The South Australian 177Lu-DOTATATE peptide receptor radionuclide therapy service: an 11-year review of toxicity, health-related quality of life, and survival
L.M. Altus, J.C. Forster, J. Mercurio, M. Kitchener, N. Corsini, M. Nenke, T. Price, D. Patel, R. Chew, D. Moffat, S. Unger, G. Cehic

TL;DR
This study reviews 11 years of Lu-DOTATATE therapy outcomes, showing improved quality of life and a median survival of nearly 4 years.
Contribution
A comprehensive 11-year audit of Lu-DOTATATE therapy outcomes in a single center, including toxicity, quality of life, and survival data.
Findings
Median overall survival from first Lu-DOTATATE cycle was 48.4 months.
Significant improvements in health-related quality of life were observed after induction therapy.
4.2% of patients developed haematological malignancy following treatment.
Abstract
The aim of this study was to audit clinical and patient-reported outcomes of patients treated with [177Lu]-DOTA-octreotate (177Lu-DOTATATE) at a single Australian centre over an 11-year period. A retrospective analysis of 189 patients with metastatic or locally advanced neuroendocrine neoplasms or tumours (NENs/NETs) or other somatostatin receptor-positive tumour treated with 177Lu-DOTATATE at The Queen Elizabeth Hospital from 2011 to 2022 was carried out. Toxicity, radiological response, health-related quality of life (hr-QoL), and overall survival (OS) were summarised. Gastroenteropancreatic (NET) origin accounted for 75% of cases. The median age of diagnosis was 59 years and median age at first cycle of 177Lu-DOTATATE at The Queen Elizabeth Hospital was 64.7 years (range 16.5-92.6 years). Of the 182 patients who commenced induction peptide receptor radionuclide therapy (iPRRT), 143…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
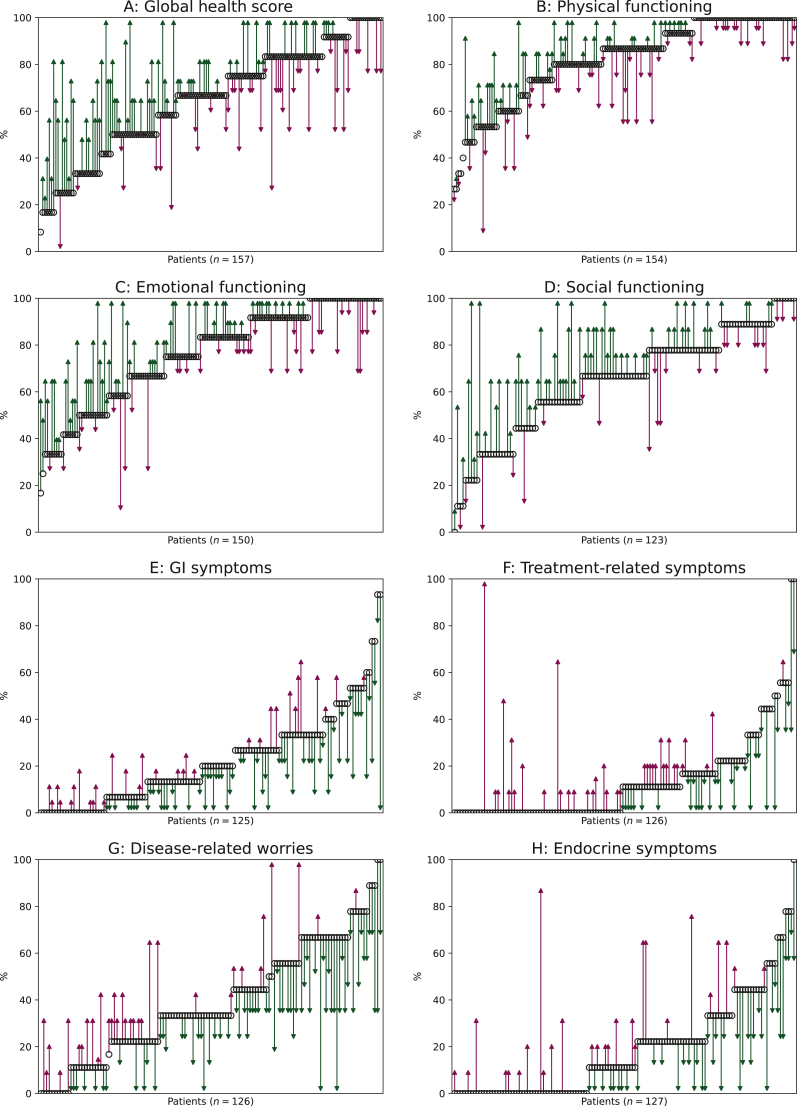 Figure 1
Figure 1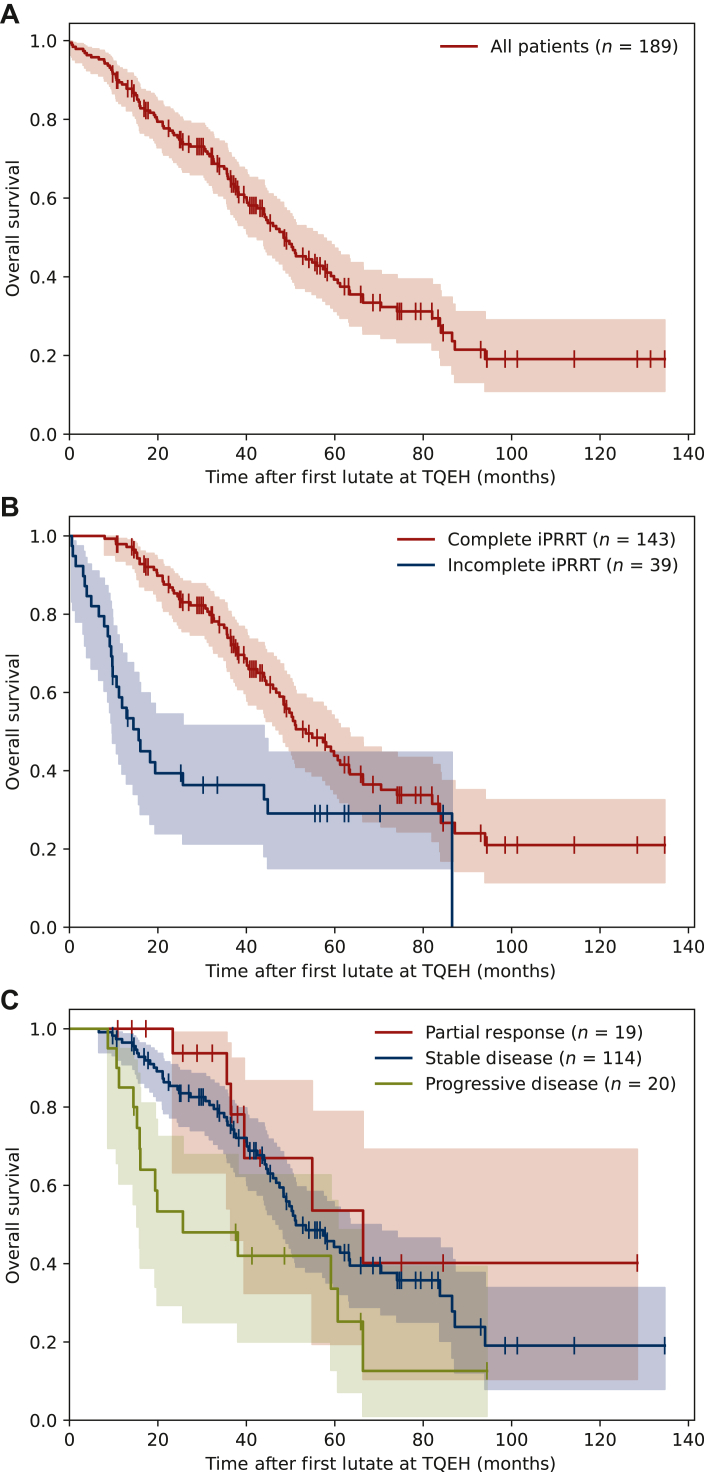 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Lung Cancer Research Studies · Neuroblastoma Research and Treatments
Introduction
