Three-Dimensional Accuracy of Digitally Planned Orthodontic Tooth Movement in a Fully Customized Self-Ligating Lingual System
Arda Arısan, Tülin Taner

TL;DR
A new customized self-ligating lingual orthodontic system accurately reproduces planned tooth movements in most areas, though accuracy is slightly lower in the back teeth.
Contribution
This study evaluates the 3D accuracy of a fully customized self-ligating lingual orthodontic system using digital models and statistical analysis.
Findings
The system achieved 92.1% overall dentition accuracy in reproducing planned tooth positions.
Anterior teeth showed the highest accuracy in mesiodistal and buccolingual movements.
Posterior teeth had lower rotational accuracy, but results remained clinically acceptable.
Abstract
Background: Lingual orthodontic systems have recently advanced with the introduction of fully customized CAD/CAM-based designs featuring self-ligating (SL) mechanisms. This study aimed to evaluate the three-dimensional accuracy of a customized SL lingual system in reproducing digitally planned tooth positions. Methods: A total of 280 teeth were analyzed following treatment with a fully customized self-ligating lingual system (Harmony®, Aso International Inc., Tokyo, Japan). Digital models obtained before treatment (T0), from the setup (TS), and after treatment (T1) were superimposed using a best fit algorithm in GOM Inspect. Tooth movements were quantified across seven biomechanically relevant parameters including tip, torque, rotation, buccolingual, mesiodistal, vertical, and overall displacement. Predicted and achieved movements were compared using paired t tests and Bland–Altman…
Click any figure to enlarge with its caption.
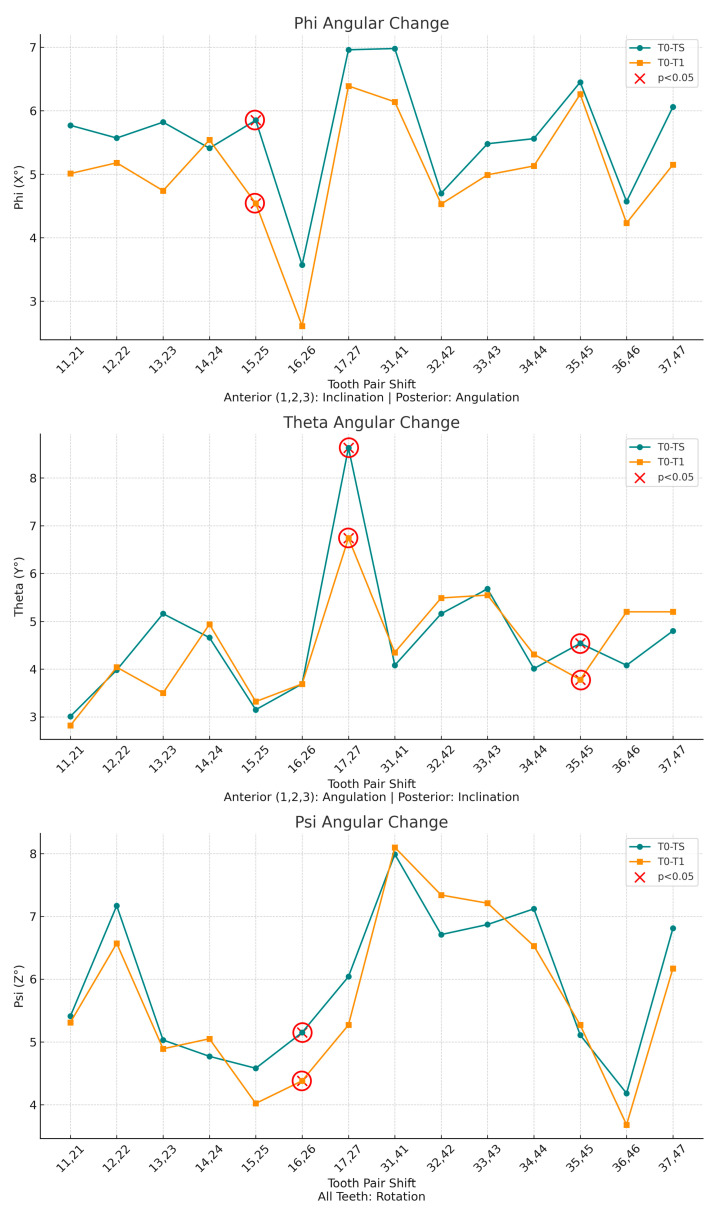 Figure 10
Figure 10|
| ||||||||
|
|
|
|
|
|
|
| ||
|
|
|
|
|
|
|
| ||
| 11,21 | T0–TS | 1.94 ± 1.42 | 0.94 ± 1 | 0.58 ± 0.29 | 0.74 ± 0.69 | 5.77 ± 2.44 | 3.01 ± 2.37 | 5.41 ± 3.24 |
| T0–T1 | 1.81 ± 1.76 | 0.92 ± 0.85 | 0.5 ± 0.39 | 0.56 ± 0.37 | 5.01 ± 2.16 | 2.82 ± 2.32 | 5.31 ± 3.3 | |
|
| 0.569 | 0.826 | 0.431 | 0.227 | 0.111 | 0.354 | 0.796 | |
| Accuracy % | 93.3 | 97.9 | 86.2 | 75.7 | 86.8 | 93.7 | 98.2 | |
| 12,22 | T0–TS | 2.56 ± 1.63 | 1.51 ± 1.35 | 1.11 ± 0.8 | 0.82 ± 0.44 | 5.57 ± 3.59 | 3.98 ± 2.36 | 7.17 ± 1.74 |
