Qualitative exploration of how clinicians navigate divergence in older adult and family caregiver priorities
Martina Azar, Katherine A. Kennedy, Marla L. Clayman, Emma D. Quach

TL;DR
This study explores how doctors handle disagreements between older patients and their caregivers about care priorities during medical visits.
Contribution
The study provides new insights into clinician communication strategies when patient and caregiver priorities conflict.
Findings
Clinicians acknowledged both patient and caregiver priorities and highlighted any common ground.
They pivoted to care planning while maintaining a neutral and warm approach.
The study suggests these visits can promote understanding and collaboration between patients and caregivers.
Abstract
Clinicians often elicit and incorporate patient priorities into care plans. This process is complicated when patients and their family caregivers express incongruent priorities. We investigated patient and family caregiver priorities expressed during medical visits and clinician responses to divergent priorities. Methods: Our data consisted of four first-time medical appointments, each attended by an older patient, at least one family caregiver, and a team of geriatrics clinicians. We audio-recorded and transcribed the appointments, each lasting at least 120 min, and performed thematic analysis of the expressed priorities and clinician responses. Results: When incongruence in priorities emerged, clinicians responded with acknowledgement to each party’s priority and highlighted the incongruence itself, pointing out common ground when present, and pivoted to care planning, while…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
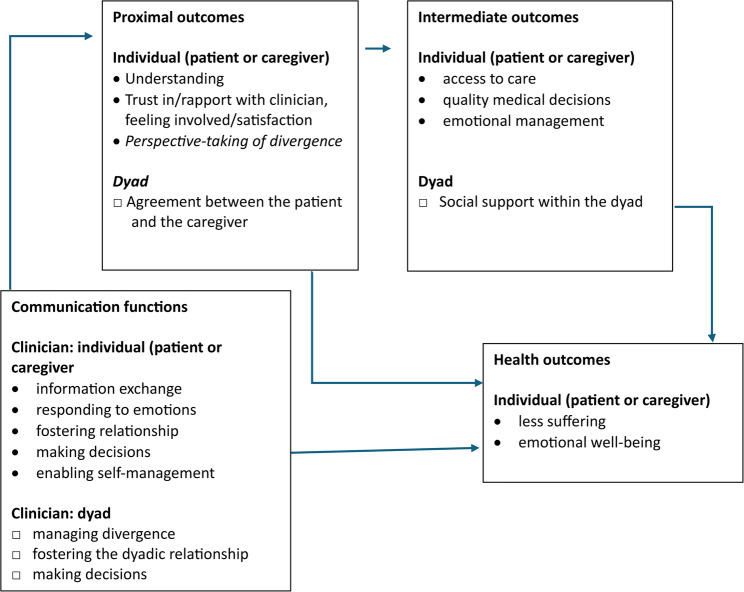 Figure 1
Figure 1- —VA New England Geriatrics Research and Education Center Advanced Fellowship in Geriatrics
- —VA Office of Academic Affiliation Advanced Fellowship in Health Services Research & Development
- —VA Veterans Health Administration, VISN 1 Career Development Award
- —VA Office of Health Equity
- —VA Office of Research and Development, Health Services Research & Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient-Provider Communication in Healthcare · Palliative Care and End-of-Life Issues · Clinical Reasoning and Diagnostic Skills
Introduction
In the U.S., older adults with physical and mental health comorbidities often rely on family caregivers to meet their daily physical, social, and mental health needs. In 2022, 34.2 million family caregivers provided unpaid care to an adult age 50 and over. Approximately 15.7 million family caregivers provided care for someone with Alzheimer’s disease or another dementia, totaling $600 billion in 2021 [22]. Such family caregiving constitutes the bulk of long-term care for older adults living in the community and may last many years, making the caregiving relationship a health policy priority.