Theranostics is an established pillar of cancer care and is increasingly used as a targeted treatment option for selected cancers. For patients with progressive metastatic gastroenteropancreatic (GEP) neuroendocrine neoplasms or tumours (NENs or NETs), peptide receptor radionuclide therapy (PRRT) with [^177^Lu]-DOTA-octreotate (^177^Lu-DOTATATE) has proven safety and efficacy in extending progression-free survival and improving health-related quality of life (hr-QoL).1, 2, 3, 4, 5 The role for PRRT in the treatment of other somatostatin receptor (SSTR)-positive neoplasms, including bronchial carcinoid,6 paraganglioma, and phaeochromocytoma,7 is also increasingly recognised.
The South Australian PRRT service, based at The Queen Elizabeth Hospital (TQEH) in Adelaide was established in 2011 and provides comprehensive care for patients with advanced SSTR-expressing tumours. Before the development of a dedicated radionuclide service, a small number of eligible patients were treated at interstate PRRT centres. The first cycle of ^177^Lu-DOTATATE was administered at TQEH in April 2011. As of 31 December 2024, the service has treated 231 individual patients and administered just over 1000 cycles.
As the sole PRRT centre for the central corridor of Australia, which includes South Australia, Northern Territory, and rural New South Wales, the geographical spread of our patients has created major challenges for equitable access. An area greater than 2 300 000 km^2^ is serviced, equivalent to the combined areas of France, Spain, Sweden, Norway, and Germany. Some patients have travelled over 2500 km for treatment in Adelaide. Approximately 30% of our patients reside in rural and remote locations.8
Demographic, clinical, pathological, and hr-QoL data have been collected as standard of care. We present the first detailed audit of our patient cohort since inception of the service, summarising outcomes including toxicity, hr-QoL, and overall survival (OS). Our intention is to share our centre’s real-world experience and add to the body of literature in clinical theranostics.
