTINY-Breast06 trial [6] demonstrated superior progression-free survival with trastuzumab deruxtecan versus standard chemotherapy in patients with HR+ HER2-low (and -ultralow) MBC, redefining therapeutic thresholds. Importantly, this trial included a central pathology review, helping to mitigate the variability in HER2 classification that has limited prior real-world comparisons.
Emerging data [17] suggest further stratification within the HER2-low group, with ultralow (IHC >0 but <1+) tumors showing intermediate response rates to HER2-directed antibody–drug conjugates. This may prompt future updates to IHC scoring criteria and therapeutic algorithms.
Recent studies [18,19] have confirmed substantial intrapatient heterogeneity and HER2 status evolution, particularly in response to systemic therapy.
HER2-low breast cancer has unique molecular characteristics and clinical behavior that distinguish it from both HER2-positive and HER2-negative disease [12]. The precise definition of HER2-low breast cancer is still evolving, and there is currently no universally accepted formal definition [9]. Conventionally, HER2-low breast cancers are defined based on an IHC score of 1+ or an IHC score of 2+ with a negative result on in situ hybridization [9].
The concept of HER2-low emerged as a response to the realization that some breast cancers have HER2 expression levels that are not high enough to be considered HER2-positive but may still have the potential to respond to certain therapies, particularly those targeting HER2. Prior analyses have shown that within the traditional HER2-negative category, there is heterogeneity in HER2 expression [20]. The HER2-low category has emerged as a result of improvements in the detection and quantification of HER2 expression as well as the development of novel antibody–drug conjugates that are posited to have both direct and bystander effects through targeting the surrounding tumor microenvironment, thus affecting cells with lower or no HER2 expression on IHC, thereby increasing the therapeutic impact [1].
The legacy HER2 IHC assay was developed as a companion diagnostic for ERBB2-targeting monoclonal antibodies such as trastuzumab. However, there exists significant discordance and less reliability between pathologists in scoring IHC 0, 1+, and 2+ cases [21]. Furthermore, this study’s results align with findings from other studies that employed different methodologies, indicating a high level of disagreement among pathologists when scoring HER2 IHC 0 versus non-0 cases. Specifically, the ONEST (Observers Needed to Evaluate Subjective Tests) method reported a substantial 40.6% disagreement in this regard [22]. These findings suggest that the legacy HER2 IHC assay is likely to be inaccurate and insufficient for making clinical decisions, particularly in prescribing HER2-low-specific treatments like trastuzumab deruxtecan [23]. Research is ongoing to better understand and quantify HER2-low breast cancer and develop effective treatment strategies for this subtype, especially advanced/metastatic cases [9]; thus, the lack of standardization in the classification of HER2-low breast cancers also poses challenges to obtaining accurate and reproducible results [9]. Improved histological assessment using immuno-fluorescent HER2 staining or other quantitative techniques is needed and is in the process of being prospectively tested in the TBCRC 066 trial [24]. In another study, involving 18 pathologists, breast cancer biopsies examined using the standard IHC scale were rated with only a 26% agreement between scores 0 and 1+; a higher concordance of 58% was found between scores 2+ and 3+ [21].
The classification of HER2-low breast cancer has significant clinical implications, as it may require alternative treatment approaches compared to HER2-positive breast cancer. While HER2-positive breast cancers have been associated with higher stage, positive lymph nodes, higher proliferation rate, and lack of expression of hormone receptors, traditional HER2-targeted therapies, such as trastuzumab have shown limited efficacy in HER2-low breast cancer [25]. However, more potent or higher affinity HER2-targeted therapies are showing activity in HER2-low breast cancer. These agents include new antibodies, small-molecule inhibitors, and immune-based therapies that may exploit the unique molecular characteristics of HER2-low tumors. In a phase 3 trial (DESTINY-Breast04) [26] involving patients with HER2-low MBC, treatment with trastuzumab deruxtecan showed a median progression-free survival of 10.1 months compared to 5.4 months with the physician’s choice of treatment (HR = 0.51, p < 0.001). Trastuzumab deruxtecan also showed significantly longer OS at 23.9 months (about 2 years) vs. 17.5 months (HR = 0.64, p = 0.003). The phase II DAISY trial [27] demonstrated that trastuzumab deruxtecan (T-DXd) achieved high activity across varying levels of HER2 expression, with objective response rates of 70.6% in patients with HER2-overexpressing disease, 37.5% in HER2-low, and 29.7% in HER2-0 metastatic breast cancer (N = 177). While responses correlated with HER2 expression and drug uptake, activity in some HER2-0 tumors suggested that additional, HER2-independent mechanisms may contribute to efficacy. Additionally, understanding the interplay between HER2-low breast cancer and the tumor microenvironment may provide insights into the potential role of immunotherapy in this subtype [28].
Our study found a 38.75% discordance in the recurrent MBC group and a 13.14% discordance in the de novo MBC group in HER2-low status (vs. HER2-0) between primary and metastatic sites. The discordance between primary and metastatic HER2 status can be due to several factors, including interobserver variability among pathologists, [21] tumor heterogeneity and subclonal selection over time under selective pressure, and a drift to ER-negative and/or HER2-negative status because of exposure to therapy [29,30,31]. This discordance highlights the need for careful evaluation of recurrent/progressive disease, particularly more rapidly proliferating lesions. Interestingly, there were lesser differences between primary and metastatic HER2-low status found in the de novo MBC group, both in the visceral metastasis subset and in the entire de novo MBC group.