| T0–T1 | 2.37 ± 1.54 | 1.38 ± 1.27 | 1.06 ± 0.86 | 0.81 ± 0.53 | 5.18 ± 3.79 | 4.04 ± 2.07 | 6.57 ± 1.87 | |
|
| 0.108 | 0.184 | 0.623 | 0.925 | 0.357 | 0.925 | 0.110 | |
| Accuracy % | 92.6 | 91.4 | 95.5 | 98.8 | 93.0 | 99.0 | 91.6 | |
| 13,23 | T0–TS | 1.62 ± 0.76 | 0.92 ± 0.72 | 0.59 ± 0.46 | 0.98 ± 0.47 | 5.82 ± 2.92 | 5.16 ± 2.78 | 5.03 ± 1.91 |
| T0–T1 | 1.65 ± 0.6 | 0.87 ± 0.5 | 0.7 ± 0.4 | 0.85 ± 0.58 | 4.74 ± 2.41 | 5.3 ± 2.04 | 4.89 ± 1.75 | |
|
| 0.710 | 0.692 | 0.265 | 0.380 | 0.089 | 0.768 | 0.539 | |
| Accuracy % | 99.0 | 94.6 | 99.0 | 86.7 | 81.4 | 99.0 | 97.2 | |
| ( | ||||||||
|
|
|
|
|
|
|
| ||
|
|
|
|
|
|
|
| ||
| 14,24 | T0–TS | 1.72 ± 0.61 | 0.91 ± 0.37 | 0.81 ± 0.69 | 0.91 ± 0.37 | 4.66 ± 3.65 | 5.41 ± 4.04 | 4.77 ± 1.97 |
| T0–T1 | 1.57 ± 0.57 | 0.74 ± 0.28 | 0.89 ± 0.57 | 0.88 ± 0.35 | 4.94 ± 4.02 | 5.54 ± 3.46 | 5.05 ± 1.96 | |
|
| 0.104 | 0.073 | 0.521 | 0.735 | 0.643 | 0.755 | 0.391 | |
| Accuracy % | 91.3 | 81.3 | 99.0 | 96.7 | 99.0 | 99.0 | 99.0 | |
| 15,25 | T0-TS | 1.81 ± 0.72 | 0.71 ± 0.38 | 0.95 ± 0.64 | 1.13 ± 0.46 | 3.15 ± 2.07 | 5.85 ± 3.16 | 4.58 ± 1.33 |
| T0-T1 | 1.62 ± 0.62 | 0.58 ± 0.33 | 0.96 ± 0.46 | 0.96 ± 0.47 | 3.32 ± 1.94 | 4.54 ± 2.31 | 4.02 ± 1.94 | |
|
| 0.102 | 0.041 * | 0.974 | 0.045 * | 0.707 | 0.045 * | 0.329 | |
| Accuracy % | 89.5 | 81.7 * | 99.0 | 85.0 * | 99.0 | 77.6 * | 87.8 | |
| 16,26 | T0–TS | 1.75 ± 0.69 | 0.69 ± 0.39 | 1.13 ± 0.66 | 0.77 ± 0.53 | 3.69 ± 1.58 | 3.57 ± 1.47 | 5.15 ± 1.88 |
| T0–T1 | 1.49 ± 0.66 | 0.47 ± 0.23 | 1.08 ± 0.54 | 0.66 ± 0.52 | 3.69 ± 1.83 | 2.61 ± 1.34 | 4.38 ± 2.34 | |
|
| 0.039 * | 0.049 * | 0.718 | 0.099 | 0.995 | 0.092 | 0.027 * | |
| Accuracy % | 85.1 * | 68.1 * | 95.6 | 85.7 | 99.0 | 73.1 | 85.0 * | |
| 17,27 | T0–TS | 2.51 ± 2.03 | 0.76 ± 0.55 | 1.13 ± 0.72 | 1.12 ± 0.76 | 8.63 ± 4.35 | 6.96 ± 3.57 | 6.04 ± 3.02 |
| T0–T1 | 2.28 ± 1.65 | 0.6 ± 0.52 | 1.32 ± 0.96 | 0.63 ± 0.58 | 6.74 ± 4.24 | 6.39 ± 3.05 | 5.27 ± 2.57 | |
|
| 0.225 | 0.231 | 0.241 | 0.027 * | 0.006 * | 0.562 | 0.227 | |
| Accuracy % | 90.8 | 78.9 | 99.0 | 56.3 * | 78.1 * | 91.8 | 87.2 | |
|
| ||||||||
|
|
|
|
|
|
|
| ||
|
|
|
|
|
|
|
| ||
| 31,41 | T0–TS | 2.24 ± 0.63 | 0.76 ± 0.73 | 0.91 ± 0.56 | 1.56 ± 0.55 | 6.98 ± 4.23 | 4.08 ± 2.24 | 7.99 ± 4.09 |