Methods
Eligibility and access
Patients eligible for referral for induction PRRT (iPRRT) or retreatment PRRT (rPRRT) were discussed at the statewide NET multidisciplinary tumour board meeting (NET MDT). Following referral, patients underwent consultation with the TQEH PRRT team, consisting of a nuclear medicine physician, physician fellow, and dedicated specialist oncology NET nurse. To confirm eligibility, renal perfusion study and 3-time-point glomerular filtration rate (GFR) using ^99^^m^Tc-diethylenetriaminepentaacetic acid (DTPA), complete blood examination, electrolytes, and renal function [estimated GFR (eGFR)], liver function tests, and disease-specific biomarkers were carried out.
Selection criteria for PRRT:
- •Histologically confirmed NEN/NET or neoplasm with neuroendocrine differentiation
- •Locally advanced/inoperable/metastatic disease
- •Progression on at least first-line therapy (as demonstrated radiologically, biochemically, and/or symptomatically)
- •Adequate SSTR expression on [^68^Ga]-DOTATATE positron emission tomography (PET), specifically a modified Krenning scale ≥2
- •Absence of 2-deoxy-2-[^18^F]fluoro-d-glucose (FDG) PET incongruent disease if carried out
- •GFR >40 ml/min based on DTPA renal perfusion study
- •Sufficient bone marrow reserve
- •Adequate functional status
- •For those referred for retreatment, previous response to iPRRT
Given the palliative nature of this treatment, some exceptions to the selection criteria were permissible by the MDT in accordance with other PRRT guidelines adopting a personalised approach. For example, PRRT was given as first-line salvage therapy when tumour and symptom burden was high, or for other SSTR-expressing tumours where PRRT is less established.
PRRT protocol and procedure
Patients were planned for an initial iPRRT course of four cycles of approximately 7.4 GBq of ^177^Lu-DOTATATE at 8-week intervals. Those undergoing rPRRT were planned for up to four cycles. Those with higher-grade disease, high tumour burden, or at the discretion of the referrer/MDT were considered for concurrent single-agent chemotherapy (intravenous 5-fluorouracil or oral capecitabine) or combination oral capecitabine/temozolomide (CAPTEM), designated as PRCRT.
Long-acting somatostatin analogues (SSAs) were held at least 3 weeks before radionuclide therapy or tailored to symptom burden. Patients classified at increased risk of carcinoid crisis were admitted to hospital for close monitoring up to 48 h before and after treatment, with administration of short-acting octreotide as per our hospital guideline.9
European Organisation for Research and Trials Collaboration (EORTC) quality-of-life questionnaires (QLQ) to assess hr-QoL were completed at multiple time points including the initial consultation, each cycle of ^177^Lu-DOTATATE, and at follow-up consultation at 3 months. From 2011 to 2014, the QLQ Core 30 (QLQ-C30) was used,10^,^11 with the addition of the QLQ–GINET21 companion questionnaire12 from 2015 onwards. Responses were used to evaluate disease-related symptom burden to inform clinical management decisions.
For each cycle, patients received anti-emetics (ondansetron or equivalent, and dexamethasone) and an infusion of amino acids (25 g lysine and 25 g arginine per litre) over 4 h for renal protection, commencing 30 min before the ^177^Lu-DOTATATE injection. ^177^Lu-DOTATATE was sourced from local or international suppliers pending availability. It was only accessible through the Special Access Scheme of the Therapeutic Goods Administration of Australia and remains unfunded in Australia at the time of publication.
Post-therapy whole body planar imaging was carried out at 4 h, with patients returning at 24 h for triple-field single photon emission computed tomography (SPECT/CT) imaging. Dexamethasone was continued for 2 days following therapy, with additional antiemetics prescribed as required. Haematological, renal, and hepatic toxicity were closely monitored. All patients received a personalised schedule detailing the timing of post-therapy medications, SSA injections, blood tests, and appointments.
After completion of iPRRT or rPRRT, patients returned for follow-up review at 3 months. Haematological, renal, and liver function blood tests; biomarkers; hr-QoL scores; and restaging imaging were used to assess treatment response and toxicity. Data were stored in the online Research Electronic Data CApture Platform (REDCap),13^,^14 sponsored by the Central Adelaide Local Health Network (CALHN) research and ethics unit.
Clinical audit
A retrospective clinical audit was conducted of our patients treated with ^177^Lu-DOTATATE between 2011 and 2022. Data were extracted from the REDCap database with approval from the CALHN human research ethics committee.
The audit included all induction and retreatment courses of ^177^Lu-DOTATATE that met the following criteria: all cycles in the course occurred before 31 December 2022; no further cycles were planned for that course; and if there was a restaging scan following the course, it was not after 31 December 2022. All patients who received at least one such course were included in the audit.
