Frequency and risk factors of carotid atherosclerosis in patients with coronary artery disease
Mohamed El-feky, Sherif Aboushara, Amr Zaki, Mohamed Loutfi, Ahmed Elhfnawy

TL;DR
This study finds that most patients with coronary artery disease also have carotid atherosclerosis, with older males and those with severe heart disease being at higher risk.
Contribution
The study provides new empirical evidence on the prevalence and risk factors of carotid atherosclerosis in CAD patients using an observational approach.
Findings
Carotid atherosclerosis was detected in 71.8% of patients with coronary artery disease.
Age ≥60 years, male sex, and ≥3-vessel CAD were independently associated with carotid atherosclerosis.
A syntax score >17 independently predicted carotid atherosclerosis in age- and sex-adjusted models.
Abstract
Carotid Atherosclerosis is more prevalent among patients with coronary artery disease (CAD). To the best of our knowledge, research on the prevalence of carotid atherosclerosis in CAD patients is mainly based on retrospective cohorts or registries. We aimed to investigate the frequency of carotid atherosclerosis among patients with angiographically proven CAD and to investigate, whether carotid atherosclerosis is more prevalent in special subgroups. We recruited consecutive patients with angiographically proven CAD, who presented to our cardiology department with manifestations of ischemic heart disease. Carotid atherosclerosis was assessed using ultrasound. We included 103 patients in our study. Eighty-three (80.6%) patients were males, the mean (± SD) age was 58 (± 9) years. Carotid atherosclerosis was detected in 74 (71.8%) patients. Of those, 6 patients (5.8%) had ≥ 50% stenosis.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
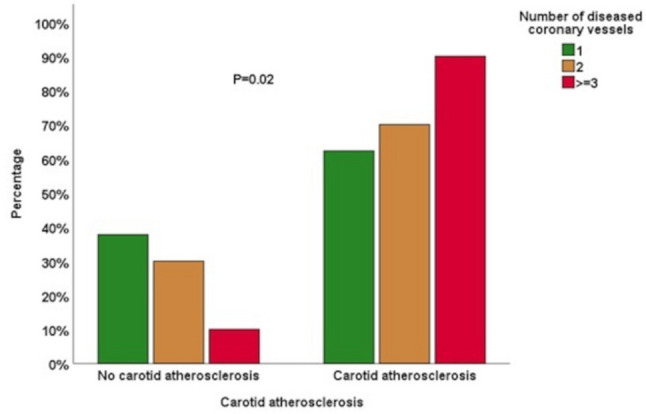 Figure 1
Figure 1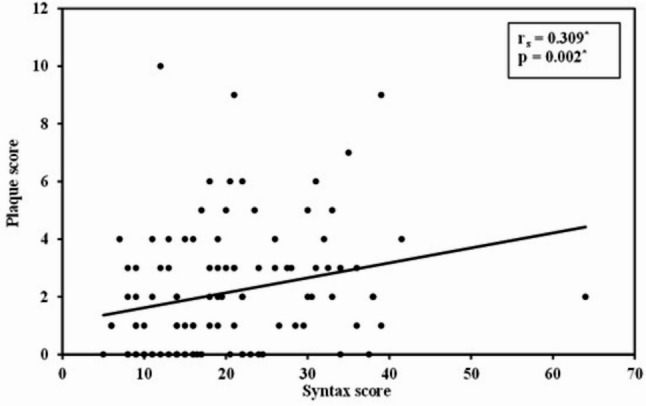 Figure 2
Figure 2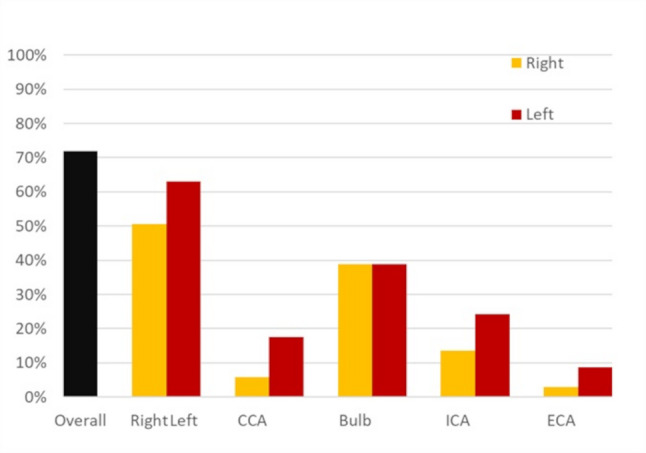 Figure 3
Figure 3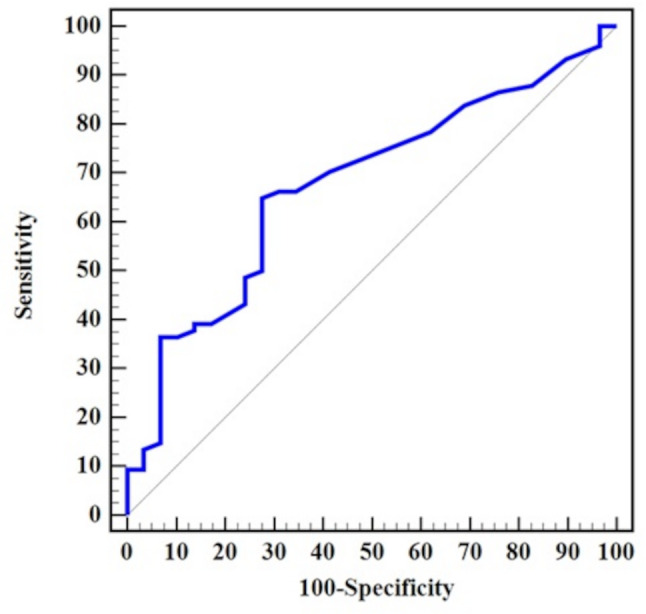 Figure 4