Limitations of our study include its retrospective nature and lack of central pathology review, although all cases were reviewed by pathologists at our institution. Central pathology review is particularly relevant for HER2-low classification, as prior studies have demonstrated interobserver variability in distinguishing IHC 0 from 1+, which may have influenced prevalence estimates and observed HER2 discordance. Interpretation of HER2 discordance should also account for clinical and treatment-related factors. Intervening systemic therapies may influence HER2 expression over time; however, limited granularity regarding treatment timing and sequencing precluded formal modeling of predictors of HER2 status change. Accordingly, discordance analyses stratified by disease presentation (recurrent versus de novo) and hormone receptor status should be interpreted as exploratory. Although multivariable models were adjusted for key clinicopathologic variables, treatment-related confounding during the metastatic phase could not be fully addressed. As a result, the observed association between HER2-low status and improved overall survival may reflect, in part, underlying hormone receptor biology and treatment responsiveness rather than a purely independent prognostic effect. Finally, subgroup analyses were not adjusted for multiple comparisons and should be considered hypothesis-generating. Missing covariates, including menopausal status, body mass index, and lymphovascular invasion were handled using available-case analyses, and residual bias due to missing data is possible. In addition to the absence of central pathology review, this study did not incorporate AI-based HER2 scoring tools, which have shown promise in reducing interobserver variability and improving identification of HER2-low cases.
Going forward, these findings underscore the importance of accurate HER2 classification, reassessment of HER2 status at diagnosis of metastatic recurrence, and further prospective validation of treatment approaches—especially those involving antibody–drug conjugates—in HER2-low metastatic breast cancer.
5. Conclusions
In this large real-world cohort of metastatic breast cancer, HER2-low disease was common and was associated with longer overall survival compared with HER2-0 disease in both de novo and recurrent settings. Clinically meaningful discordance in HER2 status between primary and metastatic tumors was observed, underscoring the dynamic nature of HER2 expression. These findings support reassessment of HER2 status at metastatic progression and reinforce the clinical relevance of HER2-low breast cancer in the era of HER2-targeted antibody–drug conjugates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agostinetto E. Rediti M. Fimereli D. Debien V. Piccart M. Aftimos P. Sotiriou C. de Azambuja E. HER 2-low breast cancer: Molecular characteristics and prognosis Cancers 202113282410.3390/cancers 1311282434198891 PMC 8201345 · doi ↗ · pubmed ↗
- 2Turova P. Kushnarev V. Baranov O. Butusova A. Menshikova S. Yong S.T. Nadiryan A. Antysheva Z. Khorkova S. Guryleva M.V. The Breast Cancer Classifier refines molecular breast cancer classification to delineate the HER 2-low subtypenpj Breast Cancer 2025111910.1038/s 41523-025-00723-039979291 PMC 11842814 · doi ↗ · pubmed ↗
- 3Baez-Navarro X. van Bockstal M.R. Andrinopoulou E.-R. van Deurzen C.H. HER 2-low breast cancer: Incidence, clinicopathologic features, and survival outcomes from real-world data of a large nationwide cohort Mod. Pathol.20233610008710.1016/j.modpat.2022.10008736788086 · doi ↗ · pubmed ↗
- 4Pauletti G. Godolphin W. Press M.F. Slamon D.J. Detection and quantitation of HER-2/neu gene amplification in human breast cancer archival material using fluorescence in situ hybridization Oncogene 19961363728700555 · pubmed ↗
- 5Modi S. Park H. Murthy R.K. Iwata H. Tamura K. Tsurutani J. Moreno-Aspitia A. Doi T. Sagara Y. Redfern C. Antitumor activity and safety of trastuzumab deruxtecan in patients with HER 2-low–expressing advanced breast cancer: Results from a phase Ib study J. Clin. Oncol.202038188710.1200/JCO.19.0231832058843 PMC 7280051 · doi ↗ · pubmed ↗
- 6Bardia A. Hu X. Dent R. Yonemori K. Barrios C.H. O’Shaughnessy J.A. Wildiers H. Pierga J.Y. Zhang Q. Saura C. Trastuzumab Deruxtecan after Endocrine Therapy in Metastatic Breast Cancer N. Engl. J. Med.20243912110212210.1056/NEJ Moa 240708639282896 · doi ↗ · pubmed ↗
- 7Salgado R.F. Bardia A. Curigliano G. Hu X. Dent R.A. Pierga J.Y. Tsurutani J. Wildiers H. Ricciardi G.R.R. MarchiòC. LBA 21 Human epidermal growth factor receptor 2 (HER 2)-low and HER 2-ultralow status determination in tumors of patients (pts) with hormone receptor–positive (HR+) metastatic breast cancer (m BC) in DESTINY-Breast 06 (DB-06)Ann. Oncol.202435 S 1213 S 121410.1016/j.annonc.2024.08.2259 · doi ↗
- 8Curigliano G. Hu X. Dent R.A. Yonemori K. Barrios C.H. O’Shaughnessy J. Wildiers H. Zhang Q. Im S.-A. Saura C. Trastuzumab deruxtecan (T-D Xd) vs physician’s choice of chemotherapy (TPC) in patients (pts) with hormone receptor-positive (HR+), human epidermal growth factor receptor 2 (HER 2)-low or HER 2-ultralow metastatic breast cancer (m BC) with prior endocrine therapy (ET): Primary results from DESTINY-Breast 06 (DB-06)J. Clin. Oncol.202442 LBA 100010.1200/JCO.2024.42.17_suppl.LBA 1000 · doi ↗