Assessment and outcomes in audit
Radiographic response was determined by a radiologist or investigator using Response Evaluation Criteria in Solid Tumours version 1.1 (RECIST 1.1), comparing pretreatment imaging to the restaging scan carried out 2-6 months after the last cycle in a course.
Hr-QoL questionnaire responses were scored according to the EORTC manual into a standardised 0-100 scale. Overall scores were compared from cycle 1 of iPRRT to the posttreatment follow-up review if available, or else to the last completed iPRRT cycle.
Renal function was reviewed at 3 months after iPRRT. The last available renal and haematological results from either before death or within 6 months of 31 December 2022 (the “census date”) were also reviewed for all patients.
Follow-up and OS were calculated from the day of the first cycle of ^177^Lu-DOTATATE at TQEH to the date of death or the census date. For calculations that required a date of diagnosis, if only a year of diagnosis was available, the date of diagnosis was designated 1 January.
Statistical analysis
Kaplan–Meier analyses were applied to evaluate median OS. Cox proportional hazards regression was used to identify markers independently associated with OS. All statistically significant markers in univariate analysis were further incorporated into multivariate analysis. One-tailed paired t-tests were used to compare mean hr-QoL scores before and after iPRRT. A P value of <0.05 was regarded as statistically significant. Statistical analyses were carried out in Python using lifelines (version 0.27.8)15 and SciPy (version 1.11.4).16
Results
Patient and disease characteristics
Between 2011 and 2022, 189 patients met the inclusion criteria for the audit. All patients were Australian residents. Patient and clinical characteristics are summarised in Table 1.Table 1. Baseline characteristics of patients who received ^177^Lu-DOTATATE treatment at TQEH during 2011-2022CharacteristicNumber of patients (% of total cohort)Total number of patients189Gender Male93 (49%) Female96 (51%)Median age at diagnosis59 years (12-84 years)Primary siteGEP-NET141 (75%) Small bowel (NOS)52 Pancreas45 Lower jejunum/ileum26 Colon/rectum9 Ovary4 Renal2 Appendix1 Gastric/stomach1 Duodenum/ampulla/proximal jejunum1Lung12 (6%) Atypical7 Typical3 Unknown2Other13 (7%) Paraganglioma8 Phaeochromocytoma2 Neuroblastoma1 Neuroendocrine carcinoma of the breast1 Myoepithelial carcinoma1Unknown23 (12%)GEP-NET grade (WHO 2017 criteria) (n = 141)aGrade 141 (29%)Grade 259 (42%)Grade 3—well differentiated4 (3%)Unknown/unable to determined37 (26%)Sites of metastasisLung18 (10%)Liver160 (85%)Bone78 (41%)Nodal97 (51%)Soft tissue39 (21%)Other site25 (13%)Disease-specific treatmentsb before first ^177^Lu-DOTATATE at TQEHSomatostatin analogue181 (96%)Surgery95 (50%)Chemotherapy47 (25%)Radiotherapy—EBRT or SBRT23 (12%)Targeted therapy (everolimus/sirolimus)8 (4%)Liver directed9 (5%)Prior PRRT (^90^Y, ^111^In, or ^177^Lu elsewhere)7 (4%)Other3 (2%)Cumulative disease specific treatments before ^177^Lu-DOTATATE at TQEH159 (31%)271 (38%)328 (15%)421 (11%)≥510 (5%)Other clinical characteristicsHormone symptoms present (clinically assessed) (n = 176)96 (55%)Raised baseline chromogranin A level (n = 183)152 (83%)Median baseline GFR (n = 183)86.6 ml/min/1.73 m^2^ (40.9-154.4 ml/min/1.73 m^2^)Median time from diagnosis to first PRRT at any centre3.1 years (0.2-42.6 years)Median age at first cycle of ^177^Lu-DOTATATE at TQEH64.7 years (16.5-92.6 years)EBRT, external beam radiation therapy; GEP, gastroenteropancreatic; GFR, glomerular filtration rate; NET, neuroendocrine tumour; NOS, not otherwise specified; PRRT, peptide receptor radionuclide therapy; SBRT, stereotactic body radiation therapy; TQEH, The Queen Elizabeth Hospital.aIf more than one pathology sample was available before cycle 1, the more recent grade was used.bSome patients received multiple of the same line of treatment.
GEP-NET origin accounted for 75% of cases. Small bowel [including not otherwise specified (NOS), jejunum, ileum, duodenum, ampulla] was the most common primary site (41%) followed by pancreas (24%). Grading was available for 104/141 GEP-NET cases, with 96% of these grades 1 and 2. Overall, 16% of grading came directly from review of histology during the MDT meeting.
The most common prior therapy was SSA (96%) followed by surgery (50%). For the eight patients not documented to have received prior SSA therapy, one had NET of unknown primary, one had atypical lung NET, and six had paraganglioma/phaeochromocytoma or neuroblastoma, for which SSA therapy was not approved. A total of seven patients had received prior PRRT; four had received ^177^Lu-DOTATATE at interstate centres and five had received PRRT with other radiopharmaceuticals: three in South Australia, one interstate, and one in the UK. Overall, 31% of patients had received three or more disease-specific treatments before their first cycle of PRRT at TQEH.