| T0–T1 | 2.28 ± 0.9 | 1.02 ± 1.18 | 0.94 ± 0.41 | 1.27 ± 0.63 | 6.14 ± 3.38 | 4.35 ± 3.06 | 8.1 ± 4.1 | |
|
| 0.743 | 0.158 | 0.806 | 0.171 | 0.154 | 0.577 | 0.883 | |
| Accuracy % | 99.0 | 99.0 | 99.0 | 81.4 | 88.0 | 99.0 | 99.0 | |
| 32,42 | T0–TS | 2.06 ± 0.81 | 1 ± 0.72 | 0.92 ± 0.69 | 1.36 ± 0.54 | 4.7 ± 2.79 | 5.16 ± 4 | 6.71 ± 4.62 |
| T0–T1 | 2.06 ± 0.8 | 1.12 ± 1.02 | 0.88 ± 0.54 | 1.27 ± 0.46 | 4.53 ± 2.28 | 5.49 ± 3.75 | 7.34 ± 4.71 | |
|
| 0.988 | 0.472 | 0.706 | 0.205 | 0.543 | 0.545 | 0.334 | |
| Accuracy % | 99.0 | 99.0 | 95.7 | 93.4 | 96.4 | 99.0 | 99.0 | |
| 33,43 | T0–TS | 2.34 ± 0.85 | 1.38 ± 0.86 | 1.2 ± 0.75 | 1.31 ± 0.72 | 5.48 ± 2.74 | 5.68 ± 2.34 | 6.87 ± 3.18 |
| T0–T1 | 2.52 ± 0.92 | 1.51 ± 1.16 | 1.19 ± 0.64 | 1.22 ± 0.4 | 4.99 ± 2.55 | 5.55 ± 2.24 | 7.21 ± 2.87 | |
|
| 0.118 | 0.442 | 0.820 | 0.583 | 0.197 | 0.776 | 0.268 | |
| Accuracy % | 99.0 | 99.0 | 99.2 | 93.1 | 91.1 | 97.7 | 99.0 | |
| ( | ||||||||
|
|
|
|
|
|
|
| ||
|
|
|
|
|
|
|
| ||
| 34,44 | T0–TS | 2.15 ± 1.1 | 0.97 ± 0.7 | 1.62 ± 1.05 | 0.9 ± 0.24 | 4.01 ± 2.24 | 5.56 ± 3 | 7.12 ± 2.45 |
| T0–T1 | 2.32 ± 1.32 | 0.96 ± 0.84 | 1.53 ± 1.09 | 0.84 ± 0.31 | 4.31 ± 2.53 | 5.13 ± 2.84 | 6.53 ± 2.36 | |
|
| 0.336 | 0.890 | 0.549 | 0.631 | 0.613 | 0.498 | 0.141 | |
| Accuracy % | 99.0 | 99.0 | 94.4 | 93.3 | 99.0 | 92.3 | 91.7 | |
| 35,45 | T0–TS | 2.28 ± 1.02 | 0.93 ± 0.59 | 1.66 ± 0.9 | 0.99 ± 0.38 | 4.54 ± 1.71 | 6.45 ± 2.99 | 5.11 ± 3.46 |
| T0–T1 | 2.25 ± 1.14 | 0.97 ± 0.93 | 1.46 ± 1 | 0.86 ± 0.37 | 3.78 ± 1.9 | 6.26 ± 2.47 | 5.27 ± 3.87 | |
|
| 0.898 | 0.793 | 0.199 | 0.406 | 0.004 * | 0.650 | 0.793 | |
| Accuracy % | 98.7 | 99.0 | 88.0 | 86.9 | 83.3 * | 97.1 | 99.0 | |
| 36,46 | T0–TS | 2.14 ± 0.84 | 0.89 ± 0.43 | 1.35 ± 1.07 | 1.14 ± 0.58 | 4.08 ± 2 | 4.57 ± 2.47 | 4.18 ± 1.41 |
| T0–T1 | 1.94 ± 0.98 | 0.86 ± 0.51 | 1.31 ± 1.06 | 0.86 ± 0.5 | 5 ± 2.12 | 4.23 ± 1.97 | 3.68 ± 2.03 | |
|
| 0.145 | 0.628 | 0.723 | 0.005 * | 0.051 | 0.389 | 0.275 | |
| Accuracy % | 90.7 | 96.6 | 97.0 | 75.4 * | 99.0 | 92.6 | 88.0 | |
| 37,47 | T0–TS | 2.38 ± 0.74 | 1.19 ± 0.47 | 1.69 ± 1.11 | 0.9 ± 0.51 | 4.8 ± 2.04 | 6.06 ± 3.46 | 6.81 ± 2.01 |
| T0–T1 | 2.25 ± 0.88 | 1 ± 0.69 | 1.57 ± 1.32 | 0.81 ± 0.57 | 5.2 ± 2.6 | 5.15 ± 2.6 | 6.17 ± 2.07 | |
|
| 0.441 | 0.297 | 0.482 | 0.442 | 0.273 | 0.202 | 0.179 | |