Figure 4- —Alexandria University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and Carotid Artery Diseases · Cardiovascular Health and Disease Prevention · Cardiovascular Disease and Adiposity
Background
Atherosclerosis is the most common cause of death worldwide [1]. Atherosclerosis is a systemic disease that affects multiple vascular beds including the coronary vessels causing ischemic heart disease as well as the carotid arteries posing the patients at risk of ischemic strokes [1, 2]. Myocardial infarction, stroke, vascular mortality, or rehospitalization rates at three-year follow-up are 40.5% for patients affected by symptomatic disease in multiple arterial systems and 25.5% for patients with symptomatic disease in one arterial system [3]. Furthermore, high burden of carotid plaques is an important predictor of new-onset myocardial infarction [4]. Over the past decades, vascular mortality has significantly decreased in high-income countries [5]. However, vascular mortality did not dramatically decline in low- and middle-income countries [5]. Routine screening for asymptomatic carotid atherosclerosis is not recommended in the general population [6]. Nevertheless, among patients with multiple risk factors, screening for carotid atherosclerotic disease may be considered [7]. Ultrasound is a reliable cost effective method to assess carotid atherosclerosis [8]. Increased carotid intima-media thickness as well as carotid plaque burden are more prevalent among patients with coronary atherosclerotic disease (CAD) [9, 10]. To the best of our knowledge, studies regarding the prevalence of carotid atherosclerosis among patients with CAD are mostly based on registries or retrospective cohorts. In the current work, we aimed to investigate the frequency of carotid atherosclerosis in a sample of patients with angiographically proven CAD and to find out, whether carotid atherosclerosis is more prevalent in special subgroups of patients with CAD.
