An Algorithm for Rapid and Low-Cost Detection of Carbapenemases Directly from Positive Blood Cultures Using an Immunochromatographic Test
Patricia del Carmen García, Pamela Rojas, Ana María Guzmán, Sofía Paz Torres, Aniela Wozniak

TL;DR
This paper introduces a rapid and low-cost test to detect carbapenemases in blood cultures, offering a faster alternative to traditional methods.
Contribution
The study evaluates a novel immunochromatographic test for direct detection of carbapenemases from blood cultures, with a pragmatic confirmation algorithm.
Findings
The test detected 100% of carbapenemase-producing blood cultures with high sensitivity.
False positives occurred in 13 cases, but confirmatory tests showed these were negative for the enzymes.
The test is a viable alternative for low-resource hospitals lacking qPCR panels.
Abstract
Background/Objectives: Detection of carbapenemases (KPC, OXA-48, VIM, IMP, NDM) from blood cultures (BCs) by standard methods takes 48–72 h and includes BC seeding, susceptibility testing and carbapenemase detection. Automated qPCR panels provide results in 1 h but are very costly. We aim to evaluate a low-cost and rapid immunochromatographic (IC) test directly from positive BCs using the reference method as a comparator. Methods: Ninety-one positive BCs from real-world patients and sixty-four simulated BCs were included. BC broth was treated with SDS and washed before analysis with the K.N.I.V.O. carbapenemase detection IC test. Discordant results were confirmed through the NG Carba-5 IC test and GeneXpert Carba-R qPCR test. Results: The test detected 100% of the 87 carbapenemase-producing BCs tested (sensitivity: 100% [CI95%: 95.8–100%]). However, 13 BCs generated false positive bands…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
