Deep immunophenotyping in aneurysmal subarachnoid hemorrhage: a prospective and controlled clinical study
Björn B. Hofmann, Dilaware Khan, Igor Fischer, Daniel Hänggi, Sajjad Muhammad

TL;DR
This study explores immune cell changes in patients with aneurysmal subarachnoid hemorrhage and finds shifts toward pro-inflammatory cells linked to complications like vasospasm and delayed cerebral ischemia.
Contribution
The study identifies specific immune cell polarization patterns in aSAH patients and links them to clinical complications, suggesting potential for immune profiling as a diagnostic tool.
Findings
Patients with aSAH show decreased anti-inflammatory monocytes and increased pro-inflammatory Th17 cells compared to healthy controls.
Loss of anti-inflammatory monocytes precedes the onset of cerebral vasospasm and delayed cerebral ischemia.
No significant correlation was found between immune cell subpopulations and long-term clinical outcomes.
Abstract
Aneurysmal subarachnoid hemorrhage (aSAH) remains a devastating cerebrovascular condition with significant morbidity and mortality. While inflammation plays a critical role in post-hemorrhagic complications, the specific polarization dynamics of monocyte and T cell subpopulations in this context remain poorly understood. This study aims to investigate these immune cell shifts and their correlation with major complications such as angiographic cerebral vasospasm and delayed cerebral ischemia (DCI). We conducted a prospective, controlled observational single-center cohort study in a neurovascular university center of maximum care in Germany. A total of 75 patients with aSAH and 20 healthy controls were included. Blood samples were collected on days 1, 4, 7, and 11 post-bleeding. Flow cytometry was used to analyze monocyte (M1, intermediate, M2) and T cell (Th1, Th2, Th17, Treg)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
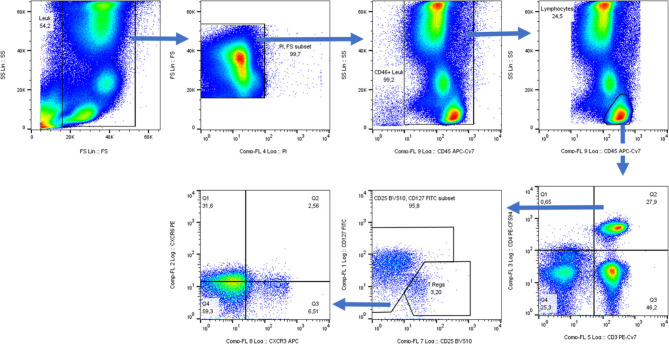 Figure 1
Figure 1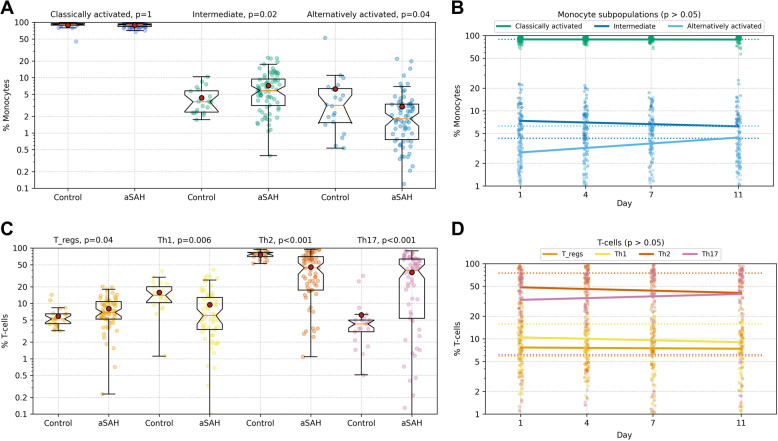 Figure 2
Figure 2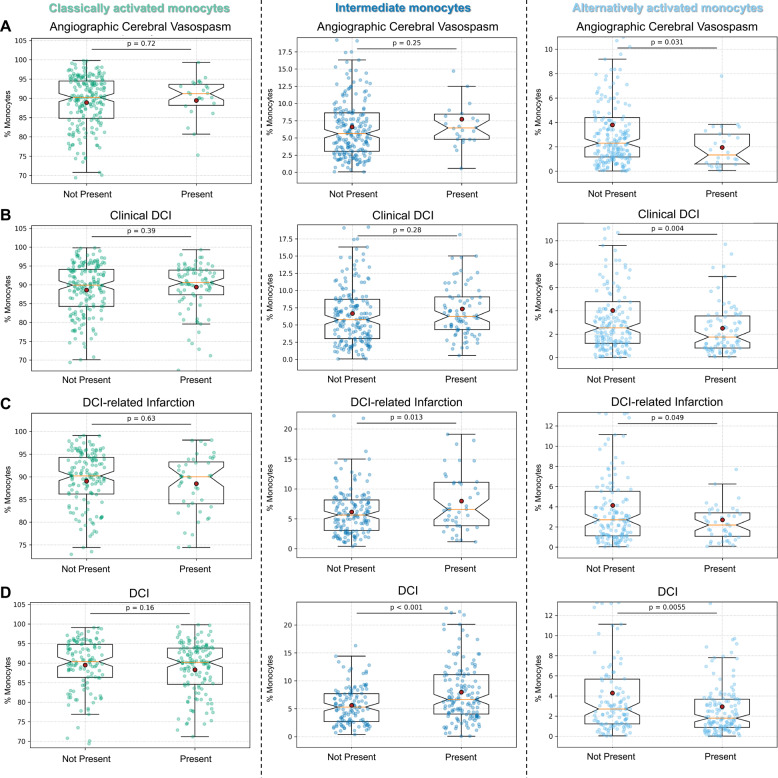 Figure 3
Figure 3- —Universitätsklinikum Düsseldorf. Anstalt öffentlichen Rechts (8911)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Intracerebral and Subarachnoid Hemorrhage Research · Neuroinflammation and Neurodegeneration Mechanisms
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH), accounting for 5% of strokes and predominantly affecting younger patients, remains one of the most severe cerebrovascular diseases, with high morbidity and mortality [1]. The pathophysiology of aSAH is complex [2, 3], involving the phase of early brain injury (EBI) with increased intracranial pressure, brain edema, and impaired perfusion [2–5]. This is followed by the phase of delayed cerebral ischemia (DCI), which involves angiographic cerebral vasospasm, microvascular dysfunction, and microthrombosis, resulting in a more heterogeneous and regional impairment of the brain tissue [2–5]. Despite the seemingly divergent pathophysiological processes, a prominent and consistent factor is becoming increasingly evident in both the early and late phases following aSAH: a sterile inflammation.
