HPV vaccination hesitancy and acceptance among parents in Saxony-Anhalt, Germany: the role of gender, awareness and fear
Paolo Gennari, Daniel Schlund, József Mészáros, Atanas Ignatov

TL;DR
A survey in Germany found that mothers are more aware of HPV and more willing to vaccinate their children than fathers, with gender dynamics and fear influencing vaccination decisions.
Contribution
This study identifies gender-specific patterns in HPV vaccine acceptance and highlights the need for targeted strategies to engage fathers and address misperceptions.
Findings
Mothers were significantly more aware of HPV and more willing to vaccinate than fathers.
Parents of daughters expressed greater fear of HPV-associated disease than parents of sons.
Logistic regression identified awareness, fear of disease, and higher education as determinants of vaccination willingness.
Abstract
Despite national recommendations in Germany for universal HPV vaccination, uptake remains suboptimal—particularly among boys. Parental awareness, gender dynamics, and hesitancy play key roles in vaccination decisions. A cross-sectional survey was conducted among 406 parents of children aged 9–14 years in Magdeburg, Saxony-Anhalt. An anonymized online questionnaire assessed HPV-associated awareness, attitudes, willingness to vaccinate, and conditions under which hesitant parents might reconsider. Statistical analyses included chi-square tests and logistic regression. Parent–child gender dyads were examined to explore interaction effects. Vaccine hesitancy was conceptualized along a continuum from acceptance to refusal, although for analysis we contrasted parents willing to vaccinate with those refusing vaccination. Mothers were significantly more aware of HPV than fathers (86.8% vs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
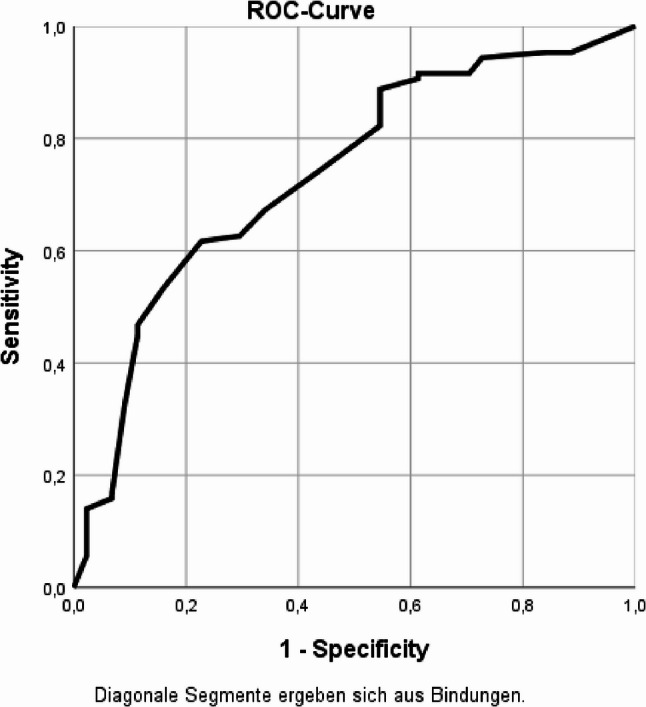 Figure 1
Figure 1- —Otto-von-Guericke-Universität Magdeburg (3121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Vaccine Coverage and Hesitancy · Herpesvirus Infections and Treatments
Introduction
Human papillomavirus (HPV) is one of the most common sexually transmitted infections worldwide and is causally linked to several types of cancer, including cervical, anal, penile, and oropharyngeal malignancies. Persistent infection with high-risk HPV types is responsible for nearly all cases of cervical cancer, making prevention through vaccination a critical public health priority [1].
In Germany, HPV vaccination has been recommended by the Standing Committee on Vaccination (STIKO) since 2007 for girls and since 2018 also for boys, ideally between the ages of 9 and 14. Despite this, national uptake remains suboptimal: in 2021, only 52% of 15-year-old girls and 27% of boys had completed the HPV vaccination series, falling short of WHO’s goal of 90% coverage for cervical cancer elimination [2]. In Saxony-Anhalt, vaccination coverage is even lower, with less than 45% of girls and fewer than 20% of boys completing the series (Robert Koch Institute, 2022; Saxony-Anhalt Regional Health Authority, 2023). These figures underline the challenge of moderate uptake in this region.
