Psychometric Validation of the Community Antimicrobial Use Scale (CAMUS) in Primary Healthcare and the Implications for Future Use
Nishana Ramdas, Natalie Schellack, Corrie Uys, Brian Godman, Stephen M. Campbell, Johanna C. Meyer

TL;DR
This study validated a tool to measure community antimicrobial use in South Africa, showing it works well for tracking knowledge and misuse.
Contribution
The study provides a validated psychometric tool for assessing antimicrobial use in African primary healthcare settings.
Findings
CAMUS has a five-factor structure with strong reliability in knowledge and misuse domains.
The tool shows good construct validity with correlations to health literacy and appropriate use intentions.
Measurement error metrics suggest the tool is suitable for group-level comparisons.
Abstract
Background/Objectives: Patient-level factors strongly influence antimicrobial resistance (AMR) through the pressure applied to healthcare professionals to prescribe antibiotics even for self-limiting viral infections, enhanced by knowledge and attitude concerns. This includes Africa, with high levels of AMR. However, validated measurement tools for African primary healthcare (PHC) are scarce. This study evaluated the reliability, structural validity, and interpretability of the Community Antimicrobial Use Scale (CAMUS) in South Africa. Methods: A cross-sectional survey was conducted with 1283 adults across 25 diverse public PHC facilities across two provinces. The 30-item theory-based tool underwent exploratory and confirmatory factor analysis (EFA/CFA), reliability, and validity testing. Results: EFA identified a coherent five-factor structure: (F1) Understanding antibiotics; (F2)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
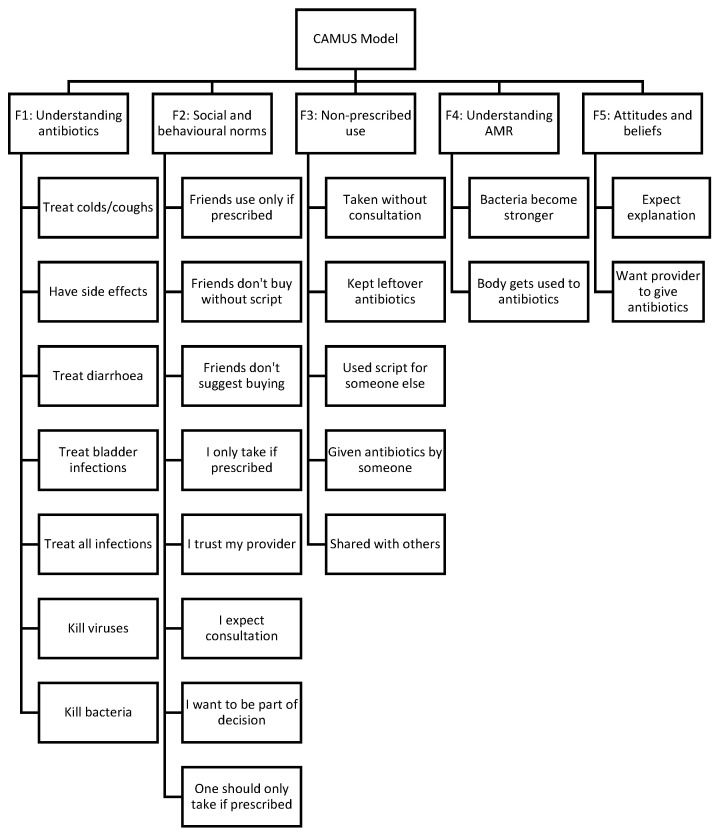 Figure 1
Figure 1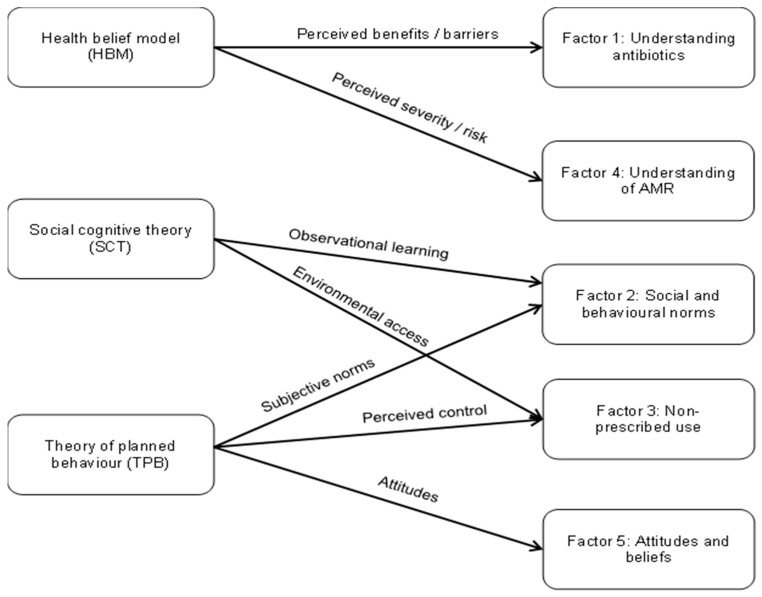 Figure 2
Figure 2| Step | Phase/Study Component | Aim | Methods/Key Activities | Main Findings and Outputs | References |
|---|---|---|---|---|---|
|
| Scoping review of patient-level drivers of | To identify knowledge, attitudes, motivations, | Systematic scoping | Widespread misconceptions about antibiotic effectiveness (e.g., for viral infections), strong patient expectations for | [ |
|
| Tool | To develop a | Item generation based on scoping review findings; expert review; mapping of items to constructs from the Theory of Planned Behaviour (TBP), Health Belief Model (HBM) and Social Cognitive Theory (SCT); iterative refinement for content validity | Draft 30-item CAMUS | [ |
|
| Pilot study of CAMUS in PHC patients | To assess feasibility, clarity and | Administration of | CAMUS was feasible in clinic workflows (mean completion time ≈10 min) and acceptable to patients. Pilot data showed marked misconceptions (e.g., 93.3% believed antibiotics treat colds/coughs; 43.3% recognised that overuse causes resistance) and led to refinement of 28 items for clarity. | [ |
|
| Large-scale | To evaluate reliability, structural validity and interpretability | Cross-sectional survey of 1283 adult PHC | Five-factor structure reflecting knowledge, social and | Current study |
| Psychometric | Analysis Performed | Statistical Method/Criteria | Purpose |
|---|---|---|---|
| Descriptive statistics | Frequencies, percentages, means, standard deviations | Distributional summaries of items and domain scores | To characterise the sample |
| Internal consistency reliability | Cronbach’s alpha | α ≥ 0.70 considered | To assess internal consistency of |
| Test–retest reliability | ICC | Two-way mixed-effects model, absolute agreement; interpreted per Koo and Li [ | To assess temporal stability over |
| Sampling adequacy | KMO measure | KMO ≥ 0.60 | To assess suitability of data for |
| Sphericity | Bartlett’s Test of Sphericity | To confirm sufficient inter-item | |
| Data transformation | CatPCA | Transformation of nominal and ordinal variables | To accommodate mixed item |
| Exploratory factor analysis | Principal axis factoring | Eigenvalues > 1.0 and | To explore underlying factor |
