Exploring the Benefits of Cranberries in Dentistry: A Comprehensive Review
Isabella Schönhofen Manso, Yasmim Guterres Bauer, Eduarda Blasi Magini, Gabriel Leonardo Magrin, Izabella Thais da Silva, Ariadne Cristiane Cabral Cruz

TL;DR
This review explores how cranberries and their compounds may help prevent and treat various oral diseases through antimicrobial, anti-inflammatory, and antioxidant effects.
Contribution
The study consolidates current scientific evidence on cranberry applications in dentistry, highlighting their potential for clinical use.
Findings
Cranberry compounds show antimicrobial activity against caries-related bacteria in preclinical studies.
Cranberry extracts reduce inflammation in periodontal diseases and inhibit dentin erosion.
Cranberry bioactives neutralize reactive oxygen species after dental bleaching and support osteogenic processes.
Abstract
Objectives: Despite the increasing scientific evidence regarding the application of Cranberries in dentistry, a comprehensive understanding of their potential benefits, active constituents, and mechanisms of action remains lacking. Consequently, this narrative review aims to meticulously analyze and consolidate the existing scientific literature on the utilization of Cranberries for the prevention and treatment of oral diseases. Materials and Methods: Electronic databases (PubMed, Scopus, and Web of Science) were searched up to October 2025. This review included in vitro, in vivo, and clinical research studies. A two-phase selection process was carried out. In phase 1, two reviewers independently screened titles and abstracts to identify potentially eligible studies. In phase 2, the same reviewers performed the full-text assessments of the eligible articles. Results: Among the 93…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
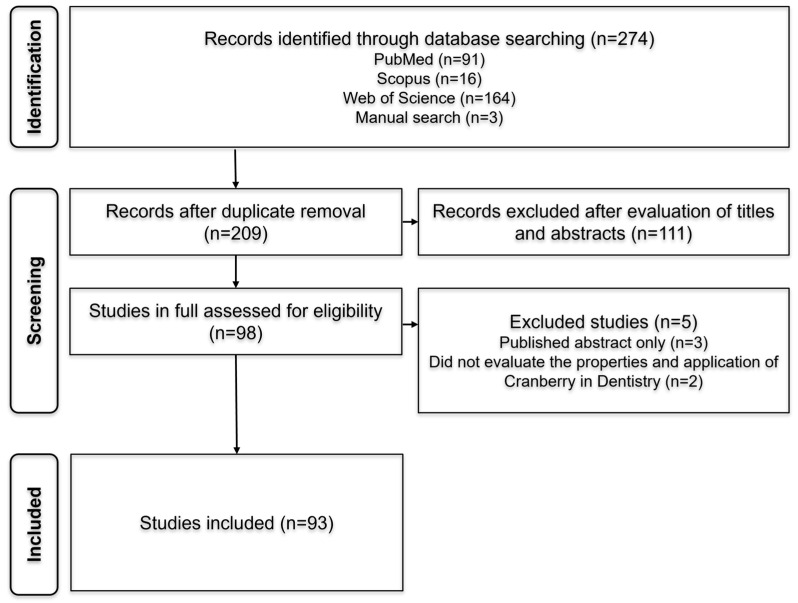 Figure 1
Figure 1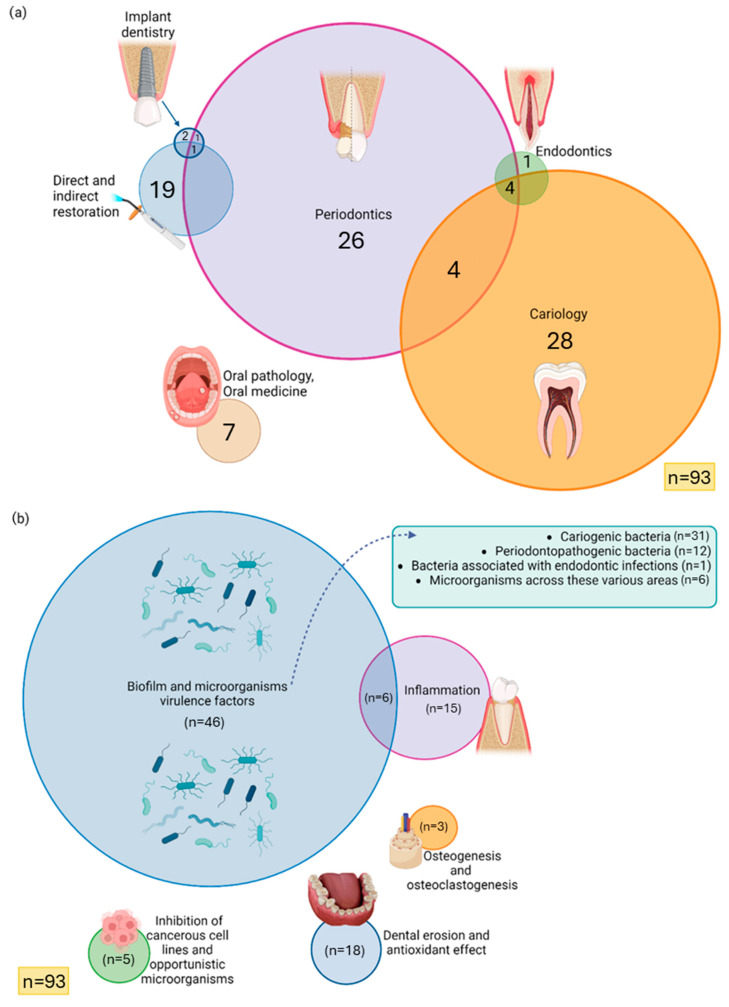 Figure 2
Figure 2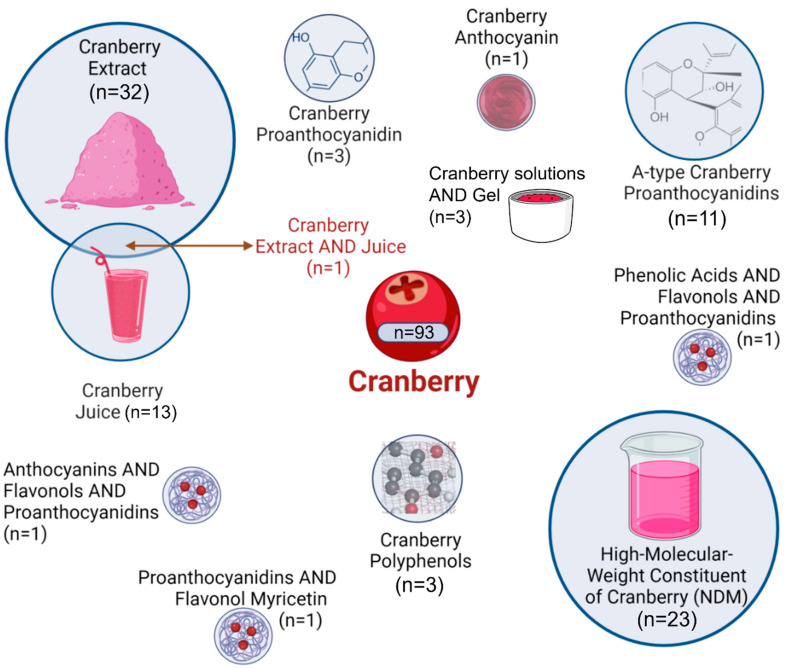 Figure 3
Figure 3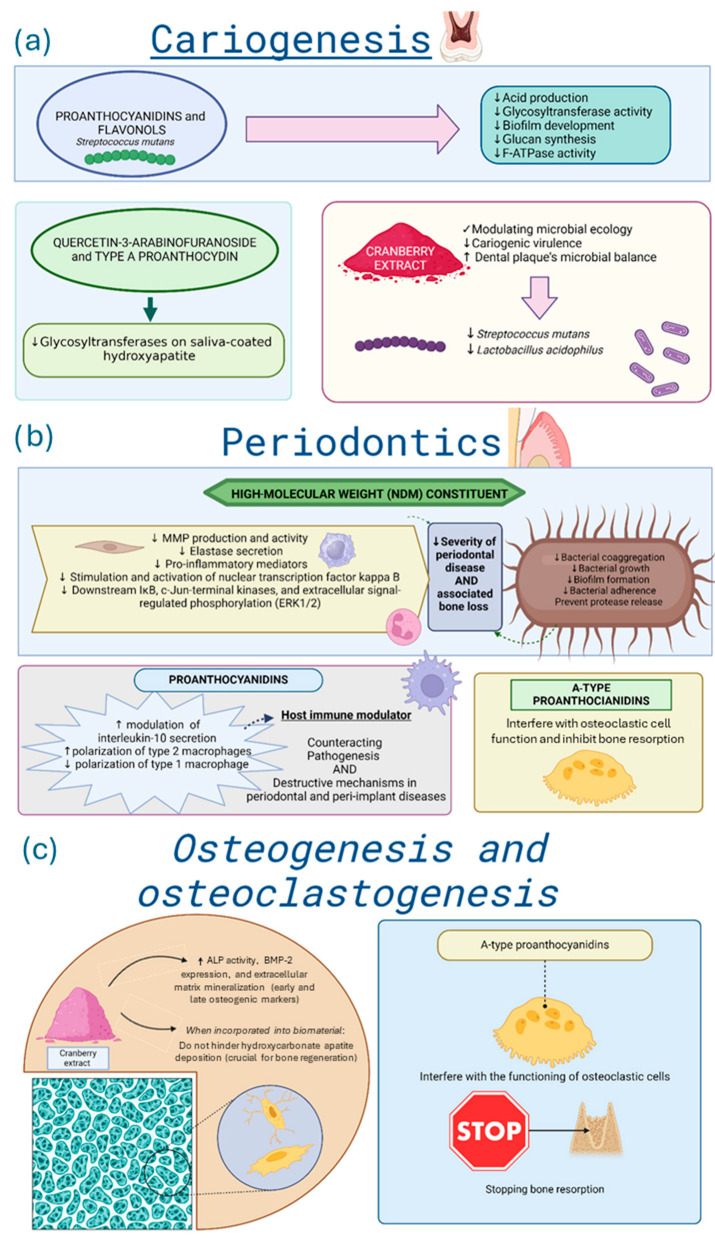 Figure 4
Figure 4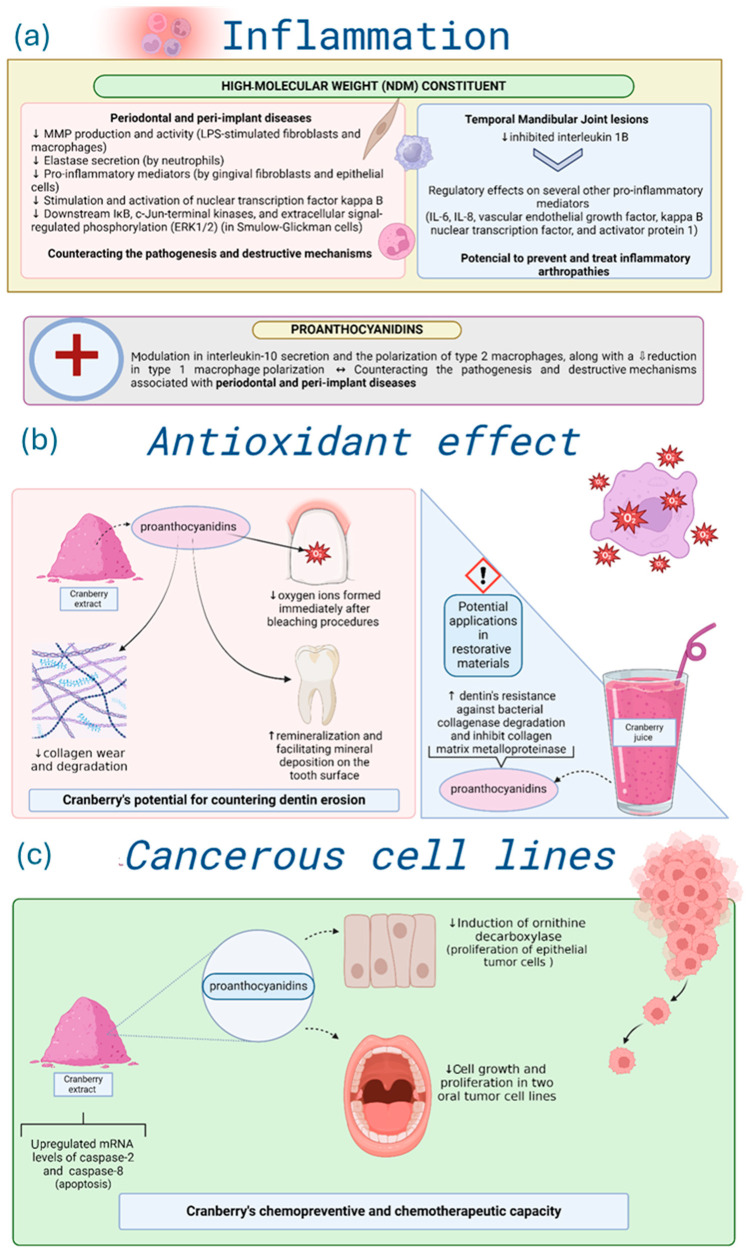 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Phytochemicals and Antioxidant Activities · Dental Erosion and Treatment
1. Introduction
Cranberries have garnered widespread recognition for their considerable potential in promoting human health [1,2,3,4]. Vaccinium macrocarpon, Vaccinium oxycoccus, and Vaccinium microcarpum are species of Cranberry, with Vaccinium macrocarpon being the most extensively studied due to its distinctive phytochemical profile and bioactivity [5,6,7]. Historically, Cranberries have been used since the 17th century as a medical fruit to manage blood disorders, lipid and glucose metabolism, hepatic steatosis, and even cancer [8,9,10,11,12,13,14]. More recently, Cranberries have become best known for their efficacy in preventing urinary tract infections, which has been largely attributed to the presence of A-type proanthocyanidins capable of inhibiting bacterial adhesion to epithelial cells [2,14]. The broad spectrum of biological activities observed in Cranberry arises from its complex polyphenol composition, which includes compounds with anti-bacterial, anti-adhesive, anti-inflammatory, antioxidant, and anti-tumorigenic effects [1,15,16].
