A Systematic Review of the Current Evidence of the Effectiveness and Safety of Immunoprophylaxis Using Sublingual Dead Whole Bacteria to Prevent Recurrent Urinary Tract Infections (rUTIs)
José Medina-Polo, Ana Arrébola-Pajares, Eva Falkensammer, Zafer Tandogdu

TL;DR
This systematic review evaluates sublingual bacterial vaccines as a safe and effective alternative to antibiotics for preventing recurring urinary tract infections.
Contribution
The study systematically reviews evidence on sublingual immunoprophylaxis using inactivated whole bacteria for rUTI prevention.
Findings
UTI recurrence decreased from 3.2–6.8 to 0–1.5 episodes/year at 12 months with immunoprophylaxis.
UTI-free rates ranged from 10–49% with autovaccines and 9.7–60% with MV140 at 12 months.
Adverse events were predominantly mild, with 0–40.8% in treated patients versus 50% in placebo patients.
Abstract
Background/Objectives: Recurrent urinary tract infections (rUTIs) remain a major clinical challenge, but sublingual immunoprophylaxis with inactivated whole bacteria is a promising alternative to antibiotic prophylaxis. The objective of this systematic review was to assess the efficacy and safety of sublingual bacterial vaccines. Methods: We searched MEDLINE, Cochrane CENTRAL, and Embase (January 1979–August 2025) for English-language studies evaluating bacterial vaccines for rUTI prevention. Eligible studies included adults receiving sublingual immunoprophylaxis with heat-inactivated whole bacteria. Outcomes were UTI recurrence, infection-free interval, and adverse events. Both MV140 and autovaccines were assessed. Results: Of the 262 records identified, 14 studies met the inclusion criteria (4 comparatives, including 1 randomized trial, and 10 observational studies). UTI incidence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
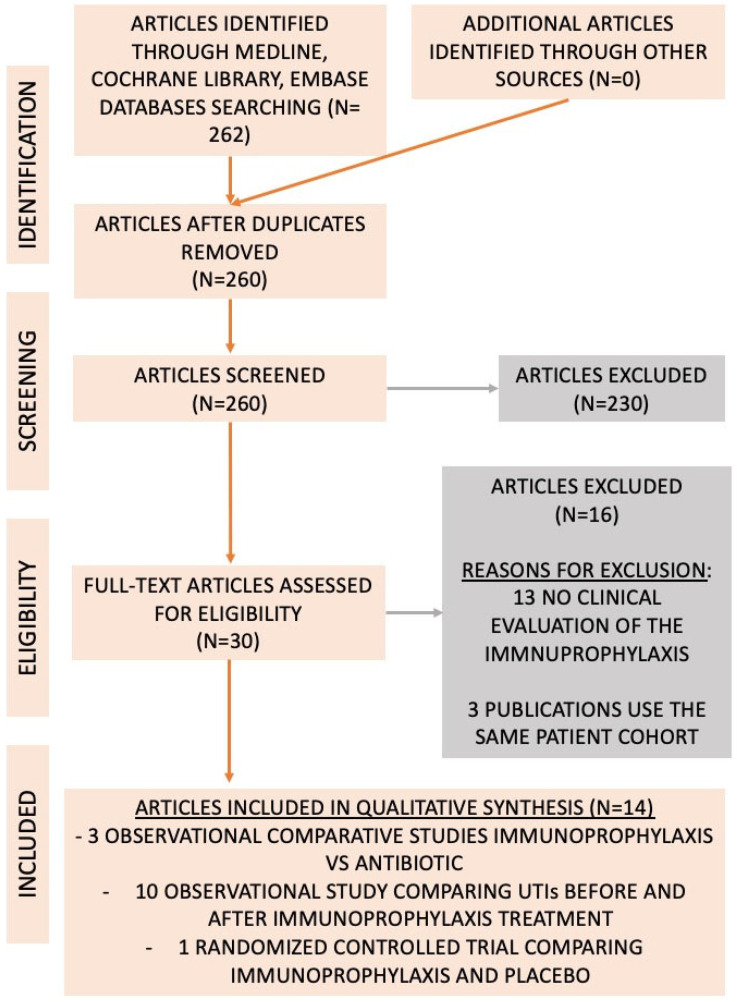 Figure 1
Figure 1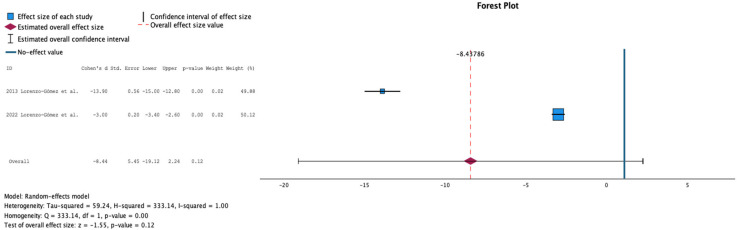 Figure 2