| Confirmatory factor analysis | Reliability and validity | CR, AVE, Cronbach’s alpha | To assess convergence and |
| Subgroup analysis | Multi-group CFA | Not performed; subgroup | To document rationale for not |
| Construct validity | Correlation analysis | Pearson’s correlation | To assess associations with health |
- —National Research Foundation of South Africa
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Health Literacy and Information Accessibility · Infection Control in Healthcare
1. Introduction
Antimicrobial resistance (AMR) represents a major and growing threat to global health security, potentially becoming the next pandemic [1,2,3]. This is especially the case among low-and middle-income countries (LMICs), including African countries, where infectious disease rates remain high and access to appropriate care and antibiotic stewardship is limited [4,5,6,7]. The diminishing efficacy of existing antimicrobial agents compromises the ability to treat common infections effectively, leading to increased morbidity, mortality, and healthcare costs [4,5,8,9,10,11,12].
AMR is driven by a number of factors especially among LMICs. These include high infectious disease prevalence rates, limited diagnostic capacity, suboptimal antibiotic prescribing and dispensing practices, and challenges in regulating access to medicines [2,5,13,14,15]. A primary driver of AMR in LMICs is the inappropriate use of antimicrobials especially in ambulatory care [8,13,16,17,18,19]. Primary healthcare (PHC) facilities are a central point of care for many patients in LMICs seeking treatment from physicians or nurses [8,16,20,21]. However, care-seeking pathways are often pluralistic, and patients, particularly for self-limiting infectious conditions in LMICs, may first consult community pharmacists or informal providers before attending PHC services as there can be challenges with access to PHC facilities [14,20,21,22,23].
PHC facilities in LMICs typically face high patient workloads, compounded by physician shortages, particularly in rural areas [5,8,22]. Alongside this, there can be variable prescribing oversight and strong patient expectations for antibiotics even for self-limiting conditions [2,8,13,14,24]. In South Africa, AMR is recognised as an increasing national priority with mortality directly attributed to resistant infections, now surpassing mortality rates from several other major causes [25,26]. This highlights the urgent need for robust, context-specific interventions in South Africa, especially given ongoing concerns with the current lower priority given by the Ministry of Health to the prevention of, and reduction in, AMR in the country [25,26,27,28].
Globally, up to 95% of human antibiotic consumption in LMICs occurs in primary care [19]. Consequently, primary care is a key focus for any national activities to improve future prescribing and reduce AMR [5,8,18,29,30]. In South Africa, PHC facilities typically serve as the first point of contact for most of the population with both infectious and non-infectious diseases [20,21]. There is currently limited if any informal providers in South Africa unlike other LMICs, which includes other African countries [23,31,32,33]. However, as detailed in Supplementary Table S1, published studies, coupled with our own preliminary audit of the study sites, have consistently documented high rates of inappropriate antibiotic prescribing among PHC facilities in South Africa, often for self-limiting viral conditions where they offer no clinical benefit [21,34,35,36,37,38,39,40]. This clinical pattern, where prescribing frequently deviates from guidelines, suggests that non-clinical factors, such as patient pressure and expectations, play a substantial role. These findings directly informed the development of the Community Antimicrobial Use Scale (CAMUS) items, specifically those investigating patient entitlement and the social norms that drive demand for antibiotics.
