Dietary and lifestyle inflammation scores in relation to colon cancer recurrence in subgroups of patients based on common molecular tumour characteristics
E. Wesselink, D.E. Kok, K.C. Smit, A.-S. van Lanen, J.W.G. Derksen, M. Koopman, M. Ligtenberg, I.D. Nagtegaal, P.D.M. Rombout, J.H.W. de Wilt, E. Kampman, A.M. May, F.J.B. van Duijnhoven

TL;DR
This study found that a pro-inflammatory lifestyle, not diet, may increase colon cancer recurrence risk, especially in certain tumor types.
Contribution
The study identifies how lifestyle inflammation affects recurrence risk in colon cancer subgroups based on tumor molecular features.
Findings
A pro-inflammatory lifestyle was linked to higher recurrence risk in some tumor subgroups.
The association was strongest in microsatellite stable and KRAS or PIK3CA wildtype tumors.
Dietary inflammation was not significantly associated with recurrence.
Abstract
The aim of this study was to investigate associations between the inflammatory potential of diet and lifestyle in relation to colon cancer recurrence in subgroups of patients based on molecular tumour characteristics that also influence the inflammatory tumour microenvironment. A nested case-control study was implemented in two prospective cohort studies of colon cancer patients. Participants who developed a recurrence were included as cases (n = 167). Matched controls (n = 668) were selected based on incidence density sampling. Lifestyle factors were assessed at diagnosis using self-administered questionnaires and dietary intake was assessed using a food frequency questionnaire. The dietary inflammation score (DIS) and the lifestyle inflammation score (LIS) were constructed. High-throughput next-generation sequencing of tumour tissue was used for mutation and microsatellite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
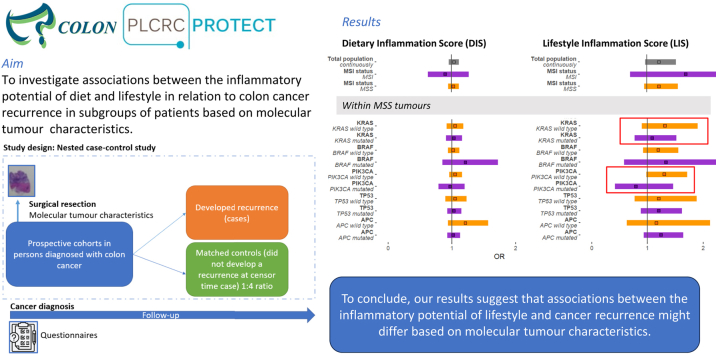 Figure 1
Figure 1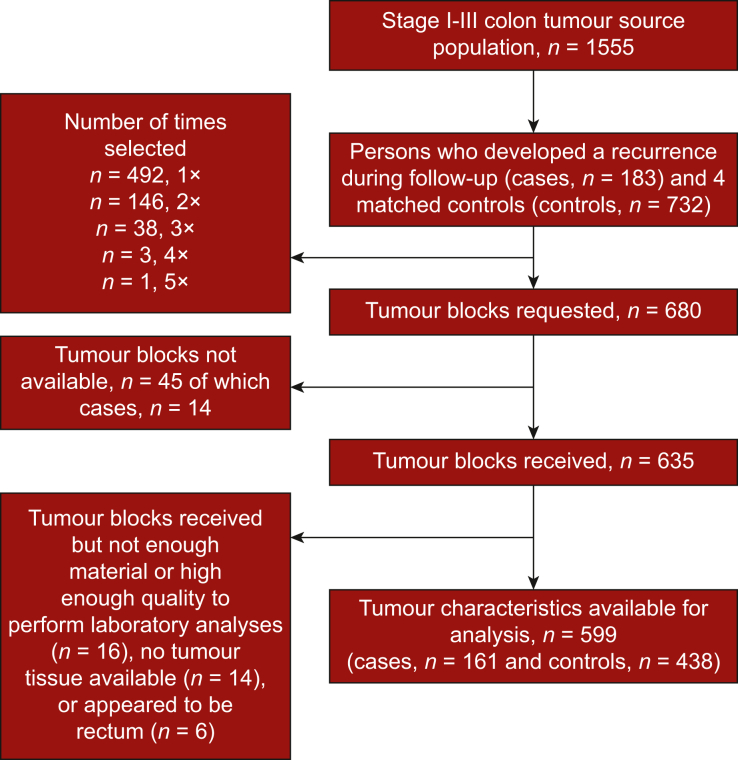 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Genetic factors in colorectal cancer · Cancer, Lipids, and Metabolism
Introduction
Inflammation is involved in every part of the cancer continuum, from development of the primary tumour to progression and recurrence.1^,^2 Inflammation plays a key role in the hallmarks and enabling characteristics of cancer, directly fostering tumour growth, inducing genome instability and mutations, and impairing the antitumour immune response.2, 3, 4, 5 Given the role of inflammation in tumour growth and development of metastasis, inhibiting inflammation could be a potential target to delay tumour recurrence.