Although HPV vaccination is recommended nationally, implementation strategies vary across federal states and there is no unified school-based delivery system. Regional and structural context may therefore influence vaccination practices. Previous public health monitoring in Germany has documented regional differences in vaccination behaviour: for example, studies during the COVID-19 vaccination campaign found lower uptake among residents of rural areas and in eastern federal states compared with urban and western regions, suggesting that access barriers, health system trust, and socio-demographic composition may play a role [3, 4]. While comparable data for HPV vaccination specifically are limited, these patterns indicate that contextual and structural factors may also contribute to the comparatively low HPV vaccination uptake observed in Saxony-Anhalt.
In recent years, international research has highlighted substantial variation in HPV vaccination uptake, parental acceptance, and hesitancy across countries, settings, and population sub-groups. A recent systematic review of 86 studies found that, while many parents support HPV vaccinations for their children, acceptance rates vary widely—ranging from very low in some settings to quite high in others—with key influencing factors including parental knowledge, perceived safety, cost, and healthcare provider recommendation [5]. Within Europe, a 2024 meta-analysis shows that parents’ hesitancy is associated with socio-demographic features (such as immigrant status, employment status, religion), psychological factors such as risk perception and safety concerns, as well as communication and awareness [6]. Globally, interventions to increase uptake (beyond just awareness raising) — including school-based vaccination programs, multicomponent and systems-level strategies, provider reminders, and decision support — have proved more effective [7–9]. These findings suggest that any study of HPV vaccine uptake (or intent to vaccinate) needs to account for not only the immediate local context (policies, cost, access), but also the broader social, economic, and communication environment, since those international patterns may help explain observed similarities or differences.
Parental attitudes and beliefs are among the most decisive determinants of HPV vaccination uptake in minors. Prior studies have shown that awareness of HPV and its consequences, trust in healthcare providers, fear of side effects, and sociocultural perceptions of sexuality significantly shape vaccination intentions. Moreover, gender norms and role expectations influence both parental engagement and vaccine acceptance. For instance, fathers are generally less informed about HPV and less involved in vaccination decisions, particularly for daughters [10–13].
While much of the existing literature originates from Anglo-American or pan-European contexts, local cultural factors may substantially affect attitudes toward vaccination. To our knowledge, no recent study has systematically assessed HPV-associated awareness and hesitancy among German parents since the expansion of vaccination recommendations to include boys. Furthermore, dyadic analyses that explore the interaction between the gender of the parent and the child are lacking, despite their relevance for communication strategies and public health outreach. Unlike most prior studies, which analyze parents in aggregate, our study applied a dyadic approach to examine how parent–child gender combinations influence HPV vaccination attitudes. This perspective has not yet been systematically explored in Germany and provides new insight into local drivers of vaccine hesitancy.
Beyond socio-demographic and contextual factors, contemporary models of vaccine behaviour emphasize psychological antecedents such as confidence, complacency, constraints, and social norms. The 7 C model of vaccine acceptance, validated among parents and adolescents in Europe, summarises these determinants as confidence, complacency, constraints, calculation, collective responsibility, confidence in the health system, and social conformity [14, 15]. Constructs examined in our study, such as HPV awareness, fear of HPV-associated disease, and educational level, can be mapped onto these dimensions, for example awareness and fear reflecting confidence and perceived disease threat, and education relating to calculation and access to trustworthy information. Positioning our findings within this framework facilitates comparison with international vaccine hesitancy research and highlights modifiable targets for intervention.
This study aimed to assess HPV-associated awareness, attitudes, and willingness to vaccinate among parents of school-aged children (aged 9–14 years) in Magdeburg, Saxony-Anhalt. We investigated differences by parent and child gender, explored parent–child dyad patterns, identified determinants of vaccination willingness, and examined conditional factors under which hesitant parents might reconsider. By capturing local attitudes in a region with moderate uptake, this study aims to inform targeted interventions to improve HPV vaccination coverage in Saxony-Anhalt.