| Accuracy % | 94.5 | 84.0 | 92.9 | 90.0 | 99.0 | 85.0 | 90.6 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Temporomandibular Joint Disorders · Dental materials and restorations
1. Introduction
Lingual orthodontics has increasingly incorporated fully customized CAD/CAM-based bracket systems that allow precise adaptation to individual dental morphology and clinical requirements [1]. These computer-designed and laboratory-manufactured appliances enable individualized bracket positioning and accurate control of archwire geometry, thereby optimizing tooth movement and overall biomechanics [2]. Alongside this development, the introduction of self-ligating (SL) designs has supported more efficient and comfortable treatment protocols [3]. Clinically, SL configurations may reduce chair time and simplify archwire engagement [4], while also meeting the high esthetic expectations of adult patients seeking discreet orthodontic treatment [5].
The accuracy of reproducing digitally planned tooth positions is a key indicator of the clinical performance of contemporary orthodontic appliances [6] and is commonly assessed through three-dimensional comparisons between the virtual setup and the final treatment outcome [7]. Several studies have specifically evaluated the accuracy with which customized systems transfer digitally planned bracket positions to the dentition during the indirect bonding process [8,9,10]. Similar analyses of labially placed customized systems have demonstrated that bracket positioning accuracy may vary depending on the bonding protocol, bracket design, and manufacturing workflow [11,12].
Clear aligner therapy has gained widespread acceptance due to its favorable esthetics and high patient acceptance among both adult and adolescent patients [13,14]. Consequently, numerous studies have investigated the accuracy with which aligners reproduce digitally planned tooth movements and achieve predictable clinical outcomes [15,16,17,18,19,20]. While predictable results have been reported for simple alignment and minor space closure, reduced accuracy persists for rotations, intrusions, and torque movements when compared with fixed appliances [20,21,22,23]. These limitations become particularly evident when treatment objectives involve complex movements or significant vertical discrepancies.