Figure 2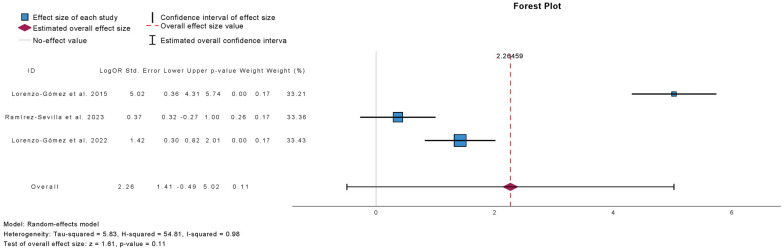 Figure 3
Figure 3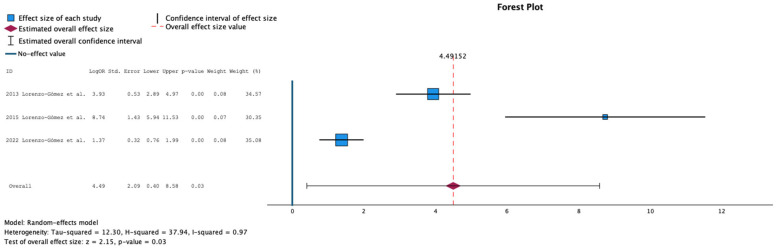 Figure 4
Figure 4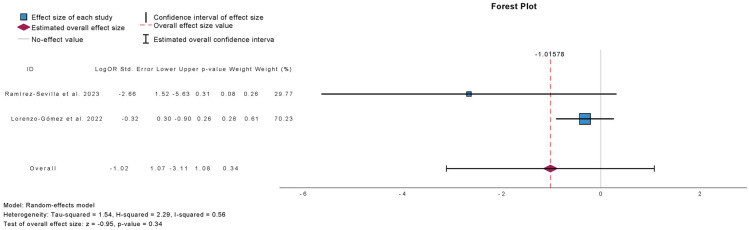 Figure 5
Figure 5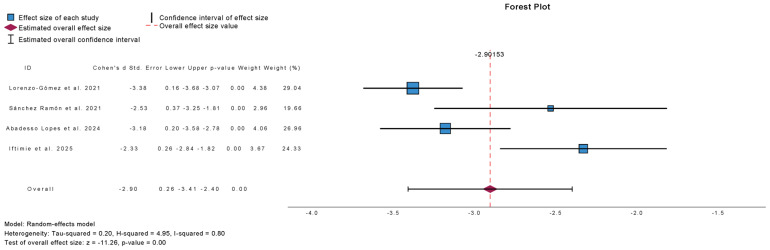 Figure 6
Figure 6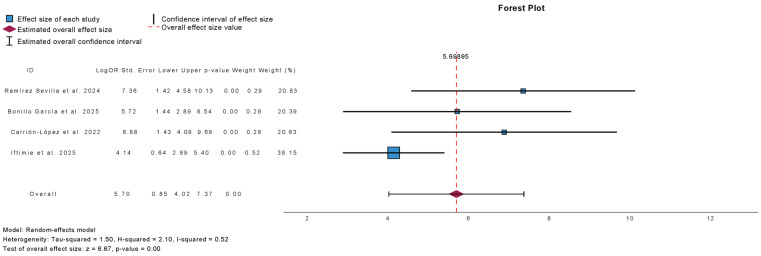 Figure 7
Figure 7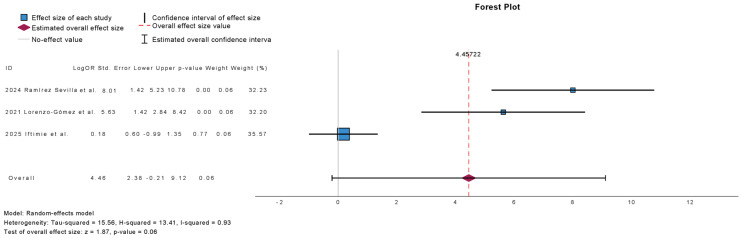 Figure 8
Figure 8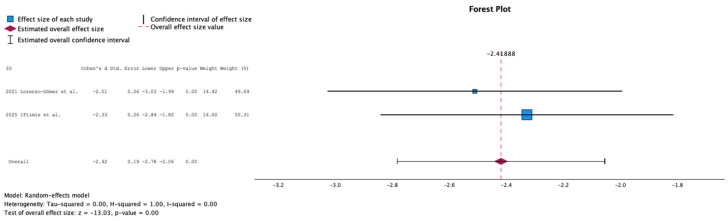 Figure 9
Figure 9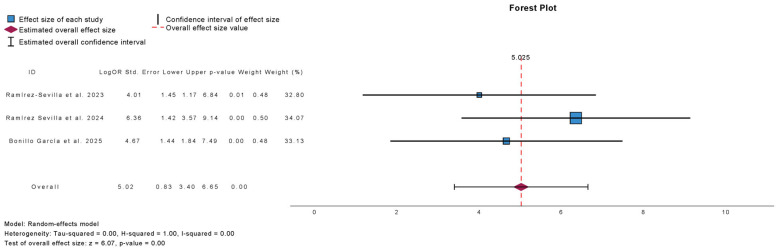 Figure 10
Figure 10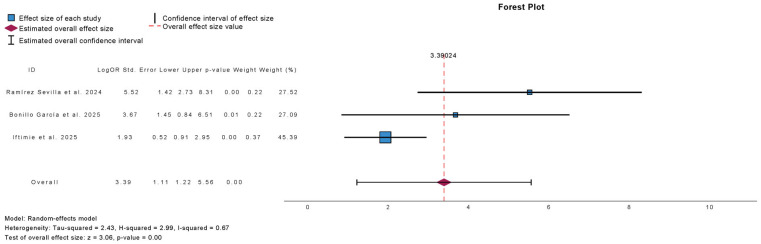 Figure 11
Figure 11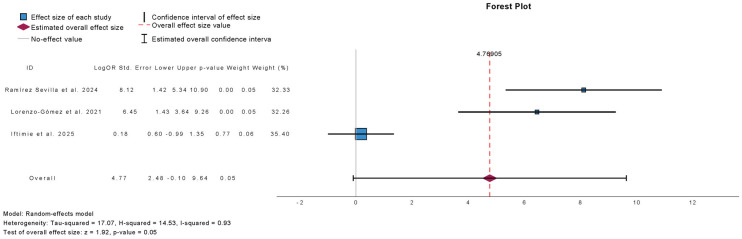 Figure 12
Figure 12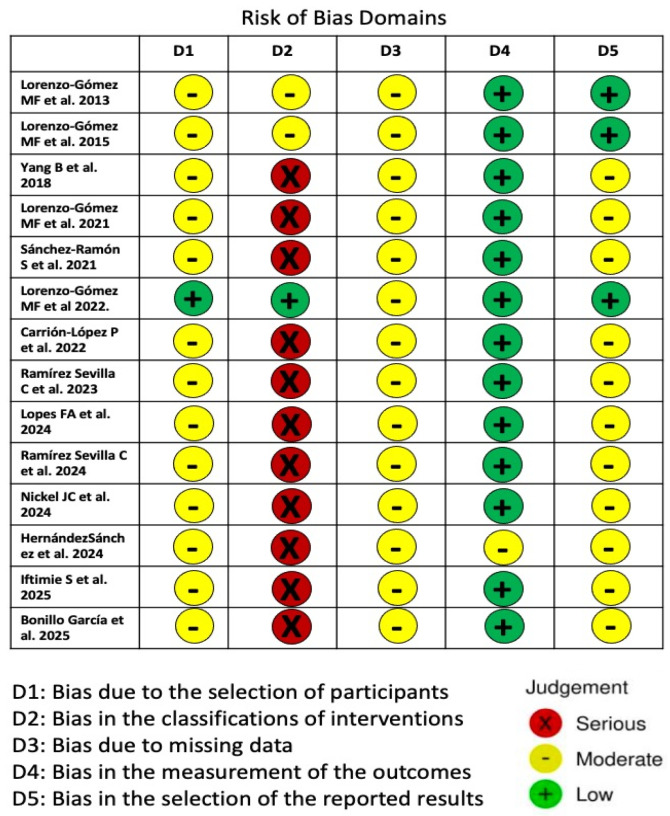 Figure 13
Figure 13Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pediatric Urology and Nephrology Studies · Bladder and Urothelial Cancer Treatments
1. Introduction
Recurrent urinary tract infections (rUTIs) are defined as at least three episodes of cystitis per year or two episodes of cystitis in six months [1]. It is estimated that up to 3% of women experience rUTIs [1]. rUTIs negatively affect patients’ quality of life, leading to a reduction in social and sexual relationships, diminished self-esteem, and impaired work capacity [2]. Prevention of rUTIs includes counseling on risk factor avoidance, non-antimicrobial strategies, and antimicrobial prophylaxis. Non-antibiotic preventive measures are recommended over antibiotic therapy to avoid antimicrobial resistance and other adverse effects associated with antibiotic use. Immunoprophylaxis using whole bacteria or bacterial components is an alternative strategy for preventing rUTIs [1]. Several immunoprophylactic approaches have been developed to stimulate the immune system via dendritic cells and T-cell-mediated cytokine production [3,4,5,6]. Formulations include oral, sublingual, intramuscular, and intravaginal preparations (StroVac, OM-89, ExPEC4V, MV140, and Solco-Urovac). Previous systematic reviews have evaluated these different agents [7,8]. The