Overcoming Opacity: The Role of Intraoperative OCT in Complex Corneal and Anterior Segment Surgery
Natalie di Geronimo, Antonio Moramarco, Vito Romano, Maurizio Mete, Luigi Fontana

TL;DR
Intraoperative OCT helps surgeons perform complex eye surgeries more safely and accurately by providing real-time imaging through cloudy or damaged corneas.
Contribution
This review highlights the novel application of intraoperative OCT in various anterior segment surgeries with limited visibility.
Findings
iOCT improves precision in endothelial keratoplasty by confirming graft orientation and interface fluid resolution.
In DALK, iOCT aids in cannula placement and stromal depth assessment.
iOCT enhances safety during hydrops management and traumatic corneal injury repair.
Abstract
Intraoperative optical coherence tomography (iOCT) has emerged as a pivotal technology in anterior segment surgery, particularly in cases limited by corneal opacity, edema, or altered anatomy. By providing real-time, cross-sectional imaging, iOCT enables surgeons to visualize otherwise hidden structures and to perform critical intraocular maneuvers with greater precision and safety. Its integration into the surgical microscope allows continuous monitoring of tissue–instrument interaction, transforming traditionally “blind” procedures into image-guided interventions. This review highlights the role of iOCT in endothelial keratoplasty, deep anterior lamellar keratoplasty (DALK), management of acute corneal hydrops, synechiolysis, glaucoma drainage device implantation, and ocular trauma. In endothelial procedures, iOCT helps confirm Descemet membrane removal, graft orientation, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
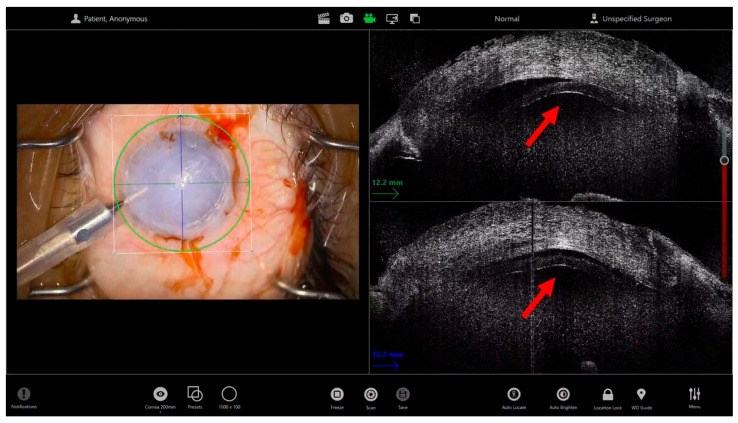 Figure 1
Figure 1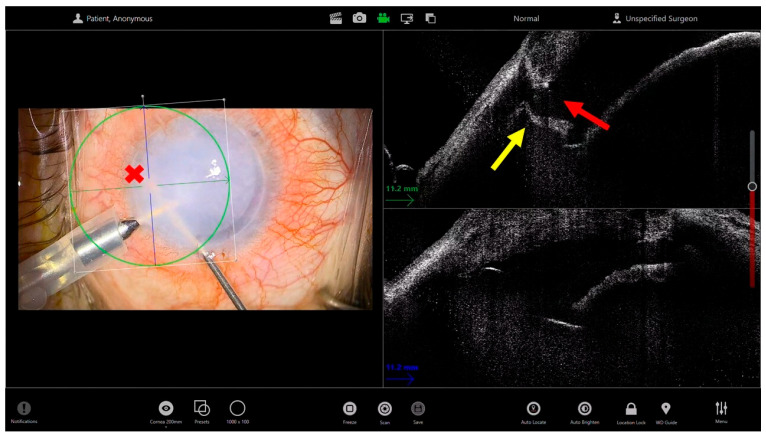 Figure 2
Figure 2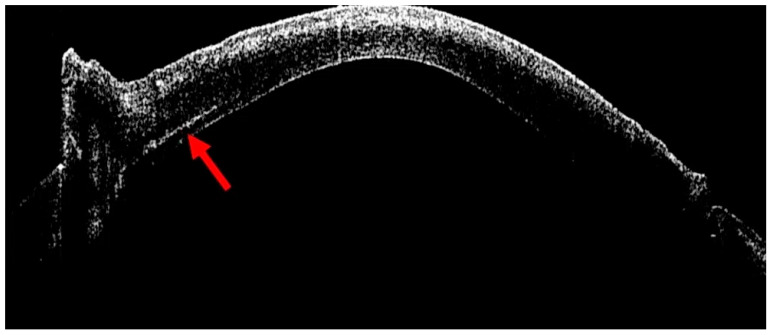 Figure 3
Figure 3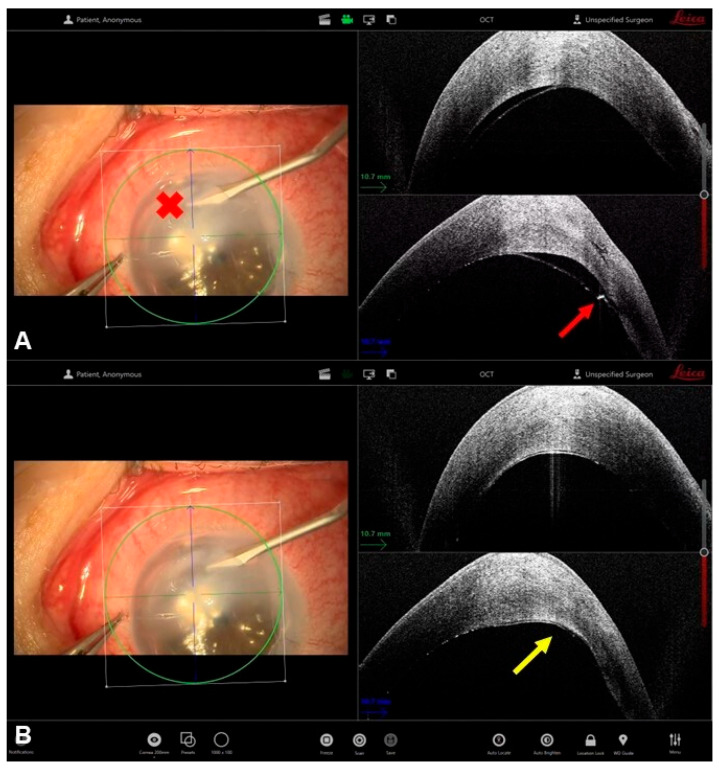 Figure 4
Figure 4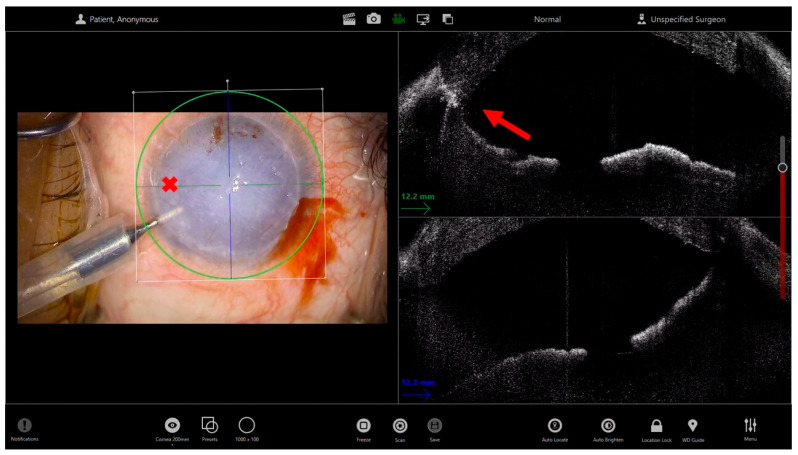 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal surgery and disorders · Intraocular Surgery and Lenses · Retinal and Macular Surgery
1. Introduction
Anterior segment optical coherence tomography (AS-OCT) was first described in 1994 by Izatt et al. [1] as a key imaging tool for the diagnosis and follow-up of corneal and anterior segment disorders. Thanks to its high resolution, AS-OCT provides near-histologic cross-sectional images that support clinical evaluation and influence both medical and surgical decision-making. Over the past decade, OCT technology has evolved remarkably, transforming from a purely diagnostic tool into a true intraoperative guidance system that enhances surgical precision. The introduction of intraoperative OCT (iOCT) into the surgical field was a natural evolution, offering real-time feedback