Palliative care interventions and outcome in patients with glioblastoma – a retrospective, single-center study
Lisa-Marie Lind, Anna Fischl, Elisabeth Goettl, Wolfgang Herr, Ulrich Kaiser, Oliver Koelbl, Ralf Linker, Julia Maurer, Markus J. Riemenschneider, Nils-Ole Schmidt, Martin Proescholdt, Tobias Pukrop, Peter Hau, Michael Rechenmacher, Elisabeth Bumes

TL;DR
This study shows that specialized palliative care may improve survival in glioblastoma patients, emphasizing the need for better integration of palliative care into treatment.
Contribution
The study demonstrates a significant association between specialized palliative care and prolonged survival in glioblastoma patients after adjusting for other factors.
Findings
Patients receiving specialized palliative care had a median survival of 16.9 months compared to 12.9 months for those without.
Specialized palliative care was significantly correlated with longer overall survival in a multivariable Cox regression analysis.
Palliative care interventions were widely available, but data on their impact in glioblastoma patients remains limited.
Abstract
Patients with glioblastoma (GB) not only suffer from a life-threatening oncological disease but also present with severe neurological symptoms and high psychosocial distress. The unfavorable prognosis and the early decline in neurological functions and activities of daily living, such as mobility, lead to a significant deterioration in quality of life aspects. The need for palliative care (PC) therefore arises at an early stage and increases as the disease progresses but is often inadequately assessed and treated. In this single-center, retrospective study, we investigated prognostic factors, survival outcomes and neuro-oncologically focused primary palliative care (nPPC) as well as specialized palliative care (SPC) interventions. Pearson’s Chi-square test and an univariable and multivariable binary logistic regression analysis were used to test the independence between categorical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
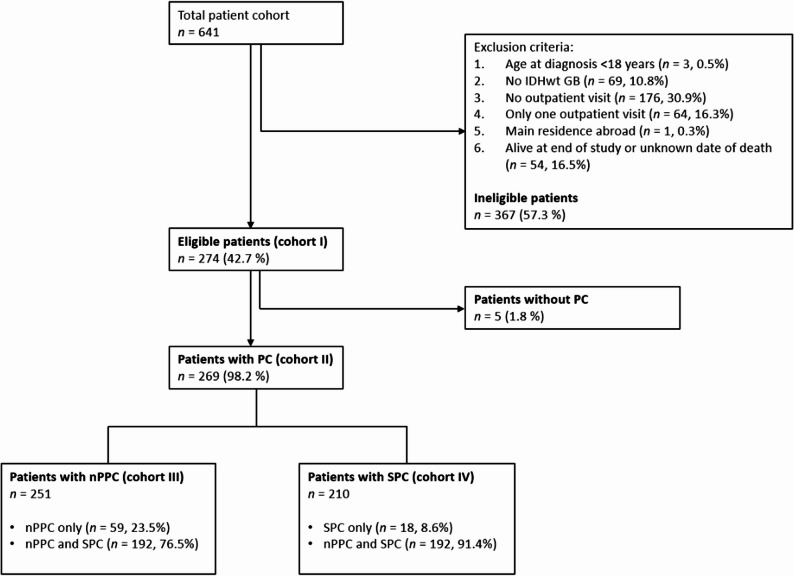 Figure 1
Figure 1- —Universitätsklinikum Regensburg (8921)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Palliative Care and End-of-Life Issues · Management of metastatic bone disease
Introduction
Glioblastoma (GB), isocitrate dehydrogenase wild type (IDHwt) (CNS WHO grade 4) [1], is the most common primary brain tumor diagnosed in adults [2]. The median overall survival (mOS) of all patients with GB remains unfavorable at 15–48 months according to meaningful clinical studies (depending on O-6-methylguanine-DNA methyltransferase (MGMT) promoter methylation status, treatment regimen, and WHO classification applied) [3–5]. Real-world data from the most recent CBTRUS report (2018–2022) reported a mOS of 8 months in patients with GB in the United States, with a one-year survival rate of only 48.7% [2]. Among therapy-independent prognostic factors, sex, age at first diagnosis, extent of resection, Karnofsky Performance Status Scale (KPS) at first diagnosis [4] and MGMT promoter methylation status are important prognostic factors [3].
Patients with GB not only suffer from a life-threatening oncological disease, but also from a severe neurological symptom burden including intracranial pressure, epileptic seizures, focal neurological symptoms such as hemiparesis and aphasia, neurocognitive dysfunction and personality changes as well as side effects of tumor therapies [6–10]. In addition to symptoms, patients feel distressed by limitations of their mobility, ability to work, social network and enjoyment of life [6, 11]. This entails a high psychosocial and emotional burden on patients and their caregivers, leading to reduced health-related quality of life (HR-QoL) [12–14].