Although many studies have focused on detecting inflammatory mediators like cytokines in aSAH, the actual drivers of inflammation appear to be parenchymal brain cells and peripheral immune cells [6–8]. Activated resident microglia, peripheral monocytes and T cells are key in initiating and sustaining the inflammatory response [7, 8]. Studies have shown that markers such as the systemic inflammation response index, CRP levels, C-reactive protein-to-lymphocyte ratio, and the lymphocyte-to-monocyte ratio correlate with outcomes after aSAH [8–13]. Additionally, the lymphocyte-to-monocyte ratio was linked to severe complications like angiographic cerebral vasospasm [9]. As a result, it is increasingly evident that monocytes and T cells, serving as pivotal drivers of inflammation, play a critical role in the inflammatory processes following aSAH.
However, simply analyzing the overall immune cell population is insufficient. Different subpopulations of monocytes (classically activated (M1), intermediate, alternatively activated (M2)) and T cells (Th1, Th2, Th17, Tregs) have distinct pro- or anti-inflammatory effects [14–17], emphasizing the necessity for a detailed examination to comprehensively grasp the inflammatory cascades in aSAH. However, the necessary detailed deep immunophenotyping in a prospective controlled trial, most likely due to the high costs and the high effort required, has not yet been done.
The impact of peripheral monocyte and T cell subpopulations in aSAH, their temporal changes, and their correlation with complications or outcomes remain unclear. Investigating these aspects could offer insights into new therapeutic strategies for reducing aSAH morbidity and mortality. This study aims to explore the polarization of monocytes (classically activated, intermediate, alternatively activated) and T cells (Th1, Th2, Th17, Tregs) in aSAH and their correlation with outcomes and complications like angiographic cerebral vasospasm or DCI, potentially revealing new therapeutic targets.
Materials and methods
Ethical statement
All procedures involving human participants adhered to institutional ethical standards and the 1964 Helsinki Declaration and amendments. The study was approved by the local ethics committee (Medical Faculty, Heinrich-Heine University, Düsseldorf; study ID: 2020 − 1037_1). Written consent was obtained from capable patients immediately, or from authorized representatives for incapacitated patients. Consent from healthy controls was also obtained. The manuscript follows STROBE guidelines.
Inclusion criteria
The study prospectively included all patients with SAH admitted to the neurovascular center from 10/2020 to 07/2022 with (1) SAH confirmed by initial non-enhanced CT, and (2) aneurysm verification by CT angiography and/or digital subtraction angiography. Exclusion criteria: (1) the patient had a known or had a history of infectious disease (to protect laboratory personnel), (2) the patient was admitted more than 24 h after the bleeding event, or (3) the patient or their relatives refused participation in the study.
aSAH management
Patients were managed according to in-house treatment guidelines, previously described in detail [18–22].
Study design and sample collection
Blood samples were collected within 24 h of admission (day 1) and on days 4, 7, and 11. Peripheral arterial, or in rare cases venous, blood samples were taken, totaling 10 ml of EDTA blood each time. The further processing of the samples was carried out within 2 h after sample collection.