Patient-level factors do exert significant influence on antibiotic utilisation patterns especially in LMICs [8]. Patients’ knowledge (or lack thereof) about antibiotics, their attitudes towards illness and treatment, personal motivations, expectations regarding consultations, and subsequent health behaviours, all shape demand for, and use of, antibiotics [8,24,41]. Published studies among LMICs, including those from South Africa, indicate that patients frequently pressure clinicians to prescribe antibiotics, enhanced by a misunderstanding of appropriate indications for antibiotics, e.g., believing antibiotics can treat coughs and colds (Table 1 and Supplementary Table S1) [8,41,42].
Despite the widely acknowledged importance of patient perspectives, antimicrobial stewardship (AMS) initiatives in South Africa, alongside many other LMICs, have traditionally focused on hospital settings rather than community settings [5,43,44,45]. However, we are beginning to see more antibiotic stewardship programmes (ASPs) being undertaken among prescribers across LMICs to improve future antibiotic use [8,46]. Having said this, potential AMS interventions targeting patients or the community often lack an evidence base regarding the specific behavioural drivers prevalent in local contexts [8,41]. A major impediment has been the absence of validated, reliable, and culturally appropriate measurement tools designed to capture the multifaceted nature of patient knowledge, attitudes, motivations, and expectations related to antibiotic use, particularly within African healthcare systems [41].
While numerous studies have assessed these factors, they overwhelmingly rely on descriptive knowledge, attitudes, and practices (KAP) surveys [8,15]. As our previously published scoping review confirmed, these existing instruments generally lack a foundation in behavioural theory and have not undergone rigorous psychometric validation [41]. Consequently, the critical gap is not a lack of surveys, but a lack of validated, theory-driven tools. Unlike traditional KAP surveys, which typically offer descriptive snapshots of isolated variables, CAMUS aims to measure the underlying latent constructs, including social pressure and entitlement, that drive behaviour. By moving beyond simple frequency reporting to psychometric structural analysis, CAMUS should offer a reproducible tool to identify the specific behavioural levers requiring intervention [8,41].
Overall, understanding patients’ perspectives is fundamental to designing interventions in South Africa and across LMICs that resonate with community members and effectively modify behaviour. To address this critical need, we conducted a multi-phase research project aimed at developing and validating the CAMUS. The phases, methods, and key findings are summarised in Table 2.
Briefly, the scoping review synthesised global evidence on patient-level drivers of antimicrobial use and highlighted major gaps in theory use and psychometric validation of existing instruments. These findings informed item generation and tool development, which were also guided by the Theory of Planned Behaviour (TPB), the Health Belief Model (HBM) and Social Cognitive Theory (SCT) [47,48]. A pilot study in PHC settings in South Africa subsequently tested the CAMUS for its feasibility, clarity and acceptability, and identified substantial baseline misconceptions and areas for item refinement [49].
While the pilot study established feasibility and content validity, it lacked the statistical power to validate the instrument’s structure. Consequently, the present study was designed as a large-scale psychometric validation. The primary objective was to rigorously evaluate the reliability, structural validity and interpretability of the CAMUS in a large, diverse sample of South African PHC patients. As a result, we sought to establish its suitability as a measure for research and programme evaluation. We chose PHC facilities for this initial study as there had been variable findings regarding the purchasing of antibiotics without a prescription in South Africa. A number of studies at the time of the development of CAMUS suggested little or no purchasing of antibiotics without a prescription [50,51]. However, others demonstrated some purchasing of antibiotics without a prescription, although typically not for self-limiting viral conditions such as upper respiratory tract infections [52].
2. Results
2.1. Participant Characteristics
A total of 1283 participants were enrolled and completed the CAMUS questionnaire. The demographic profile of the sample is summarised in Table 3.
The majority of participants were female (59.3%), and the largest age groups were 20–29 years (34.3%) and 30–39 years (24.2%). Participants primarily identified themselves as African (89.4%) and residing in townships (46.2%) or rural areas (30.2%). Educational attainment varied, with 46.0% having completed high school. In total, 42.1% of the sample was employed, while 35.5% reported being unemployed.
2.2. Phase 1: Exploratory Factor Analysis (EFA) and Test–Retest Reliability
The dataset was suitable for factor analysis (KMO = 0.867; Bartlett’s Test of Sphericity χ^2^(435) = 10,751.464; p < 0.001). EFA was conducted on the 30 CAMUS items following categorical principal components transformation. Principal axis factoring with Promax rotation identified a five-factor solution that aligned well with the theoretical domains specified in advance. Box 1 contains the final structure of CAMUS.
Box 1Final factor structure of the CAMUS.
- F1. Understanding of antibioticsGeneral knowledge regarding indications, effectiveness, and side effects of antibiotics.
- F2. Social and behavioural norms related to antibiotic usePerceived family, community, and social influences shaping antibiotic use behaviours.
- F3. Non-prescribed use Informal practices including sharing, storing, and using antibiotics without prescription.
- F4. Understanding of AMRKnowledge of resistance mechanisms and consequences of inappropriate antibiotic use.
- F5. Attitudes and beliefs toward antibioticsExpectations, entitlement beliefs, and attitudes influencing demand for antibiotics.