Owing to the palliative character of GB, there is a high demand for palliative care (PC) throughout the course of the disease [15]. Here, primary palliative care (PPC) as well as specialized palliative care (SPC) are crucial [16]. PPC is provided by any medical practitioner and remains an integral part of standard care for critically ill patients. It covers basic symptom management (e.g. pain, depression) and initiates first conversations about prognosis and end of life. In specialized neuro-oncological care, this is frequently undertaken by neuro-oncologists, so we refer to this as neuro-oncologically focused primary palliative care (nPPC).
In contrast, SPC is carried out by palliative care specialists. SPC intervenes when symptoms are complex and the course of disease requires intensified psychosocial management [16–18]. SPC occurs in various inpatient and outpatient settings that all ensure integrative and interdisciplinary PC [19–21]. Inpatient palliative consultations are not equally accessible to all inpatients due to regional and structural differences [20]. Specialized palliative outpatient care (SPOC) tries to prevent hospitalization, enabling patients to live and die in their familiar environment [21].
The need for PC is often inadequately recognized, as assessment of symptoms is time-consuming and warrants awareness of the problem. As part of neuro-oncological certification systems, a screening for PC needs is often included [22]. Also based on these innovations, PC in neuro-oncology has gained more attention in recent years [18]. However, the evidence on PC - in particular on early PC - for patients with GB is still limited [23] and despite the overall intense research on glioma, topics on end-of-life care, HR-QoL, and psychosocial aspects are still underfocused [24]. The EANO guideline on palliative care of 2017 was the first that includes standards on symptom management, needs of patients and their caregivers and end-of-life care in neuro-oncology [25].
Still, studies are heterogenous and mostly retrospective in their design and show that the prevalence of SPC in patients with glioma differs substantially, with rates between 3% and 40%, depending on the tumor entities included and the treatment situation [26–29]. In most studies, SPC is integrated late in the course of the disease. In one study from 2013, the median time from first diagnosis to SPC referral was 111 days, whereas the median time from SPC referral to death was only 33 days [9]. More recent data also demonstrate that patients with high grade glioma are only referred to SPC in the end-of-life phase [27]. Overall, the number of patients who receive early PC remains small [30]. A recent prospective clinical study investigated the influence of early integration of PC (< 4 weeks after first diagnosis/recurrent diagnosis) on QoL of patients with GB and caregiver burden in a two-arm, randomized setting [31]. An analysis adjusted for time of death demonstrated an improvement in QoL of patients in the intervention group with early integration of PC. Data on survival outcomes for patients with GB depending on receiving PC are heterogeneous. The above-mentioned prospective study indicated a reduced OS for the intervention group with early integration of PC compared to the control group [31]. A retrospective analysis by Pando et al. including 85.380 patients with GB diagnosed between 2004 and 2017 observed a shorter two-year-survival in patients with PC compared to patients without PC, although it should be noted that PC was only observed in 3.28% of the study population [29]. Wu et al. retrospectively investigated data from 1997 to 2016 and found that the median survival time for GB patients with early PC integration was shorter than for patients without PC, while longer median survival times were observed in patients with late PC integration [30]. However, a retrospective analysis by Crooms et al. indicates that there may be a survival advantage for patients with high-grade gliomas who had early PC consultation compared to PC consultation at the end of life [27]. Furthermore, a systematic review by Koekkoek et al. concludes that the (early) integration of PC is essential to adequately address the needs of patients and caregivers, but the data available is still considered sparse [32].
Overall, data on PC in neuro-oncology are still sparse and heterogenous. Hardly any study examines both PPC and the various forms of SPC. Therefore, we investigated a range of PC interventions in patients with GB, which were related to prognostic factors as well as outcomes, providing a basis for a rational approach to PC in patients with GB.
Materials and methods
Study population
Patients with GB, IDHwt (CNS WHO Grade 4) [1] who were registered in the local tumor registry between January 2014 and February 2024 and filed in our hospital data management system were included in this retrospective single-center study. Main inclusion criteria were an age at diagnosis of 18 or above, a neuropathological diagnosis of GB, according to the WHO classification of 2021, at least two outpatient visits after diagnosis, main residence in Germany and death before end of study (Fig. 1). Patients who were still alive at the time of the last data assessment were excluded for statistical reasons, as the data on PC interventions is incomplete and censoring can lead to an overestimation or underestimation of survival times.
Figure 1 lists the exclusion criteria in more detail according to the number of patients and reasons for exclusion. Cohort I comprises all eligible patients, which are divided into Cohort II (patients with PC) and patients without PC. Cohort III includes all patients who received nPPC, while Cohort IV represents patients with SPC (detailed information is provided in Fig. 1).