Survey of parameters and definitions
Patient characteristics, imaging results, medication, and medical data were recorded on a daily basis.
Definition of primary outcomes
Clinical outcome was assessed at 6 months after hemorrhage using the modified Rankin Scale (mRS) via structured clinical follow-up. The mRS scores were stratified into favorable (0–2), unfavorable (3–5), and death (6).
DCI was defined in accordance with Vergouwen et al. [23] and categorized as either clinical DCI or cerebral Infarction due to DCI.
Clinical DCI was defined as a new focal neurological deficit or a ≥ 2-point drop in GCS lasting >1 h, not immediately following aneurysm treatment, and not explained by other causes after appropriate workup [23].
DCI-related Infarction was defined as a new cerebral infarct on CT or MRI within 6 weeks, not present on early post-treatment imaging, and not attributable to surgical or endovascular intervention [23].
Both subtypes were analyzed individually and as a combined DCI endpoint.
Angiographic cerebral vasospasm was defined as a ≥ 50% vessel narrowing on digital subtraction angiography, either relative to baseline or the contralateral side. No grading of vasospasm severity was performed.
Sample Preparation and FACS analysis
Blood samples from healthy volunteer patients without aneurysms and without infection in the last 2 months were used as controls. To minimize batch effects, all blood samples, both from patients and healthy controls, were drawn in a narrow morning time window and processed using the same standardized protocol by a single trained operator. Briefly, the peripheral EDTA anticoagulated blood (3 ml) was lysed with erythrocyte lysis buffer (Cat# 00–4300−54, Thermo Fisher) at room temperature. After erythrocyte lysis, cells were centrifuged at 350 g for 5 min at 4° C and washed with 2 mL of an ice-cold 10% FBS (Cat# F7524, Sigma Aldrich) in PBS (Cat# 14040091, Thermo Fisher). After washing the cells, cells were resuspended in 1 mL of an ice-cold 10% FBS in PBS. The cells were counted using Trypan blue (Cat# 15250061, Thermo Fisher) and Neubauer chamber and adjusted to a final concentration of 2 million cells per 100 µL ice-cold 10% FBS in PBS. Then, 100 µL aliquots of the cells were dispensed into 5 ml flow cytometry tubes (Lot# 11021083, Corning Science). The panel of anti-human antibodies consisted of CD45, CD14, and CD16 for monocytes and CD45, CD4, CD3, CD127, CD25, CD183, CD186 (CXCR6) for T-cells (antibody details are depicted in Supplementary Tables 1 and 2). Antibody staining of the cells was performed at 4 ° C on ice. After incubation, cells were washed with 2 mL ice-cold 10% FBS in PBS and resuspended in approximately 500 µL of ice-cold 10% FBS in PBS. To discriminate between live and dead cells, 5 µL of Propidium Iodide Solution (Cat# BLD-421301, BioLegend (Via Biozol)) was added to each sample and incubated for 4 min on ice. After that, the samples were washed twice with ice-cold 10% FBS in PBS. The cells were resuspended in 100 µL of an ice-cold 10% FBS in PBS. To fix the cells, 5 µL of 16% PFA was added to each sample. The FACS analysis was performed as early as possible. For both panels, more than 500 thousand events were acquired for stained cells. The data was acquired on CyAn ADP High-Performance Flow Cytometer (Beckman Coulter) using the software Summit 4.3. For details of the gating strategy of the T cell subtypes, see Fig. 1. Monocytes were classified into classical monocytes (CD14 + + CD16-), intermediate monocytes (CD14 + + CD16++) and non-classical monocytes (CD14-CD16++) [24]. Unstained, single-stained, and FMO were used for performing the compensation. Unstained samples were used to assess autofluorescence. Single-stained controls for each fluorochrome were used to construct the compensation matrix and correct for spectral overlap. FMO controls were used for accurate gating. All controls were run under identical instrument settings as the experimental samples. The data was analyzed using FlowJo software version 10.8.1.