Cranberry phenolics primarily consist of flavonoids, phenolic acids, and tannins [17]. Among these, flavonoids are the predominant and encompass over 150 identified molecules, grouped into anthocyanins, flavonols, and proanthocyanidins [18]. On overage, Cranberry contains 13 anthocyanins, 16 flavonols, and 26 phenolic acids and benzoates [15]. In various cultivars, 48 polyphenols have been identified, including 19 flavonols, 8 anthocyanins, 7 phenolic acids, and 14 flavan-3-ol oligomers, with relative abundance as follows: flavan-3-ols (41.5–52.2%), flavonols (18.6–30.5%), anthocyanins (8.0–24.4%), and phenolic acids (5.0–12.1%) [19,20].
Regarding oral health, there has been increasing interest in exploring natural bioactive compounds as alternatives or adjuncts to conventional antimicrobials, particularly due to the rise in antibiotic resistance. Cranberry extracts have demonstrated promising effects in this context, encompassing the modulation of host inflammatory response to periodontopathogens, inhibition of biofilm formation and acid production by cariogenic bacteria, suppression of bacterial proteolytic enzymes, and reduction in oxidase stress [21]. These mechanisms are relevant to the control of major oral infectious diseases such as dental caries, periodontal and peri-implant diseases, endodontic infections, and candidiasis [8]. Moreover, recent studies have extended the potential application of Cranberry-derived compounds beyond infection control. Evidence suggests its use in promoting soft and hard tissue healing, reducing inflammation in temporomandibular joint disorders, and even enhancing dentin bond strength following bleaching by neutralizing reactive oxygen species. Such multifunctional properties make Cranberry a promising candidate for integration into preventive, therapeutic, and regenerative dental formulations, including mouth rinses, varnishes, biomaterials, and scaffolds.
Despite this expanding body of research, findings remain fragmented, and the mechanisms underlying Cranberries’ protective effects in the oral cavity are not yet fully elucidated. Therefore, this narrative review aims to systematically analyze and consolidate the available scientific evidence on the utilization of ranberries in the prevention and treatment of oral diseases, highlighting their bioactive constituents, mechanisms of action, and translational potential within dentistry.
2. Methods
2.1. Search Strategy
A comprehensive literature search was performed in the electronic databases PubMed, Scopus, and Web of Science up to October 2025. The search strategy was based on the MeSH terms and their combinations: “Cranberry” AND “dentistry”. Given the narrative nature of this review, the search strategy was intentionally centered on studies linking Cranberry-derived compounds to dental research, ensuring relevance while avoiding excessively broad searches for a narrative review. Studies were considered eligible if Cranberry and its derived fractions were applied within the context of dentistry, defined as any application involving oral tissues, oral microorganisms, dental materials, oral diseases, or procedures relevant to clinical practice. Eligible study designs included in vitro, in vivo, and clinical research studies, as long as they reported outcomes directly linked to oral biology or dental interventions. These heterogeneous study designs were included to synthesize evidence, providing a broad overview of the topic and highlighting existing knowledge gaps. Studies were excluded if they were review articles, conference abstracts, book chapters, or if they did not present primary data related to dentistry. Only articles published in English were included, with no restriction regarding the publication date.
2.2. Study Selection Process
The selection process was performed in two phases using Rayyan software (Qatar Computing Research Institute, Qatar). In phase 1, two independent reviewers (Y.G.B. and E.B.M.) screened titles and abstracts to identify potentially eligible studies. In phase 2, the same reviewers performed a full-text assessment of selected articles. Any discrepancies between reviewers were resolved through discussion and consensus. These simplified and structured descriptions of the search and selection process were adopted to enhance transparency and to organize the literature within the context of a narrative review.
2.3. Data Extraction
From the included studies, the following data were extracted: Author information, publication year, study design, dentistry field, Cranberry properties, study objective, applied tests, and main outcomes.