Extant literature suggests older adults with comorbidities have preferences and priorities regarding their health and overall care [2, 7, 13, 27]. These may include priorities regarding access, modality of healthcare appointment, communication, or characteristics of providers that they find welcoming. Older patients and their family caregivers may hold incongruent perspectives about health and care that may compromise the caregiving relationship [1]. Incongruence documented thus far focused on the extent of patient’s difficulties, value of social relationships [17], autonomy [16], and preferred sources of socioemotional support [24]. Incongruence within dyads has been associated with relationship strain and caregiver burden [12]; these predict, in part, family caregivers’ desire to seek institutional care (i.e., seek alternatives to family caregiving) [26]. Supporting family caregivers of community-dwelling older adults may depend on recognizing and addressing incongruent perceptions within caregiving dyads.
Medical appointments including patients and family caregivers represent a setting that is well-suited for recognizing and addressing incongruent perceptions. Research on appointments attended by the patient, the family caregiver(s), and clinicians align with the positive effects patient-clinician interactions may have on patients’ emotional and physical well-being [25]. Yet we know little about patient and caregiver priorities raised during medical visits, the incongruence of these priorities, and clinicians’ responses to potential incongruence, especially in visits with older patients with varying levels of cognitive impairment. Our exploratory, qualitative study thus examines the types of priorities that patients with and without cognitive impairment and their caregivers express, any divergence of these priorities, and clinician responses.
Conceptual framework
Our study’s framework borrows elements from Street’s conceptual model on patient-clinician communication and health outcomes [25], which, in our study, focuses on communication among three parties, rather than two. According to this framework, communication during medical appointments with various parties may achieve different functions, such as information exchange, responding to emotions, facilitation, fostering relationships, and shared decision-making. While these functions may be accomplished by communication between the clinician and the patient (or clinician and the caregiver), some may be unique to communication between the clinician and the dyad (caregiver and patient). Such communication functions are not well-understood, including when there are multiple clinicians in the same encounter. See Fig. 1 for our study’s framework, an adaptation of the Street’s conceptual model of medical visits, incorporating communication functions involving dyads and dyadic outcomes. Fig. 1 Our study’s conceptual framework of communication among the clinician, patient, and caregiver during medical visits, adapted from Street’s model of patient-clinician communication [25] Note: Our adaptations are preceded by □. For parsimony we omitted some individual intermediate and health outcomes from the original model [25]
Methods
Study setting and participant recruitment
Our study was conducted at [Blinded for Review] VA hospital’s outpatient geriatrics specialty clinic. The study’s purpose was to assess how clinicians navigate discussions with patients and their caregivers about their priorities, i.e., “what matters most” (WMM). The clinic consists of a geriatrician, nurse, social worker, and clinical pharmacist, with administrative support from a medical support assistant. Typically, first-time appointments are jointly attended by all available clinicians and, given VA’s priority to support family caregivers, include an extensive discussion about priorities of both the patient and the family caregiver(s). We therefore aimed to enroll patients attending their first-time appointments with a family caregiver.
Between July and September 2022, we approached all eligible patients (n = 4). During a phone call by the medical support assistant to confirm the appointment with the patient and family caregiver, one of the authors informed the patient or the family caregiver of the purpose of the study and invited them to participate in this study (i.e., have their upcoming appointment audio-recorded). All patients and family caregivers (n = 9) who were contacted during the calls gave verbal permission. Upon their arrival at the clinic, one author [Blinded for review] gave the patient and family caregiver(s) a written description of the study and asked for verbal confirmation that they agreed to have the appointment audio-recorded. After the patient and the family member(s) gave verbal assent, the audio-recorder was turned on and placed on the conference table, around which clinicians, patient, and family caregiver(s) sat.
Table 1 shows select characteristics of the four first-time medical appointments and the patients, caregivers, and clinicians who attended these appointments. These appointments lasted, on average, two hours. All patients were white male Veterans. Two of the four patients were diagnosed with dementia at the time of the appointments. Each appointment was attended by at least one family caregiver (i.e., spouse, child, sibling of the Veteran). All four appointments were attended by the clinic’s geriatrician, social worker, and clinical pharmacist, with one appointment also attended by the newly hired nurse.