Baseline GFR DTPA scan results were available for 183/189 (97%) patients with a median value of 86.6 ml/min (range 40.9-154.4 ml/min). Baseline eGFR results were available for 179 patients who underwent iPRRT, with 24/179 (13%) <60 ml/min/1.73 m^2^ (range 32.0 to >90 ml/min/1.73 m^2^).
Treatments
The most common reasons for referral for ^177^Lu-DOTATATE were radiological disease progression (92%), biochemical progression (57%), and worsening symptoms (48%). Only 21% of patients were referred for progression on imaging alone, while most had a combination of clinical/biochemical and radiological progression. There were six patients referred for other reasons including consolidation following chemotherapy, high tumour burden, and the presence of severe tricuspid regurgitation from carcinoid heart disease at the time of diagnosis.
Of the 251 courses of radionuclide therapy, 182 were iPRRT, with the remainder rPRRT. Treatment details are summarised in Table 2. In total, 822 cycles of ^177^Lu-DOTATATE were administered during the audit period. The median number of cycles (including both iPRRT and rPRRT courses) administered to a patient at TQEH was 4 (range 1-12).Table 2. Summary of induction and retreatment radionuclide therapyTotal number of cycles given at TQEH822Median cumulative administered activity (GBq)31.0 (4.9-88.7)Number of iPRRT cycles completed per patient (182 patients)17 (4%)214 (8%)318 (10%)4141 (77%)52 (1%)Total number of iPRRT cycles663Reasons from withdrawing from iPRRT (completing one to three cycles) (39 patients)Haematological13Medically unfit9Patient deceased since last cycle6Disease progression4Contraindicated (renal)2Good response to earlier cycles and decision made to withdraw2Contraindicated (liver)1Patient refused1Bowel obstruction1rPRRT (52 patients)Number of rPRRT courses69Number of patients who had multiple courses of rPRRT13Total number of rPRRT cycles159Median time (months) between completing iPRRT and returning for rPRRT24.7 (9.7-85.8)iPRRT, induction peptide receptor radionuclide therapy; rPRRT, retreatment peptide receptor radionuclide therapy; TQEH, The Queen Elizabeth Hospital.
Of the 182 patients who commenced iPRRT at TQEH, 143 (79%) completed four or five cycles, 18 (10%) completed three cycles, 14 (8%) completed two cycles, and seven (4%) completed only one cycle. For the 39 patients who were unable to complete a full iPRRT course, the leading causes for withdrawal were haematological reasons (13 patients) and being medically unfit to proceed (8 patients).
A total of 52 patients underwent retreatment (rPRRT), including 13 patients who had had multiple rPRRT courses. A total of 159 retreatment cycles were administered with a median of 2 cycles (range 1-8 cycles). The median interval between the last iPRRT cycle and first rPRRT cycle was 24.7 months (range 9.7-85.8 months).
Concurrent chemotherapy was administered with at least 1 cycle of PRRT for 76 patients (40%) and 273/822 cycles (33%). For the GEP-NET patients with a known histological grade, 100% of grade 3, 41% of grade 2, and 32% of grade 1 received at least one cycle of concurrent chemotherapy.
The median administered activity of ^177^Lu-DOTATATE per cycle was 7.7 GBq (range 4.0-9.0 GBq). Some 18% of patients had at least one cycle with intentionally reduced administered activity <7.0 GBq. The median total activity administered to patients was 31.0 GBq (range 4.9-88.7 GBq).
Response to treatment
Radiological response
CT was the imaging modality used for 82% of restaging scans. The median timing of restaging imaging was 3.0 months (range 0.7-9.6 months).
Radiological response to iPRRT was available for 153/182 patients (84%). Of these, 131 patients had received a full iPRRT course (four or more cycles) and 22 patients received a partial iPRRT course. For the patients who received a full iPRRT course, 99 patients (76%) had stable disease (SD), 19 (15%) had partial response (PR), and 13 (10%) progressive disease (PD) (Table 3). For the 22 patients who partially completed induction courses, 68% had SD and the remainder had PD.
Radiological response was available for 47/69 rPRRT courses; 33 courses (70%) had SD, 3 (6%) had PR, and 11 (23%) had PD.
During the audit period, no patients achieved a complete response following either iPRRT or rPRRT.
Quality of life
Of the 822 ^177^Lu-DOTATATE cycles administered at TQEH, 760 (92%) had a corresponding hr-QoL questionnaire completed. The first 40 patients completed the QLQ-C30 only, until the companion questionnaire was added in 2015. We compared available hr-QOL scores for patients undergoing iPRRT. Figure 1 shows the change in individual patient hr-QoL scores over iPRRT, highlighting at first the heterogeneity of baseline scores across the cohort before commencing ^177^Lu-DOTATATE.Figure 1Change in hr-QoL scores over inductionPRRT. For each patient, the black circle represents the initial score, and the arrow shows the direction and magnitude of change (green indicates improvement, purple indicates deterioration). GI, gastrointestinal; hr-QoL, health-related quality of life.