composition and mechanism of action of individual immunomodulatory agents are sufficiently different such that pooled analyses of results from these disparate trials are unlikely to provide robust conclusions. Therefore, each preparation should be reviewed separately [8]. Recently, interest in sublingual inactivated whole bacteria for rUTI prevention has increased, particularly with the MV140 formulation. MV140 (Uromune, Q Pharma/Inmunotek S.L.) is a glycerinated suspension of whole-cell, heat-inactivated bacteria [8,9]. The original formula consists of equal amounts of four common UTI-causing microorganisms: Escherichia coli, Klebsiella pneumoniae, Proteus vulgaris, and Enterococcus faecalis. Since 2017, the only approved formulation available in Spain has been the autovaccine. Autovaccination consists of heat-inactivated whole bacteria tailored to a patient’s urine culture results. Both immunoprophylactic preparations are administered sublingually as two daily puffs of 100 μL each (108 bacteria/puff), with no concomitant food or beverage intake [10].
The aim of this systematic review and meta-analysis was to evaluate the current evidence on the effectiveness and safety of immunoprophylaxis using sublingual inactivated whole bacteria (MV140 and autovaccination) to prevent rUTIs. The main outcomes were UTI incidence at 12 months and the proportion of patients who remained UTI-free.
2. Results
The literature search identified 262 studies evaluating the use of sublingual immunoprophylaxis with inactivated whole bacteria to manage rUTIs. Of these, 232 were excluded because they did not assess sublingual immunoprophylaxis with heat-inactivated whole bacteria. A total of 30 full-text articles were reviewed for eligibility, and 14 studies were included (4 comparative and 10 observational studies) [10,11,12,13,14,15,16,17,18,19,20,21,22,23]. Details of the literature search and reasons for exclusion are summarized in Figure 1.