on tissue anatomy and direct guidance of surgical maneuvers [2]. Microscope-mounted configurations improved stability and probe control, while the advent of microscope-integrated OCT (MIOCT) represented a major advance, enabling continuous real-time visualization of tissue–instrument interaction through a heads-up display [3,4]. Initially used in vitreoretinal surgery [5,6,7,8,9], iOCT is now widely applied in glaucoma [10], cataract [11], and corneal transplantation procedures [12]. In corneal surgery, it provides enhanced visualization of stromal planes, guides dissection depth, and confirms graft adhesion during lamellar and endothelial keratoplasty, thus improving safety and precision in anterior segment surgery [2]. Despite its growing use, the full potential of iOCT in anterior segment surgery remains underexplored, particularly in cases where corneal opacity or anatomical alterations limit direct visualization. In such situations, the images provided by the device allow the surgeon to overcome corneal opacity and safely perform intraocular maneuvers within the anterior chamber, ensuring proper completion of the surgery. For these reasons, this manuscript is conceived as a narrative, experience-based review, aimed at addressing a relevant gap in the current literature: while previous reviews have primarily focused on the technical aspects of iOCT in specific surgical settings—most notably lamellar corneal surgery—there is still a lack of comprehensive overviews specifically dedicated to the intraoperative use of iOCT in complex anterior segment procedures performed under limited visualization, such as corneal opacity, edema, or altered anatomy. In contrast to prior works, including Moramarco et al. [2], which provided a user-oriented technical guide for lamellar keratoplasty, the present review expands the perspective across multiple anterior segment scenarios, integrating published evidence with real-world intraoperative examples to highlight how iOCT directly influences surgical decision-making, safety, and feasibility in challenging clinical conditions.
2. Endothelial Keratoplasty in Advanced Corneal Edema
Descemet’s stripping automated endothelial keratoplasty (DSAEK) and Descemet membrane endothelial keratoplasty (DMEK) are currently the preferred surgical techniques for the treatment of corneal endothelial disorders [13,14]. Both procedures have demonstrated excellent outcomes in terms of corneal clarity, recovery of visual acuity, and low rates of immunologic rejection. Compared with traditional penetrating keratoplasty (PK), these posterior lamellar approaches offer faster visual rehabilitation, reduced risk of rejection and postoperative astigmatism, and better structural integrity of the globe [15,16]. Given these advantages, their indications have progressively expanded to include advanced cases and eyes with severe corneal edema, where visualization of the anterior chamber is markedly reduced or even absent. In such challenging situations, intraoperative guidance—particularly through microscope-integrated OCT (iOCT)—can provide critical real-time feedback, allowing surgeons to perform the procedure safely despite limited optical transparency.
During Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK), iOCT offers valuable feedback throughout the entire procedure. The iOCT enables the surgeon to confirm the complete removal of the recipient Descemet membrane, even when this step cannot be clearly visualized under the microscope. It also helps assess the smoothness and regularity of the posterior stromal surface, ensuring optimal conditions for donor adhesion. Once the donor lenticule is introduced into the anterior chamber, iOCT can monitor its orientation and centration in real time (Figure 1). This is particularly useful when corneal opacity prevents direct visualization of the graft edge or the interface [17]. After positioning, iOCT enables the precise identification of residual interface fluid between the graft and the host stroma—one of the primary causes of postoperative detachment (REF). The surgeon can then perform targeted corneal massage or adjust intraocular pressure until complete graft apposition is confirmed. Before concluding the procedure, iOCT can verify uniform graft adherence and central thickness, providing objective confirmation of successful graft attachment even in the absence of a clear surgical view [18] (Video S1).
In Descemet Membrane Endothelial Keratoplasty (DMEK), where the donor tissue is much thinner and more delicate, iOCT becomes even more indispensable in eyes with poor visibility: iOCT helps confirm the complete and clean removal of the diseased Descemet membrane, avoiding unrecognized remnants that may hinder donor adhesion. The donor graft, being a thin, translucent membrane, often remains invisible in edematous corneas. iOCT provides continuous monitoring of the scroll’s position during surgery and its configuration, allowing the surgeon to recognize the correct orientation (endothelium-down) and to guide gentle maneuvers for unfolding avoiding overmanipulation. During and after air injection, iOCT can verify the absence of residual fluid clefts and the uniform apposition of the graft to the host stroma. This reduces the risk of postoperative partial detachment and the need for rebubbling procedures [19]. Moreover, in both techniques, intraoperative OCT can be helpful in guiding the iridectomy performed with a vitreous cutter, as it allows localization of the instrument, verification of its contact with the iris, and subsequent confirmation of the iridectomy’s patency (Figure 2).