This structure explained a substantial proportion of the variance and showed clear conceptual coherence: F1 captured core knowledge about indications and mechanisms; F2 grouped items on family and community norms and interactions with providers; F3 captured informal or non-prescribed use; F4 measured AMR-specific knowledge; and F5 encompassed expectations and entitlement beliefs. The rotated pattern matrix and corresponding factor loadings for this five-factor solution are presented in Table 4.
Internal consistency for these exploratory factors was also explored:
- F1 Understanding of antibiotics: α = 0.806 (7 items).
- F2 Social and behavioural norms: α = 0.767 (9 items).
- F3 Non-prescribed use: α = 0.801 (6 items).
- F4 Understanding of AMR: α = 0.798 (3 items).
- F5 Attitudes and beliefs: α = 0.542 (3 items).
Consequently, three constructs (F1, F3, F4) showed good internal consistency. F2 showed acceptable to good reliability for a broad social construct, whilst F5 demonstrated marginal reliability in this preliminary phase due to both construct breadth and low item numbers (n = 3).
As part of the refinement process, five Likert items (Items 1, 2, 5, 14, and 19) were removed prior to conducting the CFA due to low communalities (<0.30), cross-loadings <0.30 on multiple factors, or conceptual ambiguity (weak primary factor loadings <0.40). Their removal improved the coherence of the factor structure without compromising theoretical coverage.
Test–retest reliability, based on a subsample of 69 participants re-assessed after 5–7 days, was good to excellent across the CAMUS domains (Table 5), with ICCs ranging from 0.72 (Attitudes and beliefs) to 0.89 (Understanding of AMR). Table 4 contains details of the rotated pattern matrix and factor loadings for the five-factor EFA solution.
2.3. Phase 2: Confirmatory Factor Analysis (CFA)
The final CFA model structure is illustrated in Figure 1. The model comprises five latent factors: Understanding of antibiotics (F1); Social and behavioural norms (F2); Non-prescribed use (F3); Understanding of AMR (F4); and Attitudes and beliefs (F5).
Table 6 summarises the CFA-based reliability and convergent validity indices. Three constructs (F1, F3, F4) achieved CR ≥ 0.79 with alpha ≥ 0.67, indicating good internal consistency and composite reliability (CR). F2 and F5 had CR in the 0.63–0.67 range and alpha around 0.62–0.73, which is acceptable for early-stage behavioural scales, particularly for shorter subscales.
For broad social/behavioural domains, average variance extracted (AVE) values were below 0.50 for F1, F2, and F3, while F4 (Understanding of AMR) showed excellent convergent validity (AVE = 0.737), and F5 approached the conventional 0.50 threshold (AVE = 0.471). While AVE values for the social and behavioural norm factors (F1, F2, F3) were below the strict threshold of 0.50, the CR for these constructs exceeded 0.60. According to the divergent validity criteria established by Fornell and Larcker (1981) [47], an AVE less than 0.50 is acceptable provided that the CR is higher than 0.60, indicating that the convergent validity of the construct is still adequate.
2.4. Construct and Convergent Validity
Construct validity was supported by associations with theoretically related variables. Among the subsample who completed the health literacy test (HELT-LL, n = 463), CAMUS factor scores correlated moderately and positively with health literacy (r = 0.48, p < 0.001) and with self-reported intentions to use antibiotics appropriately (e.g., finish prescribed courses, avoid use without prescription; r = 0.42, p < 0.01). Participants with higher health literacy demonstrated better antibiotic knowledge and more appropriate attitudes and intentions, consistent with expectations.
2.5. Interpretability and Measurement Error
Measurement error was calculated for each factor independently to account for the multidimensional nature of the scale. As shown in Table 6, the standard error of measurement (SEM) and smallest detectable change (SDC) varied across domains. The average SEM across all factors was 1.59, and the average SDC was 4.40. Using the criterion that acceptable precision requires SEM ≤ SD/2 [54], factors F1 (Understanding antibiotics), F3 (Non-prescribed use), and F4 (Understanding of AMR) demonstrated acceptable precision. However, F2 (Social and behavioural norms) and F5 (Attitudes and beliefs) exhibited higher measurement error (SEM > SD/2), indicating that scores in these specific social-attitudinal domains are subject to greater random variation and should be interpreted with caution at the individual level.
3. Discussion and Next Steps
This study provides a large-scale psychometric evaluation of the CAMUS, a theory-informed instrument developed to measure patient-level drivers of antimicrobial use in South African PHC settings. This builds on the findings from the pilot study, which demonstrated that the CAMUS was feasible and acceptable for use in PHC clinics, with a mean completion time of approximately 10 min [49]. The pilot study also revealed substantial baseline misconceptions regarding antibiotic use, including a high prevalence of incorrect beliefs about antibiotics treating viral infections [49]. Alongside this, the pilot study also identified marginal health literacy as common among PHC attendees and highlighted the influence of patient expectations and social and behavioural norms on antibiotic-seeking behaviour, informing item refinement prior to large-scale validation [49]. Using data from 1283 PHC users, the present study systematically assessed the instrument’s dimensionality, reliability, validity, and interpretability.