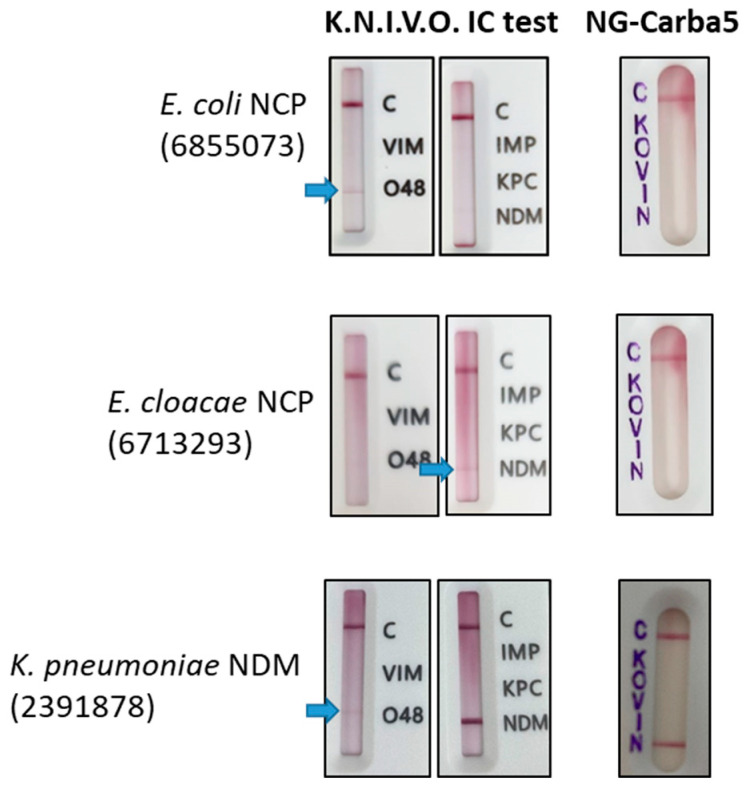 Figure 1
Figure 1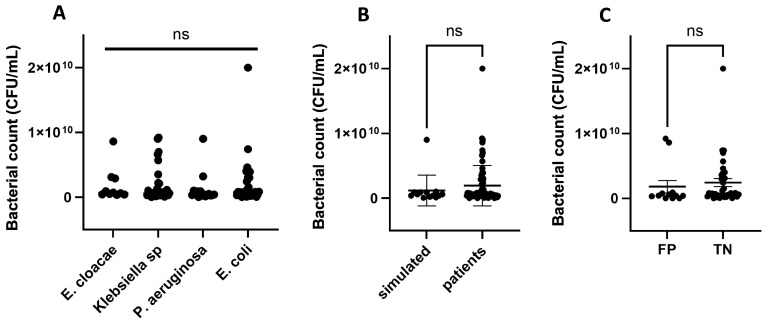 Figure 2
Figure 2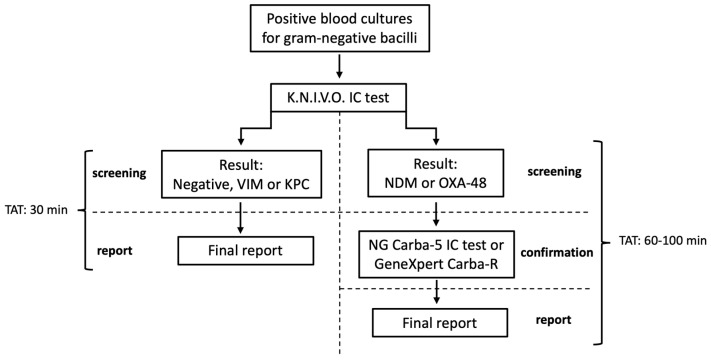 Figure 3
Figure 3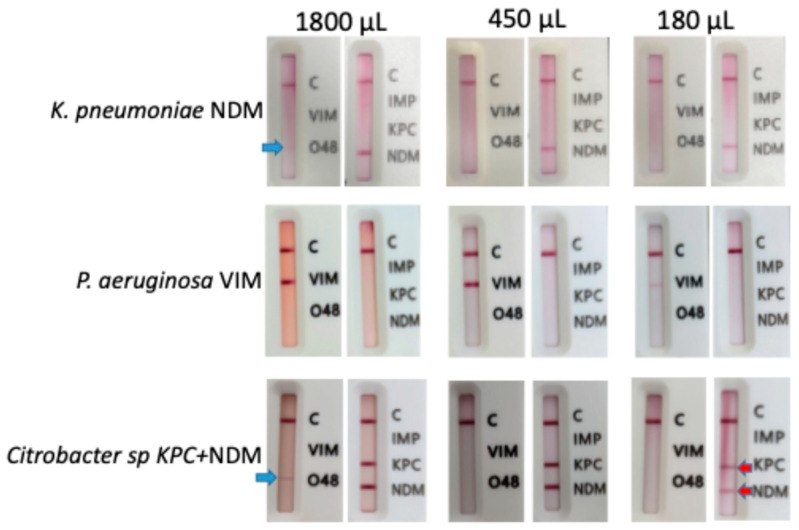 Figure 4
Figure 4- —Department of Clinical Laboratories at the School of Medicine in Pontificia Universidad Católica de Chile
- —Health Network Red de Salud UC-CHRISTUS
- —SENTRY (Antimicrobial Resistance Surveillance Program)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Antibiotic Resistance in Bacteria · Neonatal and Maternal Infections
1. Introduction
Bloodstream infections (BSIs) and associated serious conditions like sepsis and septic shock are among the top causes of mortality worldwide, killing between one in three and one in six of affected patients [1]. BSIs are associated with extended hospital stay, increased use of antimicrobials, and a major economic burden [2]. One of the most important factors determining the outcome of BSIs is the time to appropriate antimicrobial treatment. Observational data reported a 30% increase in mortality when adequate treatment was not administered within the first 24 h [3]. For this reason, broad-spectrum antimicrobials are usually administered as empirical treatment in patients with BSIs while waiting for final microbiological reports [4]. This may lead to the overuse of broad-spectrum antimicrobials and its associated side-effects, including enhancement of antimicrobial resistance [5], and increased costs, especially in developing countries.
