Drug Coverage Policy and Legacy Prescribing: A Cross‐Sectional Analysis in British Columbia
Aydan Con, Ivy Thrasher, Aaron M. Tejani

Abstract
Click any figure to enlarge with its caption.
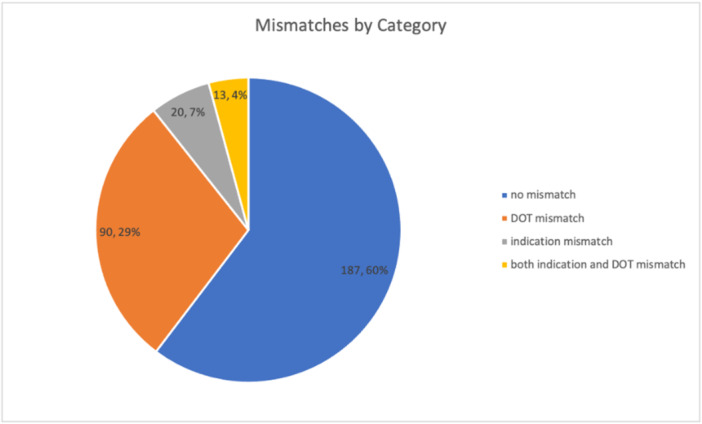 Figure 1
Figure 1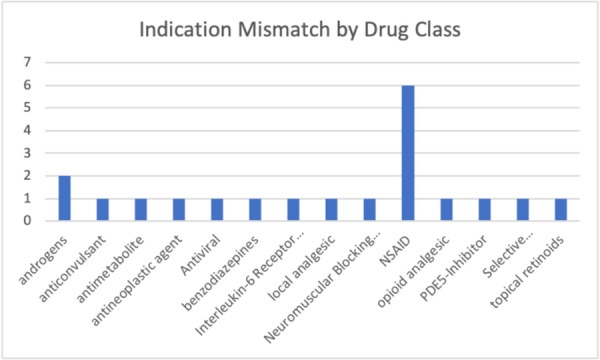 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedication Adherence and Compliance · Pharmaceutical Economics and Policy · Pharmaceutical Practices and Patient Outcomes
Introduction
1
Legacy drug‐prescribing, the practice of continuing fixed‐term drug therapy indefinitely without strong evidence of long‐term therapeutic benefit, is a growing concern in healthcare [1]. Legacy drug prescribing can contribute to polypharmacy, which is associated with adverse health outcomes [2]. Several studies have highlighted significant proportions of elderly patients receiving legacy drug prescriptions for antidepressants, bisphosphonates, and proton‐pump inhibitors (PPIs) [1, 3, 4]. In British Columbia, the provincial government operates the BC Pharmacare Drug Plan, which provides medication funding for individuals [5]. Within this plan, the Limited Coverage program (BCPLC) funds medications only when patients meet specific medical criteria, with coverage typically granted for defined durations [5].
Because such funding rules shape access, drug policy itself can influence prescribing patterns. Irish data show polypharmacy is more common among patients with subsidized coverage than those paying out‐of‐pocket [4]. Medicare Part D similarly increased both essential and low‐value drug use [3], while British Columbia's reference pricing policy shifted patients to lower‐cost equivalents without harm [6]. Together, this evidence suggests that funding arrangements can either reinforce problematic polypharmacy or promote more cost‐effective prescribing. This study aims to assess whether BCPLC funding criteria contribute to legacy drug prescribing specifically and/or problematic polypharmacy.
Methods
2
We analyzed the 2022 BCPLC formulary, comprising 302 medications, focusing on the covered indications and duration of therapy (DOT) for each medication [5]. A multidisciplinary research group consisting of two pharmacist members of the BC Ministry of Health, a pharmacist and two research assistants developed a standardized data collection form. This form extracted the BCPLC covered indications and funding durations, as well as the listed indications and durations found in best‐available evidence, such as systematic reviews, Health Canada drug monographs, Canadian Agency for Drugs and Technologies in Health (now known as Canada's Drug Agency) reimbursement recommendations, and clinical databases like UpToDate and Lexicomp [7]. We compared BCPLC criteria with referenced durations and indications and identified two types of mismatches: duration of therapy mismatch (DOTM) and indication mismatches (IM) [5]. We looked to see if medications with mismatches were listed as potentially inappropriate according to Beer's 2019 criteria [8]. All analyses were descriptive only; no statistical calculations were done. No Research Ethics Board approval was required as this was a quality assurance project.
Results
3
Of 286 medications analyzed, 40% exhibited at least one mismatch (see Figure 1), predominantly DOTMs, largely comprised of NSAIDs, PPIs, and bisphosphonates [5].
The proportion of BCPLC list with no mismatch (n = 187), DOTM (n = 90), IM (n = 20), and both IM and DOTM (n = 13).
We identified four subcategories of DOTMs (see Figure 2, n = 90): (a) medications with indefinite BCPLC coverage that should only be used for finite periods (n = 55), (b) medications that involve a suggested trial period that is shorter than or unlisted by the BCPLC formulary (n = 15), (c) medications with fixed‐period BCPLC coverage that is longer than our reference duration of therapy (n = 8), (d) medications recommended for fixed‐period therapy, with lack of consensus on the best therapeutic duration (n = 13). Additionally, 28 medications considered potentially inappropriate by Beer's 2019 criteria exhibited DOTMs [8].