Fig. 1FACS gating strategy (T cells)The initial gate was made on the events with consistent flow by bivariate plot of Forward Scatter (FS) and Side Scatter (SS). Then, these events were shown as FS and SS and the gate was used to exclude erythrocytes, platelets and debris. Next the dead cells were excluded based on FS and Propidium Iodide (PI). Then, a bivariate plot of SS vs. CD45 was used to select the CD45 + leucocytes. Further, these events were displayed once again on a bivariate plot of SS vs. CD45 and then, Lymphocytes were selected from these CD45 + events by their low side scatter and high CD45 expression. These lymphocytes were then displayed as CD3 vs. CD4 plot and a quadrant gate was applied. Then, from this quadrant gate CD3 + CD4 + events were selected as CD4 + T cells. CD4 + T cells were then displayed on a CD25 vs. CD127 plot and CD25hiCD127lo events were gated as Tregs. Then, the events other than Tregs were selected and were named as Th cells. These Th cells were further displayed on a bivariate plot of CXCR3 vs. CCR6. Then, a quadrant gate was used to identify CXCR3 + CCR6- cells as Th1, CXCR3- CCR6- cells as Th2 and CXCR3- CCR6 + Th17 cells
Statistical analysis
Clinical data, obtained from the electronic medical records system, were merged with the laboratory data based on the patients’ ID. Laboratory values between different groups were compared using ANOVA if the number of groups was three or more, and using independent samples t-test for two groups. If ANOVA showed significant differences between groups, post-hoc t-test was used to identify the differing group(s). Patient outcome was quantified using modified Rankin scale at discharge and 6 months after bleeding, reduced to three levels: 0–2 = favorable outcome, 3–5 = poor outcome, 6 = death. As the low number of time points and their unequal spacing didn’t allow for time series analysis, the development of laboratory values over time was analyzed using ordinary least squares linear regression. To better model intra-individual trajectories, we additionally employed linear mixed-effects models with patient ID as a random intercept. To adjust for potential confounders in the association between immune profiles and clinical complications, we performed multiple logistic regression analyses with the presence of angiographic cerebral vasospasm, clinical DCI, cerebral infarction due to DCI, or overall DCI as dependent variables. Models included alternatively activated monocytes as the primary independent variable and were adjusted for age, sex, WFNS grade at admission, and modified Fisher grade. Missing data were removed as required for each analysis. To complement p-values and improve interpretability, Cohen’s d effect sizes were calculated for selected group comparisons. All calculations were performed using Python 3.9.7 and the numpy, scipy, and statsmodels packages. The significance level for this study was set to p ≤ 0.05.
Statistical considerations for multiple testing
Due to the exploratory nature of the study, the small sample size, and the high dimensionality and intercorrelation of the immune parameters we decided against applying statistical corrections for multiple testing, like Bonferroni or FDR. Applying such corrections would carry a high risk of type II error and potentially obscure biologically meaningful trends, particularly in a prospective, hypothesis-generating study such as ours. Instead, we focused on consistent temporal patterns and biologically plausible associations that were supported across multiple time points and analyses.
Results
During the study period, a total of 129 patients with aSAH were treated at our neurovascular center. Out of these, 54 either did not meet the strict inclusion criteria (first sampling within 24 h of aSAH) or the patients or their relatives declined to participate in the study. Ultimately, 75 patients were included in the analysis, and an additional 20 healthy controls were recruited and enrolled as a comparison group. The patient characteristics are detailed in Table 1. No significant associations with immune cell subtypes were observed in relation to infections requiring anti-infective or immunomodulatory treatments.
Table 1. Patients characteristicsOverall (N = 75)Age Mean (SD)54 (± 12)Sex Female49 (65%) Male26 (35%)Initial WFNS I22 (29%) II11 (15%) III6 (8%) IV16 (21%) V20 (27%)mFisher 12 (3%) 25 (7%) 330 (40%) 438 (51%)Aneurysm Location ACOM31 (41%) ACA1 (1%) PcA3 (4%) MCA13 (17%) ICA7 (9%) PCOM7 (9%) PCA1 (1%) BA5 (7%) PICA2 (3%) AICA1 (1%) Other4 (5%)LOS Mean (SD)20.2 (± 8.4)mRS Discharge 0–238 (51%) 3–529 (39%) 68 (11%)mRS 6 Months 0–247 (62%) 3–512 (16%) 610 (13%) Missing6 (8%)Angiographic Cerebral Vasospasm Not Present58 (77%) Present17 (23%)Clinical DCI Not Present51 (68%) Present24 (32%)DCI-related Infarction Not Present43 (57%) Present32 (43%)DCI Not Present34 (45%) Present41 (55%)ACA anterior cerebral artery, ACOM anterior communicating artery, AICA anterior inferior cerebellar artery, BA basilary artery, ICA internal carotid artery, MCA middle cerebral artery, mRS modified Rankin scale, PcA pericallosal artery, PCA posterior cerebral artery, PCOM posterior communicating artery, PICA posterior inferior cerebellar artery, SCA superior cerebellar artery, SD standard deviation, WFNS World Federation of Neurosurgical Societies
Alterations in monocyte and T cell subpopulations: aSAH vs. Healthy controls
In comparison to healthy controls, individuals who experienced aSAH showed a significant increase in the relative number of intermediate monocytes (4.3% vs. 7.2%; p = 0.02), as well as a significant relative reduction in alternatively activated monocytes (6.3% vs. 3.0%; p = 0.04) (Fig. 2A).