Materials and methods
Study design and participants
This cross-sectional study was conducted in Magdeburg, Germany, during the first quarter of 2025. The target population consisted of parents or legal guardians of children aged 9–14 years, corresponding to the recommended age range for HPV vaccination under German guidelines. Participants were recruited via a digital, anonymized questionnaire (see Supplementary File 1) distributed through four middle schools in Magdeburg. A total of 12 schools in the Magdeburg municipal area were contacted and invited to support the study by distributing the survey link to parents. Four schools agreed to participate and shared the link via their existing communication platforms. Schools declining participation cited limited administrative capacity or internal data privacy concerns. No objections regarding the study content were reported. Within these schools, approximately 1195 eligible students were enrolled in the relevant age group, and 406 parents provided complete responses, yielding an estimated response rate of 33.9%. Only fully completed questionnaires were included in the analysis. Partially completed surveys and responses with missing data on the main outcome were excluded, and no imputation of missing values was performed. Before accessing the survey, parents viewed an electronic consent statement outlining study aims, anonymity, and voluntary participation. Consent was provided by selecting an ‘I agree’ checkbox, which was required to proceed. Inclusion criteria were: [1] being the parent or legal guardian of a child aged 9–14 years; [2] residing in the Magdeburg area; and [3] provision of informed consent for anonymous participation.
Questionnaire and variables
The questionnaire comprised five sections. The first section collected sociodemographic characteristics, including the parent’s age, gender, marital status, education level, occupation, and annual household income. The second section focused on child characteristics, specifically age and gender. The third section assessed HPV awareness by asking whether the parent had heard of HPV or HPV-associated diseases. The fourth section addressed HPV vaccination awareness and attitudes, including whether the parent had heard of the HPV vaccine, actively sought information, and whether they were willing to vaccinate their child. The fifth section explored barriers and conditions for acceptance through multiple-response items assessing which circumstances might persuade vaccine-hesitant parents to accept HPV vaccination.
HPV vaccination status of the child was self-reported. The main outcome variable, willingness to vaccinate, was defined as answering “yes” to the question “Would you have your child vaccinated against HPV?”. In line with contemporary literature, vaccine hesitancy is understood as a position on a continuum between full acceptance and refusal, including indecision and delay. In the present analysis, we contrasted parents who were willing to vaccinate with those who answered “no” to this question, whom we classified as refusing HPV vaccination. We therefore refer to this subgroup as ‘refusing’ in a strict behavioural sense, while acknowledging that broader conceptualisations of hesitancy also encompass more ambivalent positions. For analytical purposes, parent–child gender dyads (e.g., mother–daughter, father–son) were constructed to explore interaction effects.
The questionnaire was developed specifically for this study, with items adapted from previously validated instruments in European studies on parental vaccine hesitancy and HPV vaccination [10–13]. The questionnaire underwent cognitive pre-testing with five parents from the target population to assess clarity and comprehension. Minor wording adjustments were made based on feedback. Given that most items were adapted from validated European instruments, no additional psychometric validation (e.g., Cronbach’s alpha) was conducted. An English version of the full questionnaire is provided as Supplementary File 1.
No a priori power calculation was performed, as recruitment feasibility depended on school participation. However, the final sample exceeded minimum recommended thresholds for logistic regression modelling based on events-per-variable guidelines.
Statistical analysis
Descriptive statistics were calculated to characterize the sample. Pearson’s chi-square test was used to assess associations between sociodemographic variables and awareness or attitudes. Variables were entered into the logistic regression model based on (a) significance in bivariate analysis (p < 0.10) and (b) theoretical relevance according to established vaccine hesitancy research frameworks. Multicollinearity was assessed using variance inflation factors (VIF), and no variable exceeded acceptable thresholds (VIF < 2.5). Model performance was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC).
All analyses were performed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY), with statistical significance defined as p < 0.05.
Results
Sample characteristics
A total of 406 parents of school-aged children (aged 9–14 years) in Magdeburg, Germany, completed the questionnaire (Table 1). The sample was predominantly female (74.6%), with a mean age of 40.9 years (SD = 6.3). Children were evenly split by gender. Most respondents were married (54.8%) and had completed vocational training or a university degree (65.1%). The most common employment sectors were healthcare/social services (35.1%) and office/administration (29.7%). Annual household income varied, with 26.5% earning €40,000–60,000 per year.
