In Vitro Activity of Zoliflodacin Against Neisseria gonorrhoeae Isolates from Shanghai, China (2020–2023)
Linxin Yao, Tingli Tian, Xinying Lu, Danyang Zou, Zhuojun Tang, Xin Feng, Tong Zheng, Zhen Ning, Yi Lin, Meiping Ye, Jianping Jiang, Pingyu Zhou

TL;DR
Zoliflodacin shows strong effectiveness against drug-resistant gonorrhea bacteria in Shanghai, offering a promising new treatment option.
Contribution
Demonstrates zoliflodacin's potent in vitro activity against multidrug-resistant Neisseria gonorrhoeae isolates in Shanghai.
Findings
Zoliflodacin had low MIC values (≤0.004 to 0.25 mg/L) against 876 N. gonorrhoeae isolates.
It remained effective against isolates resistant to ceftriaxone, azithromycin, and other antibiotics.
Genomic analysis found no mutations linked to zoliflodacin resistance in most isolates.
Abstract
Background/Objectives: The escalating threat of drug-resistant Neisseria gonorrhoeae underscores the urgent need for novel therapeutic agents. Zoliflodacin, a first-in-class spiropyrimidinetrione antibiotic that targets bacterial DNA gyrase and topoisomerase IV, represents a promising candidate for gonorrhea treatment. Methods: From 2020 to 2023, a total of 876 urogenital N. gonorrhoeae isolates were collected from 35 hospitals across Shanghai, China. In vitro susceptibilities to zoliflodacin and six conventional antibiotics (penicillin, tetracycline, ciprofloxacin, azithromycin, ceftriaxone, and spectinomycin) were determined using the agar dilution method. Whole-genome sequencing was conducted to identify sequence types (STs) and amino-acid substitutions in GyrA, GyrB, ParC, ParE, and MtrR. Results: Zoliflodacin exhibited potent in vitro activity, with minimum inhibitory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
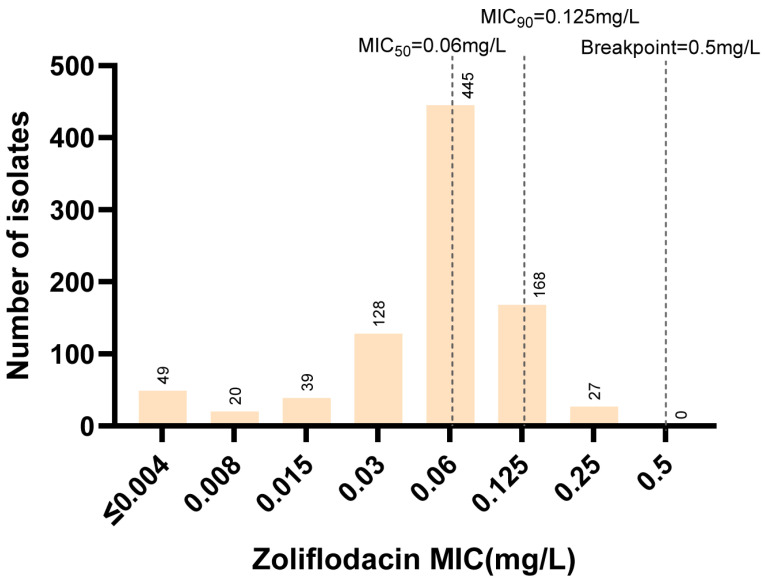 Figure 1
Figure 1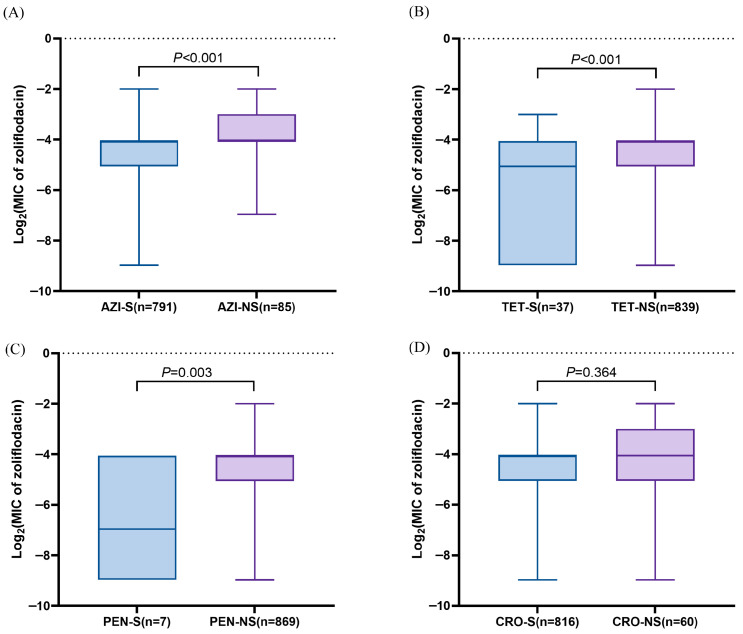 Figure 2
Figure 2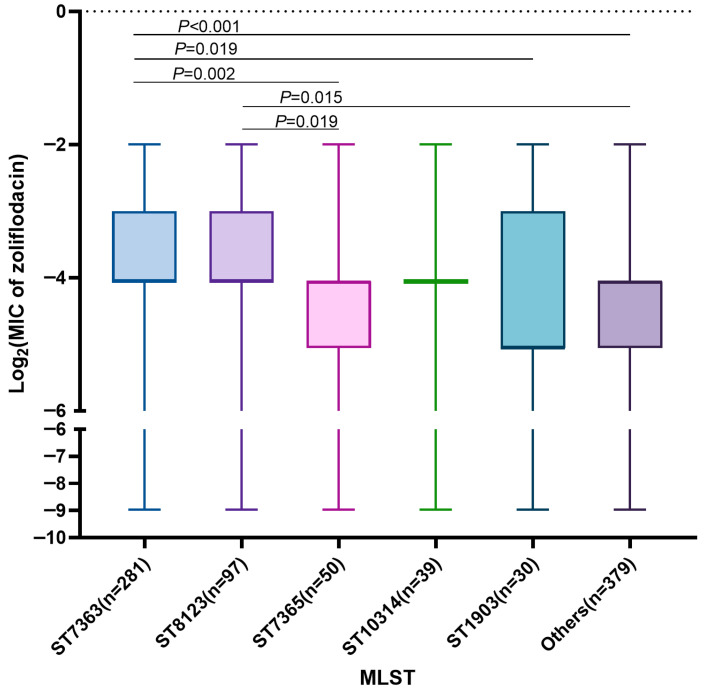 Figure 3
Figure 3- —National Natural Science Foundation of China
- —Natural Science Foundation of Shanghai
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive tract infections research · Bacterial Infections and Vaccines · Virology and Viral Diseases
1. Introduction