Table 1. Select characteristics of four initial medical appointments, their patients, caregivers, and cliniciansPatient 1Patient 2Patient 3Patient 4AppointmentDuration (hours)1 h:20 m1 h:50 m2 h:35 m2 h:00 mPatient Patient’s genderMaleMaleMaleMale Patient’s age76928787 RaceWhiteWhiteWhiteWhiteDementia diagnosisNoNoYesYesCaregiver(s) # of caregivers present1121 Relationship of caregiver(s) to patientWifeDaughterWife & DaughterBrother Caregiver considered “primary caregiver”WifeDaughterDaughterDaughterClinicians # of Clinicians3343 Type of CliniciansMDSWPharmDMDSWPharmDMDSWPharmDRegistered NurseMDSWPharmDThe geriatrician, social worker, and pharmacist were the same clinicians in each appointmentMD Geriatrician, SW Social worker, PharmD Pharmacist
Data collection and analysis
During the appointments, [Blinded for review] sat at a separate table in the same conference room. The physical positioning was designed to enable [Blinded for review] to listen to the conversation as unobtrusively as possible as well as observe and take notes of paraverbal (e.g., tone) and non-verbal communication. The audio recorder was turned off by [Blinded for review] at the end of the appointment (when individuals in the appointment stood up to prepare to leave the room). Audio files were transcribed verbatim by a professional transcriber. Transcripts were not returned to participants for comment or correction. Transcripts and field notes of paraverbal and non-verbal communication were uploaded to NVivo 12 [15] for code management and thematic analysis.
We performed our coding and analyses iteratively, guided by both an inductive approach rooted in the data [4, 5, 23] as well as by our conceptual framework. First, three authors ([Blinded for review]) constituted the coding team, each member independently listening to the audio recordings, reading the transcripts and engaging in, open coding of data elements (i.e., attach meanings or codes to excerpts of text). In group discussions, these three authors ([Blinded for review]) compiled notes and developed a first draft of the codebook of codes and their definitions. We used the codebook and coded in pairs ([Blinded for review]) to promote consistent coding. In follow-up meetings between coding pairs, coding discrepancies were discussed and resolved, and codes and their definitions were modified, with all changes made by coding pairs subsequently discussed and agreed upon in meetings with the entire coding team. We also sought feedback during the coding process from our fourth co-author to promote reflexivity and methodologic rigor. Our coding produced 24 codes that captured key concepts from the medical appointments. Our current study focuses on 22 codes describing patient and family caregiver’s priorities and the clinician’s responses. All authors ([Blinded for review]) then contributed to data interpretation.
We then performed thematic analyses from our codes [4, 5, 23], analyses rooted in a realist theoretical position to report on participants’ experiences [4] and informed by elements of the Street’s conceptual framework. To facilitate development of themes, we grouped codes into categories by speaker (i.e., patient-, caregiver-, clinician- codes). We grouped priorities by source (i.e., patient’s or caregiver’s priorities) and clinician responses by type (e.g., validation and acknowledgment). During thematic development, we also examined the content of our codes against elements of Street’s model, noting when codes were not explicitly specified in the Street’s model. Our analysis was performed by a set of coders consisting of researchers (PhDs in gerontology and education, with formal training in qualitative research methods) and a team member (PhD in clinical psychology with neuropsychology focus) who provided clinical care. In brief, to enhance rigor and consistency, we sought feedback from each co-author throughout the thematic development and data interpretation, including group discussions and resolutions of coding discrepancies. See Appendix Table 3 for our codebook of codes and their definitions. Member checking was not included. In other words, we did not return to the participants to present our data or results for their feedback or validation.
Ethical considerations
This study was approved by the Research and Development Committee of a Veterans Affairs Medical Center in Veterans Integrated Service Network 1 [exact name of institution omitted during blinded review and in publication] as quality improvement to examine and improve clinician-patient-caregiver communication during WMM medical appointments. Our study was therefore not subject to Institutional Review Board oversight, and the need for informed consent to participate was deemed unnecessary according to the US Department of Veterans Affairs Office of Research Development Program Guide 1200.21(22). Nevertheless, we adhered to ethical principles throughout our study (e.g., all participants in the study were provided with a written document describing the voluntary nature of the study; verbal agreement to participate was obtained from all participants in the study prior to study participation).