Lifestyle factors, including diet and physical activity, could influence chronic inflammation.6^,^7 In several studies among colorectal cancer (CRC) survivors, a more pro-inflammatory diet, linked to higher levels of circulating inflammation markers, has been associated with an increased risk of CRC-specific mortality.8, 9, 10 In our previous research in the COLON study, we observed that a more pro-inflammatory diet, by means of a higher Empirical Dietary Inflammatory Pattern (EDIP) score, was associated with a higher risk of CRC recurrence.11
While chronic inflammation can induce mutations, several molecular tumour characteristics, including microsatellite instability (MSI) and driving mutations commonly observed in colon tumours, such as KRAS (30%-40%), BRAF (10%-20%), PIK3CA (20%-25%), TP53 (40%-50%) and APC (>80%),2^,^5^,^12^,^13 can also influence the inflammatory tumour environment and, subsequently, antitumour immune responses.14, 15, 16, 17 KRAS mutations, but also TP53 mutations, are hypothesized to drive a pro-inflammatory tumour environment by activation of several inflammatory pathways, including the NF-kB, NLRP3 and STAT3 pathways, leading to immune evasion and treatment resistance.12^,^14^,^16^,^18^,^19 PIK3CA- and BRAF-mutated tumours generally have a pro-inflammatory and immune-suppressive profile, mainly through interactions with the COX-2 pathway and up-regulation of PEG2, leading to diminished immune response against the tumour.20, 21, 22 Patients with tumours that are less pro-inflammatory and more responsive to immune activation may respond differently to lifestyle-induced inflammation compared with tumours with a pro-inflammatory and immune-suppressive profile. Hence, a more anti-inflammatory lifestyle might be more beneficial for a subgroup of patients with a less inflammatory and immune-sensitive tumour.
The overall aim of this study was to evaluate the association between the inflammatory potential of the diet and other lifestyle factors and colon cancer recurrence in a subgroup of patients based on MSI and mutation status of KRAS, BRAF, PIK3CA, TP53 and APC. Ultimately, insight into these associations in the presence or absence of specific molecular tumour characteristics could contribute to the development of personalized lifestyle guidelines for individuals diagnosed with colon cancer.
Methods
Study population
Both the COLON study (ClinicalTrials.gov Identifier NCT3191110) and the Prospective Dutch Colorectal Cancer (PLCRC)-PROTECT study (ClinicalTrials.gov Identifier NCT-02070146) have been described in detail previously.23, 24, 25 Briefly, in the COLON study, newly diagnosed CRC patients were recruited from 11 Dutch hospitals, from August 2010 until February 2020. Men and women >18 years with all stages of disease were eligible. Participants were not invited when unable to speak Dutch; or with a history of CRC, (partial) bowel resection or inflammatory bowel disease, inherited CRC syndrome (Lynch syndrome, familial adenomatous polyposis and Peutz–Jeghers syndrome); or with mental conditions such as dementia that make it difficult to fill out surveys. For the PLCRC-PROTECT study, newly diagnosed CRC patients were recruited from 21 Dutch hospitals starting from February 2016. Both studies were approved by a medical ethics committee (COLON: CMO region Arnhem-Nijmegen, 2009-349; PLCRC-PROTECT: University Medical Center Utrecht, 15-770). All study participants provided written informed consent.