2.1. Comparative Studies
Four comparative studies were included. Three were observational studies using antibiotic prophylaxis as the control [11,12,18], and one was an RCT comparing the MV140 formulation with placebo [16]. The number of patients in the treatment arms ranged from 139 to 360. Study characteristics are summarized in Table 1. Across these studies, the mean annual incidence of UTIs decreased from 3.2–6 episodes at baseline to 0–1.35 episodes at 12 months in patients receiving immunoprophylaxis [11,12,16]. The proportion of patients who remained UTI-free at 12 months was 56–90% in the immunoprophylaxis group, 0–2.5% in those managed with low-dose antibiotics, and 25% in those managed with a placebo. The RCT reported adverse events in 40.8% of patients receiving immunoprophylaxis and 50% receiving placebo (205 adverse reactions in 101 patients) [11,12,16,18]. The most common adverse events were chest infections (2.6%), candidiasis (2.6%), and vaginitis (2.0%). A total of 5 of 152 patients (3.2%) reported serious adverse events unrelated to immunoprophylaxis [16]. A total of 9 of the 101 adverse events were considered adverse reactions related to the study intervention (2 in the placebo group and 3 in MV140). The number of patients who withdrew from the study due to adverse events was 2 (2.5%) in the placebo group and 5 (6.2%) in the MV140-treated group [24]. Several studies also reported reduced isolation of non-Escherichia coli pathogens, lower antimicrobial resistance rates, and improved quality of life with immunoprophylaxis [11,12,16]. In the study by Lorenzo et al., Klebsiella spp. isolation was 12% in the antibiotic prophylaxis group and 0% in the immunoprophylaxis group. Furthermore, the percentage of bacteria resistant to different antibiotics was 31% and 45% in those receiving immunoprophylaxis and antibiotic prophylaxis, respectively [12]. The main findings from comparative studies are summarized in Table 2.
2.2. Observational Studies
Ten observational studies were included, all comparing UTI incidence before and after immunoprophylaxis [10,13,14,15,17,19,20,21,22,23]. Although both men and women were studied, women accounted for more than 65% of cases overall. In the study by Bonillo-García et al., which focused on patients with neurogenic bladder, men comprised 68% of the cohort [23]. Treatments included both the MV140 formulation (1228 cases) and autovaccination (1367 cases). Study characteristics are summarized in Table 3. The mean annual UTI incidence decreased from 3.7–6.8 episodes at baseline to 0.2–1.58 episodes after 12 months of immunoprophylaxis [14,15,17,19,20,22]. Reported UTI reduction at 12 months ranged from 9.8% to 78%, and the proportion of patients experiencing ≥3 UTIs at follow-up ranged from 14.3% to 57.6% [10,13,14,17,19,20,22,23]. Adverse events occurred in 0–14% of patients and were generally mild. Adverse effects include skin rash, mucosal burning, upper gastrointestinal discomfort, and fatigue [10,13,14,15,17,19,20,22]. Several studies also reported reduced healthcare costs and improved patient quality of life with immunoprophylaxis [17,20,21]. The main findings from observational studies are summarized in Table 4.
Autovaccines were evaluated explicitly in six studies (1493 patients) [10,14,18,21,22,23]. Characteristics are summarized in Table 5. The mean annual incidence of UTIs decreased from 3.7–5 episodes at baseline to 0.3–0.98 episodes at 12 months [14,22]. At 12-month follow-up, UTI-free rates ranged from 10 to 49% for autovaccines and 9.7 to 60% for MV140, while the proportion of patients with ≥3 UTIs ranged from 14.3 to 60.2% for autovaccines and 20 to 56.1% for MV140 [10,14,22]. Reported adverse events with autovaccination were rare (0–1.3%) and mild [10,15,18,22]. In patients with neurogenic bladders, Bonillo-García et al. reported improved quality of life following autologous vaccine therapy [23]. The main findings from autovaccine studies are summarized in Table 6.
2.3. Metanalysis
Figure 2 shows the meta-analysis comparing placebo or antibiotic prophylaxis with sublingual immunoprophylaxis using the MV140 formulation for the outcome of UTI incidence. Two studies were included, comprising 160 patients in the antibiotic group, 76 in the placebo group, and 298 in the immunoprophylaxis group. No significant reduction in UTI incidence was observed with immunoprophylaxis compared with controls (mean difference: −8.44; 95% CI: −19.12 to 2.24; p = 0.12). Statistical heterogeneity was high (Q = 333.14, p < 0.001; τ^2^ = 52.24; H^2^ = 333.14; I^2^ = 99%), indicating considerable variability between studies.
Figure 3 presents the meta-analysis comparing placebo or antibiotic prophylaxis with sublingual immunoprophylaxis using the MV140 formulation for the outcome of UTI-free prevalence at 6 months. Three studies were included, comprising 465 patients in the antibiotic group, 76 in the placebo group, and 750 in the immunoprophylaxis group. Immunoprophylaxis did not significantly increase the proportion of UTI-free patients at 6 months compared with controls (mean difference: 2.27; 95% CI: −0.49 to 5.02; p = 0.11). Heterogeneity was substantial (τ^2^ = 5.83; H^2^ = 54.81; I^2^ = 98%), reflecting considerable variability across studies.
Figure 4 summarizes the meta-analysis comparing placebo or antibiotic prophylaxis with sublingual immunoprophylaxis using the MV140 formulation for the outcome of UTI-free prevalence at 12-month follow-up. Three studies were included, comprising 499 patients in the antibiotic group, 76 in the placebo group, and 558 in the immunoprophylaxis group. Immunoprophylaxis was associated with a significantly higher proportion of UTI-free patients at 12 months compared with controls (mean difference: 4.49; 95% CI: 0.40 to 8.58; p = 0.03). Heterogeneity was substantial (τ^2^ = 12.30; H^2^ = 34.94; I^2^ = 97%), indicating considerable variability across studies.
Figure 5 presents the meta-analysis comparing placebo or antibiotic prophylaxis with sublingual immunoprophylaxis using the MV140 formulation for the outcome of side-effect prevalence. Two studies were included, comprising 126 patients in the antibiotic group, 76 in the placebo group, and 390 in the immunoprophylaxis group. There was no significant difference in the prevalence of side effects between immunoprophylaxis and control groups (mean difference: −1.02; 95% CI: −3.11 to 1.08; p = 0.34). Heterogeneity was low (τ^2^ = 1.54; H^2^ = 2.29; I^2^ = 56%), indicating modest variability across studies.