Gonorrhea poses a significant global public health challenge, with antimicrobial resistance in Neisseria gonorrhoeae representing a particular concern [1,2]. N. gonorrhoeae has developed resistance to all commonly used antimicrobial classes, including sulfonamides, penicillins, tetracyclines, and fluoroquinolones [3]. Currently, intramuscular ceftriaxone is recommended as the primary treatment for gonorrhea in both China and the United States [4,5], and European guidelines recommend combining it with azithromycin [6]. However, the global emergence and spread of ceftriaxone-resistant N. gonorrhoeae underscores the urgent need to develop novel antibacterial drugs to combat this growing threat [7].
The DNA gyrase (composed of GyrA and GyrB) and topoisomerase IV (composed of ParC and ParE) of N. gonorrhoeae are essential type II topoisomerases that play crucial roles in promoting DNA replication and transcription [8]. Several novel topoisomerase II inhibitors with potent activity against N. gonorrhoeae are currently under development. These include zoliflodacin, gepotidacin, and TP0480066, among others [8,9,10]. Zoliflodacin is a novel spiropyrimidinetrione antibiotic that induces DNA breaks mediated by gyrase and topoisomerase IV. Unlike fluoroquinolones, zoliflodacin primarily interacts with the GyrB subunit [8]. In vitro selection experiments with TP0480066 have identified substitutions in ParE in resistant mutants, although its precise target preference requires further elucidation [10]. In contrast, gepotidacin exhibits a well-balanced dual-targeting activity against both gyrase and topoisomerase IV in N. gonorrhoeae [11]. These novel topoisomerase II inhibitors exhibit potent antibacterial activity against N. gonorrhoeae, including strains resistant to fluoroquinolones. The phase III clinical trial demonstrated that a single 3-g oral dose of zoliflodacin achieved non-inferiority compared with intramuscular ceftriaxone combined with oral azithromycin [12]. Given zoliflodacin’s promising clinical efficacy and its unbalanced target interaction profile, understanding the pre-existing genetic landscape for potential resistance becomes an urgent public health priority.