Fig. 2. Monocyte and T cell subtypes – comparison with healthy controls and temporal dynamics in aSAHA Relative number of monocyte subtypes and (C) T cell subtypes in peripheral blood of healthy individuals (no aneurysm; no aSAH) compared to patients 24 h post-aneurysmal subarachnoid hemorrhage (aSAH), depicted as bar graphs. B Representation of relative number of monocyte subtypes and (D) T cell subtypes over time following aSAH, with measurements taken on days 1, 4, 7, and 11
Examining T cell subtypes revealed consistent significant differences between healthy controls and those with aSAH. The relative number of T regulatory cells (5.9% vs. 8.0%; p = 0.04) and Th17 T cells (6.2% vs. 36.3%; p < 0.001) was significantly increased in patients with aSAH, while the relative number of Th1 (15.1% vs. 9.5%; p = 0.006) and Th2 T cells (75.2% vs. 45.5%; p < 0.001) showed a significant decrease (Fig. 2C). The exact numerical values are provided in Table 2.
Table 2. Relative distribution of monocyte subtypesClassically Activated MonocytesIntermediate MonocytesAlternatively Activated Monocytes% of monocytes (± SD)n Control 89.0 (11.6)4.3 (2.4)6.3 (11.2)20 Time Course Day 188.9 (7.1)7.2 (5.3)3.0 (3.9)72 Day 489.1 (6.0)7.3 (4.7)2.9 (3.0)74 Day 789.0 (6.5)6.4 (4.1)3.9 (3.7)64 Day 1188.6 (8.7)6.2 (4.3)4.4 (5.2)60 Outcome Favorable88.9 (8.1)7.1 (5.3)3.1 (4.6)35 Poor90.3 (4.6)6.6 (4.4)2.3 (1.4)28 Death83.6 (7.5)10.2 (6.9)5.0 (5.6)8 Angiographic Cerebral Vasospasm Not Present89.0 (6.0)6.5 (3.8)3.8 (3.4)58 Present88.3 (5.6)8.2 (3.2)2.7 (2.3)17 Clinical DCI Not Present88.7 (6.1)6.6 (3.9)4.0 (3.5)51 Present89.1 (5.5)7.6 (3.4)2.5 (2.0)24 DCI-related Infarction Not Present89.0 (5.9)6.2 (3.3)4.1 (3.5)43 Present88.6 (5.9)7.8 (4.2)2.8 (2.5)32 DCI Not Present89.6 (5.4)5.6 (2.7)4.3 (3.7)34 Present88.2 (6.2)8.0 (4.2)2.9 (2.6)41Representation of the relative proportions of monocyte subgroups among all monocytes in percentage ± SD standard deviation. Outcome = mRS 6 months post bleeding (favorable = 0–2; poor = 3–5, death = 6). DCI delayed cerebral ischemia, n number of patients
Temporal dynamics in monocyte and T cell subpopulations in aSAH patients
Over time following aSAH, a non-significant trend was observed for monocytes, indicating a relative decrease in intermediate monocytes (day 1 vs. day 11; 7.2% vs. 6.2%; p = 0.115) and a relative increase in alternatively activated monocytes (day 1 vs. day 11; 3.0% vs. 4.4%; p = 0.136).
To better account for intra-individual variability and irregular spacing of timepoints, we additionally performed linear mixed-effects modeling. This confirmed a significant increase in alternatively activated monocytes (β₁ = +0.14, 95% CI [0.05–0.23], p = 0.003) and a significant decrease in intermediate monocytes (β₁ = − 0.12, 95% CI [–0.23 to − 0.01], p = 0.033) within the observation period.
Concerning T cells, a non-significant relative decrease in Th2 cells was observed over time (day 1 vs. day 11; 45.5% vs. 40.0%; p = 0.075), as well as a relative increase in Th17 cells (day 1 vs. day 11; 36.3% vs. 40.5%; p = 0.47). The mixed-effects model revealed this trend to be a significant temporal decrease in Th2 cells (β₁ = − 0.87, 95% CI [–1.61 to − 0.13], p = 0.021). For Th17, Th1, and Tregs, no significant longitudinal changes were detected in the mixed-effects model.
Monocyte and T cell subpopulations in aSAH patients with vs. without angiographic cerebral vasospasm
In 17 patients, angiographic cerebral vasospasm was observed during the observation period, which was preceded by a shift in monocyte and T cell subpopulations. Patients with angiographic cerebral vasospasm showed a significantly lower relative number of alternatively activated monocytes (3.8% vs. 2.0%; p = 0.031, Cohen’s d=−0.57, CI [–0.98 to − 0.15]) (Fig. 3A). This association remained evident in multiple logistic regression although statistical significance was not reached (p = 0.081). Regarding T cell subpopulations, a significantly increased relative number of Th1 T cells was observed (Supplementary Fig. 1). The exact numerical values are provided in Table 2.