3.1. Behavioural Structure of Antimicrobial Use
The EFA and subsequent CFA confirmed that antimicrobial use behaviour among PHC patients is multidimensional. The refined model comprises five inter-related but distinct constructs: Understanding of antibiotics; Social and behavioural norms; Non-prescribed use; Understanding of AMR; and Attitudes and beliefs towards antibiotics. This structure is consistent with both the scoping review and the behavioural frameworks underpinning CAMUS. The emergence of distinct factors for ‘understanding antibiotics’ (F1) and ‘social and behavioural norms’ (F2) empirically supports our theoretical integration. This confirms that patients distinguish between the cognitive beliefs derived from the HBM and the social pressures described in SCT and TPB as visualised in our theoretical framework. As a result, reinforces the fact that antibiotic-related behaviour is not reducible to knowledge alone [41,48,55].
The separation of knowledge, social and behavioural norms, misuse practices, AMR understanding, and attitudes/expectations supports a more nuanced view of antibiotic use than traditional KAP surveys. The findings show that patients may simultaneously hold accurate knowledge about some aspects of antibiotics, e.g., their side effects, while maintaining misconceptions about viral infections or engaging in informal sharing and storage. This complexity mirrors reported findings from other LMIC contexts [8] but with greater structural resolution. For example, Nepal et al. (2019) reported that 47.7% of community members in the Rupandehi District of Nepal believed antibiotics help recovery from colds and coughs [56], while a systematic review by Torres et al. (2019) found that misconceptions regarding viral infections in LMICs vary widely [57]. There were similar findings in the reviews of Belachew et al. (2021), Yeika et al. (2021) and Saleem et al. (2025) [8,15,58,59]. Some studies in the review of Torres et al. reported misconception rates as high as 80% [57]. This places the current study’s finding (76.5%) at the upper end of global concern. Unlike the unitary measures often used in these reviews, the CAMUS structurally separates these knowledge deficits from social drivers, offering a more nuanced target for intervention. This emphasises the need for multi-component interventions when looking to improve antibiotic use in primary care.
Despite the statistical distinction between the factors, we acknowledge the conceptual proximity between social and behavioural norms (F2) and attitudes and beliefs (F5), as individual expectations are often shaped by broader societal narratives. However, retaining them as separate domains does appear to be behaviourally critical to guide future ASPs. Social and behavioural norms (F2) capture the extrinsic pressure to conform to group behaviour (e.g., ‘my family expects me to get antibiotics’), whereas attitudes and beliefs (F5) capture the intrinsic sense of entitlement and urgency, e.g., ‘I have a right to demand treatment’. Differentiating between patients acting out of social compliance versus those acting out of personal entitlement leads to future ASPs being based on the most appropriate levers; i.e., utilising community-wide messaging to shift norms versus for instance training clinicians in conflict resolution to manage individual entitlement during consultations.
3.2. Reliability and Internal Consistency
Reliability analysis demonstrated that the CAMUS performs best in domains where constructs are more concrete and behaviourally specific. Understanding of antibiotics (F1), non-prescribed use (F3), and understanding of AMR (F4) all showed good internal consistency (α ≈ 0.80) and strong composite reliability. As a result, indicating these domains can be used confidently in future research and programme evaluations.
When evaluated against the conventional threshold of α ≥ 0.70, the social and behavioural norms domain (F2) showed acceptable reliability (α = 0.732; CR = 0.672). However, the shorter attitudes and beliefs construct (F5) demonstrated marginal reliability (α = 0.619; CR = 0.635). It is important to remind readers, including researchers, that reliability coefficients are inherently sensitive to scale length and construct breadth; shorter scales often yield lower alpha values even when the underlying construct is valid. In this context, while the F5 value falls below the 0.70 standard, Hair et al. (2019) [60] note that values between 0.60 and 0.70 are acceptable in exploratory research, particularly for newly developed scales. We attribute this lower value to the sensitivity of Cronbach’s alpha to the number of items, e.g., Factor 5 contains only two items in the final model alongside the broad nature of ‘entitlement beliefs’.
Consequently, we do not claim full psychometric adequacy for this specific subscale in its current form. Instead, these results indicate that F5 requires item expansion. Specifically, adding items related to patient entitlement and expectations, to improve internal consistency in future iterations.
The good to excellent test–retest reliability (ICC 0.72–0.89) provides further evidence that CAMUS domains are stable over short periods, supporting their development and future use for monitoring and evaluating future ASP interventions.
3.3. Confirmatory Factor Analysis and Construct Validity
The CFA did not simply replicate the exploratory structure but refined it. Splitting the broad social/behavioural factor into a norms construct and a compact attitudes and beliefs construct improved structural coherence, while retaining alignment with TPB, HBM, and SCT. The resulting five-construct model is theoretically consistent and empirically supported at the factor-level.
We acknowledge that the AVE values for the social and behavioural norms (F2), non-prescribed use (F3), and attitudinal (F5) domains fell below the standard threshold of 0.50 (Table 6). This indicates that the variance captured by these latent constructs is lower than the variance attributable to measurement error. However, the CR for these constructs exceeded 0.60. According to the criterion established by Fornell and Larcker (1981) [47], convergent validity is considered adequate when CR is sufficient, even if AVE falls below 0.50. This suggests that, while the items in these broad behavioural domains are heterogeneous, they share sufficient common variance to be reliable as a composite measure.