BSIs caused by carbapenemase-producing bacteria pose a significant challenge for the management of BSIs because they have a higher mortality rate than those caused by carbapenem-susceptible bacteria [6]. KPC, OXA-48, VIM, NDM and IMP are the most frequent carbapenemases, referred to as the “big five”, and confer resistance to a broad range of antimicrobials including penicillins, cephalosporins and carbapenems, the latter being often used a last resort for severe infections. A study involving carbapenem-resistant bacteria obtained from blood cultures (BCs) between January 2018 and April 2024 among 11 hospitals in Chile showed that 2626 were Enterobacterales (83%) and 533 were P. aeruginosa (17%). Fourteen percent of Enterobacterales produced NDM, KPC and VIM, and 43% of P. aeruginosa were producers of VIM and KPC (unpublished data from the MICROB-R Network in Chile).
Detection of carbapenemase-producing bacteria from BCs by the reference method usually takes 48–72 h [4]. The BCs are subcultured in appropriate media, and after 18–24 of growth, identification is performed through MALDI-TOF (Bruker, Bremen, Germany) mass spectrometry. Susceptibility testing takes another 18–24 h and carbapenem-non-susceptible bacteria are analyzed through Carba-NP test for biochemical detection of carbapenemase activity. Finally, the enzyme is identified using an immunochromatographic (IC) test to detect the “big five” carbapenemases. The FilmArray blood culture ID panel (BCID2) (BioFire, Salt Lake City, UT, USA) detects 43 different targets, including the “big five” carbapenemases, directly from positive BCs in 1 h. However, its main hurdle is the elevated cost [7]. Similarly, the GeneXpert Carba-R (Cepheid, Sunnyvale, CA, United States) platform is an automated q-PCR that detects the “big-five” carbapenemase genes in rectal swabs and has shown high sensitivity and specificity (100%) when used directly from positive BCs [8]. Unfortunately, the GeneXpert test is also very expensive. Although IC tests for carbapenemase detection are standardized to be performed with pure bacterial suspensions, they were evaluated directly in positive BCs: the NG Carba-5 IC test (NG-Biotech, Marcy l’Étoile, France) [9,10,11,12] and Resist-5 O.K.N.I.V. (CORIS Bio-concept, Gemblouxm Belgium) IC test [13,14] are the most reported ones. In the present work, we evaluated the K.N.I.V.O. (which stands for KPC, NDM, IMP, VIM, OXA-48) carbapenemase detection IC test (Genobio, Tianjin, China) directly in positive BCs from both simulated and real-world patients, using an in-house-developed method for BC preparation prior to IC testing, using the reference method as a comparator.
2. Results
2.1. Performance of K.N.I.V.O. IC Test
Ninety-one positive BCs from real-world patients and sixty-four simulated BCs were included in this study (total = 155 BCs). Distribution of species and carbapenemases produced by the different isolates is shown in Table 1.
On the other hand, 87 BCs had carbapenemase-producing bacteria and 68 had non-carbapenemase-producing (NCP) bacteria. The K.N.I.V.O. IC test detected 100% of the 87 carbapenemase-positive BCs, including 30 NDM, 16 KPC, 24 VIM and 4 OXA-48 and 13 double-carbapenemase producers (Table 1). No BCs with IMP carbapenemase were analyzed because of the low prevalence of this carbapenemase in Chile. Therefore, this carbapenemase was not included in our study. According to these results, the direct IC test for detection of carbapenemases in positive BCs had a global sensitivity of 100%. However, 13 BCs generated false positive bands in the screening IC assay: 3 for NDM, 5 for OXA-48 and 5 for NDM + OXA-48, meaning that the global specificity of the test was 80.8% (Table 2). The positive and negative predictive values were 87.0% and 100%, respectively. Non-specific bands were weak (Figure 1); in contrast, bands generated by true OXA-48 and NDM isolates had the same intensity as the control band. False positives occurred in K. pneumoniae (n = 4), E. coli (n = 5), E. cloacae (n = 1), S. marcescens (n = 1) and M. morganii (n = 1). Of the 13 false positives, 12 occurred in real-world BCs whereas only 1 occurred in a simulated BC. The sensitivity, specificity, positive and negative predictive value were calculated for each carbapenemase as shown in the lower part of Table 2. Sensitivity was 100% for the four carbapenemases analyzed. Specificity values for VIM and KPC were 100%. In contrast, specificity values for NDM and OXA-48 were 92.8% and 93.3%, respectively.