For patients who prioritize esthetics under challenging treatment conditions, lingual orthodontic appliances represent a reliable alternative. Previous studies have demonstrated that their biomechanical efficiency is comparable to that of conventional labial systems, enabling precise tooth movement while maintaining effective esthetic concealment [24,25,26,27,28]. Despite these advantages, the amount of clinical evidence available on fully customized SL lingual systems remains relatively limited. Further well-designed studies are required to confirm their accuracy, long term stability, and overall clinical performance in complex treatment scenarios.
The aim of this study was to evaluate the accuracy with which a fully customized SL lingual orthodontic appliance (Harmony^®^, Aso International Inc., Tokyo, Japan) reproduces the planned digital treatment setup using three-dimensional superimposition and quantitative analysis.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of Hacettepe University (Decision No: KA-15016). Additionally, compliance certification was obtained from the Turkish Medicines and Medical Devices Agency (TMMDA), approval number 71146310 [2016-CE-004]. All participants provided written informed consent prior to inclusion. All patients were treated at the Hacettepe University Faculty of Dentistry, Department of Orthodontics.
2.2. Participants and Eligibility Criteria
15 adults who had completed skeletal growth and requested lingual orthodontic treatment for esthetic reasons were screened. Inclusion criteria were Class I malocclusion with stable habitual occlusion, skeletal symmetry, a mesofacial growth pattern (FMA: 25° ± 4), and mild to moderate arch length deficiency in both arches (2–5 mm). Exclusion criteria included a need for orthognathic surgery or skeletal anchorage, skeletal anomalies, an unreproducible maximum intercuspation, or incomplete records. 10 consecutive patients (7 females, 3 males; mean age, 27.3 ± 6.9 years; range, 18–38 years) met the criteria, providing 20 dental arches and 280 teeth for three-dimensional evaluation.
2.3. Data Collection and Digital Setup
Standard orthodontic records were obtained at T0 (pretreatment) and T1 (posttreatment). Digital models were generated using a 7Series desktop optical scanner (Dental Wings, Montreal, QC, Canada) at 15 μm resolution. The treatment setup (TS) was created by the Harmony Technical Center (ASO International Inc., Japan) and delivered in STL format. For each time point (T0, TS, T1), three STL files were generated per patient: maxillary arch, mandibular arch, and occlusal bite registration (Figure 1).
2.4. Orthodontic Treatment Protocol
After approval of the setup, fully customized self-ligating lingual brackets and transfer trays were fabricated using CAD/CAM technology. Indirect bonding was performed on etched lingual enamel surfaces (37% phosphoric acid) using a dual-cure resin cement (Maxcem Elite, Kerr, Orange, CA, USA). Brackets were light cured according to the manufacturer’s recommendations, with additional curing performed after tray removal. The archwire sequence consisted of 0.014-inch NiTi, 0.016 × 0.016-inch NiTi, 0.016 × 0.022-inch NiTi, and 0.018 × 0.025-inch NiTi. Interproximal reduction was performed according to the digital plan. Treatment was completed after achieving Class I canine and molar relationships and ideal overbite (0–3 mm) and overjet (2–3 mm), based on the American Board of Orthodontics Objective Grading System thresholds [29]. A fixed lingual retainer (Bond-A-Braid, Reliance Orthodontic Products, Itasca, IL, USA) was bonded from canine to canine in both arches and used together with an Essix retainer. The progressive changes in archwire dimensions and bracket configurations during treatment are illustrated in Figure 2.
2.5. Digital Model Processing and Superimposition
STL models (T0, TS, T1) were imported into GOM Inspect (GOM GmbH, Braunschweig, Germany). The T0 maxillary model was oriented to the local coordinate system using the incisive papilla as the origin. Maxillary superimposition was performed using initial three-point registration on palatal rugae followed by best-fit surface alignment, selected due to their documented stability [30,31]. The setup (TS) and posttreatment (T1) models were aligned to T0 using the same protocol.
The mandibular models were registered with the help of the bite scan. The bite scan was aligned to the maxillary models, and its maxillary portion was then removed, leaving the mandibular segment positioned in the same coordinate system. Registration was refined by identifying lingual cortical bone contours and applying best-fit surface alignment. Figure 3 shows color-coded superimpositions illustrating the T0–T1 and T0–TS alignments, as well as the combined T0–T1–TS alignment obtained from bite registration.