Fig. 1. Patient cohorts regarding inclusion and exclusion criteria. Abbreviations: IDHwt, Isocitrate dehydrogenase wild type; PC, palliative care; nPPC, neuro-oncologically focused primary palliative care; SPC, specialized palliative care
Sociodemographic, clinical and treatment factors
Important demographic factors included date of birth, sex, age at first diagnosis, place of main residence and place of death. According to the WHO classification of 2021 [1], the histological or molecular diagnosis of GB was assessed. Patients who were initially diagnosed before 2021 underwent neuropathological reclassification according to the criteria of the 2021 WHO classification. Sex, age at first diagnosis, extent of resection, KPS at first diagnosis [33] and MGMT promoter methylation status were recorded as relevant prognostic factors. KPS is an established tool for assessing functional status in neuro-oncology and is an important aspect of prognosis assessment and treatment decisions [34]. Clinical and treatment-related aspects comprised primary therapy as well as date and type of any relapse/progression therapy, and the KPS at the respective stage of therapy. The last documented KPS refers to the most recent tumor progression in each patient. All abovementioned parameters were drawn from the electronic medical records.
Primary palliative care
In the context of this study, nPPC refers exclusively to the PPC that has been provided by neuro-oncologists at the Regensburg Brain Tumor Center. To qualify as nPPC, symptoms were not treatment-related side effects and were not based on the pre-morbid medical history of the patient. The start date of nPPC, initial symptoms and medical interventions were assessed and documented from electronic patient records. The symptoms were assigned to categories in line with the SPOC prescription, which were divided into subcategories in consultation with a panel of experts consisting of neuro-oncologists and PC specialists (Supplementary Table 1). Validity checks were carried out repeatedly to ensure good inter-rater reliability. For this purpose, data was assessed, and symptoms were assigned to categories/subcategories independently by two researchers (LML and EB). Possible discrepancies were discussed and led to modification.
Specialized palliative care
In view of SPC, the start date of SPC and all types of SPC interventions were further evaluated in detail. For inpatient palliative consultation, the start date, number of contacts and indications were drawn, and the reasons for consultation were assessed as symptoms of complex palliative care, consultation at first diagnosis, therapy goal setting, care coordination and other indications (Supplementary Table 2).
In evaluating the outpatient sector, the respective SPOC teams were individually queried. Patients were allocated to at least one SPOC team according to the postal codes of their main residence. An indication for SPOC is typically based on severe pain and/or neurological/psychiatric/psychological, cardiac/respiratory or gastrointestinal symptoms, ulcerating/exulcerating wounds/tumors, urogenital symptoms and some other symptoms (Supplementary Table 3) [35]. The survey also included standardized questions on start, duration and indication of SPOC, and number of in-person and phone contacts with SPOC. We further queried data on stays in a palliative care unit (PCU), hospice care and place of death. For patients who were not cared for by SPOC, we contacted their primary care physician for further information.
Study endpoints
The endpoints of our study include the receipt of tumor-specific therapy within the last 30 days prior to death, the OS and progression-free survival (PFS). Tumor-specific therapy contains interventions such as surgery, system therapy and radiotherapy. Supportive therapy such as antiseizure medication, corticosteroids and bevacizumab as therapy for cerebral edema was excluded. The PFS was defined as the time from diagnosis up to first relapse/progression or death.
Statistics
Pseudonymized data were assembled and recorded in IBM SPSS (Chicago, IL, USA) Statistics (Version 29). Continuous data was displayed as means, medians, standard deviations, minima, and maxima. A Student’s t-test was applied to compare the mean values in the case of a normal distribution of continuous variables. Categorical variables were characterized as absolute frequencies and relative percentages. The Pearson’s chi-square test was performed to test the independence between categorical variables. The Fisher’s exact test was applied if the sample size was too small. The level of significance was set at p < 0.05.
The correlation between SPC and tumor-specific therapy within the last 30 days before death was investigated with an univariable and multivariable binary logistic regression analysis. Possible prognostic confounders were assessed. A cut-off p-value of p < 0.2 in the univariable binary logistic regression analysis was defined as a selection criterion for possible confounders for the multivariable binary logistic regression analysis. The level of significance was set at p < 0.05 in the multivariable analysis.
The Kaplan-Meier method was used to estimate OS and PFS. Differences between groups were compared using the two-sided log-rank test with a level of significance at p < 0.05. A Cox proportional-hazards regression model was applied to assess the impact of SPC on OS and PFS. As possible confounders were included: sex, age at diagnosis, KPS at first diagnosis, MGMT promoter methylation and extent of resection. Parameters which were significant at the p < 0.2 level in the univariable cox regression analysis were included in the multivariable analysis. The level of significance was set at p < 0.05.
We defined SPC exposure as receipt of one or more SPC interventions after first diagnosis and therefore treated SPC as a time-fixed covariate (ever vs. never during the window). This reflects our interest in the association between receipt of SPC services and OS from diagnosis. Alternative approaches such as landmark analyses or time-dependent Cox models that treat SPC initiation as a time-varying treatment answer different causal contrasts (effects of initiating SPC at a particular time among survivors, or immediate hazard changes after SPC start) and are vulnerable here to selection bias or confounding by indication given that SPC is an ongoing, non-randomized service typically initiated in response to clinical deterioration.