BCs showing discordant results between the reference method and K.N.I.V.O. IC test directly from BC were analyzed using the NG Carba-5 IC test and GeneXpert Carba-R. Confirmatory testing of false positive samples with NG Carba-5 IC and GeneXpert Carba-R was negative for OXA-48 and NDM, indicating that the weak bands observed were non-specific (Table 3, Figure 1).
2.2. Bacterial Load of Blood Cultures
Because non-specific bands were observed in the optimization step when using 1800 µL of BC fluid (see Materials and Methods), we hypothesized that false positive results could arise from a high bacterial count. Bacterial counts of BCs were between 10^8^ and 10^9^ CFU/mL and they were not different among the different species nor among simulated and real-world BCs (Figure 2A,B). Furthermore, samples exhibiting false positive results did not have higher bacterial counts than true negative samples (Figure 2C).
In view of the results obtained, we propose an algorithm for early detection of carbapenemases in positive BCs for Gram-negative bacilli, using the K.N.I.V.O. IC test followed by a confirmatory test in case the results are NDM and/or OXA-48 (Figure 3). The total turn-around time (TAT) for negative, KPC and VIM results is 30 min. In the case of NDM and OXA-48, which require confirmatory testing, the total turn-around time is 60–100 min. Confirmation of NDM and OXA-48 may be performed through the NG Carba-5 IC test in low-resource settings (30 min for screening IC test + 30 min for confirmatory IC test), or through GeneXpert Carba-R in higher-resource settings (30 min for screening IC test + 70 min for confirmatory GeneXpert Carba-R).
3. Discussion
Early adequate antimicrobial therapy in cases of sepsis or septic shock is crucial to improve patient outcome. Empirical treatment should be broad enough to cover possible pathogens according to local epidemiology data [4]. Ceftazidime/avibactam (CZA) is a last-generation β-lactam/β-lactamase-inhibitor combination, widely used as an empirical therapy in BSIs in regions with a high prevalence of carbapenemase-producing organisms [15], like Chile. Class A and D enzymes like KPC and OXA-48 are inhibited by avibactam, whereas class B enzymes like NDM or VIM are not, and so other options like aztreonam/CZA may be used [16]. Because bacterial species and carbapenemase class are not known at the time of empirical treatment prescription, the antibiotics prescribed may not be adequate [17]. For this reason, once laboratory results are available, they must be used to adjust the initial empirical treatment. The procedure evaluated here can determine the carbapenemase class 48–72 h earlier than the reference method. Knowing carbapenemase class before standard tests are ready would avoid unnecessary overuse of broad-spectrum antimicrobials like CZA in case no carbapenemases are detected, and consequently would prevent or delay the emergence of antimicrobial resistance towards last-resort antimicrobials like CZA. Importantly, in case a class B enzyme is detected, the early diagnostic would support an empiric therapy with aztreonam/CZA instead of CZA alone; in this case, early diagnosis would also contribute to patient survival.
