Isolated Gallbladder Tuberculosis Mimicking Chronic Cholecystitis: A Case Report
Ananya Vig, Dikshit Chawla, Parth Dhamija, Ashwani Kumar, Mansi Singh

TL;DR
A rare case of gallbladder tuberculosis was diagnosed after imaging suggested chronic cholecystitis, highlighting the need for histopathological evaluation.
Contribution
This case report emphasizes the importance of histopathological analysis in diagnosing isolated gallbladder tuberculosis.
Findings
GBTB is rare and often misdiagnosed due to nonspecific symptoms and imaging findings.
Histopathological evaluation is crucial for confirming GBTB, as seen in this case.
GBTB should be considered in patients with a history of tuberculosis and atypical gallbladder findings.
Abstract
Isolated gallbladder tuberculosis (GBTB) is a rare disease, even in endemic areas, and is often misdiagnosed due to its nonspecific clinical and imaging findings. Histopathological evaluation, demonstrating granulomatous inflammation with caseous necrosis, remains the only definitive method of diagnosis. Thus, maintaining a high index of suspicion and routine histological assessment of resected specimens are vital for its timely management, especially in patients with a history of tuberculosis. We report a similar case in a 50‐year‐old male patient with imaging suggestive of gallbladder perforation and chronic cholecystitis, which later revealed a cryptic GBTB dug up during histopathological examination.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure FIGURE 1
Figure FIGURE 1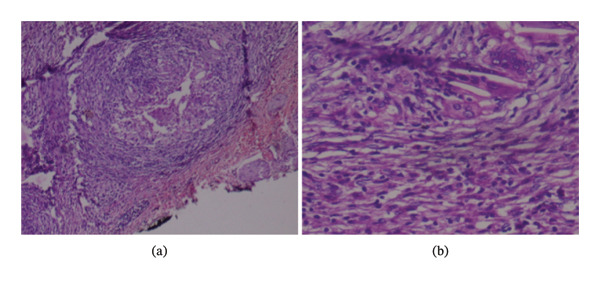 Figure FIGURE 2
Figure FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and treatment of tuberculosis · Infectious Diseases and Tuberculosis · Gallbladder and Bile Duct Disorders
1. Introduction
Gallbladder tuberculosis (GBTB) is a rare infectious disease, constituting only 1% of abdominal tuberculosis cases [1]. It is uncommon even in areas of endemicity due to the gallbladder’s high resistance to tubercular infections [2]. With less than 180 cases of GBTB reported in the literature, its diagnosis remains challenging even for experienced clinicians [3]. The nonspecific pathognomonic presentation and lack of preoperative diagnostic tests often lead to misdiagnosis as chronic cholecystitis or gallbladder malignancy [4–6].
We report the case of a 50‐year‐old patient who presented in the OPD with a chief complaint of pain in the right upper abdomen, initially diagnosed with chronic cholecystitis, for which he underwent laparoscopic cholecystectomy under general anesthesia. However, he was later diagnosed with GBTB on histopathological examination. This manuscript aims to increase awareness and suspicion in identifying the rare cases of GBTB, which will be essential in eradicating tuberculosis from society.
2. Case Presentation
A 50‐year‐old male presented to the outpatient department with chief complaints of recurrent pain in the right upper abdomen for the past 4 months, along with dyspepsia, weight loss, and loss of appetite. No history of fever, night sweats, nausea, vomiting, jaundice, or cough with expectoration was reported. The patient had been diagnosed with gallbladder perforation 3 months before admission based on ultrasound and contrast‐enhanced computed tomography (CECT) whole abdomen findings, managed conservatively with antibiotics and analgesics, and advised to undergo cholecystectomy within the next 2 months. However, he deferred surgery and returned with a recurrence of more severe symptoms and additional complaints. He had a history of pulmonary tuberculosis 30 years back, for which he took anti‐tubercular therapy (ATT) for 6 months as per the National Tuberculosis Elimination Programme (NTEP).
The general physical and abdominal examinations were unremarkable. Routine laboratory investigations showed slightly elevated serum bilirubin (2.4 mg%) and serum glutamic‐oxaloacetic transaminase (SGOT) (54 U/L) levels. Ultrasound of the abdomen (Figure 1) revealed a thickened, edematous gallbladder (7.5 mm) with a narrow lumen and a few hypodense, echogenic masses with positive DAS suggestive of cholelithiasis. Magnetic resonance cholangiopancreatography (MRCP) images showed a contracted gallbladder with few intraluminal voids in the neck (largest measuring 17 mm), diffuse wall thickening (up to 10 mm), and a streak of fluid in the pericholecystic region, causing adhesions to the liver, duodenum, and hepatic flexure. A diagnosis of chronic cholecystitis with concealed gallbladder perforation was considered, and the patient was scheduled for laparoscopic cholecystectomy.
Ultrasound showing diffuse gallbladder wall thickening with stones.
Intraoperatively, a thickened, adherent, and distended gallbladder was visualized and resected from the liver bed. The cut section of the specimen showed an obliterated lumen and numerous chalky white areas extending into the peritoneal layer. Histopathological examination (Figure 2) revealed chronic granulomatous inflammation with caseous necrosis, multinucleated giant cells, and Langhans giant cells, confirming GBTB. The patient’s postoperative recovery was uneventful. The patient was prescribed ATT as per the guidelines of the NTEP of India with isoniazid (I), rifampicin (R), ethambutol (E), and pyrazinamide (P) for 6 months and was scheduled for a follow‐up after completing the full course. The patient was followed for 6 months postoperatively and was further lost to follow‐up for long‐term outcomes.