Methods
In the current observational study, we prospectively recruited successive patients with angiographically proven significant CAD. The patients presented to the cardiology Department in Alexandria University Hospital because of ischemic heart manifestations in the period between March 2023 and January 2024 and received coronary angiography. CAD was defined as a lumen diameter stenosis of > 70% in ≥ 1 major coronary artery. Previous stroke or transient ischemic attacks were exclusion criteria for the current study. Patients were asked about their willingness to participate in our study. Those who signed an informed consent received carotid ultrasound examination.
Significant CAD was categorized into one of the following groups according to the number of diseased vessels: 1-vessel disease (i.e. patients with disease in 1 vessel), 2-vessel disease (i.e. patients with disease in 2 vessels or left main trunk disease without right coronary artery stenosis), ≥ 3-vessel disease (i.e. patients with disease in 3 vessels or left main trunk disease with right coronary artery stenosis or patients with disease in 3 vessels and the left main trunk disease). The syntax score I was calculated for each patient from the coronary angiographic images (syntaxscore.org). This score quantifies the extent and complexity of CAD by assessing the number of stenotic lesions with ≥ 50% stenosis in vessels ≥ 1.5 mm in diameter. It further encompasses anatomical factors including total occlusions, bifurcations, presence of calcified lesions, vascular tortuosity and lesion length. Atherosclerosis of carotid artery was assessed using duplex ultrasound examination by a single experienced investigator (AE) with ≥ 10 years of experience in neurovascular ultrasound. Plaque assessment was performed blinded to medical history and cardiovascular risk profile. The examination was done for academic research purposes, so that excessive attention was paid for each patient to detect carotid plaques. We examined our patients using the following ultrasound machine: Philips ClearVue 350 (Philips HealthCare, Best, Netherlands) using 4–12 MHz linear array probe. Ultrasound was performed while subjects were lying supine with the head slightly turned away from the side being scanned and the neck slightly extended. We examined the following segments: common carotid artery, carotid bifurcation, internal and external carotid arteries on both sides. The plaque was defined according to the Mannheim Carotid Intima–Media Thickness and Plaque Consensus as a focal lesion in the vessel wall that is at least 1.5 mm thick and protrudes into the vascular lumen [11]. To calculate the plaque score, the carotid artery was divided into 4 segments (common carotid artery, bifurcation, and internal and external carotid artery), and plaques were evaluated in each segment [12]. The diameter of the largest plaque in each segment was measured. Plaque diameters ≥ 1.5, ≥ 2.5, and ≥ 3.5 mm received 1, 2, and 3 points, respectively. The point scores for each of the 4 segments were summarized into a total plaque score, ranging from 0 to 24 points [12]. If a plaque was detected, the degree of stenosis was calculated using the hemodynamic criteria of the North American Symptomatic Carotid Endarterectomy Trial (NASCET) [13]. Hypertension was defined as blood pressure ≥ 140/90 mmHg in at least 2 different measurements or current use of antihypertensive medications [14]. Diabetes mellitus was defined as Hemoglobin A1c ≥ 6.5% or current use of antidiabetic medications [15].
Statistical analysis
The statistical Package for Social Sciences (SPSS) software version 25 (SPSS, Chicago, IL, USA) was used for data analysis. Continuous variables were expressed as mean ± SD for normally distributed data and as median (interquartile range) for abnormally distributed data. Statistical analysis of categorial data were performed with the χ2 or Fischer exact test (if n < 5). Multivariate binary logistic regression analysis was performed to detect independent predictors of carotid artery atherosclerosis with inclusion of variables that showed p < 0.1 in the univariate analysis. We conducted a receiver operating curve (ROC) for the relation between syntax score and carotid atherosclerosis. A cut-off value for the syntax score was calculated using the Youden-index. A value of P < 0.05 was considered statistically significant.