In both techniques, iOCT serves as an “invisible assistant”, translating cross-sectional images into actionable information. It increases the surgeon’s confidence in challenging cases, allows for an earlier transition from penetrating to lamellar techniques, even in eyes with minimal transparency, and ultimately contributes to safer, more predictable surgical outcomes.
3. Deep Anterior Lamellar Keratoplasty for Leucomatous Corneas
Deep anterior lamellar keratoplasty (DALK) is considered the procedure of choice for corneal pathologies that primarily affect the stroma while sparing the endothelium [20]. By selectively replacing diseased stromal tissue and preserving the host Descemet membrane and endothelium, DALK restores corneal transparency and surface regularity while minimizing the risks of open-sky surgery. This lamellar approach virtually eliminates the possibility of endothelial rejection, the most common cause of graft failure after penetrating keratoplasty, and significantly reduces the risk of intraoperative complications such as expulsive hemorrhage or wound dehiscence [21,22]. Furthermore, preservation of the host endothelium enhances long-term graft survival and maintains endothelial cell density. Another relevant advantage of DALK lies in its favorable refractive outcomes [23]. The technique enables the use of large-diameter grafts, improving optical quality and reducing postoperative irregular astigmatism compared with penetrating keratoplasty [24]. These features make DALK a safe and effective option for a wide range of stromal disorders, including advanced keratoconus, stromal dystrophies, and postinfectious or posttraumatic corneal scars.
The success of Deep Anterior Lamellar Keratoplasty (DALK) largely depends on achieving an optimal stromal dissection plane just above Descemet’s membrane, which is traditionally obtained through the “big bubble” technique [25]. This method involves inserting a cannula into the deep stroma to inject air into the corneal tissue, thereby creating a cleavage plane between the posterior stroma and the Descemet’s membrane. A key factor for successful bubble formation is the accurate placement of the cannula at the appropriate stromal depth. In eyes with good corneal transparency, correct cannula positioning can often be inferred from the appearance of radial stromal folds radiating from the cannula tip during air injection. However, in leucomatous or opaque corneas, this characteristic sign is frequently absent, making it more challenging to determine the correct insertion depth. In such situations, intraoperative OCT can be extremely helpful for verifying the cannula’s position within the stroma. After cannula removal, a hyperreflective linear track can typically be observed within the stroma, indicating the exact depth of insertion (Figure 3). Moreover, iOCT can sometimes visualize the cannula tip in real time during advancement, producing the characteristic “seagull wing” sign, which represents the hyperreflective appearance of the metallic tip as it approaches the pre-Descemetic plane [2]. This real-time feedback allows the surgeon to fine-tune the depth of dissection and optimize the chance of achieving a successful big bubble while minimizing the risk of Descemet membrane perforation.
Another application of iOCT during anterior lamellar keratoplasty is the exploration and assessment of the transparency of the deeper layers. Indeed, during the preoperative and intraoperative evaluation of corneal leucomas, assessment of the integrity of the deeper layers is often hindered by the presence of the anterior leucoma and by backscattering phenomena that may occur on anterior segment OCT. In the intraoperative setting, a superficial stromectomy can be performed, thereby improving visualization of the deeper layers and allowing a more adequate evaluation of the deep stroma. At this point, the deep stroma can also be analyzed using intraoperative OCT to confirm tissue integrity, providing the surgeon with useful information to decide whether to proceed with lamellar surgery or convert to penetrating keratoplasty. Moreover, assessment of the depth of the leucoma is instrumental in evaluating the likelihood of achieving a type 1 bubble. Indeed, deeper leucomas more frequently result in the formation of a type 2 bubble, which may significantly increase the technical difficulty of the procedure as well as the risk of unintended conversion [26]. Conversely, identification of a deep leucoma may influence the surgeon’s decision-making process, leading them to choose manual dissection rather than attempting bubble formation.