Table 1. Demographic characteristics of parents of school-aged children in Magdeburg, GermanyCharacteristicFrequency (n)Percent (%)Age of parents (mean ± SD)–40.9 ± 6.3Gender of parents Female30374.6 Male10325.4Age of child (years)–9–14 (modal age = 12)Gender of child Female20350.0 Male20350.0Marital status Married22354.8 In a registered partnership5814.3 Single6115.0 Divorced4110.1 Widowed235.7Highest educational qualification Lower secondary education297.1 Intermediate secondary education4210.3 University entrance qualification6716.5 Vocational training or university degree26565.1 No response30.7Employment sector Industrial/production work399.6 Service sector7117.4 Healthcare/social services14335.1 Office/administration12129.7 Unemployed327.9Annual gross income (€) ≤ 20,0004410.8 20,000–40,0009924.3 40,000–60,00010826.5 60,000–100,0009623.6 > 100,000317.6 No response286.9
Awareness and attitudes by parent gender
Mothers were significantly more likely than fathers to have heard of HPV (86.8% vs. 68.0%; p < 0.001) and of the HPV vaccine (96.4% vs. 89.3%; p = 0.006), and to have actively sought information (68.3% vs. 44.7%; p < 0.001). Willingness to vaccinate was higher among mothers than fathers (90.4% vs. 74.8%; p < 0.001). Mothers were also more likely to agree that HPV vaccination should occur before first sexual intercourse (86.8% vs. 62.1%; p < 0.001) and to prefer vaccination at 9–11 years (63.7% vs. 39.8%; p < 0.001) (Table 2).
Table 2HPV-associated awareness and attitudes by gender of parent and child (Magdeburg)QuestionParent Female (N = 303)Parent Male (N = 103)p-valuechild female (N = 203)child male (N = 203)p-valueHave you heard of HPV? Yes263 (86.8%)70 (68.0%)< 0.001168 (82.8%)165 (81.2%)0.698 No40 (13.2%)33 (32.0%)35 (17.2%)38 (18.7%)Have you heard of the HPV vaccine? Yes292 (96.4%)92 (89.3%)0.006192 (94.6%)192 (94.6%)1.000 No11 (3.6%)11 (10.7%)11 (5.4%)11 (5.4%)Have you actively sought information about HPV or the vaccine? Yes207 (68.3%)46 (44.7%)< 0.001136 (67.0%)117 (57.6%)0.124 No85 (28.1%)46 (44.7%)56 (27.6%)75 (36.9%)Would you have your child vaccinated against HPV? Yes279 (90.4%)77 (74.8%)< 0.001176 (86.7%)175 (86.2%)0.885 No29 (9.6%)26 (25.2%)27 (13.3%)28 (13.8%)When should HPV vaccination be given to children? before first sexual intercourse263 (86.8%)64 (62.1%)< 0.001168 (82.8%)159 (78.3%)0.231 after first sexual intercourse0 (0%)0 (0%)0 (0%)0 (0%) do not know34 (19.9%)30 (31.6%)8 (3.9%)16 (7.9%)Preferred age for HPV vaccination < 96 (2.0%)5 (2.8%)< 0.0016 (3.0%)41 (39.8%)0.092 9–11193 (63.7%)41 (39.8%)130 (64.0%)17 (16.5%) 12–1461 (20.1%)17 (16.5%)29 (14.3%)1 (1.0%) > 152 (0.7%)1 (1.0%)1 (0.5%)13 (12.6%) do not know12 (4.0%)13 (12.6%)10 (4.9%)15 (7.4%)Are you afraid of your child developing an HPV-associated disease? Yes167 (78.4%)119 (71.3%)0.151137 (67.5%)76 (37.4%)< 0.001 No46 (21.6%)48 (28.7%)57 (28.1%)110 (54.2%)
Awareness and attitudes by child gender
Parental awareness of HPV (82.8% vs. 81.2%; p = 0.698), awareness of the HPV vaccine (94.6% vs. 94.6%; p = 1.000), active information seeking (67.0% vs. 57.6%; p = 0.124), and willingness to vaccinate (86.7% vs. 86.2%; p = 0.885) did not differ significantly between parents of daughters and parents of sons. However, parents of daughters were significantly more likely to report fear of their child developing an HPV-associated disease (67.5% vs. 37.4%; p < 0.001) (Table 2).