Most reports of IC tests for early diagnosis of carbapenemases in BCs mainly include Enterobacterales [10,12,13,14], with few reports in P. aeruginosa and using a very low number of isolates (two IMP producers and eleven NCP P. aeruginosa isolates) [9,11]. Our results show that this test can detect carbapenemase-producing P. aeruginosa, with 100% (95% CI: 95.8–100%) sensitivity using the reference method as a comparator. Although our method achieved an excellent sensitivity for detection of the “big five” carbapenemases, NDM and OXA-48 showed low specificity (80.8%; CI 95%: 69.5–89.4%). Most reports about the evaluation of IC tests to detect carbapenemases directly from BCs used the NG Carba-5 IC test and reported overall sensitivities that ranged from 93% to 100% [9,10,11,12]. In these reports, the IC test failed to detect some VIM and/or NDM carbapenemases, whereas all KPC and OXA-48 were detected. A recent work compared NG Carba-5 with the K.N.I.V.O. IC test using different inoculum sizes of bacterial suspensions as recommended by the manufacturer and reported false positive results for OXA-48 and NDM using the K.N.I.V.O. IC test with all inoculum sizes [18]. In contrast, the NG Carba-5 test showed false positive results only when a heavy inoculum was used. These results suggest that whereas the K.N.I.V.O. IC test seems to have improved sensitivity for the detection of VIM and NDM, it has lower specificity for detection of NDM and OXA-48. To our knowledge, this is the first evaluation of the K.N.I.V.O. IC test applied directly to positive BCs, with a pragmatic confirmation algorithm that addresses K.N.I.V.O.’s specificity gap. We observed that false positive results occurred in BCs having similar bacterial counts to the true positive samples, suggesting that inoculum size is not the problem. False positives occurred in almost all species tested (Supplementary Material, Table S1), indicating that species is not the problem either, and suggesting that particular bacterial traits may be responsible for these non-specificities. False positives in lateral flow assays may arise due to sub-optimal composition of lysis buffers, non-specific protein–conjugate interactions and cross-reactivity [19].
The limitations of this work include the fact that only two health networks were included. In addition to this, because the NG Carba-5 IC test and GeneXpert Carba-R were performed only in samples exhibiting false positive results, a partial-verification bias may have occurred. In addition, only five BCs with an OXA-48-producing organism were tested, basically due to the low prevalence of this carbapenemase in our setting, and IMP carbapenemase was not tested. The multi-site workflow may be another limitation of this work, because real patients’ BCs that became positive during the weekend were stored before testing whereas simulated BCs were not. However, false positive bands were not generated by BCs that had been stored over the weekend; they were generated by BCs that were analyzed immediately or within 2–3 h. Validation of the algorithm proposed in real-world conditions would be required to use this test in routine analysis.
Screening positive BCs with the K.N.I.V.O. IC test plus mandatory confirmation for NDM/OXA-48 positives delivers rapid and implementable stewardship value in routine BC workflows. Because of its low cost and short turn-around time, it may be an alternative for rapid and low-cost detection of carbapenemases directly from BCs in low-resource hospitals, where automated qPCR panels are not available.
4. Materials and Methods
4.1. Blood Cultures from Patients
The real-world positive BCs were obtained from patients hospitalized during 2024 and 2025 in the Hospital of UC-CHRISTUS Health Network and in the Padre Hurtado Hospital, both in Santiago, Chile. BCs were analyzed using the reference method as follows. After being incubated in a BACT/ALERT VIRTUO™ system (Biomerieux, Marcy l’Étoile, France) and flagged positive, BCs were Gram-stained, microscopically observed and cultured in appropriate media. Colonies obtained were identified using MALDI-TOF spectrometry analysis in UC-CHRISTUS Hospital, and Phoenix^TM^ (Beckton-Dickinson, Sparks, MD, USA) in Padre Hurtado Hospital. Antimicrobial susceptibility testing was performed through the agar dilution method and those isolates that were non-susceptible (intermediate or resistant) to at least one carbapenem (imipenem, meropenem, ertapenem) were analyzed for carbapenemase production through the Carba-NP test according to CLSI guidelines (Clinical and Laboratory Standards Insitute 2024) [20]. Isolates exhibiting a positive Carba-NP test were analyzed to determine the identity of the carbapenemase/s produced through the K.N.I.V.O. Carbapenemase-Detection IC test (Genobio, Tianjin, China; LOT: 231103) in UC-CHRISTUS Hospital and Resist-5 O.K.N.I.V. (CORIS Bio-concept, Gembloux, Belgium) in Padre Hurtado Hospital. The technician was blinded to the result of the IC test that was performed directly from BCs 2–3 days prior.