Nested case-control design
For the current analyses with colon cancer recurrence as the outcome, a nested case-control study was implemented in the COLON and PLCRC-PROTECT studies. Patients who received neoadjuvant treatment were not eligible for the nested case-control study, since tumour characteristics assessed in the surgical specimens may have been affected by this treatment. Because ∼70% of all rectal cancer patients received neoadjuvant treatment within the COLON and PLCRC-PROTECT studies, we specifically focussed on patients with stage I-III colon cancer26 who did not receive neoadjuvant treatment. In addition, patients with missing dietary data were excluded from this study. In total, 1555 participants were eligible for the nested case-control study (n = 1176 from the COLON study and n = 379 from the PLCRC-PROTECT study).
During the follow-up of the COLON and PLCRC-PROTECT studies, 183 participants (n = 140 COLON; n = 43 PLCRC-PROTECT) diagnosed with stage I-III colon cancer developed a recurrence and were included as cases. The median follow-up time until the occurrence of an event (recurrence) was 1.7 years [inter quartile range (IQR) 1.2-3.3 years] in the cases. Recurrence was defined as a locoregional recurrence and/or distant metastasis. Information on colon cancer recurrence was collected through the medical records by the Netherlands Cancer Registry. Controls were selected based on incidence density sampling from all eligible participants alive and free of a colon cancer recurrence at the time of the recurrence of the matching case with a 4 : 1 control to case ratio. Cases and controls were matched on age (±10 years), sex (men, women), stage of disease (I, II, III) and hospital in which they were treated. Selection and matching were done for each cohort separately. When it was not possible to match four controls based on all these matching criteria, the hospital criterion was omitted, and remaining controls were selected based on age, sex and stage of disease. Since it was possible to be selected more than once as a control (Figure 1), 167 cases and 668 controls were selected in the nested case-control study, which corresponds to 680 tumour tissue blocks.Figure 1. Flowchart of selection of tissue blocks.
Tumour tissue and laboratory analyses
Tissue blocks were obtained from the pathology archives to assess the molecular tumour characteristics. In The Netherlands, tissue specimens for all patients who received surgical resections are stored and registered in the Dutch nationwide pathology databank (PALGA).27 Of the 680 formalin-fixed and paraffin-embedded (FFPE) tissue blocks requested from 25 labs, 635 were sent to Radboudumc, Nijmegen, The Netherlands, for analyses. Of these FFPE tissue blocks, 621 could be used for analyses, and 14 could not be used because they did not have any available tumour tissue or contained noncolon tumour tissue. In the case of multiple tumour blocks per participant, tumour sections with the highest tumour percentage were selected for further analyses.