Results
We included 103 patients in our study. Eighty-three (80.6%) of our patients were males, the mean (± SD) age was 58 (± 9) years. The demographic and clinical characteristics of our study population are presented in Table 1 and the comparison of variables between patients with and without carotid atherosclerosis are shown in Table 2. Carotid atherosclerosis was diagnosed in 74 (71.8%) patients. Specifically, 67 (65.1%) patients had non-stenotic plaque, 1 (1%) patient had 20–40% stenosis and 6 (5.8%) patients had ≥ 50% stenosis. Patients with carotid atherosclerosis were older, with a median (IQR) age of 60 (53–67) years, compared to 55 (48–61) years in those without carotid atherosclerosis (p = 0.01). The Syntax score was also higher among patients with carotid atherosclerosis, with a median (IQR) of 20 (14–30) versus 14 (11–21) in those without (p = 0.006). Non–ST-elevation myocardial infarction (NSTEMI) was more prevalent among patients with carotid atherosclerosis; 20.3% (n = 15) of these patients had NSTEMI compared to 3.4% (n = 1) of those without carotid atherosclerosis (p = 0.04). Carotid atherosclerosis was found in 33 patients (62.3%) with 1-vessel disease, 14 patients (70%) with 2-vessel disease and 27 patients (90%) with ≥ 3-vessel disease (p = 0.02) as shown in Fig. 1. The distribution of atherosclerosis across different carotid segments on both sides is illustrated in Fig. 2. Moreover, we observed a statistically significant positive correlation between syntax and plaque score (ρ 0.31, p = 0.002). The regression line showing this relation is shown in Fig. 3. In the ROC curve, a syntax score > 17 yielded a sensitivity of 64.9% and specificity of 72.4% for carotid atherosclerosis (AUC 0.68, 95% CI 0.57–0.79, p = 0.006) as shown in Fig. 4. Furthermore, we performed a univariate regression model to measure the strength of association between various variables and carotid atherosclerosis as shown in Table 3. Using a multivariate binary logistic regression adjusted for age and sex, we found that age ≥ 60 years (OR 5.1, 95% CI 1.64–15.86, p = 0.005), male sex (OR 3.61, 95% CI 1.03–12.67, p = 0.045), and presence of ≥ 3-vessel coronary heart disease (OR 4.18, 95% CI 1.06–16.51, p = 0.04) were related to carotid atherosclerosis as shown in Table 4. In another age- and sex dependent multivariate logistic regression, syntax score > 17 independently predicted carotid atherosclerosis (OR 4.51, 95% CI 1.68–12.16, p = 0.003) as shown in Table 5.
Table 1. Baseline characteristicsCharachteristicNo. (%)Male sex, n (%)83 (80.6%)Age (years), median (IQR), mean (± SD) 59 (51–65), 58 (± 9)Hypertension, n (%)68 (66%)Diabetes mellitus, n (%)55 (53.4%)Current smoking, n (%)75 (72.8%)Chronic coronary syndrome, n (%)67 (65%)Unstable angina, n (%)5 (4.9%)NSTEMI, n (%)16 (15.5%)STEMI, n (%)54 (52.4%)History of PAD, n (%)11 (10.7%)Syntax score median (IQR)19 (13–27) Mild (≤ 22), n (%)69 (67%) Moderate (23–33), n (%)21 (20.4%) Severe (> 33), n (%)13 (12.6%)No. of diseased coronary vessels 1-vessel disease53 (51.5%) 2-vessel disease20 (19.4%) ≥3-vessel disease30 (29.1%)Carotid plaque score, median (IQR)2 (0–3)Carotid atherosclerosis, n (%)74 (71.8%) Non-stenotic plaque67 (65.1) 20–40% stenosis1 (1%) 50% stenosis6 (5.8%)IQR Interquartile range, NSTEMI Non-ST-Elevation myocardial infarction, STEMI ST-Elevation Myocardial infarction, PAD Peripheral arterial disease