Results
To illustrate our themes and codes in context, we selected three scenarios. In each scenario, we first describe the viewpoints of the patient and the family caregiver and the extent to which they diverge, whether disagreements were explicit or more nuanced (implicit), and subsequently describe responses by clinicians. Within each scenario, we annotate selected passages (using brackets and bold text) that exemplify the clinical responses to divergence underlying our themes. In addition, to the extent possible without video recording, we annotated observations of para-verbal and non-verbal communication (in brackets and italicized text) to provide additional context.
Scenario 1: clinician responses to concerns regarding cannabis use to cope with Post-Traumatic Stress Disorder (PTSD)
A male Veteran (Patient 1) who attended the appointment with his wife described his struggle to find effective ways to cope with PTSD following his military service in Vietnam. Although both the patient and his wife agreed on the patient’s need to manage PTSD symptoms, they stated their own perspectives regarding the patient’s cannabis use as a coping strategy. Specifically, the patient strongly appreciated cannabis as a way to control his PTSD symptoms whereas his wife expressed her discomfort surrounding the source of cannabis and her lack of knowledge regarding choosing products with the “right” potency. In addition, the spouses disagreed on smoking in the house, as the patient stated, “If I could smoke it in my room and jump into bed, that would be okay. But that’s not going to work [for my wife]. Both parties, nevertheless, expressed their mutual desire to reduce cannabis’ side effects, such as the patient’s reduced mobility while under the influence. The quotes below show clinician strategies include acknowledgement and validation of priorities of each member of the dyad and reframing of the problem and pointing out common ground or mutual understanding between the spouses.Wife: …I came home one time in the middle of winter and a really cold night, he was out on the breezeway, and I can’t get him up. I can’t get him -- I tried to get him up but can’t. …[tone of concern,* distress*].Pharmacist: Sure. Number one that sounds like a really difficult situation for both of you [clinician validates caregiver and patient] and so, I just want to say that… it sounds like, [wife’s name], some of what you’re worried about …is safety [reframes the problem expressed by caregiver and patient]. Is him being safe, and I think that’s really valid…worrying about his safety, especially if you’re not there. And he’s [the patient] impaired… [Addressing patient] …what worries you…?Patient: The same thing.Pharmacist: Okay. Tell me a little more in your own words about that?Patient: Well, I need something to control my -- the aftereffects of the flashbacks. The marijuana helps. But, like alcohol would have a devastating effect on me.…Pharmacist: …-- managing the symptoms of your PTSD is certainly something that matters to you. Your safety and feeling like you’re able to move around and do your day-to-day in light of having those symptoms controlled also matters to both of you. [clinician reframes problem expressed by the patient; pointing out common ground] It sounded like you told me, and I’d like to hear more, that the pain clinic has been very helpful to you [pivots to care planning].
In addition to pointing out common ground, the clinicians also calmly listened to divergent perspectives and, at times, frustrations about daily routines. For example, the caregiver expressed her frustrations about their differences in preferred meal and sleep routines, “then if I fix a supper, most of the time he won’t eat it. Or he’ll eat a third of it or something. … But then I say you got to stay up, don’t -- try not to doze and stay up and then maybe you’ll be able to sleep through the night. … [drove] me crazy,” even though the patient remarked plainly “I don’t have an appetite…I can’t eat”. As shown below, in the absence of a clear common ground, clinicians acknowledged the divergence and, in due time, shifted the conversation to care planning inclusive of proposed coordination with the dental office and nutritionist—agreed by both parties—to address the patient’s poor appetite.
Wife:. I don’t know what to do to get him to kind of more schedule to his life….Pharmacist: Okay. So, it sounds like two different philosophies for sure just for day-to-day, both valid. I totally understand both sides. [clinician’s acknowledgement of incongruence; calm tone] ….
Wife: …I wondered …you’re [Patient] getting [cannabis] from a girl who grows it up in Maine, and … Dr. XXX said that some are different strengths, and some are stronger than others and you don’t know and…the pot store…talks about chronic pain…[and] relaxation… I don’t know enough.
Patient: You need to understand, and you never will, the horror that goes through my mind when I relive some of those events and those flashbacks, and then you’ll understand and none of you ever will.
Pharmacist: You’re right. You’re right. [clinician’s acknowledgement of patient’s priority]
Social worker: Agree.