4. Management of Corneal Hydrops
Acute corneal hydrops represents a complication of advanced ectatic disorders, mainly keratoconus, characterized by a sudden rupture of Descemet’s membrane and subsequent stromal imbibition of aqueous humor. This results in marked stromal edema and a profound reduction in corneal transparency, which can significantly delay visual rehabilitation and complicate future keratoplasty [27]. In recent years, intraoperative OCT has emerged as a valuable adjunct for both diagnostic assessment and surgical management of hydrops. Intracameral air or gas injection (descemetopexy) has been proposed as an effective approach to promote reapposition of the ruptured Descemet membrane and accelerate the resolution of stromal edema in acute corneal hydrops [28]. The goal of this technique is to create a temporary tamponade effect by filling the anterior chamber with air or gas (such as SF_6_ or C_3_F_8_), thereby pushing the detached Descemet membrane back toward the posterior stroma and facilitating its reattachment. Intraoperative OCT plays a pivotal role in this procedure by allowing precise identification of the Descemet break and the extent of detachment before the injection [29]. During air injection, iOCT provides real-time visualization of the anterior chamber fill, helping to prevent overinflation and minimizing the risk of pupillary block or endothelial touch. The surgeon can directly observe the contact interface between the air bubble and the detached membrane, confirming adequate tamponade and immediate reduction in stromal edema. Residual pockets of intrastromal fluid can also be identified and, if necessary, drained through a controlled paracentesis or gentle corneal massage under OCT guidance (Figure 4) [29].
In addition to air injection, iOCT has proven instrumental during compression suture placement, a technique aimed at approximating the edges of the Descemet break and promoting stromal compaction. Real-time cross-sectional imaging enables surgeons to identify the extent and depth of intrastromal fluid clefts, confirm the location of the Descemet membrane tear, and guide the optimal depth of partial-thickness sutures (typically 50–60% of stromal depth) [30]. During suture application, iOCT provides dynamic visualization of stromal compaction and collapse of intrastromal fluid pockets, allowing intraoperative adjustment of suture tension to achieve uniform compression. This real-time feedback is particularly valuable in markedly edematous or opaque corneas, where conventional slit-lamp visualization is inadequate [31]. The surgeon can observe the progressive reduction in stromal thickness and closure of intrastromal clefts directly on iOCT, ensuring adequate mechanical support without excessive tension that might induce Descemet’s membrane trauma. Postoperatively, iOCT or AS-OCT follow-up enables objective monitoring of corneal thickness stabilization and Descemet’s stromal reattachment, guiding optimal suture removal timing and preventing hydrops recurrence. In cases where both compression sutures and descemetopexy are employed, iOCT helps to optimize their sequence and synergy, ensuring that the sutures are placed at an appropriate depth and that the intracameral bubble provides uniform posterior support along the rupture line [32].
By offering continuous anatomical feedback, iOCT-guided air injection increases the precision and safety of descemetopexy, particularly in eyes with dense stromal edema or poor anterior chamber visibility. This image-guided approach not only shortens the recovery time and promotes faster resolution of corneal edema but also reduces the need for later keratoplasty, improving long-term structural and visual outcomes.
5. Synechiolysis
Peripheral anterior synechiae (PAS) can develop as a sequela of intraocular inflammation, trauma, or previous corneal surgery such as penetrating keratoplasty (PK). These adhesions between the peripheral iris and the corneal endothelium or graft interface may compromise the aqueous outflow, leading to secondary angle closure and progressive endothelial decompensation. Surgical synechiolysis is often required to restore anterior chamber anatomy and prevent glaucoma or graft failure; however, this procedure can be technically demanding in eyes with peripheral corneal opacification, where direct visualization of the angle is limited [33].
In such cases, iOCT serves as an invaluable tool, providing real-time, cross-sectional visualization of anterior segment anatomy. iOCT enables the precise localization and mapping of synechial adhesions that may not be visible clinically through the operative microscope, allowing surgeons to plan the extent and depth of dissection with accuracy (Figure 5). During the procedure, iOCT confirms the progressive separation of the iris from the corneal endothelium or graft-host junction, and visualizes the reformation of the anterior chamber angle as the adhesions are lysed. Furthermore, iOCT can immediately verify the completeness of synechiolysis at the end of surgery, distinguishing residual attachments from normal anatomic structures.