2.6. Tooth Movement Measurements
After model alignment, reference points and axes were established for each tooth in all models. The facial axis point was used as the reference point, with the facial axis of the clinical crown defined as the tooth axis. A horizontal axis and a vertical axis were also assigned to standardize angular measurements. These reference points and planes served as the basis for calculating angular and linear tooth movements, as illustrated in Figure 4.
Angular measurements between reference planes and linear measurements between reference points were performed for two intervals: T0–T1 (pretreatment to posttreatment) and T0–TS (pretreatment to digital setup). Movements were evaluated along seven parameters, including three angular (Phi, Theta, Psi) and four linear (L, LX, LY, LZ) components. Linear movements were measured in millimeters, while angular movements were measured in degrees. Detailed definitions and axis-specific interpretations for anterior and posterior teeth are summarized in Table 1. Representative examples of these measurement parameters are presented in Figure 5, Figure 6, Figure 7 and Figure 8.
2.7. Statistical Analysis
A priori power analysis was performed using G*Power 3.1 software (Heinrich Heine University, Düsseldorf, Germany) to estimate the required sample size for paired t-test analysis. Based on previous orthodontic accuracy studies [32], assuming a medium effect size (Cohen’s d = 0.5), an alpha level of 0.05, and a desired power of 0.80, a minimum of 34 paired measurements was required.
To reduce intra-subject variability, 280 teeth were grouped into 140 symmetrical pairs according to the FDI tooth numbering system, with each pair serving as one analytical unit. Seven movement parameters were analyzed, including three angular (torque, angulation, and rotation) and four linear (L, LX, LY, and LZ) displacements. Analyses were performed at the paired-tooth unit level; potential within-subject clustering is acknowledged as an inherent limitation. Accuracy was calculated using the formula described by Kravitz et al. [33]: Accuracy (%) = 100 − (|predicted − achieved|/|predicted| × 100).
All statistical analyses were performed using IBM SPSS Statistics 20.0 (IBM Corp., Armonk, NY, USA). Predicted (T0–TS) and achieved (T0–T1) tooth movements were compared using paired sample t tests. Agreement was evaluated using Bland–Altman analysis, and reliability was assessed using intraclass correlation coefficients (ICCs). Statistical significance was set at p < 0.05.
3. Results
3.1. Quantitative Movement Analysis
Table 2a,b and Table 3a,b present detailed measurements of planned (T0–TS) versus achieved (T0–T1) tooth movements across all spatial parameters. The results show systematic variations in precision between anatomical regions and movement types, with linear movements generally demonstrating higher accuracy than angular movements.
The distribution of linear and angular tooth movements across symmetrical tooth pairs, along with the mean values for each pair, is illustrated in Figure 9 and Figure 10.
3.2. Statistical Significance and Movement Precision
Ten parameters showed statistically significant differences between planned and achieved values (p < 0.05), primarily involving posterior teeth. In the maxillary posterior region, the largest deviations were observed for vertical displacement of teeth 17 and 27 (accuracy: 56.3%), buccolingual displacement of teeth 16 and 26 (68.1%), and angulation of teeth 15 and 25 (77.6%). In the mandible, fewer parameters reached statistical significance, with deviations observed for inclination of teeth 35 and 45 (83.3%) and vertical displacement of teeth 36 and 46 (75.4%). No statistically significant deviations were detected for mandibular anterior teeth. Maxillary anterior teeth demonstrated consistently high accuracy across most parameters.
Angular tooth movement measurements comparing planned (T0–TS, green) and achieved (T0–T1, orange) rotations. Phi (X°): inclination (anterior teeth)/angulation (posterior teeth); Theta (Y°): angulation (anterior teeth)/inclination (posterior teeth); Psi (Z°): rotation around the tooth’s long axis. Red X markers (circled in red) indicate statistically significant differences (p < 0.05).
3.3. Regional Movement Analysis
The fully customized self-ligating lingual appliance achieved an overall dentition accuracy of 92.1%. Mean accuracy for linear tooth movements was 94.5% ± 2.1% in the maxilla and 93.8% ± 2.5% in the mandible. The highest accuracy values were observed in the mandibular anterior region. In the maxillary anterior region, angulation accuracy was 97.2% and rotation accuracy was 95.7%, whereas vertical displacement accuracy was lower (87.1%). Posterior accuracy was lower overall, particularly in the maxillary arch (buccolingual: 77.5%; vertical: 80.9%). In the mandible, posterior accuracy remained higher (total displacement: 95.7%), despite reduced vertical displacement accuracy (86.4%).