Fig. 3. Monocyte subtype distribution in angiographic cerebral vasospasm and DCIRepresentation of the relative number of alternatively activated monocytes (left column), intermediate monocytes (middle column), and alternatively activated monocytes (right column) for patients with aSAH, categorized by the presence (n = 17) or absence (n = 58) of angiographic cerebral vasospasm (A), presence (n = 24) or absence (n = 51) of clinical DCI (B), presence (n = 32) or absence (n = 43) cerebral infarction due to DCI (C), and presence (n = 41) or absence (n = 34) of overall DCI (D). Data are presented as mean ± SD. Significance was defined as a p-value < 0.05 for comparisons between the mean of the subpopulations before the event in affected patients and the mean of the subpopulations over the entire observation period in unaffected patients. The red circle symbolizes the mean, and the orange line indicates the median
Monocyte and T cell subpopulations in aSAH patients with vs. without DCI
Patients who developed DCI (n = 41) exhibited a distinct and significant shift in monocyte subpopulations compared to aSAH patients without DCI. Specifically, prior to or at the onset of DCI, these patients showed an increased relative proportion of intermediate monocytes (5.6% vs. 8.0%; p < 0.0001; Cohen’s d = 0.53, CI [0.29 to 0.78]) and a decreased relative number of alternatively activated monocytes (4.3% vs. 2.9%; p = 0.006; Cohen’s d=−0.34, CI [–0.58 to − 0.10]) (Fig. 3D). This shift remained significant even when considering the individual subcategories of DCI (Table 2; Fig. 3B/C). These associations remained statistically significant in multiple logistic regression models (p = 0.007 for clinical DCI, p = 0.012 for cerebral infarction due to DCI, p = 0.007 for pooled DCI). For the T cell subpopulations, only non-significant trends were observed, as depicted in Supplementary Fig. 1. The exact numerical values are provided in Table 3.
Table 3. Relative distribution of T cell subtypesTh1Th2Th17Tregs% of T cells (± SD)n Control 15.08 (8.5)75.2 (11.6)6.2 (7.7)5.9 (2.7)20 Time Course Day 19.5 (9.0)45.5 (29.9)36.3 (28.4)8.0 (4.4)72 Day 411.5 (10.2)51.0 (29.7)29.6 (27.4)7.0 (3.7)74 Day 79.4 (9.1)42.7 (32.1)38.4 (30.7)7.7 (4.9)64 Day 118.6 (9.7)40.0 (32.8)40.5 (30.8)7.5 (4.2)60 Outcome Favorable9.7 (10.5)49.1 (30.5)34.4 (29.8)6.6 (3.5)35 Poor9.5 (7.5)39.7 (28.5)39.4 (27.3)9.5 (4.5)28 Death9.1 (5.7)53.7 (25.2)30.7 (22.3)9.3 (5.3)8 Angiographic Cerebral Vasospasm Not Present9.9 (8.4)45.1 (25.7)36.1 (24.3)7.6 (3.6)58 Present11.9 (8.1)47.0 (23.2)31.4 (20.4)7.7 (3.5)17 Clinical DCI Not Present10.0 (8.5)46.1 (25.8)35.3 (24.3)7.6 (3.7)51 Present11.2 (7.9)44.2 (23.5)34.8 (21.9)7.6 (3.2)24 DCI related Infarction Not Present10.2 (9.0)47.2 (25.5)33.9 (23.6)7.4 (3.5)43 Present10.4 (7.4)43.2 (24.6)36.9 (23.6)7.6 (3.2)32 DCI Not Present11.0 (9.8)48.2 (26.5)32.3 (24.7)7.5 (3.7)34 Present9.7 (6.8)43.2 (23.8)37.6 (22.4)7.7 (3.5)41Representation of the relative proportions of monocyte subgroups among all monocytes in percentage ± SD standard deviation. Outcome = mRS 6 months post bleeding (favorable = 0–2; poor = 3–5, death = 6). DCI delayed cerebral ischemia, n number of patients
Relationship between monocyte and T cell subpopulations with the outcome in aSAH patients
For the distribution of monocyte subpopulations, no significant correlation was observed with clinical outcomes at 6 months after bleeding (classically activated: p = 0.26, intermediate: p = 0.43, alternatively activated: p = 0.54) (numerical values: Table 2). Similarly, T cell subpopulations showed no significant correlation with the outcome 6 months after bleeding (Th1: p = 0.65, Th2: p = 0.77, Th17: p = 0.83. Tregs: p = 0.19). The exact numerical values are provided in Table 3.
Discussion
It is well-established that inflammation plays a key role after aSAH, but no definitive therapeutic intervention has proven successful in modulating this response. Monocytes and T cells play a critical role in the sterile inflammation seen after aSAH [8, 9, 14, 25–27], with evidence from various diseases, including infections, cardiovascular and inflammatory disorders, cancer, and autoimmune conditions, suggesting that their subpopulations exert distinct, sometimes opposing effects on the inflammatory response [28–31]. These subpopulations of monocytes and T cells secrete, among other factors, different and varying amounts of cytokines, exerting partially opposing effects, whereby inflammation can be either exaggerated or attenuated depending on their polarization to different subgroups [28–31]. To date, however, despite their eminent role in initiating and upholding an inflammatory response, it is not known how monocyte and T cell subpopulations behave after aSAH and their role in post-hemorrhagic complications is not fully understood. By analyzing these immune cell subtypes, our study contributes to filling this knowledge gap, providing new avenues for diagnostic and therapeutic approaches.