Ethical and regulatory framework
The study was approved by the Regensburg University Institutional Ethics Review Board (vote no. 24-3606-104). Owing to the retrospective character of this analysis, no informed consent was required in accordance with local regulations. The data protection concept of the Department of Neurology – NeuroOncology at Regensburg Brain Tumor Center, which operates within the framework of the European General Data Protection Regulation and relevant national legislation, was applied. Our study was conducted in accordance with the STROBE checklist for observational studies (Supplementary Table 4).
Results
Patient cohorts and characteristics
A data query at the Regional Cancer Center identified 641 patients who were diagnosed with GB between January 01, 2014, and February 28, 2024, of whom 274 (42.7%) met the pre-specified inclusion criteria (Fig. 1, cohort I). Data on nPPC were available in all patients. Amongst them, we identified 138 patients with SPOC (50.4%); data were acquired in 137 of them (99.3%). A data request was sent to the primary care physician for patients who could not be identified by a SPOC team in 136 cases (49.6%), and 121 (89.0%) primary care physicians fully completed the request.
In cohort I, 158 (57.7%) patients were male and 151 (55.1%) were older than 60 years at first diagnosis. The MGMT promoter was methylated in 117 patients (42.7%), and 183 (66.8%) patients presented with a KPS of 90 or above, 79 (28.8%) patients with a KPS of 70–80, and 12 (4.4%) with a KPS below 70 at first diagnosis. Two hundred and sixty-nine (98.2%) patients received either nPPC or SPC or both (cohort II); of these, 251 patients received nPPC (cohort III; including nPPC only, n = 59, and combined nPPC/SPC, n = 192) and 210 patients SPC (cohort IV; including SPC only, n = 18, and combined nPPC/SPC, n = 192) (Table 1, Supplementary Tables 1 and 2). Age at first diagnosis and sex did not differ notably from the overall cohort (Supplementary Tables 5 and 6). Details on the course of therapy can be obtained from the authors upon reasonable request.
Table 1. Demographic and clinical characteristics of cohort I (n = 274)Valid NumberPercentAge at first diagnosis(years)20.0–49.93312.1%50.0–59.99032.8%60.0–69.99534.7%≥ 705620.4%SexMale15857.7%Female11642.3%MGMT Methylation StatusNo Methylation15757.3%Methylation11742.7%KPS at first diagnosis< 70124.4%70–807928.8%90–10018366.8%EpilepsyNo7527.4%Yes19972.6%Psycho-oncological careNo15355.8%Yes12144.2%nPPC and SPCNeither nor51.8%Yes, both19270.1%Only nPPC5921.5%Only SPC186.6%nPPCNo238.4%Yes25191.6%SPCNo6423.4%Yes21076.6%Place of deathAt home11140.5%PCU5018.2%Hospice3111.3%Hospital3111.3%Nursing home124.5%No data available3914.2%Total274100%Abbreviations: MGMT O-6-methylguanine-DNA methyltransferase, KPS Karnofsky Performance Scale, nPPC Neuro-oncologically focused primary palliative care, SPC Specialized palliative care, PCU Palliative care unit
Place of death
In cohort I, 111 (40.5%) patients deceased at home, whereas 50 (18.2%) patients deceased at a PCU, 31 (11.3%) at hospice, 12 (4.4%) patients in a nursing home and 31 (11.3%) in other medical departments of a hospital (Table 1). Details on cohort III and IV are shown in Supplementary Tables 5 and 6. In cohort IV, we further investigated whether SPC correlates with the place of death. Patients who deceased out of hospital received significantly more often SPC (89.0% vs. 75.3%; p = 0.006) (Table 2).
Table 2. Place of death in relation to SPCPlace of death in hospitalNoYesTotalX^2^ n (%) n (%) n (%) p SPCNo1711.0%2024.7%3715.7%0.006Yes13789.0%6175.3%19884.3%Total154100.0%81100.0%235100.0%Abbreviation: n Valid number, X2 Pearson’s Chi-square test
Neuro-oncologically focused primary palliative care (nPPC)
Characteristics of nPPC interventions
At the beginning of nPPC, 177 (70.5%) patients in cohort III were without relapse/progression, and 120 (47.8%) presented with a KPS of 90 or above (Supplementary Table 5). The mean time from first diagnosis to start of nPPC was 22.5 weeks; 21 (8.4%) patients received nPPC already before the initial diagnosis, 51 (20.3%) within the first week of diagnosis and 59 (23.5%) within 1–10 weeks. Patients obtained their first nPPC intervention on average 13 months before death, with 109 (43.4%) patients with their first nPPC intervention more than 12 months before death (Supplementary Table 5).