Indication mismatches by therapeutic class.
Discussion
4
BCPLC coverage criteria revealed inconsistencies that may contribute to inappropriate legacy prescribing and problematic polypharmacy, particularly with NSAIDs, PPIs, and bisphosphonates. Based on our findings, we recommend limiting NSAID coverage to a finite period with re‐evaluation for prolonged use; restricting PPI coverage to 8–12 weeks with renewals as needed; and replacing indefinite bisphosphonate coverage with an initial 5‐year period requiring subsequent renewals. These shorter coverage periods encourage regular reassessment, promoting safe, appropriate, and time‐limited medication use.
Although shorter coverage periods may promote safer, time‐limited prescribing, they also carry risks. In BC's ongoing primary care shortage, more frequent assessments and requests for prescription renewals could increase administrative burden, create access barriers for patients without a regular provider, and delay necessary treatment. A subset of patients might also require longer durations of NSAIDs, PPIs, or bisphosphonates based on clinical need. While these changes may shift workload toward primary care, frequent therapy re‐evaluation is standard‐of‐care, and renewals can be supported by other authorized providers, including community pharmacists or nurse practitioners. To prevent unintended harm, coverage policies that default to shorter intervals could include pharmacist‐initiated renewals under protocol, streamlined electronic reassessments, automated reminders with coverage grace periods, and clear criteria for extended coverage (e.g., PPI for Barrett's Esophagus). These measures could help balance appropriateness with access while minimizing avoidable treatment interruptions. Our findings align with evidence that drug coverage policy shapes prescribing. Subsidized patients often experience more polypharmacy, coverage changes can increase both low‐ and high‐value drug use, and expanded benefits can raise overall medication use [3, 4]. In British Columbia, limited coverage under BC Pharmacare may unintentionally encourage potentially harmful prescribing [6]. Unlike prior studies, we specifically examine policy design as a driver of suboptimal medication use, addressing a gap in understanding the unintended consequences of funding rules.
By systematically evaluating BCPLC criteria, we generated actionable recommendations supported by widely used clinical tools and regulatory guidance [5]. Limitations include the lack of data on actual prescribing patterns or patient outcomes, and a narrower resource pool than may capture all nuances. Future research should examine the impact of coverage policies on prescribing behavior and patient outcomes.
Conclusion
5
Policymakers in BC should reconsider indefinite coverage for medications with potential harm, including NSAIDs, PPIs, and bisphosphonates, to ensure therapy is regularly reassessed and to reduce the risk of problematic polypharmacy.
Author Contributions
Aydan Con: data curation, formal analysis, investigation, methodology, project administration, writing – original draft, writing – review and editing. Ivy Thrasher: data curation, formal analysis, methodology, project administration. Aaron M. Tejani: conceptualization, data curation, formal analysis, methodology, project administration, supervision, validation, writing – original draft, writing – review and editing.
Funding
The authors received no specific funding for this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The corresponding author, Aaron M. Tejani, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. Mangin , J. Lawson , J. Cuppage , et al., “Legacy Drug‐Prescribing Patterns in Primary Care,” Annals of Family Medicine 16, no. 6 (2018): 515–520.30420366 10.1370/afm.2315 PMC 6231929 · doi ↗ · pubmed ↗
- 2F. Pazan and M. Wehling , “Polypharmacy in Older Adults: A Narrative Review of Definitions, Epidemiology and Consequences,” European Geriatric Medicine 12 (2021): 443–452.33694123 10.1007/s 41999-021-00479-3PMC 8149355 · doi ↗ · pubmed ↗
- 3J. M. Polinski , J. M. Donohue , E. Kilabuk , and W. H. Shrank , “Medicare Part D's Effect on the Under‐ and Overuse of Medications: A Systematic Review,” Journal of the American Geriatrics Society 59, no. 10 (2011): 1922–1933.21806563 10.1111/j.1532-5415.2011.03537.x PMC 3400925 · doi ↗ · pubmed ↗
- 4A. Varley and J. Cullinan , “Are Payment Methods for Prescription Drugs Associated With Polypharmacy in Older Adults in Ireland? Evidence From the TILDA Cohort Study,” BMJ Open 10, no. 10 (2020): e 036591.10.1136/bmjopen-2019-036591 PMC 753470133004388 · doi ↗ · pubmed ↗
- 5BC Ministry of Health , “Limited Coverage Drug List [Internet]” BC Pharmacare for Health Professionals, published 2022, https://www 2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/programs/limited-coverage-drug-program.
- 6S. Schneeweiss , A. M. Walker , R. J. Glynn , M. Maclure , C. Dormuth , and S. B. Soumerai , “Outcomes of Reference Pricing for Angiotensin‐Converting‐Enzyme Inhibitors,” New England Journal of Medicine 346, no. 11 (2002): 822–829.11893794 10.1056/NEJ Msa 003087 · doi ↗ · pubmed ↗
- 7Lexicomp , “Various Medications,” in Lexi‐Drugs. Up To Date Inc., accessed September 15, 2022, https://online.lexi.com.
- 8American Geriatrics Society , “2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults,” Journal of the American Geriatrics Society 67 (2019): 674–694, 10.1111/jgs.15767.30693946 · doi ↗ · pubmed ↗