Parent–Child gender dyads
Gender combinations of parent–child dyads revealed notable differences in awareness and attitudes (Table 3). Mothers of daughters exhibited the highest HPV awareness (86.5%) and willingness to vaccinate (91.7%). Fathers of daughters, in contrast, reported high fear of HPV-associated disease (74.5%) but lower willingness to vaccinate (70.2%). Fathers of sons consistently showed the lowest HPV awareness (66.1%) and comparatively low willingness (78.6%). Most comparisons across dyads reached statistical significance. The only exception was awareness of HPV-associated diseases, where differences between dyads did not reach significance (p = 0.293).
Table 3– Parent–Child gender dyads and attitudes toward HPV and vaccination (N = 406)ItemMother–Daughter (N = 156)Mother–Son (N = 147)Father–Daughter (N = 47)Father–Son (N = 56)p-valueHeard of HPV Yes135 (86.5%)128 (87.1%)33 (70.2%)37 (66.1%)< 0.001 No21 (13.5%)19 (12.9%)14 (29.8%)19 (33.9%)Heard of HPV-associated disease Yes150 (96.2%)136 (92.5%)44 (93.6%)50 (89.3%)0.293 No6 (3.8%)11 (7.5%)3 (6.4%)6 (10.7%)Fear of HPV-associated disease Yes102 (65.4%)65 (44.2%)35 (74.5%)11 (19.6%)< 0.001 No48 (30.8%)71 (48.3%)9 (19.1%)39 (69.6%) Don’t know6 (3.8%)11 (7.5%)3 (6.4%)6 (10.7%)Heard of HPV vaccine Yes148 (94.9%)144 (98.0%)44 (93.6%)48 (85.7%)0.007 No8 (5.1%)3 (2.0%)3 (6.4%)8 (14.3%)Actively sought information Yes110 (70.5%)97 (66.0%)26 (55.3%)20 (35.7%)< 0.001 No38 (24.4%)47 (32.0%)18 (38.3%)28 (50.0%) Don’t know8 (5.1%)3 (2.0%)3 (6.4%)8 (14.3%)Willing to vaccinate child Yes143 (91.7%)131 (89.1%)33 (70.2%)44 (78.6%)< 0.001 No13 (8.3%)16 (10.9%)14 (29.8%)12 (21.4%)
Predictors of willingness to vaccinate
In logistic regression analysis (Table 4), three determinants of willingness to vaccinate emerged as significant: having heard of HPV (OR = 3.77; 95% CI: 1.48–9.65; p = 0.006), reporting fear of HPV-associated disease (OR = 3.69; 95% CI: 1.45–9.41; p = 0.006), and higher educational level (OR = 1.60; 95% CI: 1.04–2.46; p = 0.032). Parent gender, child gender, active information-seeking behaviour and employment status were entered into the model but were not statistically significant predictors. These results suggest that cognitive and affective factors, rather than demographic characteristics alone, primarily shaped parental intention to vaccinate.
Table 4– Logistic regression analysis: predictors of willingness to vaccinatePredictorBSEWalddfp-valueOR (Exp(B))95% CI (Lower–Upper)Parent gender (male)−0.6980.4692.21210.1370.4980.198–1.248Child gender (male)0.7100.4342.67110.1022.0340.868–4.764Heard of HPV before study1.3280.4797.67610.0063.7721.475–9.648Fear of disease1.3050.4787.45910.0063.6871.445–9.405Actively sought info−0.4180.4680.79910.3710.6580.263–1.647Education (high)0.4690.2194.57910.0321.5991.040–2.457Employment status−0.1950.1871.09310.2960.8230.570–1.186Constant−1.9951.5391.68010.1950.136—
Model performance
The model showed acceptable fit (Hosmer–Lemeshow p = 0.326) and classification accuracy (74.2%). The ROC curve yielded an AUC of 0.736, indicating acceptable discriminatory ability (Fig. 1).