3. Results
3.1. Study Selection Outcomes
In phase 1, a total of 274 references were retrieved from the databases: PubMed (91), Scopus (16), and Web of Science (164). Three additional references were identified manually (3). After removing duplicates, 209 articles remained. Following title and abstract screening, 111 studies were excluded based on inter-reviewer agreement, leaving 98 articles for full-text analysis in phase 2. After full-text reading, 5 references were excluded for not meeting the inclusion criteria, resulting in a total of 93 articles eligible for further analysis. A detailed flowchart depicting the identification, inclusion, and exclusion process is presented in Figure 1.
3.2. Study Characteristics
The included studies were published from 1998 to 2025. Additionally, as despicable in Figure 2a, the distribution of research fields was as follows: Cariology (n = 28); Periodontics (n = 26); Direct and indirect restoration (n = 19); Oral pathology and Oral medicine (n = 7); Cariology, Periodontics, and Endodontics (n = 4); Periodontics and Cariology (n = 4); Implant dentistry (n = 2); Endodontics (n = 1); Periodontics and Implant dentistry (n = 1); and Periodontics, Implant dentistry, Direct and indirect restoration (n = 1). Most studies evaluated biofilm formation and microbial virulence factors (n = 46), followed by inflammation (n = 15), and inflammation associated with biofilm formation (n = 6), and dental erosion and antioxidant effect (n = 18). Additional topics included cytotoxicity of cancerous cell lines and antifungal effects (n = 5), osteogenesis and osteoclastogenesis (n = 3) (Figure 2b).
As represented in Figure 3, the most frequently studied Cranberry fractions were Cranberry extract (n = 32) and high-molecular-weight non-dialyzable material (NDM) (n = 23). Other forms included Cranberry juice (n = 13), A-type proanthocyanidins (n = 11), proanthocyanidin fraction (n = 3), polyphenol (n = 3), unspecified Cranberry gels or solutions (n = 3), anthocyanin (n = 1), and several combined formulations. Most investigations were in vitro (n = 82), followed by clinical trials (n = 13) and in vivo studies (n = 2), with some employing hybrid experimental designs. The main characteristics of the selected studies are summarized in Table 1, Table 2 and Table 3.
3.3. Biofilm and Microbial Virulence Factors
Among the 93 studies included, nearly half (n = 46) addressed biofilm formation and microbial virulence. Some of these examined periodontopathogenic bacteria (n = 12) [15,20,23,24,29,30,36,40,43,58,72,77], cariogenic bacteria (n = 31) [22,25,26,27,31,32,39,47,48,57,60,61,62,64,65,70,71,76,92,93,94,95,98], bacteria associated with endodontic infections (n = 1) [67], and a wide range of microorganisms across these various areas (n = 6) [21,39,42,52,66]. Some studies focused on assessing the Cranberry anti-inflammatory properties (n = 6) [40,43,72,76].
In cariology, Cranberry-derived proanthocyanidins and flavonols exhibited strong in vitro inhibitory effects on Streptococcus mutans virulence, including reduced acid production, glycosyltransferase activity, and biofilm development on tooth surfaces [4,22,32,48], as observed in Figure 4a. These beneficial effects seem to be related to inhibition of glucan synthesis, F-ATPase activity, and acid production [4,26,32,48,105]. Specific fractions from Cranberry extracts, such as quercetin-3-arabinofuranoside and A-type proanthocyanidin, exhibited potent in vitro inhibition of glycosyltransferases on saliva-coated hydroxyapatite [52,93,106]. These bioactive fractions also interfered with bacterial adhesion and reduced the acidogenic potential of dental biofilms in controlled environments [3,48,61].
Cranberry extracts inhibited Lactobacillus acidophilus, indicating broader modulation of the oral microbiota in vitro [64]. Clinically, Cranberry-based mouthwashes decreased Streptococcus mutans and total bacteria counts in saliva, showing comparable efficacy to 0.2% chlorhexidine [95]. Pediatric formulations achieved similar benefits without adverse effects in clinical [94] and laboratory conditions [70]. When incorporated into dentifrices, Cranberry extracts clinically modulated plaque ecology and reduced cariogenic virulence [98]. Overall, these findings support Cranberries as a natural, non-toxic, and effective adjunct for preventing dental caries.
In periodontitis, as described in Figure 4b, high-molecular-weight Cranberry fractions (NDM) inhibited in vitro bacterial coaggregation and adhesion, protease release by major periodontal pathogens [23,28,29]. Clinically, Cranberry mouthwash reduced plaque and gingival indices comparably to chlorhexidine [95,107]. In vitro, A-type proanthocyanidins also disrupted Candida albicans biofilms [43], likely mediated by Cranberries’ capacity to inhibit the activation of nuclear factor B p65, which influences the virulence of Candida albicans and attenuates inflammation. Cranberry proanthocyanidins and flavonoids incorporated into self-curing polymethylmethacrylate resin used in prostheses reduced the number of colony-forming units of Candida albicans in a laboratory environment [5,91].