In this prospective controlled cohort study, we demonstrate a distinct and early shift in monocyte and T-cell subpopulations toward a pro-inflammatory milieu in patients following aSAH, compared to healthy controls. Specifically, within 24 h post-hemorrhage, we observed a 52% reduction in the relative proportion of anti-inflammatory alternatively activated monocytes, a 39% decrease in anti-inflammatory Th2 cells, and a remarkable 585% increase in the proportion of inflammatory Th17 T cells (Fig. 2A/C). Although there was also a 37% increase in regulatory T cells and a 36% reduction in pro-inflammatory Th1 cells, the overall profile indicated a marked shift toward a pro-inflammatory immune response, not only in relative proportions but also in absolute numbers (Fig. 2A/C). This early and pronounced shift in immune cell subpopulations aligns with prior studies linking post-aSAH inflammation to elevated pro-inflammatory cytokine levels and immune cell activation [8, 9, 14, 25–27]. Our study provides detailed insights into immune cell dynamics, confirming previous findings on Th17 increases in a small cohort of 15 patients [32], while adding granularity by focusing on high-resolution data of systemic cellular response in a larger prospective cohort and combining clinical, radiological, and immunological data. Moreover, the pronounced increase in Th17 cells and decrease in Th2/Treg cells—evident within 24 h post‑aSAH—is reminiscent of autoimmune‑like, IL‑17‑driven mechanisms that, in other CNS diseases, have been linked to blood–brain barrier disruption and immune infiltration [33]. While our study cannot distinguish systemic from central effects, these findings raise the possibility that similar IL‑17‑mediated immune processes may occur intracerebrally after aSAH. However, we acknowledge that this interpretation remains speculative, as we did not collect serum cytokine data (e.g., IL-6 or IL-17 A) to support this hypothesis directly.
Over the course of time following aSAH, we observed trends in the composition and distribution of monocyte and T-cell subpopulations. While initial linear regression suggested non-significant trends, linear mixed-effects modeling revealed a gradual recovery of initially reduced alternatively activated monocytes, while intermediate monocytes declined significantly over time (Fig. 2B). Additionally, a significant longitudinal decline in Th2 cells and a non-significant increase in Th17 cells was observed (Fig. 2D). These shifts suggest that while the initial monocyte-driven inflammatory response may attenuate over time, T-cell subpopulations may continue to sustain a pro-inflammatory environment. Although speculative due to the non-significant trends, these observations are consistent with the expected trajectory of an evolving immune response, where innate immune cells like monocytes dominate early inflammation, followed by sustained T-cell activity as part of the adaptive immune responses.
The most significant finding of this study, however, relates to the correlation between monocyte subpopulation dynamics and the onset of complications. Notably, patients who developed angiographic cerebral vasospasm or delayed cerebral ischemia exhibited a significant reduction in alternatively activated monocytes prior to the onset of these complications (Fig. 3), with meaningful effect sizes. This finding underscores the potential role of monocyte subpopulation polarization in the pathophysiology of aSAH-related complications. The observed shift towards a pro-inflammatory milieu, characterized by a loss of alternatively activated monocytes, represents a novel and pivotal finding. This observation aligns well with previous research identifying specific cytokine patterns [34, 35] and increase in monocytes and T cells [9, 25, 36, 37] as contributors to vasospasm and DCI, but offers new insight by identifying the specific monocyte subpopulations involved. While these results suggest that monitoring monocyte subpopulations might help identify patients at higher risk for complications, the predictive utility of these findings remains to be determined and requires confirmation in future studies designed for this purpose. Importantly, these associations remained statistically significant for cerebral infarction due to DCI, clinical DCI, and pooled DCI even after adjustment for age, sex, WFNS grade, and modified Fisher grade in multiple logistic regression models, further supporting the potential clinical relevance of this immune marker. No significant differences in immune profiles were observed between patients with and without anti-infective or immunomodulatory treatment, suggesting aSAH-specific rather than treatment-driven immune alterations.
Moreover, although peripheral immune cells such as monocytes and T cells are known to cross the blood–brain barrier under pathological conditions, our study did not assess the presence or activation of these cells within the cerebrospinal fluid or brain parenchyma. As such, the findings should not be overinterpreted as direct evidence of neuroinflammation. Instead, they highlight potential peripheral immune correlates of aSAH-related complications. However, the prospective nature of our study, along with the high-quality, detailed immune profiling, adds weight to these findings and highlights the potential relevance of immune monitoring after aSAH. Future investigations incorporating CSF sampling or brain tissue studies will be essential to determine whether the observed peripheral immune changes are mechanistically linked to intracerebral immune mechanisms.