There were significant improvements in global health score, emotional functioning, gastrointestinal symptoms, disease-related worries and social functioning from before to after iPRRT. No significant association was found between change in global health score and radiological response rate or OS.
Overall survival
The median duration of follow-up was 37.6 months (0.0-134.6 months). At the census date, 110 patients had died (58%). Cause of death was NET-related in 81 patients (74%). Other causes of death were unknown (15%), unrelated (7%), and complication of treatment (5%).
The estimated median OS was 48.4 months [95% confidence interval (CI) 42.5-57.3 months] for all patients (Figure 2A). Patients who had a complete iPRRT course of at least four cycles had a significantly greater OS than patients who had an incomplete course of less than four cycles (Figure 2B).Figure 2Overall survival from the first cycle of^177^Lu-DOTATATE at TQEH. (A) OS including all patients. The median OS was 48.4 months (95% CI 42.5-57.3 months). (B) OS for complete versus incomplete iPRRT. Complete iPRRT had median 53.5 months (95% CI 47.5-63.2 months) and incomplete iPRRT had median 15.6 months (95% CI 9.7-44.0 months). (C) OS by radiological response following iPRRT. Partial response had median 66.4 months (95% CI 36.5 months to NA), stable disease had median 51.2 months (95% CI 47.5-63.4 months), and progressive disease had median 25.7 months (95% CI 15.3-60.7 months). CI, confidence interval; OS, overall survival; iPRRT, induction peptide receptor radionuclide therapy; TQEH, The Queen Elizabeth Hospital.
Patients with PD during treatment had significantly worse survival than patients with PR in univariate analysis (Figure 2C). However, this association was not significant when adjusted for iPRRT completion. OS was not significantly associated with tumour primary site or GEP-NET grade.
Safety and tolerability
^177^Lu-DOTATATE was well tolerated, with 438/822 (53%) cycles completed without any symptoms occurring on the day of therapy. The most common side-effects were minor flushing (25%) and nausea (20%), with other symptoms of dizziness, vomiting, pain, or palpitations each occurring in <2% of cycles. Only one patient required an unplanned admission for carcinoid crisis after PRRT, which was managed with octreotide infusion and the patient was discharged after 24 h.
Haematological results were available for 92% of patients from within the last 6 months of death or the census date. Over the 11-year audit period, 8/189 patients (4.2%) developed a haematological malignancy, with 7 of the patients having exposure to chemotherapy and/or external beam radiotherapy and receiving between four and seven cycles of PRRT total (Table 4). The mean latency from first PRRT to diagnostic bone marrow sampling was 54 months (range 8-132 months).Table 3. Response to treatment—imaging and hr-QoLRadiological response ratesRECIST 1.1 categoryNumber of patientsComplete iPRRT course (results available for 131/143 patients)Partial response19 (15%)Stable disease99 (76%)Progressive disease13 (10%)Partial iPRRT course (results available for 22/39 patients)Stable disease15 (68%)Progressive disease7 (32%)Retreatments (results available for 47/69 cumulative rPRRT courses)Partial response3 (6%)Stable disease33 (70%)Progressive disease11 (23%)Change in hr-QoL scores over iPRRTComposite domain (questions included)Mean score (%)P value when significantly differentPREPOSTA: Global health score (Q29/30)65700.001B: Physical functioning (Q1-5)8282n.sC: Emotional functioning (Q21-24)7679<0.01D: Social functioning (Q42, 44, 49)6572<0.001E: GI symptoms (Q34-38)2217<0.001F: Treatment -related symptoms (Q39, 40, 46)1313n.s.G: Disease-related worries (Q41, 43, 47)3932<0.001H: Endocrine symptoms (Q31-33)1917n.s.hr-QoL, health-related quality of life; iPRRT, induction peptide receptor radionuclide therapy; n.s., not significant; rPRRT, retreatment peptide receptor radionuclide therapy.Table 4. Characteristics of the eight patients diagnosed with haematological malignancies between 2011 and 2022Year of haematological diagnosisAge (years) at haematological diagnosisGenderHaematological diagnosisLatency period (months)aTotal PRRT cyclesOther bone marrow-toxic treatments received before the diagnosis of the haematological malignancy201358Femalet-MDS841 Cycle PRCRT with 5FU associated with coronary spasm201565Femalet-MDS345Prior chemoradiotherapy for breast cancer. ERBT (20 Gy) for NET. 4 Cycles PRCRT with 5FU201551Femalet-AML1327Prior EBRT (7 different courses, total Gy unknown) and chemotherapy (streptozotocin/5FU) for NET. 5 Doses of In-111 octreotide201680Malet-MDS to AML3844 Cycles PRCRT with 5FU201768Femalet-MDS344None201980Malet-MDS444Multiple courses of prior EBRT (120 Gy) for NET202170Femalet-MDS495Prior chemotherapy (carboplatin, etoposide) for NET202278Malet-AML917Prior chemotherapy (5FU, dacarbazine, CAPTEM) for NET. 5 Cycles of PRCRT with 5FU5FU, 5 fluorouracil; AML, acute myeloid leukaemia; CAPTEM, capecitabine/temozolomide; EBRT, external beam radiotherapy; Gy, Gray; NET, neuroendocrine tumour; PRCRT, peptide receptor chemoradionuclide therapy; PRRT, peptide receptor radionuclide therapy; t-MDS, treatment related myelodysplasia.aLatency period is defined as the time from first cycle of PRRT to the bone marrow sample/diagnosis date.