Wife: So, what you really are saying is that you need something strong enough that it completely just zips your mind to nothing.
Patient: No, I’m not. I’m saying something about halfway there.
Wife: Okay.
Geriatrician: That’s helpful for us. … but there are … experts in CBD and other formulations of marijuana for pain. [clinician pivots to care planning] I’m excited to work with you to see what’s out there… what’s going to keep your mind at ease as far as his safety [clinician’s acknowledgement of caregiver priority] …is this helping me be able to do the things I love without making me feel medicated. Or what is that works for [the patient]. [clinician’s acknowledgement of patient’s priority]
Patient: Yeah. … I can’t be medicated like what she is describing. That can’t work.
Pharmacist: Okay. And I think we all agree on that one too. …
Scenario 2: clinician responses to divergence on utility of doing Chair-rise exercise at home
A 92-year-old male Veteran (Patient 2) attended the appointment with his daughter, who expressed that her father’s engagement in at-home exercise was her priority. In response, the geriatrician demonstrated a chair-rise exercise to the patient during the exam portion of the appointment. Later in the appointment, the patient expressed that he did not wish to engage in the chair-rise exercise.Geriatrician: So this particular sheet shows something called the chair-rise exercise. I know you mentioned that you have family members who are fabulous at physical therapy and physical education [Clinician acknowledges caregiver priority]. I wonder if you would be up for…a little bit of exercise… into your week? ….Patient: Eh, I’ve done them before. I don’t want to bother with it.Geriatrician : I gotcha. So, it doesn’t sound like it’s something that you’re eager to build into your busy schedule at this moment, but we’ll keep it for you in the binder and we can even talk about it a little bit more next time perhaps….[Clinician states their priorities, non-judgmental/neutral tone].Patient: Okay.Daughter: …[my aunt] likes to do her exercises…She’ll be 100 in January.Pharmacist : Wow, amazing. [Clinician acknowledgement of caregiver priority]Daughter: …Yeah, [my aunt] just feels it’s so important to be able to get up out of her chair, use it or lose it.Pharmacist: Yeah, great. That’s good advice.Daughter: Yeah, lose it or lose it. Yeah, she’s amazing.Geriatrician : Certainly sounds like you have folks in addition to you being so active…so that’s wonderful. So I’ll keep this one in the binder for you.
In response to the emergent implicit divergence between priorities, the clinicians validated the patient’s perspective while echoing the caregiver’s view of the importance of exercise. The geriatrician utilized the opportunity to encourage the patient to re-consider physical exercise at a later time.
Upon the patient’s rejection of chair-rise exercise, the geriatrician then pivoted to the physical therapy and balance/gait training as an alternative (to chair-rise exercise) to improve physical activity and safety. The geriatrician also reframed the chair-rise exercise not as exercise but as falls prevention and safety, a goal for discussion in a future appointment, stating, “But in general we also just were so impressed…with your family…at that point we might like to talk more about falls prevention, always making sure that you’re safe.”
Both the patient and the caregiver subsequently agreed to these referrals.
Geriatrician: … if you would like to meet with one of our physical therapists for some balance or gait training, sometimes they will recommend an assistive device, whether it be a cane or a walker…. [Clinician pivots to another care option] We certainly could consider that.
Patient: Yeah, I’d consider it.
Daughter: And it’s only going to be a few minutes when they come…not a big investment on your part but it’s worth it.
Patient: Yeah.
Geriatrician : So…we’ll put in for the home safety assessment and…an appointment with the physical therapist… [Clinician proposes health care for common priority].
Daughter: Yeah.