4.2. Simulated Blood Cultures
Simulated BCs were inoculated with known carbapenemase-producing isolates that were stored in the laboratory, previously confirmed through PCR followed by Sanger sequencing [21] or through the IC test as described above. Isolates were grown in blood agar and used to prepare a McFarland 0.5 bacterial suspension that was diluted 1/100,000 in PBS, and 100–300 µL were added to BACT/ALERT (Biomerieux, Marcy l’Étoile, France) pediatric BC bottles. Using this inoculation protocol, time to positivity was similar to real BCs (9–16 h) [12]. All the bottles were inoculated with 5–10 mL of blood from healthy donors (the authors AW, AMG and ST). Bottles were incubated in a BACT/ALERT VIRTUO™ system until flagged positive and immediately cooled at 4 °C until processing. Time to processing varied between 1 and 10 h depending on the hour that bottles were flagged positive. The technician that read the IC tests was blinded to the species and carbapenemases produced by the isolates inoculated in the BC bottles.
4.3. Direct IC Test of BCs
Positive BCs from patients that exhibited Gram-negative bacilli in the microscopic observation were immediately analyzed using the K.N.I.V.O. carbapenemase detection IC test using the protocol as follows. Patient BCs that were flagged positive during the weekend were stored at 4 °C and processed on the next working day. An aliquot of 450 µL of the positive BC was obtained from the bottle and mixed with 50 µL of 10% SDS to lyse blood cells, vortexed and incubated for 5 min at room temperature. Tubes were centrifuged 3 min at 13,000× g and supernatant was discarded. The pellet was washed with 1 mL of distilled water and centrifuged again. Supernatant was discarded and the pellet was resuspended in 5 drops of lysis reagent of the K.N.I.V.O. carbapenemase detection IC test, and 50 µL of this mix was added to the sample window of the IC test cassette. Results were read within 15 min. The turn-around time for this test is 30 min (25–45 min). To determine the optimal volume of BC fluid to be used in the direct IC test, 6 simulated BCs of isolates producing KPC, VIM and NDM were evaluated using three different volumes of BC: 180 µL, 450 µL and 1800 µL. Proportional volumes of 10% SDS and water were added to the tubes. The pellets were resuspended in 5 drops of lysis reagent and the procedure was continued as described above. When 180 µL was used, KPC and NDM bands were clearly observed. In contrast, VIM bands had a lower but still readable intensity. When 1800 µL was used, non-specific weak bands were observed for OXA-48 and NDM. When 450 µL was used, bands had similar intensity to the control band, and non-specific bands were not observed (Figure 4). Based on these results, the 450 µL volume was used for subsequent IC tests.
4.4. Bacterial Count of BCs
A total of 100 µL of a 1/100,000 dilution of positive BCs was cultured in McConkey agar to quantitatively determine the bacterial load in simulated and real-world BCs. After 24 h of incubation at 35 °C, colonies were counted.