Figure 6 summarizes the meta-analysis of UTI incidence at 12-month follow-up in studies comparing outcomes before and after treatment with sublingual immunoprophylaxis. Four studies were included, comprising 384 patients. Immunoprophylaxis was associated with a significant reduction in UTI incidence at 12 months (mean difference: −2.91; 95% CI: −3.41 to −2.40; p < 0.01). Heterogeneity was substantial (τ^2^ = 0.20; H^2^ = 4.95; I^2^ = 80%), reflecting moderate variability across studies.
Figure 7 presents the meta-analysis of UTI-free prevalence at 3-month follow-up in studies comparing outcomes before and after treatment with sublingual immunoprophylaxis. Four studies were included, comprising 1389 patients. Immunoprophylaxis was associated with a significant increase in the proportion of UTI-free patients at 3 months (mean difference: 5.70; 95% CI: 4.02 to 7.37; p < 0.01). Heterogeneity was moderate (τ^2^ = 1.50; H^2^ = 2.10; I^2^ = 52%), indicating some variability across studies.
Figure 8 summarizes the meta-analysis of the prevalence of patients experiencing more than three UTIs at 12-month follow-up in studies comparing outcomes before and after treatment with sublingual immunoprophylaxis. Three studies were included, comprising 1353 patients. There was no statistically significant difference in the prevalence of patients with more than three UTIs at 12 months (mean difference: 4.46; 95% CI: −0.21 to 9.12; p = 0.06). Heterogeneity was high (τ^2^ = 15.56; H^2^ = 13.41; I^2^ = 93%), indicating considerable variability across studies.
Figure 9 summarizes the meta-analysis of UTI incidence at 12-month follow-up in studies evaluating autovaccine. Two studies were included, comprising 109 patients. Autovaccine treatment was associated with a significant reduction in UTI incidence at 12 months (mean difference: −2.42; 95% CI: −2.78 to −2.06; p < 0.01).
Figure 10 summarizes the meta-analysis of UTI-free prevalence at 6-month follow-up in studies evaluating autovaccine. Three studies were included, comprising 652 patients. Autovaccine treatment was associated with a significant increase in the proportion of UTI-free patients at 6 months (mean difference: 5.03; 95% CI: 3.40 to 6.65; p < 0.01).
Figure 11 summarizes the meta-analysis of UTI-free prevalence at 12-month follow-up in studies evaluating autovaccine. Three studies were included, comprising 575 patients. Autovaccine treatment was associated with a significant increase in the proportion of UTI-free patients at 12 months (mean difference: 3.39; 95% CI: 1.22 to 5.56; p < 0.01). Heterogeneity was moderate (τ^2^ = 2.43; H^2^ = 2.99; I^2^ = 67%).
Figure 12 summarizes the meta-analysis of the prevalence of patients with more than three UTIs at 12-month follow-up in studies evaluating autovaccine. Three studies were included, comprising 565 patients. Autovaccine treatment was associated with a borderline significant reduction in the prevalence of patients with >3 UTIs at 12 months (mean difference: 4.82; 95% CI: −0.10 to 9.64; p = 0.05). Heterogeneity was high (τ^2^ = 17.07; H^2^ = 14.53; I^2^ = 93%).
2.4. Risk of Bias Assessment
Patient selection and classification represented potential sources of bias in the included studies. Most studies assessed the efficacy of immunoprophylaxis using a pre- and post-treatment comparison. In the comparative studies, the criteria for treatment allocation were often unclear, as decisions were based on physician judgment, which may have influenced outcomes [24,25]. Only the randomized controlled trial, including 240 participants, had a low risk of bias regarding patient classification [16]. All studies had a low to moderate risk of bias concerning selective outcome reporting. A summary of the risk of bias for the included studies is presented in Figure 13.
2.5. Evidence Synthesis
This review evaluates the efficacy and safety of immunoprophylaxis with sublingual, inactivated whole bacteria for the prevention of rUTIs, including fourteen studies with a total of 3504 patients receiving immunoprophylaxis. Two formulations were evaluated: MV140, which consists of Escherichia coli, Klebsiella pneumoniae, Proteus vulgaris, and Enterococcus faecalis**,** and an autovaccine, prepared based on individual urine culture results. The autovaccine was evaluated in 1453 patients. Most studies assessed efficacy at 12 months of follow-up. Although UTIs frequently occurred in the follow-up, immunoprophylaxis was associated with a reduction in UTI incidence, ranging from 10% to 80% at 12 months. Ramírez-Sevilla et al. reported that patients with more than five UTIs per year had a higher incidence of infections and recommended extending immunoprophylaxis by an additional three months [8,18]. Comparative efficacy between MV140 and autovaccine has also been evaluated. Both formulations demonstrated efficacy from 3 to 12 months post-treatment. Published results suggest that MV140 may achieve higher proportions of UTI-free patients at 12-month follow-up (9.7–60% for MV140 vs. 10–49% for the autovaccine) [10,14,22]. Similarly, the proportion of patients experiencing more than three UTIs at 12 months ranged from 20% to 56% for MV140 and 14% to 90% for autovaccine [10,14,22]. Reported side effects were mostly mild and local, with the autovaccine associated with slightly fewer adverse events [10,18,26].