Despite the importance of these findings, we found no significant correlation between immune subpopulations and long-term outcomes at 6 months. This may be due to the standardized care all patients received [38], with timely treatment of complications, potentially minimizing their impact on outcomes. However, it is possible that in cohorts with different treatment protocols or less standardized care, a correlation between immune subpopulations and outcomes may emerge. Additionally, certain differences in outcomes, such as aspects of quality of life or psychological well-being, may exist but were not captured by the modified Rankin Scale used in this study. This scale is relatively coarse, may be subject to individual perception, and does not reflect the complexity of neurocognitive recovery or patient-centered outcomes. Other relevant endpoints such as ICU length of stay, cognitive status, or secondary complications were not systematically assessed and should be addressed in future studies. It must also be considered that the relatively small sample size may have limited the statistical power to detect weaker correlations between immune profiles and long-term functional outcomes. Therefore, early immune signatures may still hold value as intermediate biomarkers for patient monitoring or therapy stratification.
When considering potential therapeutic implications, alternatively activated monocytes may represent a promising avenue for further investigation. Given their significant reduction both shortly after aSAH and before the onset of complications, strategies aimed at preventing the loss of these cells or promoting their polarization could have effects on the inflammatory process and its sequelae [39]. The important role of alternatively activated monocytes has not only been demonstrated in other diseases [14], but animal models have already shown the therapeutic potential of modulating alternatively activated monocytes, such as through mesenchymal stem cell-derived extracellular vesicles, which induced alternatively activated monocyte polarization and exerted neuroprotective effects in experimental aSAH [40, 41]. Our study provides initial human data suggesting that preserving or enhancing the function of these cells might influence the inflammatory cascade after aSAH. However, whether these peripheral changes reflect central immune processes, and whether they can be safely and effectively targeted in patients, and if this results in a reduction of Complications like angiographic cerebral vasospasm and DCI, requires further research in translational models and larger clinical cohorts.
Limitations
This monocentric study included diverse ethnicities but may not be generalizable to all populations. The single-center design, however, with standard conditions and a standardized treatment protocol reduces heterogeneity and bias. The small sizes of some immune subpopulations and the high interpersonal variability also introduced variability, complicating data pooling and analysis. To address this, a larger patient cohort or a baseline would be necessary. Yet, obtaining a baseline before aSAH is not possible due to its unpredictability prior to the bleeding. Especially when considering the T cell subpopulations, the necessity for larger study populations becomes evident to potentially capture significant changes in these cells, which seem to be present but to a much lesser extent than in the monocyte subpopulations. Selection bias due to the consent process cannot be ruled out, though we believe the study population to be reasonably homogeneous. Furthermore, clinical DCI is a diagnosis of exclusion and inherently prone to confounding. However, through the prospective design and detailed clinical monitoring of all patients, including targeted diagnostics where appropriate, we aimed to minimize misclassification. Nevertheless, residual diagnostic uncertainty cannot be excluded and may have influenced the observed associations and factors such as systemic stress responses and other unmeasured variables may have influenced the observed associations and cannot be fully excluded. No formal correction for multiple comparisons was applied in this exploratory study. Given the relatively small sample size and the high variability inherent to immune cell populations, strict adjustment methods such as Bonferroni correction would have substantially increased the risk of type II errors—i.e., failing to detect true biological associations. Furthermore, given the relatively small sample size in the subgroup analyses, particularly for patients with angiographic vasospasm, the statistical power is limited and the risk of type I error must be acknowledged. Therefore, results should be interpreted cautiously and considered hypothesis-generating pending validation in larger cohorts.
Conclusion
This prospective cohort study demonstrates a distinct early shift in the peripheral immune profile after aSAH, characterized by a reduction in alternatively activated monocytes and an imbalance in T cell subpopulations suggestive of autoimmune-like responses. The consistent association between reduced alternatively activated monocytes and major complications like cerebral vasospasm and DCI, suggests a promising immunological marker and potential therapeutic target in the pathophysiology of aSAH. Validation in larger cohorts and clarification whether the observed peripheral changes reflect corresponding immune processes within the central nervous system will be key steps toward translating these findings into clinical application.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bacigaluppi S, Ivaldi F, Bragazzi NL, Benvenuto F, Gallo F, D’Andrea A, Severi P, Uccelli A, Zona G. An early increase of blood leukocyte subsets in aneurysmal subarachnoid hemorrhage is predictive of vasospasm. Front Neurol. 2020;11. 10.3389/fneur.2020.587039.10.3389/fneur.2020.587039 PMC 777967533408685 · doi ↗ · pubmed ↗