6. Glaucoma Shunt
The implantation of glaucoma drainage devices requires precise intraoperative control to ensure correct positioning of the implant and to prevent complications such as endothelial trauma, iris touch, or malposition within the anterior chamber. This is particularly challenging in eyes with corneal opacity, gerontoxon, or distorted anterior chamber anatomy, where direct visualization through the surgical microscope may be inadequate [34].
In such cases, intraoperative OCT serves as a valuable adjunct, providing real-time cross-sectional visualization of the anterior chamber and surrounding tissues during drainage device implantation. iOCT can confirm the exact entry site and trajectory of the needle tract, ensuring the device passes through the correct scleral plane into the anterior chamber without damaging the iris or the crystalline lens in phakic patients. Once the implant is positioned, iOCT imaging verifies its tip location, angulation, and proximity to the corneal endothelium, allowing adjustments before concluding the surgery. This intraoperative feedback helps prevent postoperative complications such as endothelial cell loss or malposition-related obstruction. Overall, iOCT transforms the implantation of glaucoma drainage devices from a largely experience-based procedure into a controlled, image-guided surgery, increasing accuracy, reducing intraoperative uncertainty, and enhancing the long-term safety of filtration outcomes in eyes with compromised corneal clarity [35].
7. Trauma
Ocular trauma involving the cornea and anterior segment often leads to marked stromal edema, epithelial defects, or blood infiltration into the anterior chamber, all of which severely impair intraoperative visualization. In such challenging scenarios, iOCT offers a decisive advantage by providing real-time cross-sectional imaging of the anterior segment, enabling surgeons to safely navigate anatomical planes that would otherwise be obscured.
In eyes with penetrating corneal trauma, visualization of wound margins, anterior chamber depth, and residual foreign material is often limited due to corneal opacity or localized edema. Under these circumstances, iOCT enables precise assessment of wound depth and extension, and guides the placement of sutures to ensure proper wound apposition and anterior chamber reformation. Bondalapati et al. demonstrated that iOCT can accurately identify and guide the removal of intrastromal or anterior chamber foreign bodies even when the cornea is opaque, thereby minimizing further endothelial or stromal trauma [36]. Similarly, in post-keratoplasty wound dehiscence secondary to blunt trauma, iOCT provides continuous feedback on the integrity of the graft–host junction and on the configuration of the Descemet membrane. During surgical repair, it allows real-time monitoring of graft alignment, suture depth, and intracameral air tamponade, which are otherwise difficult to judge when the cornea becomes edematous or blood-stained. As reported by Chaniyara et al., this approach facilitates accurate reapposition of the corneal layers and confirms intraoperative restoration of anterior chamber depth, even in cases with complete loss of optical clarity [37].
The ability of iOCT to penetrate edematous or leucomatous corneal tissue makes it an invaluable tool in traumatic eyes with poor visibility, transforming potentially high-risk “blind” procedures into image-guided, controlled interventions. By enabling the surgeon to visualize hidden structures—such as the Descemet membrane, graft interface, or anterior chamber boundaries—iOCT significantly enhances surgical safety, reduces iatrogenic injury, and improves the likelihood of anatomical and functional recovery in complex traumatic cases.
8. Future Directions
Future developments in intraoperative OCT are expected to further enhance its role as a decision-support tool in anterior segment surgery. Advances in real-time image processing may enable automated tissue segmentation and quantitative tracking of corneal and anterior chamber structures, providing continuous feedback on tissue thickness and instrument proximity. The integration of artificial intelligence algorithms could facilitate intraoperative recognition of surgical planes, interface fluid, or unsafe maneuvers, supporting surgeon decision-making in complex cases. Additionally, improved acquisition speed, wider fields of view, and better management of instrument-related shadowing may further optimize intraoperative visualization. Together, these innovations may contribute to safer, more standardized, and more reproducible image-guided anterior segment surgery [38].
9. Conclusions
Intraoperative optical coherence tomography (iOCT) has emerged as a transformative adjunct in anterior segment surgery performed under limited visualization. By providing real-time, cross-sectional imaging of ocular structures, iOCT enables surgeons to overcome challenges imposed by corneal opacity, edema, or distorted anterior chamber anatomy, allowing image-guided precision in procedures that were previously performed with limited or indirect visual feedback. Its integration into the surgical microscope has expanded the feasibility of lamellar keratoplasty, facilitated the safe execution of complex maneuvers such as synechiolysis and glaucoma drainage device implantation, and improved intraoperative control in traumatic or severely edematous eyes (Table 1).