Table 2. Comparison of variables between patients with and without carotid atherosclerosis (n = 103)VariableNo atherosclerosis (n = 29)Atherosclerosis (n = 74)P-valvueAge in years, median (IQR)55 (48–61)60 (53–67)0.01Male sex, n (%)21 (72.4%)62 (83.8%)0.19Diabetes mellitus, n (%)15 (51.7%)40 (54.1%)0.83Hypertension, n (%)17 (58.6%)51 (68.9%)0.32Current smoking, n (%)19 (65.5%)56 (75.7%)0.3NSTEMI1 (3.4%)15 (20.3%)0.04STEMI19 (65.5%)35 (47.3%)0.1Syntax score14 (11–21)20 (14–30)0.006**IQR* Interquartile range, NSTEMI Non-ST-Elevation myocardial infarction, STEMI ST-Elevation Myocardial infarction*Statistically significant results
Fig. 1. Relation between the number of diseased coronary vessels and carotid atherosclerosis
Fig. 2. Distribution of atherosclerosis among different carotid segments on both sides (CCA: common carotid artery, ECA: external carotid artery, ICA: internal carotid artery)
Fig. 3. Regression line showing the relation between syntax score and carotid plaque score (n = 103)
Fig. 4ROC curve showing the relation between Syntax score and carotid atherosclerosis. A cut-off syntax score > 17 yielded a sensitivity of 64.9% and specificity of 72.4% for carotid atherosclerosis (AUC 0.68, 95% CI 0.57–0.79, p = 0.006). The cut-off was calculated using the Youden-index
Table 3. Univariate logistic regression analysis for the parameters affecting carotid atherosclerosisUnivariateOR (95%CI) p Male1.97 (0.71–5.47)0.19Age ≥ 60 years4.13 (1.57–10.85)0.004Hypertension1.57 (0.64–3.8)0.32Diabetes Mellitus1.1 (0.47–2.6)0.83Current smoking1.64 (0.65–4.16)0.30PAD4.38 (0.53–35.84)0.17Number of diseased coronary vessels 1-vessel disease Reference 2-vessel disease1.41 (0.47–4.27)0.54 ≥ 3-vessel disease5.46 (1.46–20.33)0.01CI: Confidence interval, OR: Odd`s ratio, PAD: Peripheral arterial disease* Statistically significant results
Table 4. Multivariate logistic regression analysis for the parameters affecting carotid atherosclerosisMultivariateOR (95%CI) p Male3.612 (1.03–12.67)0.045Age ≥ 60 years5.1 (1.64–15.86)0.005Number of diseased coronary vessels 1-vessel disease Reference 2-vessel disease1.21 (0.37–3.93)0.75 ≥ 3-vessel disease4.18 (1.06–16.51)0.04Hosmer Lemeshow Test0.17CI* Confidence interval, OR Odd`s ratio, PAD Peripheral arterial disease* Statistically significant results#: Variables with p < 0.1 in the univariate analysis were included in the multivariable regression, with adjustment for age and sex
Table 5. Univariate and multivariate logistic regression analysis for the parameters affecting carotid atherosclerosisUnivariateMultivariateOR (95%CI) P OR (95%CI) p Male sex1.97 (0.71–5.47)0.193.63 (1-13.27)0.051Age ≥ 60 years4.13 (1.57–10.85)0.0046.2 (1.97–19.51)0.002Syntax score > 174.36 (1.73–10.96)0.0024.51 (1.68–12.16)0.003Hosmer-Lemeshow0.4OR Odd`s ratio, CI Confidence interval* Statistically significant results
Discussion
Carotid atherosclerosis was highly prevalent in our cohort of patients with coronary artery disease (CAD), with 71.8% showing carotid atherosclerosis and 5.8% having significant (≥ 50%) common or internal carotid artery stenosis. This high burden of carotid disease underscores the close interplay between coronary and carotid atherosclerosis. Moreover, age ≥ 60 years, male sex, a syntax score > 17, and ≥ 3-vessel disease emerged as important predictors of carotid atherosclerosis, highlighting that patients with more advanced or complex CAD may benefit from targeted carotid evaluation and intensified preventive strategies.