4. Discussion
4.1. Principal Findings and Clinical Implications
The higher predictability observed in mandibular anterior teeth may be attributed to biomechanical characteristics of lingual orthodontics. Bracket positioning closer to the center of resistance, combined with simpler root morphology, facilitates more controlled force application and reduces the risk of uncontrolled tipping. Clinically, these findings indicate that customized self-ligating lingual appliances are well suited for anterior alignment. Except for a single deviation observed in tooth 36 for vertical displacement (LZ), mandibular teeth generally showed good agreement between predicted and achieved positions.
In contrast, greater deviations were observed in the maxillary posterior region, particularly in teeth 16 and 17. These findings likely reflect limitations in vertical control and buccolingual molar movement with lingual mechanics. In addition to biomechanical factors, the more complex root morphology of posterior teeth may contribute to the greater deviations observed in these regions, representing a challenge for precise posterior tooth movement with lingual orthodontic systems. Although linear accuracy remained acceptable, angular control, especially torque expression, was less predictable. Clinically, this underscores the importance of realistic treatment planning, the selective use of auxiliary mechanics, and conservative objectives when substantial molar repositioning is required.
4.2. Comparison with Previous Studies
The present findings are consistent with previous studies reporting higher accuracy in anterior regions and reduced predictability in posterior teeth. Pauls et al. reported translational deviations below 0.5 mm and angular discrepancies under 4.6°, particularly in incisors, a finding that is in line with the high anterior accuracy observed in the present study [2]. In a larger sample, Grauer and Proffit evaluated Incognito (3M Unitek, Monrovia, CA, USA) cases and found accuracy values generally below 1 mm and 4°, with the exception of second molars, a result that is consistent with the observation that posterior teeth present greater challenges in vertical and angular control [28]. Sharp et al. assessed the Incognito Lite system, a partial-arch appliance focused primarily on anterior correction rather than full-arch mechanics. Their results showed that while angular (tip and torque) and rotational movements were consistently achieved within ±3°, translational discrepancies were more pronounced, with average deviations reaching 1.0 mm in maxillary central incisors [34]. Fernandes et al. compared Incognito with iLingual 3D (GAC International, Bohemia, NY, USA) and Lingual Matrix (Adenta GmbH, Gilching, Germany), showing that Incognito achieved the highest accuracy in all parameters except in-out positioning, while all three systems proved clinically reliable for anterior tooth movements [24].
For non-customized lingual systems, Albertini et al. demonstrated that the lingual straight-wire technique achieved 84–92% accuracy for torque, tip, and rotation in incisors, canines, and premolars, whereas accuracy was lower in molars (52–81%) [26]. Scisciola et al. reported that passive self-ligating lingual straight-wire appliances with square slots achieved mean accuracy values of 77.25% for torque, 78.41% for tip, and 77.99% for rotation, with accuracy decreasing from anterior to posterior regions [25]. In parallel, Palone et al. showed that the Suresmile^®^ (Dentsply Sirona, Charlotte, NC, USA) lingual technique demonstrated even lower accuracy values of 60.11% for torque, 53.52% for tip, and 59.19% for rotation, highlighting the need for overcorrections during orthodontic planning [27]. These studies relied on prefabricated rather than fully customized lingual brackets, which may partly explain their lower accuracy compared with CAD/CAM-based fully customized systems.
Clear aligner therapy has been widely evaluated with respect to the predictability of complex tooth movements, providing a useful point of comparison with fixed appliance systems. Kravitz et al. reported a mean overall accuracy of 41%, identifying extrusion and rotation as the least predictable movements [33], while Haouili et al. observed a mean accuracy of approximately 50% for Invisalign^®^ (Align Technology, San Jose, CA, USA), with crown tip showing the highest predictability (56%) and rotation the lowest (46%) [22]. More recently, Migliorati et al. reported improved accuracy values for 3D-printed aligners, with 67.6% for torque, 64.2% for tip, and 72.0% for rotation, and particularly high predictability for transverse movements (99.6%) [16]. Further investigations have shown that limitations persist for larger or more demanding movements. D’Antò et al. demonstrated that even after 15 aligners, extensive mesiodistal and vertical corrections exhibited notable deviations, especially in molars [19]. Similarly, Li et al. reported that aligner software tends to overestimate achievable tooth movement in staged treatments, particularly for posterior displacement [15]. Although Bilello et al. described more favorable outcomes for Invisalign^®^, especially in mandibular central incisors, reduced predictability remained evident for movements of greater magnitude [23]. In the present study, angular changes exceeding 6° of inclination and vertical displacements greater than 2 mm were frequently planned, particularly in posterior teeth, creating a more demanding biomechanical scenario and providing a rigorous test of the performance of the fully customized self-ligating lingual appliance.