Fig. 1ROC curve for the logistic regression model predicting willingness to vaccinate. AUC = 0.736, indicating acceptable model discrimination
Conditions for acceptance among hesitant parents
Among the 55 parents who initially declined HPV vaccination for their child, 80.0% indicated that no listed condition would change their decision. A minority reported that they might reconsider if the vaccine were recommended by a pediatrician (12.7%), endorsed by friends or family (12.7%), included in the national immunization schedule (10.9%), or offered free of cost (9.1%). Other factors, such as school recommendation (7.3%) or additional assurances of safety (7.3%), were less frequently cited. Stratification by parent–child dyad revealed no consistent pattern of responsiveness (Table 5).
Table 5. Conditions under which Vaccine-Hesitant parents would accept HPV vaccinationConditionTotal (N = 55)Mother–DaughterMother–SonFather–DaughterFather–SonIf recommended by pediatrician7 (12.7%)5101If recommended by school4 (7.3%)2101If friends/family recommend7 (12.7%)4102If included in national schedule (STIKO)6 (10.9%)5001If free of cost5 (9.1%)4100If safety is guaranteed4 (7.3%)3001None of the above44 (80.0%)201275
In a follow-up question, hesitant parents were asked to indicate why they would not vaccinate their child. The most frequently selected reasons included concerns about vaccine safety, belief that their child was too young, and the perception that HPV vaccination was unnecessary. These reasons align with international findings indicating safety concerns, low perceived susceptibility, and beliefs about sexual maturity as common determinants of HPV vaccine refusal [11, 16, 17].
Discussion
This study investigated parental awareness, attitudes, and hesitancy toward HPV vaccination among parents in Magdeburg, Saxony-Anhalt. The analysis provides new insights into gendered differences in vaccine awareness and acceptance, determinants of willingness to vaccinate, and the underlying reasons for persistent hesitancy. International evidence shows that similar patterns are observed across diverse settings. Systematic reviews covering Europe, North America, Asia, and Africa consistently identify parental awareness, perceived risk of HPV-associated disease, and trust in healthcare providers as central drivers of vaccine acceptance [5, 6]. Conversely, concerns about vaccine safety and cultural perceptions of sexuality remain among the most common barriers [17, 18]. By positioning our findings within this global context, we can better understand how local attitudes in Saxony-Anhalt both align with and diverge from international experience.
Recent conceptual models emphasise that vaccine intention is shaped not only by knowledge but also by psychological determinants such as confidence, complacency, perceived constraints, social norms and responsibility. The 7 C model of vaccine acceptance, validated among European parents and adolescents, synthesises these determinants into measurable behavioural domains [14]. Constructs assessed in this study, including HPV awareness, perceived disease severity, and trust in healthcare providers, align with components of this framework. Furthermore, vaccine acceptance is increasingly understood as a continuum rather than a binary decision, ranging from full acceptance to uncertainty, delay, or refusal [15]. The operationalisation used in this study therefore reflects only the most decisive end of this spectrum and may underestimate more ambivalent forms of hesitancy.
Gender disparities in awareness and willingness
Mothers consistently demonstrated higher awareness of HPV and the HPV vaccine, were more likely to actively seek information, and expressed greater willingness to vaccinate compared to fathers. These differences reflect patterns observed in other high-income countries, where maternal involvement in healthcare and higher health literacy among women contribute to stronger engagement with preventive measures [10–13, 16].
By contrast, fathers were both less aware and less willing to vaccinate, despite similar access to information channels. These findings underline the need for targeted communication strategies that specifically address fathers, who remain an under-engaged group in HPV vaccination campaigns. Comparable gendered patterns have been reported internationally: studies in the UK and US found that mothers were more knowledgeable and proactive in HPV vaccination decisions, while fathers were less engaged, particularly for daughters [5, 12]. In contrast, countries with school-based, gender-neutral vaccination programmes, such as Australia and Scotland, report smaller gender gaps, suggesting that structural approaches can mitigate parental role differences [19, 20].
While willingness to vaccinate did not differ between parents of daughters and sons, parents of daughters reported significantly greater fear of HPV-associated disease. This persistent perception of HPV as a “female-focused” infection remains a barrier to engaging parents of boys. Public health efforts should more clearly communicate that HPV vaccination also protects males against anogenital and oropharyngeal cancers and reduces viral transmission, thus contributing to herd immunity [21].