Scenario 3: clinician responses to divergent responses related to patient’s driving cessation
A 87-year-old male Veteran living with dementia (Patient 3) attended the appointment with his wife and daughter. Several times during the appointment, the patient noted regret and disappointment at no longer being able to drive (“I’ll never get used to [not driving] I look out the window and see if my car’s there. I know it’s not”). His wife quickly responded, with a polite smile, “Stop focusing on the car, move on.” To manage the explicit divergent responses to the patient’s driving cessation, clinicians used validation, pivoting to other priorities, such as the importance of getting to medical appointments and the family’s vacation spot, and then proposed the use of a transportation service.Pharmacist: You have been driving since you were ten -- right?Daughter: That’s right [laughing] yeah. ….Wife: Yes, he has.Geriatrician: … It’s very difficult. It takes a while for you to at least… wrap your head around that oh I’m not gonna drive anymore…[clinician’s validation of priority; tone of empathy] but we wanna make sure that all your goals are being met regarding things that matter the most to you, like … going to your doctor’s appointments, going to [vacation home]. So …we spoke with to your sister last time and we talked to her about resources…transportation [resources] [clinician pivots to care option]. So, I was wondering if she had a chance to look at it?Daughter: Yeah, so mom arranged once so far to get transportation through the Council on Aging.Wife: Um, yeah.…Geriatrician : But I – I definitely hear what you’re [patient] saying, the fact that it is so different from, you know, how you have lived up until this point. Always being able to jump into the car and it does sound like this is an incredibly important thing to you to still be able to do all the things that you could. [validation, tone of empathy] So, I think that for our team that will be a big focus because it’s so important to you. So, I really am very hopeful that the DAV [Disabled American Veterans] might be a good opportunity to be able to come back for the monthly farmer’s market and the food bank. [clinician pivots to another care option] … [we] will start to … troubleshoot together about other ways to get you to the things that you enjoy doing [clinician reframes problem]. You know, it really is so difficult to have something that you used to look forward to but you can’t – you feel like you can’t do anymore, so we definitely wanna be as supportive as we can with that. That also brings me back to the point of [reducing] so many medical appointments…[so you can go to your vacation home].[clinician pivots to another priority]….
Specifically, the clinician re-stated and validated the patient’s priorities, and even suggested that modification to the number of appointments could be made to prioritize the patient’s value of returning to his home vacation. In addition, the clinicians then reframed and pivoted to other priorities the patient had expressed, such as getting to his medical appointments and receiving food truck service.
Cross-Scenario observations of clinicians’ non-verbal or para-verbal responses to divergence in perspectives
Clinicians also used non-verbal communication techniques when incongruence emerged between the patient and the caregiver. Specifically, they used such strategies consistently across medical visits and within visits, including in the three scenarios described above as the patient and the caregiver talked about their unique perspectives. Clinicians exhibited active listening such as making eye contact to exhibit interest and attentiveness, nodding to indicate empathy or understanding, and listening without interruption. Clinicians also exhibited warmth and humor, by engaging in casual conversation topics when they were raised by the patient or caregiver (e.g., chatting about an upcoming sport event that the patient was attending, and laughing at jokes made by the patient). When incongruence emerged between the patient and the caregiver, or when the patient did not agree with the clinician’s recommendation, as with the chair-rise exercise, clinicians continued to speak with warmth and calmness and without judgement. Without taking sides, clinicians still validated each party’s priority to carry the conversation forward.
Taken together, the clinician responses align with concepts of communication functions in medical visits [25]. Table 2 displays a crosswalk mapping these communication functions (responding to emotions, fostering relationships, managing uncertainty/divergence, information exchange, making decisions, and enabling self-management) with our codes related to clinician responses and themes. For example, the communication functions of responding to each party’s emotions and fostering the relationship are achieved by provider acknowledgement of patient or caregiver priorities or addressing socioemotional needs of each party. In this way, the clinician navigated divergence while allowing all parties to feel heard and fostering a sense that all parties were working toward a mutual goal of care.
Table 2. Crosswalk of Codes, Themes, and conceptual framework’s communication functionsCode(s) Related to Clinical Responses/Skills InvolvedThemes IdentifiedCommunication functionsClinician acknowledgment of caregiver prioritiesClinician acknowledgment of patient’s prioritiesClinician’s acknowledgement of differences between caregiver and patient priorities (acknowledgment of incongruence)Addressing socioemotional needsResponding to emotionsFostering relationshipsClinician reframes problem expressed by either the patient or caregiverClinician pivots to another priority or care optionSeeking common groundManaging uncertainty/divergenceClinician gives information about health careClinician proposes health care for common priorityProposal to care planningInformation exchangeMaking decisionsEnabling self-management
Discussion
Our study characterized older adults’ and family caregivers’ divergence in health and lifestyle priorities expressed by older adults and their family caregivers. The study also identified clinicians’ responses when managing divergence in priorities during medical visits. We explored the content of the communication because the functions carried out during medical visits (e.g., information exchange) (a) may have important health outcomes on patients and their family caregivers as noted by [25] and (b) presents a unique opportunity and setting to explore divergence of priorities, and (c) to provide clinicians with guidance for navigating these encounters.