3.4. Osteogenesis and Osteoclastogenesis
Only three studies addressed bone-related mechanisms in vitro [16,54,83]. One reported that incorporating Cranberry extract into mesoporous bioactive glass preserved hydroxycarbonate apatite deposition, maintaining material bioactivity [16]. The second demonstrated that A-type proanthocyanidins inhibited osteoclastic activity, suggesting a potential role in preventing bone resorption associated with periodontitis [54]. Also, the Cranberry extract increased early and late osteogenic markers, such as alkaline phosphatase and extracellular matrix mineralization in vitro [83]. For more details, see Figure 4c.
3.5. Inflammation
Several articles (n = 21) investigated the Cranberries’ anti-inflammatory effects [28,40,43,72,76,99]. Six overlapped with biofilm-focused research [40,43,72,76,100,102].
Clinically, five studies investigated Cranberries in the context of gingival inflammation. Overall, the evidence suggests potential benefits, although with important methodological limitations across studies. A nature-based gel achieved clinical outcomes comparable to conventional dentifrices while indicating a possible host-response–modulating effect [102]. A multinutrient supplement containing Cranberry extract improved periodontal clinical parameters, albeit without statistically significant differences compared with placebo [100]. Other trials reported reductions in plaque accumulation and gingivitis scores in patients undergoing fixed orthodontic treatment [50], and omega-3–enriched Cranberry juice was associated with reduced glycated hemoglobin, increased HDL-C levels, and improved periodontal conditions [49]. Additionally, an eight-week intake of a Cranberry-based functional beverage reduced gingival inflammation, plaque index, and approximal plaque index; however, this comparison was made against a water control, which is not an adequately matched comparator and limits the interpretability of the findings [37].
Laboratory-based studies demonstrated that NDM displayed protective effects on macrophages stimulated by lipopolysaccharides (LPS) from periodontopathogens [28], inhibited matrix metalloproteinase (MMP) production and activity in LPS-stimulated fibroblasts and macrophages [33,34,50], suppressed neutrophil elastase [19], and inhibited the secretion of pro-inflammatory mediators (interleukin-6, interleukin-8, and prostaglandin E2) by gingival fibroblasts [45,46] and epithelial cells [63]. NDM also inhibited the activation of nuclear transcription factor kappa B [51], IκB, and MAPK pathways, including c-Jun-terminal kinases and extracellular signal-regulated phosphorylation kinases 1 and 2 (ERK1/2) in Smulow-Glickman cells [73]. Proanthocyanidins stimulated interleukin-10 secretion, induced M2 macrophage polarization, and suppressed M1 macrophage polarization [53]. Collectively, these laboratory findings suggest that Cranberry compounds can act as a host immune modulator in periodontal and peri-implant inflammation.
In addition, NDM mitigated in vitro temporal mandibular joint inflammation, downregulating interleukin 1β, IL-6, IL-8, vascular endothelial growth factor (VEGF), and transcription factors such as kappa B nuclear transcription factor and activator protein 1. As a result, NDM holds potential therapeutic use in inflammatory arthropathies of the temporomandibular joint [75].
Although two studies reported an increase in IL-6 after the deacidification of Cranberry juice [59,74], which is an effect inconsistent with anti-inflammatory activity, this response seems to reflect alterations in the chemical composition of the juice rather than the inherent properties of Cranberry-derived compounds. Most other studies using native extracts or purified fractions demonstrated reductions in IL-6, IL-8, VEGF, and related mediators, suggesting that these effects may be model- and preparation-dependent. Given that the evidence is predominantly derived from laboratory experiments, these findings should not be extrapolated to clinical contexts, even though they collectively suggest a potential anti-inflammatory influence under specific experimental conditions.
3.6. Dental Erosion and Antioxidant Effect
Cranberry’s role as an antioxidant and in dental erosion prevention was also evaluated (n = 18), with all studies showing in vitro results [7,89,90,96,97,101,103]. As depicted in Figure 5b, Cranberry inhibited dentin erosion [7,56,69] but had limited effects on enamel erosion [22,41]. In vitro findings indicate that Cranberries neutralized residual oxygen radicals following dental bleaching, enhancing adhesive bond strength [55,108]. This is attributed to oligomeric proanthocyanidins, which donate electrons to the bleached surface and promote radical scavenging through epicatechin–gallic acid esterification [55,108]. These proanthocyanidins also supported dentin remineralization and inhibited collagen degradation, thus reducing structural wear [7,25,41]. Nevertheless, the low pH of Cranberry extracts may counteract their protective effects on enamel [22]. Overall, Cranberries’ antioxidant capacity and MMP inhibition make them a promising additive for adhesives and restorative materials [69].