A previous literature review reported a mean prevalence of 9% for carotid artery stenosis > 60% among patients with CAD [16], which is slightly higher than the prevalence observed in our cohort. However, the populations included in that review were heterogeneous and represented different ethnic groups, which may partly account for this difference. In line with our results, the authors reported that older age increases the risk for detecting carotid artery stenosis. In a cohort of Egyptian patients with ischemic vascular events, carotid atherosclerosis, common/internal carotid artery stenosis 20–40% and common/internal carotid artery stenosis ≥ 50% were found in 35.8%, 5.2% and 9.9%, respectively [17]. Among our Egyptian patients with CAD, the prevalence of non-stenotic plaques was higher than Egyptian patients with ischemic vascular events in the aforementioned study, yet the prevalence of common/internal carotid artery stenosis ≥ 50% was slightly lower (5.8% in our cohort versus 9.9%). Two other studies from Egypt found internal carotid artery stenosis ≥ 50% among patients with ischemic vascular events in 3.6% [18] and 2.5% [19] of cases, which is lower than the 5.8% observed in our cohort. It’s worth noting that the former study was conducted in Upper Egypt and involved a different ethnic population compared with the Lower Egypt cohort in our study. Additionally, the latter study defined ≥ 50% stenosis based on a peak systolic velocity of ≥ 125 cm/s, whereas our study utilized more recent ultrasound criteria, published after the earlier study, which defines ≥ 50% stenosis as a peak systolic velocity of ≥ 200 cm/s. This updated criterion likely accounts for the higher prevalence observed in our cohort. A study from Korea showed that the prevalence of carotid plaques, defined as > 1.2 mm focal protrusion in the vascular lumen, was 30.3% among patients, who underwent coronary angiography [20]. In the aforementioned study, only 75.4% of the patients with carotid plaques and 58.3% of those without carotid plaques had CAD with luminal stenosis of > 50%. Although the authors used less sensitive criteria for carotid plaques with carotid plaque thickness > 1.2 mm in comparison to the criteria used in our study (≥ 1.5 mm), our cohort showed markedly higher prevalence of carotid plaques (71.8%). However, 100% of our study population had CAD with luminal stenosis ≥ 70%, which might explain the higher prevalence among our cohort. Moreover, ethnic difference might explain the higher prevalence in our study. Similar to our results, a previous Italian cohort detected carotid plaques (defined as increased intimal medial thickness ≥ 1 mm) in 83%, 87%, 89% and 93% of patients with 1-, 2-, 3-vessel CAD and left main trunk CAD, respectively [21]. A more recent Italian Cohort reported similar findings for carotid plaques (defined as focal thickening > 1.5 mm) among 81% of patients with chest pain undergoing coronary angiography (88% had angiographically proven CAD) [22]. Of note, the authors reported a statistically significant relation between syntax score and carotid plaque size, which is comparable with our results. In concordance with our results, other authors reported a positive correlation between carotid plaque size and the number of diseased coronary vessels [23]. In line with our findings, another study from Malaysia among patients with CAD necessitating elective coronary artery bypass surgery reported carotid plaques (defined as focal thickening ≥ 1.3 mm) in 89/119 (74.8%) patients and carotid stenosis (defined as peak systolic velocity ≥ 125 cm/s) in 10/119 (8.4%) patients [24]. Similar to our results, the authors further noted that older age is more likely associated with carotid plaques. In a Norwegian cohort of asymptomatic population aged 63–65 years, the prevalence of carotid plaques was 87% [25], which is even higher than the prevalence (71.8%) in our CAD patients with a mean (± SD) age of 58 (± 9) years. Ethnic differences between Whites and Egyptians might explain the higher prevalence of carotid plaques among Norwegian. Nevertheless, the authors of the Norwegian cohort reported a lower prevalence of > 50% carotid stenosis of 2.3% (defined as peak systolic velocity of > 125 cm/s) in comparison to the prevalence of 5.8% among our patients (defined as peak systolic velocity of ≥ 200 cm/s), which might be explained by the increased cardiovascular risk among our CAD patients.