Symptoms and indications of nPPC
The most common symptom that did lead to the first nPPC intervention was seizures in 55 patients (21.9%). Additional nPPC interventions were caused by other neurological symptoms in 122 patients (48.6%) and non-neurological symptoms in 74 patients (29.5%) (Supplementary Table 7). During the entire course of disease, the most common indications of nPPC interventions were neurological symptoms in 241 patients (96%), followed by psychiatric symptoms in 138 patients (55.0%) and pain in 63 patients (25.1%) (Supplementary Table 8).
Specialized palliative care (SPC)
At the beginning of SPC, 66 (31.4%) patients presented with a KPS below 70 and a majority of 126 (60.0%) patients were in second or later relapse/progression (Supplementary Table 6). The mean time from first diagnosis to start of SPC was 72.4 weeks. Within 9–50 weeks of first diagnosis, 77 (36.7%) patients received their first SPC contact, whereas only 8 (3.8%) patients had their first contact within 8 weeks after diagnosis. The mean period from the start of SPC to death was 13.3 weeks, whereas 78 (37.1%) patients received their first SPC intervention within 3–10 weeks before death (Supplementary Table 6).
In cohort IV, 129 (61.4%) patients received inpatient SPC, of these 80 (38.2%) with inpatient palliative consultation and 82 (39.0%) on PCU (Supplementary Table 6). In the outpatient setting, 138 (65.7%) patients received long-time care from a SPOC, while 13 (6.2%) patients had a single contact with SPOC. A total of 31 (14.8%) patients were taken care of in the hospice (Supplementary Tables 6 and 9 to 15).
SPC and tumor-specific treatment at the end of life
Patients who had at least one SPC consultation (n = 210) did not receive tumor-specific treatment in the 30 days prior to death in 83.3% (n = 175) of cases, while 16.7% (n = 35) did receive tumor-specific treatment. The Pearson´s Chi-square test showed a significant difference between both groups (p < 0.001) (Supplementary Table 16). Next, a multivariable binary logistic regression analysis confirmed that patients who received SPC were significantly less likely to have a tumor-specific therapy in the last 30 days prior to death (p < 0.001; OR: 0.302; 95% CI: 0.157–0.584) (Table 3). Furthermore, patients with methylation of MGMT promoter had the same number of progressions/relapses than patients without (p = 0.604) and received the same number of systemic treatments (p = 0.245) but were less likely to receive a tumor-specific therapy in the last 30 days before death (p = 0.005; OR: 0.375; 95% CI: 0.190–0.739). Age at first diagnosis, sex and last documented KPS showed no significant influence on the receipt of a tumor-specific therapy at the end of life (Table 3).
Table 3. Univariable and multivariable binary logistic regression analysis of the influence of clinical characteristics on tumor-specific therapy in the 30 days prior to death (cohort I, n = 274)VariableCategory (n)Univariable binary logistic regression analysisMultivariable binary logistic regression analysis p ORLower 95%-CIUpper95%-CI p ORLower 95%-CIUpper95%-CISPCNo (64)1.0001.000Yes (210)< 0.0010.3330.1790.621< 0.0010.3020.1570.584SexMale (158)1.0001.000Female (116)0.2380.6980.3841.2680.8730.9490.4961.813Age at first diagnosis^2^0.1770.9830.9591.0080.2160.9830.9581.010Last documented KPS^3^0.0661.0200.9991.0410.1171.0170.9961.040MGMT promoter methylationNo (157)1.0001.000Yes (117)0.0030.3780.1980.7190.0050.3750.1900.739Abbreviations: OR Odds Ratio, CI Confidence Interval, SPC Specialized palliative care, KPS Karnofsky Performance Scale^2^Age, as a continuous variable^3^KPS, as a categorical variable with 10 point increments
SPC and survival
Next, we analyzed the association between SPC and survival. The mOS was 16.9 months (95% CI: 14.5–19.3 months) in patients with at least one SPC consultation (n = 210) vs. 12.9 months (95% CI: 10.8–15.1 months) in patients without (n = 64) (p = 0.100) (Supplementary Fig. 1). In exploratory analyses, 148 (70.5%) patients with at least one SPC consultation vs. 37 (57.8%) without were alive at one year and 63 (30.4%) vs. 15 (23.4%) were alive at two years after diagnosis (Supplementary Fig. 1). The multivariable Cox proportional-hazards model showed that receiving at least one SPC consultation is associated with a longer OS (p = 0.017, HR: 0.707; 95% CI: 0.532–0.939) (Table 4). Furthermore, the following parameters revealed also a significant correlation with extended OS: female sex (p = 0.018, HR: 0.740; 95% CI: 0.577–0.949), complete resection (p < 0.001, HR: 0.615; 95% CI: 0.479–0.788) and methylated MGMT promoter (p < 0.001, HR: 0.379; 95% CI: 0.289–0.496). An older age at diagnosis correlated with a shorter OS (p < 0.001, HR: 1.028 per year; 95% CI: 1.016–1.041) (Table 4).