Impaired renal function during therapy resulted in two patients being unable to complete a full induction course. One patient demonstrated improvement in renal function and subsequently received two cycles of rPRRT. The other progressed to end-stage renal failure due to chronic hypertension.
At the 3-month follow-up after iPRRT, eGFR results were available for 130/182 patients. The eGFR was <60 ml/min/1.73 m^2^ in 21/130 (16%).
Longer term follow-up eGFR results from within 6 months of death or census date were available for 175/189 (93%) patients. The eGFR was <60 ml/min/1.73 m^2^ in 61 (35%) patients, of whom 15 (9%) had an eGFR <30 ml/min/1.73 m^2^. Upon review of the 15 patients whose eGFR fell to <30 ml/min/1.73 m^2^, PRRT was identified as a contributor in only 1 patient. The causes of renal failure in the remaining 14 patients were sepsis (5), other acute medical illness (4), cardio- or hepatorenal syndrome (2), chronic hypertension requiring dialysis (1), obstructive uropathy due to intra-abdominal NET (1), and unknown (1).
Discussion
This paper reports on our centre’s experience delivering a PRRT service using a clinical audit method to summarise patient characteristics, treatment, and outcomes. PRRT with ^177^Lu-DOTATATE is incorporated into multiple national17 and international18, 19, 20 NEN/NET treatment guidelines. It is currently recommended after progression on SSA therapy, however the recently published NETTER-2 trial may see PRRT increasingly used as first line in those with WHO grade 2/3 GEP-NETs.21 During the audit period, our model of care for both treatment and restaging followed the available guidelines at the time. The ongoing challenges in this area are well described.22
Concurrent chemotherapy was predominantly recommended for our patients with poor prognostic features such as high-grade disease and high tumour burden. There are increasing data on the safety and efficacy of concurrent chemotherapy.23^,^24 Larger phase III trials are underway to further define the optimal patient cohort of combination treatment due to the potential for greater haematological toxicity.
It is increasingly recognised that dual tracer imaging with FDG PET in addition to [^68^Ga] DOTATATE PET may identify patients with higher grade or heterogenous disease who would benefit from the addition of concurrent chemotherapy. FDG avidity is usually a poor prognostic indicator in a subset of patients,25^,^26 and functional scoring comparing SSTR with FDG imaging (NETPET score) can aid decision-making.27 Whilst not yet routinely included in PET reports, the NETPET score is manually assigned at our NET MDT.
We measured a median OS of 48.4 months (95% CI 42.5-57.3 months), which is comparable to the 48.0 months (95% CI 37.4-55.2 months) reported by NETTER-13 and other single-centre publications.28^,^29 Unsurprisingly, patients who completed an induction course of at least four cycles had a higher OS compared with patients who were unable to complete a full course.
NETTER-1 excluded patients with GFR <50 ml/min, however, more recent guidelines and publications accept <40 ml/min as the cut-off for exclusion.21^,^28^,^30^,^31 All our patients met eligibility based on GFR >40 ml/min derived from DTPA nuclear medicine renal perfusion study, rather than the calculated eGFR. The latter was used for follow-up and assessment of renal toxicity. As we did not routinely repeat the DTPA study after completion of PRRT, a more detailed statistical analysis of renal toxicity was not possible. Additionally, many laboratories historically reported eGFR values as ‘>60 ml/min/1.73 m^2^’ instead of providing an absolute value. The proportion of patients with eGFR <60 ml/min/1.73 m^2^ at 3 months was similar to baseline (13% versus 16%), however, this proportion increased to 35% at longer follow-up or death. PRRT was not considered the leading cause of declining renal function in patients with eGFR <30 ml/min/1.73 m^2^ at death or census date. With an increasing number of long-term cancer survivors, we acknowledge this cohort of patients are at risk of multifactorial renal decline due to increasing age, comorbidities, and cumulative toxicities from a range of cancer therapies including PRRT. DTPA renal perfusion studies could be incorporated into future studies evaluating delayed onset renal toxicity.