Nevertheless, we interpret these domains as developmental rather than fully adequate. The measurement properties observed here, specifically the lower variance in social domains compared to knowledge domains, mirror the findings from other health behaviour instruments validated in African settings, such as HIV adherence scales. This reflects the inherent complexity of capturing multifaceted social drivers relative to fixed knowledge traits. Consequently, these specific subscales should be viewed as preliminary indicators suitable for identifying broad group-level trends, rather than precise diagnostic tools for individuals. Achieving robust convergent validity in these social and attitudinal domains will require future refinement, specifically the generation of more homogenous items to better capture the ‘perceived entitlement’ and ‘social pressure’ constructs.
Construct validity was reinforced through moderate correlations with health literacy and antibiotic-use intentions, showing that CAMUS scores behave as theoretically expected. Participants who understand health information better are also more likely to score higher on knowledge, appropriate attitudes, and intentions regarding antibiotic use.
3.4. Interpretability and Intended Use
The absence of floor/ceiling effects, the near-normal distribution of total scores, and the low SEM/SDC values collectively support the interpretability of CAMUS scores. The instrument is sensitive enough to distinguish levels of antibiotic-related knowledge and behaviour across a broad PHC population and to detect meaningful shifts at the group level, for example, before and after public awareness campaigns or stewardship interventions. This psychometric capability distinguishes the CAMUS from descriptive surveillance tools, such as the WHO Multi-Country Public Awareness Survey [61]. While the WHO instrument provides valuable aggregate prevalence data for global benchmarking, it was not designed as a scalar instrument to measure individual-level behavioural change over time. By providing validated score distributions and cut-offs, the CAMUS fills this methodological gap, offering a mechanism to evaluate the specific impact of stewardship interventions in a way that descriptive surveys cannot.
At the same time, measurement error estimates suggest caution when interpreting small changes at the individual level. The CAMUS is best understood as a surveillance and research tool for population-level monitoring and evaluation, rather than as a diagnostic instrument for individual clinical decision-making. This distinction is important and should guide how the tool is deployed in practice in the future to help target specific AMS activities to improve future antibiotic use.
3.5. Implications for Policy, Practice, and Patient Engagement
The validated structure and reliability of the CAMUS have several implications as demonstrated in Table 7.
3.6. Future Directions and Next Steps
Table 8 summarises the validation of the findings to date and the next steps to take the CAMUS forward.
3.6.1. Instrument Refinement
The immediate next step is a detailed item-level review of the CFA and EFA data. This analysis will form the basis for future instrument development.
This involves identifying and revising or excluding items that showed low factor loadings, high cross-loadings, or contributed to weaker reliability and convergent validity, particularly within the social/behavioural norms (F2) and attitudes and beliefs (F5) domains. For Factor 5, the marginal reliability suggests that the current two items are insufficient to fully capture the construct. Future development will involve generating 3–5 additional items focusing on ‘perceived rights to healthcare’ and ‘expectations of speed of recovery’ to strengthen the homogeneity and reliability of this domain.
The goal is to develop a shorter, more streamlined and psychometrically stronger refined iteration of CAMUS that preserves the well-performing knowledge, AMR and misuse domains whilst seeking to improve measurement precision for social and attitudinal constructs.
3.6.2. Operationalization in Future ASPs
To improve translational relevance, the CAMUS is designed to be operationalized within routine ASPs in three distinct ways:
- Diagnostic triage: Facility managers can use the scale to identify which specific driver is problematic in their catchment area. For example, a facility scoring low on understanding of antibiotics (F1) would benefit from direct patient education, e.g., posters, and pamphlets, whereas a facility scoring high on social and behavioural norms (F2) would require broader community engagement campaigns to appreciably change societal expectations.
- Benchmarking: Districts can use the CAMUS to benchmark facilities against one another, identifying ‘hotspots’ of high patient entitlement (F5) that may require additional support for clinicians in conflict resolution.
- Impact evaluation: As a validated measure with known sensitivity, CAMUS can potentially serve as a pre- and post-intervention assessment tool to quantify the effectiveness of public health campaigns.
3.6.3. Re-Validation
Once a refined version of the instrument is proposed, it must be subjected to a new, full validation study on an independent dataset. This new validation must repeat the entire process, i.e., EFA to identify the new factor structure, followed by a CFA to confirm it. The aim is to produce a final, validated tool that achieves acceptable model fit, strong internal consistency (alpha > 0.7), and good convergent validity (AVE > 0.5).
3.6.4. Future Use in South Africa (Post-Refinement)
The future application of CAMUS following refinement and validation can be summarised across three key areas, as outlined in Table 9:
The 30-item CAMUS represents essential groundwork for measuring community antimicrobial use. These validation findings provide the foundation for a refined, psychometrically promising tool suitable for future surveillance and intervention planning.
3.7. Strengths and Limitations
3.7.1. Strengths
This study contributes to the field by offering a psychometrically validated instrument specifically tailored to the resource-limited context of South African primary care. Unlike many existing KAP surveys, the CAMUS is grounded in established behavioural theory (TPB, HBM, SCT), allowing for a structural analysis of the drivers of antibiotic use rather than simple descriptive reporting. The large sample size (n = 1283) and the inclusion of diverse demographic groups across two provinces strengthen the stability of the factor structure. Furthermore, the calculation of measurement error metrics (SEM/SDC) provides practical benchmarks for future interventional research.