During these exchanges, explicit and implicit incongruence emerged. Specifically, older adults and their family caregivers often did not explicitly state that they disagreed with one another, which may indicate their preference to avoid confrontation. Family caregivers may find it difficult or uncomfortable to openly disagree with patients during medical appointments, as they strive to balance their own self-expression with their support of patient involvement [6]. Patients may not express disagreement with their family caregivers during the medical visit due to potential difficulties comprehending discussed information [10] or have difficulty finding the right words to express what they want to say, if a certain level of cognitive impairment is present. Nonetheless, patients may feel ostracized, isolated, or inferior [19] when their family members and clinicians focus on and discuss their “weaknesses” in such detail. Patients’ behavior may, in turn, inadvertently spur family members to take a leading role in the medical visit [30] and therefore voice their own priorities more. This is consistent with differences between patients and caregivers’ levels of engagement and contributions during the medical visits we observed.
Clinical applications
Given these delicate and complex dynamics during medical visits, our analysis supports clinical strategies that foster candor and promote “balanced” involvement from both the patient and the family caregiver. Clinicians need to exhibit an openness to hearing and exploring divergent views [25]. Specifically, they need to convey (through verbal and non-verbal communication) to the patient and the family caregiver that both agreements and disagreements are normal and benefit from compromise [10]. If they do not, divergent views that may already be a source of relational strain can add to caregiver burden and patient’s own difficulty managing symptoms [25]. To demonstrate openness and promote perspective-taking by each dyad’s member during visits, clinicians could directly solicit patients’ thoughts on caregiver-expressed priorities and vice-versa. Another strategy to foster candor includes holding separate conversations with the patient and with the caregiver(s), prior to a joint meeting with both parties [8, 9, 20, 28]. This would allow patients and caregivers to voice priorities separately and subsequently come together to solve problems and decide on the next steps. This strategy is especially valuable for patients with cognitive impairment because, in separate conversations, clinicians could tailor and simplify information to help patients understand, encode, and retain it. Given that such communication skills take practice and education, clinicians may need training that includes role-playing related to disagreements (e.g., “act or verbalize your response to divergent views from various caregivers and patient surrounding driving”) and negotiation training [18]. Such training may be delivered via clinical consultation groups, webinars (which VA provides and continues to develop), and structured peer support. Such training could be instrumental in educating clinicians and pioneering further work in this area [21].
Several evidence-based clinical strategies observed in our study may be adopted by other clinicians. Validation and reframing are consistent with effective communication strategies used in health care [29], accompanied by elements of warmth and humor. Although not necessarily targeting disagreement, conveying warmth (smiling), calmness, and humor have been previously shown to benefit patients [11]. Patients and family caregivers also appeared comforted by the team’s counseling and care coordination, consistent with prior research [11, 13, 21], as such care coordination facilitates access to care. One way to strengthen effective communication is to form a clinical consultation group that targets disagreements during visits. Such a group could raise awareness of other difficult situations during medical visits with patients and their family caregivers. An example of one such difficult situation is of clinicians supporting caregiver-expressed priorities, which may build alliance with the caregiver but compromise rapport-building with the patient. A clinical consultation group could also be a forum for clinicians to discuss their own priorities during medical visits and how these priorities may influence the dynamics between patient and the caregiver and ultimately the outcome of the visit [3]. As such, these complexities during medical visits with patients and caregivers necessitate creative communication approaches and further study.