Dyadic interactions and parental hesitancy
The parent–child dyad analysis revealed more nuanced gender dynamics. Mother–daughter dyads showed the highest awareness and willingness to vaccinate, while father–son dyads demonstrated the lowest awareness. Strikingly, father–daughter dyads combined high levels of fear of HPV-associated disease with comparatively lower willingness to vaccinate. This pattern may reflect cultural discomfort in discussing sexuality and preventive measures across the father–daughter relationship.
Such findings highlight the importance of tailoring interventions to both parental and child gender roles. Fathers, in particular, should be directly addressed in awareness campaigns, both to strengthen their knowledge and to normalize proactive involvement in vaccination decisions for sons and daughters alike [12, 13].
Determinants of willingness to vaccinate
Multivariable analysis identified three determinants of willingness to vaccinate: prior awareness of HPV, fear of HPV-associated disease, and higher educational attainment. Demographic characteristics such as parent or child gender were not significant once awareness and fear were accounted for. This suggests that emotional and cognitive factors—knowledge of HPV and perceived disease threat—outweigh structural variables in shaping vaccination intentions. These findings are consistent with international studies demonstrating that prior awareness of HPV, perceived disease threat, and higher education levels are robust predictors of parental willingness across settings [5, 6]. Importantly, provider recommendation has emerged as a particularly influential factor in multiple countries [20, 22], underscoring the global relevance of strengthening physician-parent communication.
These results align with previous studies demonstrating that awareness and perceived susceptibility are strong behavioral drivers of vaccine acceptance [10]. The acceptable discriminatory ability of the model further supports the robustness of these determinants.
Vaccine hesitancy and conditional acceptance
Among parents refusing vaccination, most reported that none of the listed conditions would influence their decision. This suggests a subgroup with strong pre-existing attitudes, distinct from undecided parents described in international literature as ‘fence-sitters,’ who typically respond to paediatric recommendations, social endorsement, or structural facilitation (Table 5). Conditional acceptance was limited and most commonly associated with pediatrician recommendation (12.7%) or social endorsement by family and peers (12.7%), followed by inclusion in the national immunization schedule (10.9%) and cost removal (9.1%). Other factors, such as school recommendation (7.3%) or assurances of safety (7.3%), were rarely cited (Table 5). International comparisons suggest that our proportion of firmly resistant parents may be higher than in other countries, where conditional acceptance is more common. For instance, systematic reviews show that pediatrician or school recommendations often sway undecided parents [5, 23]. In contrast, the limited responsiveness observed in our study points toward a subgroup with entrenched views, requiring tailored strategies beyond standard information campaigns.
Compared with studies in other European and US contexts, where provider recommendation and school mandates have shown stronger influence [16, 21, 24], the low conditional acceptance observed here suggests deeper ideological or informational resistance. This aligns with systematic reviews reporting that provider trust and social norms are among the most important modifiable factors influencing parental vaccine hesitancy. Importantly, these findings highlight the need to distinguish between “fence-sitters,” who may be influenced by physician advice or peer endorsement [21], and a smaller group of firmly resistant parents, for whom traditional informational campaigns are unlikely to be effective. For these parents, resources should instead focus on strengthening provider–parent communication and targeted interventions that leverage trusted relationships. The dyadic analysis highlights unique gender effects that extend beyond the sex of the parent alone. Parent–child relational patterns appear relevant for understanding how vaccination decisions are negotiated within families. To our knowledge, this perspective is novel in the German context and can guide the design of gender-sensitive communication strategies. Placing our findings in an international context emphasizes both commonalities and unique contributions. Similar drivers of HPV vaccination uptake—knowledge, fear of disease, and healthcare provider influence—have been reported worldwide. However, our dyadic analysis adds a novel perspective by explicitly examining parent–child gender interactions, an area rarely addressed in global literature. This approach complements existing international evidence and highlights the need for gender-sensitive interventions that are adaptable to local cultural and structural conditions [5, 18, 19].