Previous studies have shown that zoliflodacin has high activity in vitro against N. gonorrhoeae [13,14,15,16,17]. To date, only a single clinical isolate of N. gonorrhoeae with reduced susceptibility to zoliflodacin has been reported globally, the H035 strain from Japan, identified in 2000, which carries the GyrB-D429V substitution [18]. In contrast, in vitro selection experiments have identified the GyrB-D429A/N or K450T substitutions as first-step mutations that confer an increase in the minimum inhibitory concentration (MIC) of zoliflodacin (0.5–4 mg/L) [19,20]. These findings highlight the urgent need for large-scale, continuous surveillance of mutations in type II topoisomerases among clinical gonococcal isolates prior to the widespread implementation of zoliflodacin therapy.
In this multicenter study, we collected 876 N. gonorrhoeae isolates from 35 hospitals across different districts of Shanghai, China between 2020 and 2023. We assessed the in vitro susceptibility of these isolates to zoliflodacin and compared zoliflodacin MICs between drug-susceptible and drug-resistant strains, as well as among strains belonging to different multilocus sequence typing (MLST) clones. Finally, mutations in genes associated with zoliflodacin resistance, including gyrA, gyrB, parC, parE, and mtrR were analyzed. Together, our findings provide evidence supporting the potential clinical use of zoliflodacin for the treatment of N. gonorrhoeae infections.
2. Results
2.1. Clinical and Microbiological Characteristics
In this study, we collected 876 N. gonorrhoeae isolates (one per patient) from the urogenital tracts of patients attending 35 hospitals across Shanghai, China, between 2020 and 2023. The majority of patients were male (85.73%, 751/876), over 20 years of age (93.49%, 819/876), and primarily presented with urethral infections (86.07%, 754/876) (Table 1). Most isolates (75.91%, 665/876) were obtained from hospitals located in suburban regions, reflecting the widespread distribution of gonorrhea cases across both central and peripheral healthcare facilities in Shanghai.
The susceptibilities of all isolates to six commonly used antimicrobials were evaluated (Table 2). High resistance rates were observed for ciprofloxacin (99.54%, 872/874), tetracycline (78.54%, 688/876), and penicillin (78.20%, 685/876). The non-susceptible rates to ceftriaxone and azithromycin were 6.85% (60/876) and 9.70% (85/876), respectively. All isolates remained susceptible to spectinomycin. These findings suggest the continued effectiveness of spectinomycin, ceftriaxone, and azithromycin in Shanghai, while underscoring the need for ongoing surveillance of emerging ceftriaxone and azithromycin resistance.
2.2. In Vitro Activity of Zoliflodacin Against Drug-Susceptible and Drug-Non-Susceptible N. gonorrhoeae Isolates
We next determined the susceptibilities of these isolates to zoliflodacin. The overall distribution of zoliflodacin MICs ranged from ≤0.004 to 0.25 mg/L, with MIC_50_ and MIC_90_ values of 0.06 mg/L and 0.125 mg/L, respectively (Figure 1). Notably, all isolates, including those non-susceptible to ceftriaxone and azithromycin, were susceptible to zoliflodacin (Table 2), with MICs below the breakpoint of 0.5 mg/L. This indicates high in vitro activity of zoliflodacin against N. gonorrhoeae isolates.
Comparative analysis of zoliflodacin MICs between drug-susceptible and drug-non-susceptible N. gonorrhoeae isolates revealed that azithromycin-non-susceptible (p < 0.001), tetracycline-non-susceptible (p < 0.001), and penicillin-non-susceptible (p = 0.003) isolates exhibited significantly higher zoliflodacin MICs than their susceptible counterparts. In contrast, no significant difference in zoliflodacin MICs was observed between ceftriaxone-non-susceptible and ceftriaxone-susceptible isolates (p = 0.364) (Figure 2). These findings suggest potential cross-tolerance between zoliflodacin and certain classes of antimicrobials, although the mechanism underlying this association remains to be elucidated.
2.3. Zoliflodacin Susceptibility Across Different MLST Clones
Among the 876 N. gonorrhoeae isolates, 70 distinct sequence types (STs) were identified based on MLST. The predominant STs were ST7363 (32.08%, 281/876), ST8123 (11.07%, 97/876), and ST7365 (5.71%, 50/876), together accounting for nearly half of all isolates. Although all isolates were susceptible to zoliflodacin, their MIC values varied across different MLST clones. For example, ST7363 exhibited significantly higher zoliflodacin MICs compared with ST7365 (p = 0.002), ST1903 (p = 0.019), and the other minor sequence types (p < 0.001). Similarly, ST8123 showed higher MICs than ST7365 (p = 0.019) and the other minor sequence types (p = 0.015) (Figure 3). These findings suggest that certain clonal lineages may harbor genetic backgrounds conducive to increased zoliflodacin MICs.