4.3. Limitations and Future Directions
The findings of this study should be interpreted considering limitations. Although sample adequacy was confirmed, planned movements were generally moderate and did not encompass a wide range of malocclusion types. The retrospective design limited treatment standardization, and minor digitization and landmarking variability may have influenced superimposition accuracy despite validated protocols. Factors such as wire–bracket play, torque expression limitations, and archwire coordination may partially explain reduced accuracy in certain parameters. As only one fully customized lingual system was evaluated, the findings may not be directly generalizable to other systems. Although contralateral tooth pairing reduced intra-subject variability, tooth movement within an arch is biomechanically interdependent, representing an inherent limitation of this analytical approach [35,36].
Despite these limitations, the study provides a detailed three-dimensional evaluation of a fully customized self-ligating lingual appliance and contributes meaningful clinical insight. Future prospective, multi-center studies with larger and more heterogeneous samples are needed, and emerging artificial intelligence–based tools may further enhance the objective assessment of orthodontic treatment accuracy [37].
5. Conclusions
The fully customized self-ligating lingual orthodontic appliance showed a high level of accuracy in achieving planned tooth movements in patients with mild to moderate malocclusions. Accuracy was generally higher in anterior teeth, while posterior regions showed reduced predictability, particularly for vertical and angular movements. Future multi-center studies including more complex malocclusion types are needed to further assess the clinical performance of this system.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wiechmann D. A New Bracket System for Lingual Orthodontic Treatment. Part 1: Theoretical Background and Development J. Orofac. Orthop.20026323424510.1007/s 00056-002-0211-512132311 · doi ↗ · pubmed ↗
- 2Pauls A. Nienkemper M. Schwestka-Polly R. Wiechmann D. Therapeutic Accuracy of the Completely Customized Lingual Appliance WIN: A Retrospective Cohort Study J. Orofac. Orthop.201778526110.1007/s 00056-016-0058-927858111 PMC 5247553 · doi ↗ · pubmed ↗
- 3Rafi R. Silvia G. Pablo E. Lingual & Esthetic Orthodontics Quintessence Publishing Co., Ltd.Batavia, IL, USA 2011692 p
- 4Fritz U. Diedrich P. Wiechmann D. Lingual Technique--Patients’ Characteristics, Motivation and Acceptance. Interpretation of a Retrospective Survey J. Orofac. Orthop.20026322723310.1007/s 00056-002-0124-312132310 · doi ↗ · pubmed ↗
- 5Dalessandri D. Lazzaroni E. Migliorati M. Piancino M.G. Tonni I. Bonetti S. Self-Ligating Fully Customized Lingual Appliance and Chair-Time Reduction: A Typodont Study Followed by a Randomized Clinical Trial Eur. J. Orthod.20133575876510.1093/ejo/cjs 09323180385 · doi ↗ · pubmed ↗
- 6Awad M.G. Ellouze S. Ashley S. Vaid N. Makki L. Ferguson D.J. Accuracy of Digital Predictions with CAD/CAM Labial and Lingual Appliances: A Retrospective Cohort Study Semin. Orthod.20182439340610.1053/j.sodo.2018.10.004 · doi ↗
- 7Sereewisai B. Chintavalakorn R. Santiwong P. Nakornnoi T. Neoh S.P. Sipiyaruk K. The Accuracy of Virtual Setup in Simulating Treatment Outcomes in Orthodontic Practice: A Systematic Review BDJ Open 202394110.1038/s 41405-023-00167-337640693 PMC 10462720 · doi ↗ · pubmed ↗
- 8Li Y. Zhou L. Chen M. Du Y. Gan Y. Li B. Feng J. Accuracy of Digital Indirect Bonding Technology for Customized Orthodontic Brackets Based on Personalized Typodonts BMC Oral Health 20252547810.1186/s 12903-025-05777-x 40181340 PMC 11966935 · doi ↗ · pubmed ↗