3.7. Inhibition of Cancerous Cell Lines
Cranberry potential in controlling cancerous cell lines was addressed in vitro (n = 5) [6,26,27]. The primary objective, as highlighted in three of the articles, was to assess the chemopreventive and chemotherapeutic potential of Cranberry polyphenols at various stages of oral carcinogenesis. Notably, it was reported that proanthocyanidins effectively inhibit the induction of ornithine decarboxylase, an enzyme involved in the proliferation of epithelial tumor cells [28]. In vitro evidence suggests that administering proanthocyanidins derived from Cranberry extract significantly reduces cell growth and proliferation in two oral tumor cell lines. Furthermore, within just 24 h, the Cranberry extract upregulated the mRNA levels of caspase-2, an initiator of apoptosis, and caspase-8, an effector. Moreover, the extract demonstrated the ability to decrease cell adhesion in both cell lines. These findings highlight Cranberry extract’s chemopreventive and chemotherapeutic capacity, selectively targeting cancer cells without affecting normal cells and tissues [26]. Another in vitro study reinforces these findings by demonstrating the effect of Cranberry extract in reducing tumor cell viability and proliferation while maintaining the viability of normal cells [6]. For more details, see Figure 5c.
4. Overview on the Use of Cranberries in Dentistry
Collectively, the reviewed evidence demonstrates that Cranberry possesses multifaceted therapeutic properties, including antimicrobial, anti-inflammatory, and antioxidant properties. Among various Cranberry fraction types, the Cranberry extract (n = 32) and high-molecular-weight non-dialyzable material (NDM) were the most studied (n = 23). These components were found to exert significant effects, particularly on oral pathogens such as Streptococcus mutans and periodontopathogenic bacteria. Other fractions, including proanthocyanidins and flavonols, have also shown promise in inhibiting biofilm formation and bacterial coaggregation, crucial factors in dental caries and periodontitis development.
Additionally, proanthocyanidins and flavonols demonstrated specific efficacy against Streptococcus mutans, a key player in dental caries, by inhibiting acid production and biofilm development on tooth surfaces. Cranberry fractions presented inhibitory effects on glycosyltransferase activity, essential for glucan synthesis, and on F-ATPase activity, reducing acidogenicity and cariogenic potential. Concerning periodontopathogenic bacteria, the high-molecular-weight constituents of Cranberries effectively inhibited biofilm formation and bacterial adherence related to periodontal disease. Studies revealed that Cranberry extracts reduced plaque index and gingival inflammation in clinical trials, suggesting their potential as a therapeutic agent in periodontal disease management. Cranberry extracts, particularly A-type proanthocyanidins, showed potential in promoting bone regeneration and inhibiting osteoclast activity. These findings suggest applications in treating periodontitis and promoting osseointegration in dental implants. Cranberry extract also demonstrated antifungal properties against Candida albicans, with potential applications in prosthetic dentistry. Incorporating Cranberry-derived proanthocyanidins into acrylic resins used in dental prostheses effectively reduced Candida colonization.
The anti-inflammatory effects of Cranberries were linked to their ability to suppress matrix metalloproteinase activity and inhibit the production of pro-inflammatory mediators. Moreover, its antioxidant properties were beneficial in preventing dentin erosion and enhancing the bond strength of dental materials after bleaching. Studies also revealed that Cranberry polyphenols, particularly proanthocyanidins, exhibited chemopreventive and chemotherapeutic effects by inhibiting tumor cell proliferation and inducing apoptosis in oral cancer cell lines. These properties underscore Cranberry’s potential as a complementary therapeutic agent in oral cancer management.
One limitation of this review is that most studies included are based on in vitro analyses (n = 82), with a limited number of clinical trials available (n = 13, including 2 hybrid studies combining in vitro and clinical designs). While these laboratory studies are valuable for understanding the potential effects of Cranberries in a controlled environment, they do not fully reflect their efficacy in real-world clinical settings. Therefore, further clinical trials are essential to validate these findings and determine the true therapeutic potential of this specific berry in dentistry. Consequently, the results presented in this review should be interpreted with caution, as the predominance of in vitro evidence limits the extent to which clinical applicability can be inferred at this stage.