2.4. Association Between Substitutions in GyrA, GyrB, ParC, ParE, and MtrR and Zoliflodacin Susceptibility in N. gonorrhoeae
Following a previous study, we investigated amino acid substitutions within the quinolone resistance-determining regions (QRDRs) of GyrA, GyrB, ParC, ParE, as well as in MtrR [15], to assess their potential impact on zoliflodacin susceptibility. In total, 8 distinct substitutions were identified in GyrA, 10 in GyrB, 17 in ParC, 7 in ParE, and 3 in MtrR (Table 3 and Table S1). The most prevalent alterations were GyrA-S91F (99.77%, 874/876), GyrA-D95A (72.95%, 639/876) and MtrR-A-53del (56.85%, 498/876). Most of the GyrB (91.10%, 798/876), and ParE (65.87%, 577/876) were wild-type.
To explore genotype-phenotype associations, isolates were categorized into lower-MIC group (MIC < MIC_90_, n = 681) and higher-MIC group (MIC ≥ MIC_90_, n = 195) based on zoliflodacin susceptibility. Univariate logistic regression analysis revealed that GyrA-D95Y (OR, 1.67; 95% CI, 1.04–2.70), ParC-D86N (OR, 1.47; 95% CI, 1.05–2.04), and MtrR-A39T (OR, 1.46; 95% CI, 1.06–2.01) were significantly associated with higher zoliflodacin MICs, suggesting a potential role in reduced susceptibility. Conversely, GyrA-D95G (OR, 0.54; 95% CI, 0.30–0.98), GyrA-D95N (OR, 0.26; 95% CI, 0.08–0.84), and ParE-P456S (OR, 0.55; 95% CI, 0.35–0.86) were correlated with lower MICs (Table 3). However, none of these associations remained statistically significant after correction, indicating that these associations may be weak.
3. Discussion
The increasing resistance of N. gonorrhoeae to first-line drugs including ceftriaxone and azithromycin underscores the urgent need for new antimicrobial agents for gonorrhea treatment [21]. Zoliflodacin, a novel spiropyrimidinetrione antibiotic, has demonstrated promising results in phase III clinical trials, showing strong efficacy against gonorrhea and offering a new therapeutic option [12]. In this study, zoliflodacin exhibits high in vitro activity against 876 N. gonorrhoeae isolates with varied resistance backgrounds and no resistance-associated substitutions were identified in GyrA, GyrB, ParC, ParE, and MtrR. Although overall susceptibility remained high, ST7363 and ST8123 show elevated zoliflodacin MICs compared with other sequence types. Together, these findings provide a molecular basis for zoliflodacin’s sustained antibacterial efficacy while also highlighting that resistance-associated mutations could spread clonally, emphasizing the need for ongoing monitoring as zoliflodacin moves toward clinical use.
The MIC_50_ and MIC_90_ of zoliflodacin against the 876 N. gonorrhoeae isolates were determined to be 0.06 mg/L and 0.125 mg/L, respectively, aligning with previous studies [13,15,17]. However, isolates with decreased susceptibility to penicillin, tetracycline, and azithromycin exhibited elevated zoliflodacin MICs compared to their susceptible counterparts. This phenomenon potentially mediated by non-target mechanisms such as enhanced efflux pump activity. For example, mutations in mtrR can lead to overexpression of the MtrCDE efflux pump [22], which may elevate zoliflodacin MICs in the harboring strains. However, MtrR-A39T lost significance after correction, suggesting that this substitution alone may exert only a minor effect on zoliflodacin susceptibility. Supporting this, previous studies indicated that while efflux pump overexpression can elevate zoliflodacin MICs, it is insufficient to confer full resistance in the absence of concomitant zoliflodacin-associated GyrB substitutions [20].