Study limitations and research implications
The strengths of the current exploration involve the inclusion of real-time conversations during medical visits with dyads or triads of patients, at least one family member, and multiple clinicians. Analysis of these conversations brought to light types of disagreements among the three parties and clinician strategies employed to carry out conversations on WMM. However, our study also had several limitations that can inform future research. At the time of this writing, we were unable to ascertain the level of cognitive impairment of two patients in our study due to lack of cognitive screening and neuropsychological evaluation performance. We therefore were unable to address how levels of cognitive status may affect the expression of priorities (e.g., frequency and types) in medical visits, though current literature in this area does indicate that cognitive status and expression of priorities via engagement in medical appointments are related [14]. Future work on patient-caregiver-clinician communication should measure cognition specifically and comprehensively, as cognition can be viewed as being on a continuum, spanning from no cognitive concerns to subjective cognitive decline to mild cognitive impairment to dementia. Another limitation pertains to the nature of appointments in our study setting. Within Veterans Affairs geriatrics clinics, medical visits may be concurrently attended by members of an interprofessional team, so that the variation and nature of provider responses may have been directly influenced by the presence of multiple professions, hindering generalizability of findings to medical visits attended by a single clinician. The initial visits that were the focus of the current paper were also lengthier (2 h = mean duration) than typical general medical visits that older adult civilians or VA patients may receive (i.e., 20–45-minute visits). Furthermore, while there was a research observer in these medical appointments taking field notes, we did not conduct a systematic analysis of non-verbal and para-verbal communication because these appointments were not video recorded. Further, our sample was not representative of different cultural backgrounds. Since extensive literature indicates that culture influences perceptions of mentation (cognition and mental health) [19] and thus may influence report of priorities, future research should investigate how cultural background, and sociodemographic factors influence “what matters most” conversations and navigation around divergence in priorities. Such research will inform the development of practice guidance for “what matters most” conversations in underserved populations and prepare health systems to deliver age-friendly care in a culturally informed manner. In addition to overcoming these study limitations, future studies should examine how longitudinal changes in types of and self-reported ratings of priorities influence patient and caregiver proximal and intermediate outcomes.
Summary/Conclusions
Our exploratory study focused on divergence in health and lifestyle priorities of patients with and without cognitive impairment and their caregivers and identified themes of clinicians’ responses in navigating such divergence. Although our study does not investigate distal outcomes, our study elucidates clinicians’ responses (a mix of addressing socioemotional needs, finding common ground, and care coordination to address commonly-held priorities) that likely foster proximal (perspective-taking by the patient and the caregiver) and intermediate outcomes (strengthen social support or mutual understanding within the dyad, access to care). In light of the exploratory nature of our findings, more research is still needed to understand divergence and clinical responses using larger and more ethnically and cognitively diverse samples of patients in various clinical settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davenport C, Ouellet J, Tinetti ME. Use of the Patient-Identified top health priority in care Decision-making for older adults with multiple chronic conditions. JAMA Netw Open. 2021;4(10). 10.1001/jamanetworkopen.2021.31496.10.1001/jamanetworkopen.2021.31496 PMC 855463734709390 · doi ↗ · pubmed ↗
- 2Lumivero. N Vivo (Version 12). 2023. https://www.lumivero.com.
- 3Miller LM, Whitlatch CJ, Lee CS, Caserta MS. Care values in dementia: patterns of perception and incongruence among family care dyads. Gerontologist. 2019;59(3):509–18.10.1093/geront/gny 008PMC 652447529546327 · doi ↗ · pubmed ↗
- 4Murawski A, Ramirez-Zohfeld V, Schierer A, Olvera C, Mell J, Gratch J, Brett J, Lindquist LA. Transforming a negotiation framework to resolve conflicts among older adults and family caregivers. Geriatr (Basel). 2023;8(2). 10.3390/geriatrics 8020036.10.3390/geriatrics 8020036 PMC 1003756236960991 · doi ↗ · pubmed ↗
- 5Reinhard SC, Caldera S, Houser A, Choula RB. Valuing the invaluable: 2023 Update. Strengthening supports for family caregivers. AARP Insight on the Issues. 2023. https://www.aarp.org/content/dam/aarp/ppi/2023/3/valuing-the-invaluable-2023-update.doi.10.26419-2Fppi.00082.006.pdf. Downloaded on November 14, 2025.