5. Perspectives on Cranberry Applications in Dentistry
Despite encouraging in vitro results, several formulation challenges must be resolved before Cranberry extracts can be incorporated into dental products. Polyphenols are chemically unstable and highly sensitive to pH, temperature, oxygen, and light, which may reduce their bioactivity in commercial formulations. Compatibility issues with common excipients in dentifrices, gels, and mouthwashes (including surfactants, thickeners, and preservatives) may further affect their stability or performance. Additionally, the natural variability of Cranberry extracts, driven by fruit origin, processing methods, and differing concentrations of active compounds, complicates standardization and reproducibility.
Safety considerations are also critical, as the antimicrobial and antibiofilm activity of Cranberry extracts is dose-dependent, with stronger effects observed at higher concentrations of their active polyphenols. However, long-term safety data for topical oral applications remain scarce, and no reference thresholds have been established for dental formulations. This dose dependence, combined with the substantial variability in extraction and concentration protocols, limits the comparability of published studies and challenges the translation of effective in vitro concentrations into clinically acceptable products.
Given these limitations, future research should prioritize clinical validation of Cranberry-derived mouthwashes, dentifrices, and restorative materials. The incorporation of proanthocyanidins and NDM into oral care formulations could offer a natural, biocompatible alternative to conventional antimicrobials such as chlorhexidine. Moreover, the antioxidant and bond-strength-enhancing effects of Cranberry compounds could be leveraged to develop advanced adhesive and restorative systems with greater longevity. Overall, Cranberries hold great promise for advancing preventive and therapeutic strategies in dentistry, emphasizing a bio-based, non-toxic approach to oral health care.
6. Conclusions
Growing evidence suggests that Cranberry bioactives, particularly flavonols, anthocyanidins, and proanthocyanidins, may exert promising biological effects relevant to dentistry, including antimicrobial, anti-inflammatory, antioxidant, and antiproliferative actions in preclinical models. These activities have been demonstrated predominantly in vitro, with limited findings in animal or clinical research. Therefore, while these compounds show potential as multifunctional agents, their clinical applicability remains uncertain.
Given their versatility, further translational, mechanistic, and product-development research is warranted to determine whether Cranberry-derived agents can be integrated into both clinical practice and daily oral care in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Philip N. Walsh L.J. Cranberry Polyphenols: Natural Weapons against Dental Caries Dent. J.201972010.3390/dj 701002030823634 PMC 6473364 · doi ↗ · pubmed ↗
- 2Guay D.R.P. Cranberry and Urinary Tract Infections Drugs 20096977580710.2165/00003495-200969070-0000219441868 · doi ↗ · pubmed ↗
- 3Philip N. Leishman S. Bandara H. Walsh L. Growth Inhibitory Effects of Antimicrobial Natural Products against Cariogenic and Health-Associated Oral Bacterial Species Oral Health Prev. Dent.2020185375423251542510.3290/j.ohpd.a 44307 PMC 11654489 · doi ↗ · pubmed ↗
- 4Philip N. Leishman S.J. Bandara H. Walsh L.J. Polyphenol-Rich Cranberry Extracts Modulate Virulence of Streptococcus mutans-Candida albicans Biofilms Implicated in the Pathogenesis of Early Childhood Caries Pediatr. Dent.201941566230803479 · pubmed ↗
- 5Anitha K.V. Rajkumar K. Effect Of Vaccinium Macrocarpon On Candida Albicans Adhesion To Denture Base Resin J. Pharm. Negat. Results 20221398999710.47750/pnr.2022.13.s 09.119 · doi ↗
- 6Ankola A. Kumar V. Thakur S. Singhal R. Smitha T. Sankeshwari R. Anticancer and antiproliferative efficacy of a standardized extract of Vaccinium macrocarpon on the highly differentiating oral cancer KB cell line athwart the cytotoxicity evaluation of the same on the normal fibroblast L 929 cell line J. Oral Maxillofac. Pathol.20202425810.4103/jomfp.JOMFP_129_2033456234 PMC 7802834 · doi ↗ · pubmed ↗
- 7Kato M.T. de Cardoso C.A.B. Jordão M.C. de Galvão R.P.O. Iscuissati A.G.S. Kinoshita A.M.O. Buzalaf M.A.R. Effect of the cranberry (Vaccinium macrocarpon) juice on reducing dentin erosion: An in vitro study Braz. Oral Res.202236 e 07610.1590/1807-3107 bor-2022.vol 36.007635946732 · doi ↗ · pubmed ↗
- 8Bodet C. Grenier D. Chandad F. Ofek I. Steinberg D. Weiss E.I. Potential Oral Health Benefits of Cranberry Crit. Rev. Food Sci. Nutr.20084867268010.1080/1040839070163621118663617 · doi ↗ · pubmed ↗