Our rate of severe grade 3/4 haematological toxicity (4.2%) is comparable to other centres and publications, which range from 2.2% to 7.0%.28, 29, 30, 31 Most of these patients had also received chemotherapy and/or radiotherapy. Since the introduction of the REDCap™ database in late 2021, we have routinely recorded all haematological and biochemical results to allow future analyses of all toxicities as per Common Terminology Criteria for Adverse Events (CTCAE) v5.0 grading. We will be able to report on all CTCAE grades in future studies. Additionally, we now routinely record the results of echocardiogram and/or N-terminal pro-brain natriuretic peptide before PRRT to assess the prevalence of carcinoid heart disease. In combination with clinical symptoms and biomarkers, this cardiac specific information is used to risk stratify patients at increased risk of PRRT-induced carcinoid crisis.
We have demonstrated that treatment with PRRT resulted in statistically significant improvements in hr-QoL across multiple domains. It is well known that navigating a complex health system with an uncommon cancer causes anxiety, time, and financial toxicity. When combined with a high symptom burden due to hormone excess, hr-QoL is often significantly impacted for patients with metastatic SSTR-expressing malignancies. The early adoption and integration of hr-QoL surveys as part of our routine care pathway has translated to a greater understanding of patient well-being, perceptions towards health, and challenges for rural and remote patients.
Limitations
There are several limitations to our data including their retrospective nature and personalisation of treatment regimens within the available protocols that need to be taken into account when comparing our findings with other services.
We did not evaluate the time from MDT recommendation to commencing PRRT. This was contingent on many factors including clinical need, stabilisation of other comorbidities and acute medical episodes, organising logistics for rural and remote patients, radiopharmaceutical supply chain, and service availability.
We relied on predominantly structural imaging when gathering treatment response data. RECIST criteria were not routinely reported, and this was retrospectively evaluated. Choice of follow-up imaging was at the discretion of the primary treating clinician, thus some patients underwent structural imaging alone (contrast enhanced CT), whereas others underwent functional imaging ([^68^Ga] DOTATATE PET ± FDG PET). Although the additive role of functional imaging is well established, there was limited availability for our cohort. The use of CT to restage aligns with the latest Australian17 and European guidelines.17^,^18
After the 3-month post-treatment review, ongoing care was provided by the primary treating clinician, and follow-up data were not always available.
Conclusions
We have presented our single-centre experience over an 11-year period from a complex and heterogenous patient cohort. Our findings are consistent with other published data demonstrating safety and efficacy of ^177^Lu-DOTATATE for metastatic or locally advanced SSTR-expressing malignancies. We have demonstrated that treatment with PRRT resulted in statistically significant improvements in hr-QoL across multiple domains. We advocate for routinely evaluating hr-QoL indices to guide clinical care and ultimately improve patient’s outcomes and quality of life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Strosberg J.El-Haddad G.Wolin E.Phase 3 trial of 177Lu-Dotatate for midgut neuroendocrine tumors N Engl J Med 376220171251352807670910.1056/NEJ Moa 1607427 PMC 5895095 · doi ↗ · pubmed ↗
- 2Strosberg J.Wolin E.Chasen B.Health-related quality of life in patients with progressive midgut neuroendocrine tumors treated with 177Lu-Dotatate in the phase III NETTER-1 trial J Clin Oncol 36252018257825842987886610.1200/JCO.2018.78.5865 PMC 6366953 · doi ↗ · pubmed ↗
- 3Strosberg J.R.Caplin M.E.Kunz P.L.177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial Lancet Oncol 22122021175217633479371810.1016/S 1470-2045(21)00572-6 · doi ↗ · pubmed ↗
- 4Starr J.S.Sonbol M.B.Hobday T.J.Sharma A.Kendi A.T.Halfdanarson T.R.Peptide receptor radionuclide therapy for the treatment of pancreatic neuroendocrine tumors: recent insights Onco Targets Ther 132020354535553243150910.2147/OTT.S 202867 PMC 7205451 · doi ↗ · pubmed ↗
- 5Ricci C.Lamberti G.Ingaldi C.Treatment of advanced gastro-entero-pancreatic neuro-endocrine tumors: a systematic review and network meta-analysis of phase III randomized controlled trials Cancers (Basel)13220213583356108710.3390/cancers 13020358 PMC 7835931 · doi ↗ · pubmed ↗
- 6Lim L.E.Chan D.L.Thomas D.Australian experience of peptide receptor radionuclide therapy in lung neuroendocrine tumours Oncotarget 11272020263626463267616510.18632/oncotarget.27659 PMC 7343632 · doi ↗ · pubmed ↗
- 7Jha A.Taieb D.Carrasquillo J.A.High-specific-activity-131I-MIBG versus 177Lu-DOTATATE targeted radionuclide therapy for metastatic pheochromocytoma and paraganglioma Clin Cancer Res 27112021298929953368586710.1158/1078-0432.CCR-20-3703 PMC 8172462 · doi ↗ · pubmed ↗
- 8Australian Government | Department of Health and Aged Care. Health Workforce Locator - rural, remote and metropolitan areas classification 1991 Available athttps://www.health.gov.au/resources/apps-and-tools/health-workforce-locator/app?language=en