Strengths and limitations
This study has several strengths, including a relatively large sample size, detailed analysis of parent–child dyads, and the use of multivariable modeling to identify determinants of willingness to vaccinate. To our knowledge, this is the first study in Germany to explore dyadic interactions between parent and child gender in relation to HPV vaccination attitudes.
Nevertheless, important limitations must be acknowledged. Only 4 of the 12 contacted schools participated, which may have introduced selection bias and limits the representativeness of the sample. The sample overrepresented mothers and individuals with higher education, which likely leads to an overestimation of awareness and willingness compared to the general parent population, and therefore our results may represent an optimistic scenario rather than the true situation in Saxony-Anhalt. All data were self-reported and vaccination status was not independently verified, which may have introduced reporting bias. Furthermore, the cross-sectional design precludes conclusions about causality, and results may not be generalizable beyond the Magdeburg region.
Despite these limitations, the study highlights critical gendered dynamics in HPV vaccination acceptance and identifies modifiable determinants that can inform more targeted interventions.
Conclusion and implications
Efforts to improve HPV vaccination uptake in Saxony-Anhalt should aim to engage all parent groups, including fathers, who in this study demonstrated lower awareness and willingness compared to mothers. Communication strategies that explicitly address the relevance of vaccination for boys and correct gendered misconceptions may be particularly valuable. Strengthening paediatric counselling and providing clear, accessible information targeting both cognitive (knowledge) and emotional (perceived severity) drivers may help translate awareness into acceptance.
A substantial proportion of refusing parents reported that no listed condition would change their decision, suggesting a subgroup with firm prior attitudes distinct from undecided or ambivalent individuals described in vaccine behaviour frameworks. Addressing this subgroup may require tailored approaches beyond standard information campaigns, including trust-building interventions and consistent long-term communication.
These findings may inform local and national HPV vaccination strategies and support Germany’s progress within the WHO Cervical Cancer Elimination Initiative, while contributing to the broader evidence base on gendered patterns in vaccine behaviour.
Future research should explore whether these gendered patterns persist across regions and whether school-based or system-level delivery models could reduce parental variation in HPV vaccine acceptance.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heyde S. Global parental acceptance, attitudes, and knowledge related to HPV vaccinations for their children: A systematic review and meta-analysis. BMC Women’s Health; 2024.10.1186/s 12905-024-03377-5PMC 1142890939334328 · doi ↗ · pubmed ↗
- 2Achimaș-Cadariu T. Vaccine Hesitancy among European Parents: Socio-demographic and Psychological Factors. Vaccines. 2024.10.3390/vaccines 12020127 PMC 1089184038400111 · doi ↗ · pubmed ↗
- 3Tobaiqy M, Mac Lure K. A systematic review of human papillomavirus vaccination challenges and strategies to enhance uptake. Vaccines. 2024;12(7):746. 10.3390/vaccines 12070746 PMC 1128145639066384 · doi ↗ · pubmed ↗
- 4Mavundza EJ. Factors associated with HPV vaccine acceptance and uptake among adolescents and young adults globally. Front Public Health. 2024;14(11):e 082592. 10.1136/bmjopen-2023-082592 PMC 1157525339542479 · doi ↗ · pubmed ↗
- 5Ntonifor MMN. Factors associated with parental hesitancy towards the human papillomavirus vaccine: a cross-sectional study in Cameroon. Sci Rep. 2025;15(1):18284. 10.1038/s 41598-025-94067-1PMC 1210438440415103 · doi ↗ · pubmed ↗
- 6Brunton CGA, Cross-Cultural. Qualitative analysis in Scotland. Spain… Int J Behav Med. 2025. 10.1007/s 12529-025-10387-6.10.1007/s 12529-025-10387-640775576 · doi ↗ · pubmed ↗
- 7Shapiro GK. The impact of publicly funded immunization programs on HPV vaccine uptake in boys when school-based or government-funded programs are introduced. Lancet Regional Health – Americas; 2022.10.1016/j.lana.2021.100128 PMC 990407536778727 · doi ↗ · pubmed ↗
- 8Chan DNS. Factors affecting HPV vaccine uptake among ethnic minority adolescent girls: a systematic review. Cancer Epidemiol. 2023;10(9):100279. 10.1016/j.apjon.2023.100279 PMC 1047193637661962 · doi ↗ · pubmed ↗