Overall, ethnic differences, variations in the definition of carotid plaque (> 1 mm, > 1.2 mm, or ≥ 1.5 mm), differences in ultrasound criteria for grading significant carotid stenosis, and varying risk profiles across studies may collectively explain the discrepant findings.
We found a statistically significant positive correlation between syntax score and plaque score (ρ 0.31, p = 0.002). Moreover, in our study, a syntax score > 17 was found to be a potential predictor of carotid atherosclerosis, with an area under the curve (AUC) of 0.68, reflecting moderate diagnostic performance. Although this predictive ability is modest, it indicates that patients with more complex coronary artery disease are more likely to have concurrent carotid artery involvement. Clinically, this threshold could help identify patients who may benefit from additional vascular assessment, particularly in settings where carotid imaging is not routinely accessible. However, this cut-off should be applied with caution and requires validation in larger, prospective cohorts. Similar to our findings, a systematic review demonstrated a statistically significant positive correlation between carotid intimal medial thickness and syntax score (r = 0.42, p < 0.001) as well as between carotid and coronary stenosis (r = 0.53, p < 0.001) [26]. Another meta-analysis found a positive linear relation between carotid intimal medial thickness and the number of diseased coronary vessels as well as the severity of CAD [27]. In concordance with our study, previous authors reported an association between bilateral rather than unilateral carotid plaques and significant CAD as well as multi-vessel CAD [20].
We found that the presence of ≥ 3-vessel CAD are important predictors of carotid atherosclerosis. Similarly, Tanimoto et al. reported an association between carotid atherosclerosis with age and extent of CAD among Japanese population [28]. Another study from South Korea noted that carotid plaques predicts multi-vessel CAD [20].
Although carotid atherosclerosis is highly prevalent among patients with CAD, atherosclerotic involvement can vary across vascular territories [29]. Routine screening of the carotid arteries may be beneficial for patients who already have CAD. Evidence shows that reducing the carotid intima-media thickness is linked to significantly lower risks of major adverse cardiovascular and major adverse cerebral and coronary events, myocardial infarctions, ischemic strokes and cardiovascular mortality. Conversely, an increase in carotid intima-media thickness is associated with higher risk [30]. Because carotid ultrasound is a simple and widely available tool, targeted follow-up in this high-risk group could help improve risk assessment and guide secondary prevention efforts. However, routine screening for carotid artery disease in people without symptoms is not advised, in line with recommendations from the U.S. Preventive Services Task Force [6]. Therefore, an individualized evaluation is the cornerstone to stratify the cerebro-cardiovascular risk profile and guide patient-tailored management.
The main limitation of the current work is our small sample size (n = 103), which limits the generalizability of our findings. However, we recruited our patients after undergoing coronary angiography and conducted ultrasound examination with the aim of detecting possible plaques or stenosis. Because this study used a cross-sectional design, we cannot determine cause-and-effect relationships, so the findings should be viewed as generating hypotheses rather than definitive conclusions. Therefore, any clinical implications—like identifying patients at increased risk for carotid atherosclerosis and complications such as ischemic stroke—should be interpreted carefully. To confirm these results and help develop effective prevention strategies, larger prospective studies with more detailed data are needed. Additionally, the predictive performance of the syntax score > 17 was only moderate (AUC = 0.68), which may limit its clinical utility. Furthermore, the exclusion of asymptomatic CAD patients or those with less severe disease or even physiologically determined lesion severity significantly limits the applicability of the findings to the broader CAD population. Another limitation of our study is that the carotid ultrasound examinations were performed by a single investigator. Although this reduces interobserver variability, it may introduce potential observer bias, and the absence of interobserver validation may affect the reliability of the measurements.
Conclusions
Ultrasound carotid screening can be considered for patients with CAD, particularly older males with high syntax scores and/or ≥ 3-vessel CAD.