We identified 10 distinct GyrB substitutions, with 91.10% of isolates retaining the wild-type genotype, indicating high conservation of GyrB in clinical N. gonorrhoeae. Previous in vitro selection experiments under zoliflodacin pressure consistently yielded mutants with GyrB-D429N/A or K450T/N substitutions, conferring MICs of 0.5–4 mg/L [19,20,23]. Notably, these critical substitutions were absent in our clinical collection and have not been reported in other surveillance studies, suggesting they are specifically induced by zoliflodacin. Previous work by Richard A. Alm et al. demonstrated that while the GyrB-S467N substitution alone does not confer resistance, it acts synergistically with GyrB-D429N, elevating the zoliflodacin MIC to 8 mg/L [19]. A concerning route to resistance involves horizontal gene transfer; N. macacae has been identified as a potential source of the GyrB-S467N allele for N. gonorrhoeae [24,25]. The low prevalence of GyrB-S467N in our study (0.68%, 6/876) and global surveillance (0.12%) indicates that it has not disseminated via horizontal gene transfer to become a stepping-stone to high-level zoliflodacin resistance [26]. Furthermore, zoliflodacin exhibits a low spontaneous mutation frequency, and resistant mutants selected in vitro demonstrate a substantial fitness cost [19,27].
In comparison, gepotidacin, another novel oral topoisomerase II inhibitor in advanced clinical development for gonorrhea, exhibits a well-balanced dual-targeting of gyrase and topoisomerase IV [11]. Similarly to zoliflodacin, the frequency of resistance to gepotidacin is low [28]. However, a key concern is that in the context of widespread fluoroquinolone resistance, acquired substitutions such as ParC-D86N can accumulate and act as stepping-stones, enabling N. gonorrhoeae to develop high-level gepotidacin resistance more rapidly [29,30,31]. Therefore, while both are promising oral agents with low resistance frequencies, the different mechanisms of zoliflodacin and gepotidacin pose distinct genetic challenges and may drive divergent evolutionary paths to resistance in N. gonorrhoeae.
However, the emergence of resistance-associated substitutions may vary across clones. Previous studies reported that the majority of N. gonorrhoeae isolates carrying the GyrB-S467N substitution belong to ST7363 (74%, 37/50) [24], and the two Norwegian isolates with the highest zoliflodacin MIC (0.5 mg/L) were clonally related [32]. Our study showed that isolates belonging to ST7363 and ST8123 exhibited higher zoliflodacin MICs compared with others. ST7363 and ST8123 are reported to harbor mosaic penA alleles and to be associated with elevated ceftriaxone MICs [33,34,35], reflecting their capacity for clonal expansion and accumulation of resistance determinants. This suggests that once zoliflodacin-resistant-associated substitutions arise, they may be preferentially amplified within certain genomic backgrounds.
Pharmacokinetic studies have shown that a single 3-g oral dose in the single-ascending-dose (SAD) study achieved a geometric mean maximum plasma concentration (Cmax) above 20 mg/L, and mean terminal elimination half-life (t_1/2_) was 6.2 h [36]. This PK profile supports that serum concentrations can be maintained above 5 mg/L for approximately 12 h following the peak. No drug-related serious adverse events were reported (ClinicalTrials registration no. NCT03959527).
In conclusion, the high in vitro activity of zoliflodacin against N. gonorrhoeae observed in this study supports the potential clinical effectiveness of this novel agent. However, continued phenotypic and genomic surveillance of zoliflodacin-resistant N. gonorrhoeae is warranted, as mutations associated with elevated zoliflodacin MICs may emerge and spread clonally, potentially compromising its long-term clinical utility.
4. Materials and Methods
4.1. Isolation and Cultivation of N. gonorrhoeae Strains
From 2020 to 2023, a total of 876 N. gonorrhoeae strains were collected from patients in Shanghai. The strains were inoculated onto Thayer-Martin (TM) selective agar and cultured at 37 °C with 5% CO_2_ and controlled humidity for 18 h. After cultivation, the strains were suspended in tryptic soy broth with glycerol and stored at −80 °C for future use.
4.2. Antimicrobial Susceptibility Testing
MICs were determined using the agar dilution method in accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines. The quality control strain used was ATCC49226. Penicillin, tetracycline, ceftriaxone, azithromycin, spectinomycin, ciprofloxacin, and zoliflodacin were purchased from MCE (MedChemExpress, Monmouth Junction, NJ, American). The breakpoint for zoliflodacin of ≥0.5 mg/L was utilized as previously described [37]. Antibiotic resistance breakpoints were applied based on the CLSI and European Committee on Antimicrobial Susceptibility Testing (EUCAST) criteria (for spectinomycin only) as follows: penicillin (MIC ≥ 2 mg/L), tetracycline (MIC ≥ 2 mg/L), ceftriaxone (MIC > 0.25 mg/L, non-susceptible), azithromycin (MIC > 1 mg/L, non-susceptible), spectinomycin (MIC ≥ 128 mg/L), and ciprofloxacin (MIC ≥ 1 mg/L) [38,39].