3. Discussion
The systematic review of the evidence indicates that prevention of rUTIs with sublingual formulations of inactivated whole bacteria or autovaccines appears to be a promising strategy with high efficacy, which could avoid low-dose prophylaxis. Non-antibiotic treatment should be considered first-line management for the prevention of rUTIs [1,27,28]. Two prior systematic reviews have assessed the effect of immunoprophylaxis in patients with rUTIs. However, the analysis was conducted using different types of preparations. Different administration routes, mechanisms of action, and dosages may influence clinical outcomes [16,29,30,31]. In the meta-analysis by Mak et al., 16 studies were evaluated, 4 of which used the MV140 formula. Similarly, in the meta-analysis by Pratley et al., 3 of 17 studies reported outcomes using MV140 [7,8]. The present systematic review included 14 studies involving 3504 patients. Moreover, many studies assessing the efficacy of immunoprophylaxis had short follow-up periods and were predominantly conducted using female populations [7].
The focus of this systematic review was to analyze the efficacy of sublingual dead whole-bacteria formulations in preventing rUTIs, including the MV140 formula (Escherichia coli, Klebsiella pneumoniae, Proteus vulgaris, and Enterococcus faecalis) and autovaccines. The proposed mechanism of action involves modulation of the innate and adaptive immune response via dendritic cells in the sublingual epithelium. Activation of these dendritic cells induces a T-lymphocyte-mediated response, producing Th1, Th17, and IL-10 cytokines. Sublingual administration avoids intestinal metabolism, and multiple studies in both animal models and humans have demonstrated effective immune activation [3,4,5,6,32].
Most evidence on the efficacy of sublingual immunoprophylaxis is derived from studies comparing UTI incidence before and after treatment. Across more than 3000 patients, reductions in UTI incidence were observed at 12-month follow-up [10,12,14,17,22,23,24]. Although the incidence of urinary tract infections (UTIs) has decreased, it should be noted that UTIs may still occur after treatment. Studies by Lorenzo-Gómez et al. reported that the proportion of patients remaining UTI-free at 12 months ranged from 56% to 90% in the immunoprophylaxis group, compared with 0–2.5% in the low-dose antibiotic group; these data are derived from observational studies [11,12,14]. The Cochrane review on the efficacy of low-dose prophylaxis for recurrent UTIs reported recurrence rates of 0 to 0.9 episodes per patient-year during antibiotic prophylaxis. After discontinuation of prophylaxis, recurrence rates based on microbiological criteria were 1.2 episodes per patient-year in patients receiving nitrofurantoin and 1.3 episodes per patient-year in those receiving cotrimoxazole [33]. Data from an RCT reported a 12-month follow-up prevalence of UTI-free patients of 56% for the MV140 formulation and 25% in the placebo group [16]. These findings are concordant with other studies evaluating alternative strategies for the management of rUTIs, such as the ALTAR study assessing the use of methenamine hippurate [34].
The design of most studies carries a risk of reporting bias, as they lacked a comparator group or were retrospective [9,10]. In some studies, treatment choice was left to the clinician’s discretion, introducing potential group heterogeneity. Studies comparing UTI rates before and after immunoprophylaxis may also be prone to bias owing to improvements attributable to factors such as spontaneous changes in risk factors over time and behavioral modifications (e.g., hydration and sexual activity). Publication bias may also be present, with a tendency for studies showing positive results to be published preferentially. However, although much of the research has been conducted by a limited number of authors, the data have been followed prospectively and results updated periodically in some series [10,15,18,26]. Finally, the definition of UTI used in these studies generally required the presence of symptoms and a positive urine culture using a threshold of >10^5^ CFU/mL. However, in some studies, the threshold was not specified. In patients with typical UTI symptoms, or in those with urinary catheters, a lower threshold of ≥10^3^ CFU/mL may also be acceptable [1].
Sublingual immunoprophylaxis was predominantly evaluated in women, with only 185 men included in the studies [14,18,19,22,23]. A substantial proportion of participants were postmenopausal women, 1738 out of 2601 (66.8%). Hormonal status influenced outcomes: premenopausal women had higher UTI-free rates (14/22, 63.6%) compared to postmenopausal women (13/42, 33.3%; p = 0.012) [20]. Conversely, Ramírez et al. reported that postmenopausal women experienced a greater reduction in UTI episodes than premenopausal women (74.7% vs. 59.4%, p = 0.029) [19]. Lorenzo-Gómez et al. reported efficacy in older patients with both MV140 and autovaccine formulations, with enhanced outcomes following booster doses. No significant sex differences were observed, although both formulations appeared more effective in females [14]. Sub-analyses indicated comparable efficacy among smokers and patients with metabolic syndrome, while risk factors for UTIs included urostomy, chronic kidney disease, and immunosuppression [22,35].
Two different immunoprophylaxis approaches using sublingual administration of whole inactivated bacteria were analyzed: the standardized MV140 formulation and tailored autovaccines derived from the patient’s urine culture. The individual analysis of both formulations was evaluated in the research conducted by Ramírez et al. [10,18]. Among patients receiving MV140, reported efficacy rates were 95.8%, 88.4%, and 56.1% at 3, 6, and 12 months of follow-up, respectively. In patients treated with autovaccines, efficacy rates were 85.7%, 73.6%, and 60.2% at the same follow-up intervals. Moreover, the same research group reported that patients presenting with five or more UTIs experienced lower efficacy (80.2%, 64.3%, and 40%) compared to those with fewer than five UTIs (97.7%, 91.1%, and 64.7%) at 3, 6, and 12 months of follow-up (n = 611 with 12-month follow-up) [10]. Therefore, patients must be informed about the risk of recurrence. The one-year recurrence rates were 79.2% and 94.9% in patients with fewer than five and more than five UTIs prior to treatment, respectively. The authors recommended that immunoprophylaxis be maintained for more than three months in patients with more than five UTIs per year [10].