3.7.2. Limitations
We are aware that several limitations should be noted. While reliability at the factor level was generally acceptable, convergent validity was suboptimal for some behavioural constructs, reflecting conceptual breadth and indicating a need for further item refinement. The cross-sectional design also precluded assessment of predictive validity and responsiveness to change; these measurement properties will require longitudinal and pre–post intervention studies. Reliance on self-reported behaviours introduces the potential for social desirability bias, particularly for socially undesirable practices such as sharing leftover antibiotics or stopping treatment early. In addition, sample sizes within certain demographic subgroups, especially participants with very low education levels, were insufficient to support multi-group confirmatory factor analysis, limiting the assessment of measurement invariance across education categories.
Finally, the administration of the CAMUS exclusively in English represents a significant limitation given the rich socio-linguistic diversity of South Africa and the wider African continent. While English was chosen to ensure standardisation during this initial validation phase, this likely introduced a selection bias favouring participants with higher functional literacy and English proficiency. Consequently, our findings may not fully capture the extent of misconceptions or specific cultural drivers of antibiotic use present in non-English speaking sub-populations. Future research must prioritise the translation, cultural adaptation, and validation of the CAMUS into indigenous languages (e.g., isiZulu, Setswana) to ensure the tool is inclusive and truly representative of the PHC population in South Africa.
4. Methods
This study employed a cross-sectional survey design for the psychometric validation of the CAMUS instrument, building on the findings from the pilot study.
4.1. The CAMUS Instrument
The development of the CAMUS was grounded in an integrated framework drawing on the TPB, the HBM, and SCT as described in Ramdas et al. (2025) [49]. These theories were selected as complementary lenses to capture the multidimensional nature of antibiotic use. While the TPB maps the path from attitude to intention, it often overlooks specific knowledge gaps. In view of this, we integrated the HBM into our approach to help capture cognitive misconceptions, e.g., ‘antibiotics cure flu’, that drive perceived benefits.
To account for environmental and social learning prevalent in South African communities, e.g., sharing leftover antibiotics, we incorporated SCT constructs, which map directly to the social and behavioural norms and non-prescribed use domains. Figure 2 illustrates how these theoretical constructs were explicitly mapped to the final CAMUS factors.
The diagram illustrates the integration of theoretical constructs into the final factor structure. Arrows indicate hypothesised directional relationships between theoretical constructs and CAMUS domains. The figure though does not represent a causal model. The HBM informed the cognitive domains regarding risk and antibiotic function (Factors 1 and 4). SCT and the TPB informed the behavioural and social domains, linking observational learning and subjective norms to Factor 2, and environmental access and perceived control to Factor 3. Attitudes (TPB) mapped directly to Factor 5.
In summary, the instrument comprises five core domains designed to capture patient perspectives on AMU (Table 10).
4.2. Validation Study Design and Sample
The main validation survey was conducted between August 2024 and September 2025. Participants were adult patients (aged 18 years or older) attending routine (non-urgent) consultations at 25 public PHC facilities. These sites were purposively selected from geographically distinct areas within two provinces (urban, peri-urban, and semi-rural) to build upon the findings from the pilot study, and to capture a diverse patient population representative of the South African PHC setting. The two provinces chosen were Gauteng and Limpopo.
This study focused on PHC facilities within the public health sector, as they are the first point of contact for most South Africans and the primary source of prescribed antibiotics. Whilst we are aware that there are sales of antibiotics without a prescription among community pharmacies in South Africa, the literature on its prevalence in the country is conflicting [50,51,52]. Most studies prior to the development of the CAMUS showed very low rates of purchasing of antibiotics without a prescription in South Africa [50,51]; however, others have shown higher rates [52]. Given these conflicting findings, coupled with the current illegal nature of such sales, we only targeted public sector PHC clinics to robustly measure patient-prescriber interactions and the behavioural drivers (like expectations and motivations) that influence prescribed antibiotic use.
Consecutive sampling was employed in the waiting areas of PHC clinics. Patients were excluded if they were seeking emergency care. This is because this study focused on routine, non-urgent PHC consultations rather than acute urgent conditions, which would typically be managed at a hospital outpatient department. Patients were also excluded if they were too unwell to participate, unwilling to provide informed consent, or unable to communicate in English. English was used as the language of administration for this initial validation study to ensure standardisation and allow for potential international comparison with English recognised as the universal scientific language. This is a recognised approach, given the linguistic diversity in South Africa, and validated translations are a recommended next step.
A total of 1283 participants meeting the inclusion criteria provided informed consent and were enrolled. This sample size comfortably exceeds the standard recommendation of at least 10 participants per scale item, providing sufficient statistical power for robust factor analysis.
4.3. Data Collection Procedures
Trained fieldworkers administered the CAMUS questionnaire in English via face-to-face interviews lasting approximately 10–15 min. Responses were captured directly onto electronic tablets using Google Forms. Demographic information was also collected.