4.3. Whole-Genome Sequencing and Analysis
Genomic DNA was extracted from the 876 isolates using the bacterial genomic DNA extraction kit from TIANGEN Biotech (Beijing, China) as previous described [40]. Sequencing was performed on the Illumina HiSeq platform using 150 bp paired-end sequencing technology. Reads were assembled using SPAdes V3.8 software with default parameters, and alleles shorter than 500 nucleotides were excluded [41]. The sequence types were matched based on the pubMLST database (https://pubmlst.org/). Mutations in gyrA, gyrB, parC, parE, and mtrR were identified using pyngSTar with a database from CARD [42,43] and Snippy v4.6.0 (https://github.com/tseemann/snippy, accessed on 1 July 2025).
4.4. Statistical Analysis
The 876 isolates were categorized into a high-MIC group (MIC ≥ MIC_90_) and a low-MIC group (MIC < MIC_90_). The frequency of each genetic feature was calculated, and features with frequencies <1% or >99% were excluded. Univariate logistic regression was then performed to assess the impact of GyrA, GyrB, ParC, ParE, and MtrR substitutions on zoliflodacin susceptibility. The distributions of log_2_-transformed zoliflodacin MIC values were compared among isolates with different antimicrobial susceptibility profiles and sequence types using the Wilcoxon test. All statistical analyses were conducted using R software (version 4.3.0), with a significance level set at p < 0.05. p values were adjusted using the false discovery rate (FDR) method.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unemo M. Seifert H.S. Hook E.W.3rd Hawkes S. Ndowa F. Dillon J.R. Gonorrhoea Nat. Rev. Dis. Primers 201957910.1038/s 41572-019-0128-631754194 · doi ↗ · pubmed ↗
- 2Wi T. Lahra M.M. Ndowa F. Bala M. Dillon J.R. Ramon-Pardo P. Eremin S.R. Bolan G. Unemo M. Antimicrobial resistance in Neisseria gonorrhoeae: Global surveillance and a call for international collaborative action P Lo S Med.201714 e 100234410.1371/journal.pmed.100234428686231 PMC 5501266 · doi ↗ · pubmed ↗
- 3Unemo M. Shafer W.M. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: Past, evolution, and future Clin. Microbiol. Rev.20142758761310.1128/CMR.00010-1424982323 PMC 4135894 · doi ↗ · pubmed ↗
- 4Wang Q.-Q. Zhang R.-L. Liu Q.-Z. Xu J.-H. Su X.-H. Yin Y.-P. Qi S.-Z. Xu D.-M. Zhou P.-Y. Li Y.-Y. National Guidelines on Diagnosis and Treatment of Gonorrhea in China (2020)#Int. J. Dermatol. Venereol.2020312913410.1097/jd 9.0000000000000072 · doi ↗
- 5Workowski K.A. Bachmann L.H. Chan P.A. Johnston C.M. Muzny C.A. Park I. Reno H. Zenilman J.M. Bolan G.A. Sexually Transmitted Infections Treatment Guidelines, 2021 MMWR. Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep.202170118710.15585/mmwr.rr 7004 a 134292926 PMC 8344968 · doi ↗ · pubmed ↗
- 6Unemo M. Ross J. Serwin A.B. Gomberg M. Cusini M. Jensen J.S. 2020 European guideline for the diagnosis and treatment of gonorrhoea in adults Int. J. STD AIDS 202095646242094912610.1177/095646242094912633121366 · doi ↗ · pubmed ↗
- 7Unemo M. Lahra M.M. Cole M.J. Marcano Zamora D. Jacobsson S. Galarza P. Martin I. Kreisel K.M. Galas M. Bertagnolio S. WHO global gonococcal antimicrobial surveillance programmes, 2019–2022: A retrospective observational study Lancet Microbe 2025610118110.1016/j.lanmic.2025.10118141015046 PMC 12715682 · doi ↗ · pubmed ↗
- 8Collins J.A. Osheroff N. Gyrase and Topoisomerase IV: Recycling Old Targets for New Antibacterials to Combat Fluoroquinolone Resistance ACS Infect. Dis.2024101097111510.1021/acsinfecdis.4c 0012838564341 PMC 11019561 · doi ↗ · pubmed ↗