Quality of life (QoL) outcomes improved significantly. At 12 months, 80.3% of patients reported moderate or marked improvement, 58.1% were satisfied or delighted, and mean QoL scores increased by 1.5 points (21). Bonillo-Garcia et al. reported that neurological patients indicated “Improved greatly” (30.4%) or “Improved” (43.5%), with only 2.9% reporting deterioration [23].
Economic analyses suggest that sublingual immunoprophylaxis may be more cost-effective than both antibiotic and non-antibiotic adjuvant measures at reducing emergency visits, follow-up appointments, infection recurrence, and diagnostic testing [17,21].
Most studies reported an adverse event rate of less than 5%, with the majority of events being mild and including skin rash, mucosal irritation, gastrointestinal discomfort, and fatigue [14,17,19,20]. For example, Ramírez-Sevilla et al. reported side effects in 1.36% of 1104 patients, consisting of dry mouth, gastritis, and mild nausea. No adverse events were reported in patients treated with autovaccines [10]. However, it should be noted that the randomized controlled trial reported a higher rate of adverse effects—40.8% in the immunoprophylaxis group and 50% in the control group. However, the percentages of patients who withdrew from the study due to adverse effects were 2.5% and 6.2% in the placebo and MV240 groups, respectively. The study design permitted systematic assessment of all symptoms and signs during follow-up. Nevertheless, the authors stated that most adverse events were not treatment-related, as reflected in the high prevalence of side effects in the placebo group [16,24]. The study by Bauer et al., which compared immunotherapy using OM-89 with placebo, reported an even higher incidence of adverse events, with 13% considered treatment-related [29]. The Cochrane review by Albert et al. reported that up to 20% of patients required withdrawal, and some studies reported a prevalence of 28% adverse effects in the placebo group and up to 10% severe adverse effects [34]. Therefore, future studies are needed to more accurately determine the adverse effects directly attributable to sublingual immunoprophylaxis.
The strength of this review lies in its focus on one type of immunoprophylaxis—sublingual whole-bacteria formulations—and in its analysis of both MV140 and autovaccine formulations with independently reported outcomes. The main limitation is the risk of bias in the included studies, as only one was a randomized controlled trial; most studies compared UTI incidence before and after treatment. Observed improvements may be influenced by changes in risk factors or concomitant measures. Furthermore, in observational comparative studies with low-dose antibiotics, treatment allocation often depended on physician recommendation, potentially limiting comparability between groups. Moderate heterogeneity was observed among studies. A longer follow-up is recommended, as UTIs frequently recur during this period. Adverse events should be reported systematically, as reported rates varied considerably, with the highest percentage observed in the RCT. Robust randomized controlled trials are necessary to provide firm recommendations regarding immunoprophylaxis with oral formulations of inactivated whole bacteria for rUTI prevention. Following this route, a multicenter double-blind randomized controlled trial evaluating MV140 was recently published as a protocol [25].
4. Materials and Methods
4.1. Definitions Used
A comprehensive literature review was conducted. PubMed, Cochrane CENTRAL, and Embase libraries were searched with the terms ‘‘recurrent urinary tract infections’’ and ‘‘Uromune’’ or ‘‘MV140’’ or ‘‘sublingual vaccine’’ or “whole cell” or “bacterial vaccine”. References of the included studies and previous reviews were also examined to identify additional relevant studies.
4.2. Study Variables and Outcomes
The primary aim of this study was to evaluate the effectiveness of sublingual immunoprophylaxis with inactivated whole bacteria (MV140 formula and autovaccine) for the prevention of rUTIs. Effectiveness was assessed using the following criteria:
- The number of UTIs experienced during follow-up.
- The proportion of patients remaining UTI-free during follow-up.
- Comparisons were made against no treatment or prophylaxis with low-dose antibiotics.
Secondary outcomes included the following for patients receiving sublingual immunoprophylaxis, placebo, or low-dose antibiotic prophylaxis:
- The proportion of patients experiencing fewer than three UTIs during follow-up;
- Infection-free interval;
- Microbiological patterns, including rates of multidrug-resistant organisms (MDROs);
- Quality of life;
- Adverse events;
- Comparative efficacy between MV140 and autovaccine.
The systematic review was preregistered at PROSPERO. The detailed review protocol can be viewed under CRD number 420251003894 at https://www.crd.york.ac.uk/PROSPERO/view/CRD420251003894 (accessed on 4 May 2025).
4.3. Literature Search
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Materials) [36,37]. The following PICO question was formulated: Patients (adult patients with recurrent urinary tract infections), Intervention (treatment using sublingual immunoprophylaxis with whole bacteria inactivated via heat), Control (prophylaxis using a low dose of antibiotics, placebo, or number of infections before treatment using sublingual immunoprophylaxis with whole bacteria inactivated via heat), Outcome (rates of urinary tract infections, time free of infections, microbiological patterns, quality of life assessment, and side effects).
Search Strategy: Eligible studies were English-language manuscripts that addressed the prevention and management of rUTIs using sublingual dead whole bacteria treatment. The inclusion criteria were adult patients (older than 16 years old), including males and females, and studies evaluating the effect of sublingual immunoprophylaxis for rUTI prevention.
4.4. Eligibility of Studies
Eligible study designs included randomized controlled trials (RCTs), non-randomized controlled trials (non-RCTs), observational studies (prospective or retrospective), cross-sectional studies, case–control studies, and single-arm studies with ≥25 patients. When multiple publications evaluated the same cohort, the larger or more comprehensive study was included. Excluded studies comprised case reports, expert opinions, commentaries, editorials, and conference abstracts. Only studies documenting the effectiveness and safety of sublingual inactivated whole-bacteria immunoprophylaxis for rUTI prevention were included.