Histopathology of the resected gallbladder specimen: low‐power view of gallbladder showing necrotizing granulomas (a) composed of epithelioid cells and Langhans type multinucleated giant cells (b).
3. Discussion
GBTB remains one of the rarest manifestations of extrapulmonary tuberculosis, accounting for approximately 1% of abdominal TB cases [2, 7]. The gallbladder’s inherent resistance, attributable to the bactericidal properties of bile, renders it an uncommon site for Mycobacterium tuberculosis infection. This natural defense leads to a low index of preoperative clinical suspicion, frequently leading clinicians to overlook tuberculosis as a potential etiology in gallbladder pathology.
In the present case, the clinical and radiological features closely mimicked more common conditions such as chronic cholecystitis and gallbladder perforation [6, 8]. The imaging studies revealed findings that were not pathognomonic and could easily be confused with cholelithiasis or even gallbladder malignancy. Such overlap in presentation complicates the differential diagnosis, particularly in regions where gallbladder carcinoma and benign inflammatory conditions are more routinely encountered.
A notable aspect of our patient’s history is a remote episode of pulmonary tuberculosis, which should prompt a heightened clinical suspicion for extrapulmonary reactivation, even decades after the initial infection [2, 7]. Although antecedent TB may seem clinically insignificant over time, it serves as a crucial diagnostic clue in cases with atypical presentations. This underlines the imperative that every cholecystectomy specimen be rigorously examined histopathologically to detect granulomatous inflammation and caseous necrosis, the hallmarks of tubercular infection.
4. Limitations
This case report describes a single patient with GBTB, and therefore the findings cannot be generalized to all patients with gallbladder disease or extrapulmonary TB. The disease was not considered preoperatively in the differential diagnosis because the patient did not present with signs or symptoms of pulmonary or extrapulmonary TB (no H/o cough, fever, night sweats, and no palpable lymph nodes); consequently no preoperative TB‐specific diagnostic tests were undertaken before scheduling cholecystectomy. As the patient was lost to follow‐up, contact tracing, screening of contacts, and further evaluation could not be done.
5. Conclusion
This case report contributes significantly to the current literature by highlighting the diagnostic challenges associated with GBTB and reinforcing the importance of incorporating a thorough patient history and mandatory histopathological evaluation in managing gallbladder diseases. By advocating for a meticulous approach in patients with previous TB exposure and ambiguous clinical presentations, our findings aim to improve diagnostic accuracy, incorporate stringent protocols for such cases, and optimize patient outcomes in regions where tuberculosis remains endemic [6, 8, 9].
Funding
This research received no specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Swain B. , Otta S. , and Mohapatra S. S. G. , Tuberculous Cholecystitis, Indian Journal of Medical Microbiology. (2013) 31, no. 3, 10.4103/0255-0857.115672, 2-s 2.0-84883150645.23883730 · doi ↗ · pubmed ↗
- 2Dhali A. , Maity R. , Biswas J. , Mukherjee S. , and Dhali G. K. , Gallbladder Tuberculosis Mimicking Carcinoma: A Case Report of a Rare Entity, International Journal of Surgery Case Reports. (2024) 123, 10.1016/j.ijscr.2024.110228.PMC 1178038439226636 · doi ↗ · pubmed ↗
- 3Sagar M. , Rawat S. , Verma A. , Singh A. , and Singh U. S. , Gallbladder Tuberculosis: A Rare Case Report With Review of Literature, Indian Journal of Case Reports. (2022) 8, no. 10, 311–313, 10.32677/ijcr.v 8i 10.3607. · doi ↗
- 4Wolde T. G. , Jiang K. , Miao Y. , and Wei J. , Gallbladder Tuberculosis in a Dialysis Patient: A Case-Report, BMC Surgery. (2020) 20, 1–4, 10.1186/s 12893-020-00722-x.32264878 PMC 7137183 · doi ↗ · pubmed ↗
- 5Soni S. , Sreesanth K. S. , Varshney V. , and Swami A. , Gall Bladder Tuberculosis: Review of Literature, Indian Journal of Tuberculosis. (2022) 69, no. 4, 421–426, 10.1016/j.ijtb.2021.08.028.36460370 · doi ↗ · pubmed ↗
- 6Varshney B. , Elhence P. , Soni S. , Varshney V. K. , Yadav T. , and Saha S. , Gallbladder Tuberculosis Presenting as Obstructive Jaundice, ACG Case Reports Journal. (2020) 7, no. 6, 10.14309/crj.0000000000000414.PMC 753577933062787 · doi ↗ · pubmed ↗
- 7Verma S. K. , Mishra A. K. , and Jaiswal A. K. , Tuberculosis of Gallbladder Neck: A Cause of Cholecystitis With Cholelithiasis, Case Reports. (2013) 2013, 10.1136/bcr-2012-008007, 2-s 2.0-84875933968.PMC 360420023413288 · doi ↗ · pubmed ↗
- 8Chan K. S. , Shelat V. G. , Tan C. H. , Tang Y. L. , and Junnarkar S. P. , Isolated Gallbladder Tuberculosis Mimicking Acute Cholecystitis: A Case Report, World Journal of Gastrointestinal Surgery. (2020) 12, no. 3, 123–128, 10.4240/wjgs.v 12.i 3.123.32218895 PMC 7061240 · doi ↗ · pubmed ↗