Table 4. Cox proportional-hazards regression model of the influence of clinical aspects on OS (cohort I with n = 274)VariableCategory (n)Univariable coxregression analysisMultivariable coxregression analysis p HRLower 95%-CIUpper95%-CI p HRLower 95%-CIUpper95%-CISPCNo (64)1.0001.000Yes (210)0.1080.7940.6001.0520.0170.7070.5320.939SexMale (158)1.0001.000Female (116)0.0790.8050.6321.0250.0180.7400.5770.949Age at first diagnosis^2^0.0031.0171.0061.028< 0.0011.0281.0161.041KPS^3^ at first diagnosis0.1470.9930.0941.0020.3670.9950.9851.005MGMT promoter methylationNo (157)1.0001.000Yes (117)< 0.0010.4750.3690.611< 0.0010.3790.2890.496Macroscopic complete resectionNo (157)1.0001.000Yes (117)0.0010.6690.5250.852< 0.0010.6150.4790.788Abbreviations: OS Overall survival, HR Hazard Ratio, CI Confidence Interval, KPS Karnofsky Performance Scale, SPC Specialized palliative care^2^Age, as a continuous variable^3^KPS, as a categorical variable with 10 points increments
The median PFS (mPFS) did not differ significantly between the two groups: mPFS was 7.8 months (95% CI: 6.763–8.941 months) for patients with at least one SPC consultation (n = 210) vs. 7.1 months (95% CI: 6.002–8.191 months) for patients without (n = 64) (p = 0.775) (Supplementary Fig. 2). In exploratory analyses, 53 (25.2%) vs. 17 (26.6%) patients with at least one SPC consultation were relapse/progression-free and/or alive at one year after diagnosis and 17 (8.1%) vs. 5 (7.8%) at two years after diagnosis (Supplementary Fig. 2). In accordance with this, our multivariable Cox proportional-hazards model demonstrated no significant correlation of SPC and PFS (p = 0.496). Hence, patients with a complete resection (p < 0.001, HR: 0.651; 95% CI: 0.509–0.833) and patients with a methylated MGMT promoter (p < 0.001, HR: 0.401; 95% CI: 0.306–0.527) had a prolonged PFS (Supplementary Table 17).
Discussion
Data on the impact of PC on the clinical course and survival of patients with GB are scarce [23]. In this retrospective study, we evaluated different types of PC interventions and their association with treatment patterns and outcomes in a single-center sequential cohort of 274 patients with GB. To our knowledge, this study marks the first complete evaluation of inpatient and outpatient nPPC and SPC interventions in patients with GB.
Whereas the positive impact of PC on symptom control and HR-QoL on patients with a life-limiting disease has been proven in several studies [36], data on the association of PC and survival outcomes, particularly in GB, is scarce and heterogenous. Our retrospective study contributes new scientific insights highlighting an association between SPC and prolonged OS in patients with GB in a real-world setting. In some clinical studies, partly retrospective [29, 30] but also prospective [31], a correlation between PC and reduced survival in patients with GB was observed. There is also data suggesting a positive association of survival outcomes and PC in patients with GB depending on PC referral prior to end of life or during end of life [27]. However, comparability is severely restricted due to methodological differencies: some studies covered different time periods [27, 29–31], PC rates were low [29], or the aim was to investigate early integration of PC [30, 31]. Two published studies in patients with gliomas had severe weaknesses, as they did not exclusively refer to GB and they did not regard both inpatient and outpatient SPC, leading to a underreporting of PC interventions [23, 29]. Other studies focused on comparing early and late integration of PC [27, 29, 31], whereas in our setting, PC supply was included irrespective of timing. Our study does not oppose previous publications on this point, but rather enriches them with a real-world setting.
There are some hypotheses to consider regarding the association between SPC and prolonged survival in this cohort. This could be due to a slower disease progression that allows integration of SPC, while patients with a rapid progression may not have enough time to integrate SPC. However, we hypothesize that improving symptom control and HR-QoL enhances the patients` overall health and may lead to prolonged survival, as shown in other tumor entities [37, 38]. SPC is based on a multidimensional approach with validated assessments and established therapeutic interventions that go beyond the scope of nPPC. Therefore, the inclusion of SPC in standard neuro-oncological care, especially at an early stage of the disease, may help to ensure the most appropriate and effective as well as tolerable administration of cancer therapy.