For the assessment of test–retest reliability, a randomly selected subsample of 69 participants from one site was asked to complete the CAMUS questionnaire a second time 5 to 7 days after the initial administration.
Additionally, a subset of participants (n = 463) completed the Health Literacy Test for Limited Literacy Populations (HELT-LL), previously validated in South Africa, to provide an external criterion for assessing construct validity.
4.4. Statistical Analysis
Data were analysed using IBM SPSS Statistics for Windows, Version 30.0 (IBM Corp., Armonk, NY, USA). Table 11 summarises the statistical analyses undertaken to evaluate the psychometric properties of CAMUS. Detailed formulas and citations for the derivation of measurement error metrics (SEM and SDC) are provided in Supplementary Box S1.
4.5. Ethical Considerations
The study protocol was approved by the Sefako Makgatho University Research Ethics Committee (SMUREC/P/220/2023:PG). Permissions were obtained from the relevant Provincial Departments of Health. Participation was entirely voluntary. Fieldworkers explained the study purpose, procedures, confidentiality measures, and the right to withdraw at any time without consequence. Written informed consent (or witnessed verbal consent for participants unable to write) was obtained from every participant before enrolment (Supplementary Table S2). Data were anonymized using unique study identifiers, and electronic data were stored securely on password-protected servers accessible only to the core research team.
5. Conclusions
This study presents a rigorous, large-scale psychometric evaluation of the CAMUS among PHC patients in South Africa. The instrument demonstrates a coherent five-factor structure grounded in behavioural theories, good internal consistency for core knowledge and misuse domains, acceptable reliability for social and attitudinal domains, good to excellent test–retest stability, and supportive evidence of construct validity via associations with health literacy and antibiotic-use intentions.
Measurement error and distributional properties indicate that CAMUS is well suited to group-level assessment, surveillance, and evaluation of patient-level drivers of antibiotic use, while small individual-level changes should be interpreted with caution. The weaker convergent validity and lower reliability in some behavioural domains identify clear targets for item refinement and future scale development.
CAMUS emerges as a psychometrically promising, contextually relevant tool that can support more behaviourally informed ASP activities in South African PHC settings and, with further adaptation, in other LMIC settings. Future work should focus on item refinement in social and attitudinal domains, translation and cultural validation in major local languages, testing in diverse geographical settings, and longitudinal use to assess responsiveness to stewardship interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patra M. Gupta A.K. Kumar D. Kumar B. Antimicrobial Resistance: A Rising Global Threat to Public Health Infect. Drug Resist.2025185419543710.2147/IDR.S 53055741158783 PMC 12558087 · doi ↗ · pubmed ↗
- 2Totaro V. Guido G. Cotugno S. De Vita E. Asaduzzaman M. Patti G. Segala F.V. Putoto G. Frallonardo L. Farkas F.B. Antimicrobial Resistance in Sub-Saharan Africa: A Comprehensive Landscape Review Am. J. Trop. Med. Hyg.202511325326310.4269/ajtmh.25-003540393439 PMC 12360106 · doi ↗ · pubmed ↗
- 3Gautam A. Antimicrobial Resistance: The Next Probable Pandemic JNMA J. Nepal. Med. Assoc.2022602252283521063410.31729/jnma.7174 PMC 9200017 · doi ↗ · pubmed ↗
- 4Murray C.J. Ikuta K.S. Sharara F. Swetschinski L. Aguilar G.R. Gray A. Han C. Bisignano C. Rao P. Wool E. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis Lancet 202239962965510.1016/s 0140-6736(21)02724-035065702 PMC 8841637 · doi ↗ · pubmed ↗
- 5Loosli K. Davis A. Muwonge A. Lembo T. Addressing antimicrobial resistance by improving access and quality of care-A review of the literature from East Africa P Lo S Negl. Trop. Dis.202115 e 00095293429293210.1371/journal.pntd.0009529 PMC 8297743 · doi ↗ · pubmed ↗
- 6Sartorius B. Gray A.P. Weaver N.D. Aguilar G.R. Swetschinski L.R. Ikuta K.S. Mestrovic T. Chung E. Wool E.E. Han C. The burden of bacterial antimicrobial resistance in the WHO African region in 2019: A cross-country systematic analysis Lancet Glob. Health 202412 e 201e 2163813494610.1016/S 2214-109X(23)00539-9PMC 10805005 · doi ↗ · pubmed ↗
- 7Lewnard J.A. Charani E. Gleason A. Hsu L.Y. Khan W.A. Karkey A. Chandler C.I.R. Mashe T. Khan E.M. Bulabula A.N.H. Burden of bacterial antimicrobial resistance in low-income and middle-income countries avertible by existing interventions: An evidence review and modelling analysis Lancet 20244032439245410.1016/S 0140-6736(24)00862-638797180 · doi ↗ · pubmed ↗
- 8Saleem Z. Moore C.E. Kalungia A.C. Schellack N. Ogunleye O. Chigome A. Chowdhury K. Kitutu F.E. Massele A. Ramdas N. Status and implications of the knowledge, attitudes and practices towards A Wa Re antibiotic use, resistance and stewardship among low- and middle-income countries JAC Antimicrob Resist.20257 dlaf 0334013481510.1093/jacamr/dlaf 033PMC 11934068 · doi ↗ · pubmed ↗