4.5. Analysis of Discordant Results
Discordant results (inconsistent with reference method, i.e., false positives) were analyzed with the NG Carba-5 IC test (NG-Biotech, Guipry, France; LOT: 230515-01-B) using the same sample preparation protocol described above. The turn-around time for this test is also 30 min (25–35 min). Discordant results were also analyzed through GeneXpert Carba-R (Cepheid; LOT: 1001425237) using the protocol described by Cointe and coworkers [8]. Briefly, 40 µL of positive blood culture fluid was mixed with 1700 µL of GeneXpert sample reagent buffer and incubated for 10 min at room temperature. Using a disposable plastic pipette, 1.5 mL was loaded into the cartridge and analyzed in the GeneXpert equipment. The turn-around time for this test is 75 min (70–80 min). To ensure reproducibility of the results, the tests were performed by technicians with >3 years of experience in laboratory microbial diagnosis.
4.6. Statistical Analysis
All statistical analyses were carried out using GraphPad Prism 10 v 10.6.1. One-way ANOVA analyses were performed when 3 or more variables were evaluated. Tukey’s test was used for multiple comparisons. Student’s t-test was used to compare two variables. For all analyses, a p value = 0.05 was considered statistically significant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evans L. Rhodes A. Alhazzani W. Antonelli M. Coopersmith C.M. French C. Machado F.R. Mcintyre L. Ostermann M. Prescott H.C. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021 Intensive Care Med.2021471181124710.1007/s 00134-021-06506-y 34599691 PMC 8486643 · doi ↗ · pubmed ↗
- 2Zhang Y. Du M. Johnston J.M. Andres E.B. Suo J. Yao H. Huo R. Liu Y. Fu Q. Estimating length of stay and inpatient charges attributable to hospital-acquired bloodstream infections Antimicrob. Resist. Infect. Control 2020913710.1186/s 13756-020-00796-532811557 PMC 7431751 · doi ↗ · pubmed ↗
- 3Adrie C. Garrouste-Orgeas M. Ibn Essaied W. Schwebel C. Darmon M. Mourvillier B. Ruckly S. Dumenil A.S. Kallel H. Argaud L. Attributable mortality of ICU-acquired bloodstream infections: Impact of the source, causative micro-organism, resistance profile and antimicrobial therapy J. Infect.20177413114110.1016/j.jinf.2016.11.00127838521 · doi ↗ · pubmed ↗
- 4Tabah A. Lipman J. Barbier F. Buetti N. Timsit J.F. On Behalf Of The Escmid Study Group For Infections In Critically Ill Patients—Esgcip Use of Antimicrobials for Bloodstream Infections in the Intensive Care Unit, a Clinically Oriented Review Antibiotics 20221136210.3390/antibiotics 1103036235326825 PMC 8944491 · doi ↗ · pubmed ↗
- 5Arulkumaran N. Routledge M. Schlebusch S. Lipman J. Conway Morris A. Antimicrobial-associated harm in critical care: A narrative review Intensive Care Med.20204622523510.1007/s 00134-020-05929-331996961 PMC 7046486 · doi ↗ · pubmed ↗
- 6Chen L. Han X. Li Y. Li M. Assessment of Mortality-Related Risk Factors and Effective Antimicrobial Regimens for Treatment of Bloodstream Infections Caused by Carbapenem-Resistant Enterobacterales Antimicrob. Agents Chemother.202165 e 006982110.1128/AAC.00698-2134228539 PMC 8370219 · doi ↗ · pubmed ↗
- 7Mauri C. Consonni A. Briozzo E. Giubbi C. Meroni E. Tonolo S. Luzzaro F. Microbiological Assessment of the Film Array Blood Culture Identification 2 Panel: Potential Impact in Critically Ill Patients Antibiotics 202312124710.3390/antibiotics 1208124737627667 PMC 10451250 · doi ↗ · pubmed ↗
- 8Cointe A. Walewski V. Hobson C.A. Doit C. Bidet P. Dortet L. Bonacorsi S. Birgy A. Rapid Carbapenemase Detection With Xpert Carba-R V 2 Directly On Positive Blood Vials Infect. Drug Resist.2019123311331610.2147/IDR.S 20443631695450 PMC 6815938 · doi ↗ · pubmed ↗