4.5. Selection of Studies and Data Extraction
Data extraction (selection and coding)
Study selection: Studies were selected in a two-step process. Titles and abstracts were first screened against the predefined inclusion criteria. Second, the full texts of potentially eligible studies were assessed for eligibility using the same criteria. Two authors independently screened and selected the studies.
Data extraction: Data extraction was undertaken by one author. The extracted data were checked by a second author. Any discrepancies were resolved through discussion.
Extracted data included the following:
- Study characteristics (design, objective, sample size, follow-up duration, publication year, and statistical methods).
- Type of immunoprophylaxis with sublingual dead whole bacteria: MV140 formula or autovaccine.
- Definition of rUTIs.
- Definition of UTI episode.
- Treatment indicated (duration and dose).
- Incidence of UTIs.
- No UTIs during follow-up.
- Prevalence of more than three UTIs during follow-up.
- Time free of UTIs.
- Microorganism patterns, including the rate of MDRO.
- Quality of life evaluation.
- Adverse effects.
4.6. Risk of Bias Assessment
Risk of bias was assessed using the Cochrane Risk of Bias tool for RCTs, considering the following domains: selection bias, performance bias, classification of interventions, missing data, outcome measurement, and reporting bias. For non-randomized studies, the ROBINS-I tool (Risk Of Bias in Non-randomized Studies of Interventions) was employed.
4.7. Meta-Analysis
A meta-analysis was performed using a random-effects model. Between-study heterogeneity was assessed visually using forest plots and quantified using the I^2^ statistic (95% CI) and the Chi-square test for heterogeneity. The analysis included the estimated average log odds ratios based on the random-effects model and the Q-test for heterogeneity. All analyses were conducted using SPSS Statistics for Mac, version 29.0.2.0 (IBM Corporation).
5. Conclusions
Although the quality of evidence regarding the efficacy of whole inactivated bacteria immunoprophylaxis for the prevention of rUTIs is limited, current data indicate that it may confer a beneficial effect. This systematic review suggests that MV140 and autovaccine formulations, administered sublingually as whole inactivated bacteria, represent safe and effective non-antibiotic alternatives for reducing UTI frequency and prolonging UTI-free intervals in women with recurrent urinary tract infections. Nonetheless, well-designed prospective randomized controlled trials are required to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bonkat G. Kranz J. Cai T. Geerlings S.E. Köves B. Pilatz A. Medina-Polo J. Schneidewind L. Schubert S. Veeratterapillay R. EAU Guidelines on Urological Infections European Association of Urology Arnhem, The Netherlands 2025978-94-92671-29-5Available online: https://uroweb.org/guidelines/urological-infections(accessed on 10 December 2025)
- 2Medina-Polo J. Arrébola-Pajares A. Corrales-Riveros J.G. Alidjanov J.F. Lorenzo-Gómez M.F. Tapia A.-M.H. Martínez-Berganza M.L. Ospina-Galeano I.A. Padilla-Fernández B. Pilatz A. Validation of the Spanish Acute Cystitis Symptoms Score (ACSS) in Native Spanish-Speaking Women of Europe and Latin America Neurourol. Urodyn.20234226328110.1002/nau.2507936335613 PMC 10098495 · doi ↗ · pubmed ↗
- 3Saz-Leal P. Ligon M.M. Diez-Rivero C.M. García-Ayuso D. Mohanty S. Viñuela M. Real-Arévalo I. Conejero L. Brauner A. Subiza J.L. MV 140 Mucosal Vaccine Induces Targeted Immune Response for Enhanced Clearance of Uropathogenic E. Coli in Experimental Urinary Tract Infection Vaccines 20241253510.3390/vaccines 1205053538793786 PMC 11126127 · doi ↗ · pubmed ↗
- 4Martin-Cruz L. Sevilla-Ortega C. Benito-Villalvilla C. Diez-Rivero C.M. Sanchez-Ramón S. Subiza J.L. Palomares O. A Combination of Polybacterial MV 140 and Candida Albicans V 132 as a Potential Novel Trained Immunity-Based Vaccine for Genitourinary Tract Infections Front. Immunol.20201161226910.3389/fimmu.2020.61226933552074 PMC 7858650 · doi ↗ · pubmed ↗
- 5Martín-Cruz L. Angelina A. Baydemir I. BulutÖ. Subiza J.L. Netea M.G. Domínguez-Andrés J. Palomares O. Candida Albicans V 132 Induces Trained Immunity and Enhances the Responses Triggered by the Polybacterial Vaccine MV 140 for Genitourinary Tract Infections Front. Immunol.202213106638310.3389/fimmu.2022.106638336505433 PMC 9729253 · doi ↗ · pubmed ↗
- 6Benito-Villalvilla C. Cirauqui C. Diez-Rivero C.M. Casanovas M. Subiza J.L. Palomares O. MV 140, a Sublingual Polyvalent Bacterial Preparation to Treat Recurrent Urinary Tract Infections, Licenses Human Dendritic Cells for Generating Th 1, Th 17, and IL-10 Responses via Syk and My D 88Mucosal Immunol.20171092493510.1038/mi.2016.11227966556 · doi ↗ · pubmed ↗
- 7Mak Q. Greig J. Dasgupta P. Malde S. Raison N. Bacterial Vaccines for the Management of Recurrent Urinary Tract Infections: A Systematic Review and Meta-Analysis Eur. Urol. Focus 20241076176910.1016/j.euf.2024.04.00238644097 · doi ↗ · pubmed ↗
- 8Prattley S. Geraghty R. Moore M. Somani B.K. Role of Vaccines for Recurrent Urinary Tract Infections: A Systematic Review Eur. Urol. Focus 2020659360410.1016/j.euf.2019.11.00231806578 · doi ↗ · pubmed ↗