In our cohort, more than 90% of patients with GB received nPPC, and the indications for nPPC were primarily neurological. This study was conducted in a neuro-oncological setting, so neurological indications were reliably recorded, but indications from other specialties may have been underestimated. Nevertheless, this highlights, that the medical needs of this patient group are not equivalent to those of other tumor entities and require special expertise for their treatment [39]. This also emphasizes that neuro-oncologists must be alerted in view of PC needs and interventions. While PPC is gaining importance in almost all specialist areas and first efforts are being made to define nPPC interventions for neurological patients more precisely [18], nPPC is not yet an integral part in most neurological residency programs [40].
Recent published data reveal a heterogeneous SPC rate in neuro-oncological patients varying between 3 and 40%, depending on the specific tumor entity, the definition of SPC interventions and the method of data collection [26–29]. The level of SPC supply in our patient cohort exceeds the literature references by far, with 76.6% of patients receiving SPC. The reasons for that superior rate must be evaluated in more detail, but they may be, amongst others, that our study was performed in an established certified brain tumor center with a direct affiliation to a university PC center and that we included both inpatient and outpatient settings. In our SPC cohort, 65.7% of patients were integrated into a SPOC team, reflecting the high needs that reach beyond an inpatient stay. The high rate could also be a hint that the implementation of SPC in patients with GB is advancing. Interestingly, amongst the German neuro-oncological certification system that includes a mandatory evaluation of palliative needs from 2023 on, the rates of PC integration vary from 0 to 100% with a median of 26.2% in 2022 [41]. To date, only 35% of neuro-oncological sites in Germany include PC specialists in tumor boards [42]. An increased attendance by PC specialists could reduce the barriers to initiation of SPC and strengthen interdisciplinary cooperation.
Nonetheless, PC integration typically occurs late. The mean time from first diagnosis to start of SPC was 72.4 weeks, with only 8 patients (3.8%) referred to SPC within 8 weeks of diagnosis - contrary to the ASCO guidelines, which recommend early integration within 8 weeks of first diagnosis [43]. A survey among 46 German neuro-oncology sites showed that only 28% of sites refer their patients to PC within first diagnosis [42]. Owing to the rapid progression, high symptom load and reduced life expectancy of patients with GB, the integration of SPC can be unfortunately considered as delayed in most cases.
Several studies proved that SPC is of high benefit for cancer patients [36]. There is recent evidence, that early integration of PC improved QoL, mood and PC problems in patients with GB [31]. However, there are remaining barriers to the initiation of SPC in clinical practice, especially at an early stage of the disease. This may include persistent stigmatization of SPC, leading to the assumption that SPC is not compatible with tumor therapy and is inevitably associated with the end of life [44, 45]. This problem is not only evident in the area of SPC, but also analogously in PC in hospices, which further underscores this point [46, 47]. We hypothesize that an international definition of early integration of SPC and standardized screening assessments for SPC needs is essential. However, cultural and regional specifications may interfere with such a standardization.
Importantly, we demonstrated that patients who received SPC were significantly less likely to have a tumor-specific therapy in the last 30 days prior to death, consistent with the results of previous studies [48]. In accordance to international guidelines, patients with a KPS below 70 are considered ineligible for tumor therapy, at least in a non-curative setting [25]. However, no association between the last documented KPS and the receipt of tumor-specific therapy within the last 30 days of life could be observed. It should be noted that the last documented KPS refers to the most recent tumor relapse/progression in each patient and therefore a temporal variation in this parameter may appear. To this day, simultaneous tumor-specific therapy and PC is not standard practice. A recommendation for early integration of PC clearly argues against this strict separation of tumor-specific therapy and PC, as commonly done in the USA [43], the Netherlands, Australia and New Zealand. We therefore advocate to overcome this strict separation, enabling a simultaneous application of both tumor-specific therapy and PC.
Remarkably, patients with a methylated MGMT promoter status are less likely to receive tumor-specific therapy in the last 30 days before death. Although the patient group with MGMT promoter methylation in our cohort does not differ in the total number of relapse/progression therapies, the treatment regimens are most likely spread over an extended period, as the disease of these patients is frequently progressing less rapidly [4]. Differences in the extent of treatment and care requirements exist even within the same tumor entity, so further research on treatment factors associated with PC referral is needed.
There are several limitations to this study. This is a single-center analysis in a certified brain tumor center with a direct affiliation to a certified university PC center and a wide rural outreach. Results may vary in multi-center studies or in centers with a more urban population, different sociodemographic, cultural background or without an established brain tumor or PC center. However, the Regensburg Brain Tumor Center represents average quality standards of the German certification system. Furthermore, due to the retrospective design, it is possible that symptoms and PC interventions are not fully recorded. The retrospective assignment of symptoms to categories and subcategories may also be subject to bias, although we have performed repeated validity checks. However, the high rate of both nPPC and SPC suggests that the documentation is largely complete. Furthermore, recording PPC by primary care physicians was not possible owing to a lack of documentation. However, we consciously focused on collecting data on nPPC, as this is a special feature of care for patients with GB in a brain tumor center setting. As a result of the retrospective design, the timing of data collection, such as the last documented KPS, varies according to the individual clinical course, which may lead to a potential inaccuracy. Patients who were still alive at the time of the last data assessment were excluded from the analysis for methodological reasons, which could, however, lead to bias. Lastly, the retrospective nature of the study did not allow us to include caregivers. Future research should address the problems of caregivers and their potential for the patient’s disease trajectory.