It should be acknowledged that the evidence supporting many current applications of iOCT in anterior segment surgery is predominantly derived from observational studies, small case series, and expert experience, with limited availability of high-level comparative data. In addition, access to microscope-integrated iOCT systems remains variable across institutions, and the technology entails costs, workflow considerations, and a learning curve that may restrict widespread adoption. Despite these limitations, across published reports and real-world clinical practice, iOCT consistently provides unique intraoperative anatomical information that is otherwise unavailable in eyes with compromised visualization, offering a level of real-time guidance that cannot be fully replicated by alternative imaging modalities such as ultrasound biomicroscopy or endoscopy.
Within this context, the contribution of the present narrative review lies not in quantitative synthesis, but in the integration of available evidence with real-life intraoperative scenarios, illustrating how iOCT directly influences surgical decision-making, enhances safety, and expands the range of anterior segment procedures that can be performed in challenging clinical conditions. As image resolution and acquisition speed continue to improve, future developments may include automated depth tracking, artificial intelligence–assisted intraoperative feedback, and integration with digital and robotic surgical platforms. These advances may further strengthen the role of iOCT as a decision-support tool in complex anterior segment surgery, bridging the gap between imaging and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Izatt J.A. Hee M.R. Swanson E.A. Lin C.P. Huang D. Schuman J.S. Puliafito C.A. Fujimoto J.G. Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography Arch. Ophthalmol.19941121584158910.1001/archopht.1994.010902400900317993214 · doi ↗ · pubmed ↗
- 2Moramarco A. di Geronimo N. Airaldi M. Gardini L. Semeraro F. Iannetta D. Romano V. Fontana L. Intraoperative OCT for Lamellar Corneal Surgery: A User Guide J. Clin. Med.202312304810.3390/jcm 1209304837176489 PMC 10179477 · doi ↗ · pubmed ↗
- 3Ray R. Barañano D.E. Fortun J.A. Schwent B.J. Cribbs B.E. Bergstrom C.S. Hubbard G.B. Srivastava S.K. Intraoperative microscope-mounted spectral domain optical coherence tomography for evaluation of retinal anatomy during macular surgery Ophthalmology 20111182212221710.1016/j.ophtha.2011.04.01221906815 · doi ↗ · pubmed ↗
- 4Ehlers J.P. Dupps W.J. Kaiser P.K. Goshe J. Singh R.P. Petkovsek D. Srivastava S.K. The Prospective Intraoperative and Perioperative Ophthalmic Imagi Ng with Optical Coher Enc E Tomog Raphy (PIONEER) Study: 2-year results Am. J. Ophthalmol.2014158999100710.1016/j.ajo.2014.07.03425077834 PMC 4250395 · doi ↗ · pubmed ↗
- 5Yee P. Sevgi D.D. Abraham J. Srivastava S.K. Le T. Uchida A. Figueiredo N. Rachitskaya A.V. Sharma S. Reese J. i OCT-assisted macular hole surgery: Outcomes and utility from the DISCOVER study Br. J. Ophthalmol.202110540340910.1136/bjophthalmol-2020-31604532376609 · doi ↗ · pubmed ↗
- 6Wykoff C.C. Berrocal A.M. Schefler A.C. Uhlhorn S.R. Ruggeri M. Hess D. Intraoperative OCT of a full-thickness macular hole before and after internal limiting membrane peeling Ophthalmic Surg. Lasers Imaging Off. J. Int. Soc. Imaging Eye 20104171110.3928/15428877-20091230-0120128563 · doi ↗ · pubmed ↗
- 7Abraham J.R. Srivastava S.K. Le T.K. Sharma S. Rachitskaya A. Reese J.L. Ehlers J.P. Intraoperative OCT-Assisted Retinal Detachment Repair in the DISCOVER Study: Impact and Outcomes Ophthalmol. Retina 2020437838310.1016/j.oret.2019.11.00231948909 PMC 7150644 · doi ↗ · pubmed ↗
- 8Falkner-Radler C.I. Glittenberg C. Gabriel M. Binder S. Intrasurgical microscope-integrated spectral domain optical coherence tomography-assisted membrane peeling Retina 2015352100210610.1097/IAE.000000000000059625978733 · doi ↗ · pubmed ↗