This study also contains important strengths. We analyzed a large and homogeneous cohort of patients with GB, reclassified in the WHO classification from 2021, who were treated at a major brain tumor site over a period of 10 years. By collecting data not only from medical records, but also through personal queries of SPOC teams and primary care physicians, it was possible to achieve a high level of data quality. In addition, we collected data from the inpatient and outpatient setting, and data from nPPC and SPC, making this cohort unique in literature.
As a major result, we show a positive association between OS and SPC in our Kaplan Meier estimation as well as multivariable regression analysis. The next steps will be to verify our data in an independent cohort and to develop a prospective strategy for the early and full implementation of PC for patients with GB.
Conclusion
We conclude that patients with GB benefit from the implementation of both nPPC and SPC. As this is not standard for all patients with GB, utmost efforts should be made to incorporate PC into the early care of every patient with GB within a standardized framework. This study further highlights the importance of future research on a cross-sectional approach to identify PC needs as well as the kind and frequency of interventions in this highly burdened patient group, including caregivers. Demographic changes and more effective tumor therapies may lead to an increase in long-term disease trajectories and less rapid progression, which will make PC even more relevant in the future. Therefore, further research should focus on the ideal timing of PC integration and on identifying patient groups who are most likely to benefit from PC.
Supplementary Information
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-oncology 2021; 23(8):1231–51. Available from: URL: https://pubmed.ncbi.nlm.nih.gov/34185076/.10.1093/neuonc/noab 106PMC 832801334185076 · doi ↗ · pubmed ↗
- 2Price M, Ballard CAP, Benedetti JR, Kruchko C, Barnholtz-Sloan JS, Ostrom QT. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2018–2022. Neuro-oncology. 2025; 27(Supplement_4):iv 1-iv 66. Available from: URL: https://pubmed.ncbi.nlm.nih.gov/41092086/10.1093/neuonc/noaf 194PMC 1252701341092086 · doi ↗ · pubmed ↗
- 3Hegi ME, Diserens A-C, Gorlia T, Hamou M-F, de Tribolet N, Weller M, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352(10):997–1003. Available from: URL:. https://pubmed.ncbi.nlm.nih.gov/15758010/10.1056/NEJ Moa 04333115758010 · doi ↗ · pubmed ↗
- 4Stupp R, Taillibert S, Kanner A, Read W, Steinberg D, Lhermitte B et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma: A Randomized Clinical Trial. JAMA. 2017; 318(23):2306–16. Available from: URL. https://pubmed.ncbi.nlm.nih.gov/29260225/10.1001/jama.2017.18718 PMC 582070329260225 · doi ↗ · pubmed ↗
- 5Armstrong TS, Vera-Bolanos E, Acquaye AA, Gilbert MR, Ladha H, Mendoza T. The symptom burden of primary brain tumors: evidence for a core set of tumor- and treatment-related symptoms. Neuro-oncology. 2016; 18(2):252–60. Available from: URL. https://pubmed.ncbi.nlm.nih.gov/26289592/10.1093/neuonc/nov 166PMC 472418026289592 · doi ↗ · pubmed ↗
- 6Peeters MCM, Dirven L, Koekkoek JAF, Gortmaker EG, Fritz L, Vos MJ et al. Prediagnostic symptoms and signs of adult glioma: the patients’ view. Journal of neuro-oncology. 2020; 146(2):293–301. Available from: URL. https://pubmed.ncbi.nlm.nih.gov/31894516/10.1007/s 11060-019-03373-y 31894516 · doi ↗ · pubmed ↗
- 7Coomans MB, Dirven L, Aaronson NK, Baumert BG, van den Bent M, Bottomley A et al. Symptom clusters in newly diagnosed glioma patients: which symptom clusters are independently associated with functioning and global health status? Neuro-oncology. 2019; 21(11):1447–57. Available from: URL. https://pubmed.ncbi.nlm.nih.gov/31682733/10.1093/neuonc/noz 118PMC 682782431682733 · doi ↗ · pubmed ↗
- 8Lin E, Rosenthal MA, Eastman P, Le BH. Inpatient palliative care consultation for patients with glioblastoma in a tertiary hospital. Internal Medicine Journal. 2013; 43(8):942–5. Available from: URL. https://pubmed.ncbi.nlm.nih.gov/23919337/10.1111/imj.1221123919337 · doi ↗ · pubmed ↗