FFPE tissue sections were used to determine molecular tumour characteristics. Haematoxylin–eosin (H&E)-stained sections were used to semiquantify tumour percentage within the tissue and tumour tissue was isolated from surrounding healthy tissue by means of macrodissection. DNA of the tumour was isolated using a method based on Chelex, followed by ethanol precipitation. A comprehensive panel, the PATH gene panel (PATHv3D), established at the laboratory of pathology of the Radboudumc and encompassing regions in 47 relevant CRC-associated genes, including the oncogenes KRAS, BRAF and PIK3CA, and tumour suppressor gene TP53, was analysed.28 Additionally, the APC gene was sequenced at Radboudumc. The mutation status of these genes (PATH gene panel, as well as APC) was determined using high-throughput next-generation sequencing (NGS) on the Novaseq 6000 (NovaSeq 5000/6000 S1 Rgt Kit; Illumina, San Diego, CA). Demultiplexed FASTQ files were uploaded and analysed in Sequence Pilot version 5.2.0 (JSI Medical Systems, Ettenheim, Germany),29 which included removal of PIK3CA and PTEN pseudogene reads from the alignment and subsequent analysis.28 After variant calling, all variants with a variant allele frequency >3% were visually inspected in Sequence Pilot software, and curated and classified as benign, likely benign, variant of unknown significance, likely pathogenic, or pathogenic. Pathogenic and likely pathogenic variants were considered ‘mutated’. Additionally, 57 markers that were also sequenced using the PATHv3D panel were used to define MSI28^,^30 with mSINGS,31 in which ≥30% unstable loci is considered as MSI, ≤15% as microsatellite stable (MSS) and 15%-30% as uncertain. The PATH panel analyses were carried out in duplicate, the APC analyses in singleplex. The mutation status of included genes was evaluated by two assessors; in case of discrepancy consensus was reached by consulting a third independent assessor. Of the 621 analysed samples, 16 samples could not be used because the material was of insufficient quality to determine mutation status and MSI and 6 samples appeared to originate from rectal tissue instead of colon tissue, resulting in 599 valid samples for further data analyses (Figure 1).
Data collection
In the COLON and PLCRC-PROTECT studies, information on demographics, smoking status, education, medication usage and self-assessed anthropometric measurements such as weight and height were collected through a self-administered questionnaire.23 A semiquantitative food frequency questionnaire (FFQ) of 204 items developed by the Division of Human Nutrition and Health of Wageningen University & Research was used to assess habitual dietary intake in the month before primary cancer diagnosis.23^,^32^,^33 Dietary supplement use was assessed in both cohorts using a self-administered dietary supplement questionnaire developed by the Division of Human Nutrition and Health of Wageningen University & Research, The Netherlands.23 Type of dietary supplements, frequency and duration of intake and dosage was recorded. Physical activity was assessed by the Short Questionnaire to ASsess Health-enhancing physical activity (SQUASH).34 The dietary inflammation score (DIS) and the lifestyle inflammation score (LIS) were used as proxy for the inflammatory potential of diet and lifestyle, respectively. In our previous work in the full COLON and PLCRC cohorts we assessed associations between inflammation markers and the DIS and LIS in the subpopulation for which inflammation marker data was available. A higher DIS seems to be associated with higher circulating levels of interleukin (IL)-6, IL-8 and high-sensitive C-reactive protein (hsCRP). A higher LIS was associated with higher circulating levels of IL-6, IL-8, tumour necrosis factor-α and hsCRP.35
Dietary inflammation score components and calculation
The DIS consists of 19 items and was calculated as previously described by Byrd et al.36 Although the DIS was developed and validated in a United States population, it has been successfully applied in other settings before, such as European populations.37 The 18 food groups in the DIS are ‘leafy greens and cruciferous vegetables’, ‘tomatoes’, ‘apples and berries’, ‘deep yellow or orange vegetables and fruits’, ‘other fruits and real fruit juices’, ‘other vegetables’, ‘legumes’, ‘fish’, ‘poultry’, ‘red and organ meats’, ‘processed meats’, ‘added sugar’, ‘high-fat dairy’, ‘low-fat dairy’, ‘coffee and tea’, ‘nuts’, ‘other fats’, ‘refined grains and starch vegetables’. Next to the food groups, supplement use was also included in the score. For the dietary supplement component, a combined score of micronutrients was calculated. This component was obtained by first ranking single supplemental micronutrient intakes into tertiles, stratified by sex. Secondly, a value of 2 was assigned to the highest tertile, 1 to the middle and 0 to the lowest tertile. Thirdly, multiplication took place with a value of −1 for the pro-inflammatory micronutrient iron.36 Multiplication with a value of +1 took place for the anti-inflammatory micronutrients (vitamins A, B12, B6, C, D and E; β-carotene, folate, niacin, riboflavin, calcium, magnesium, selenium, thiamine and zinc).36 Finally, a total supplemental micronutrient intake score was derived by summing all the values of the single nutrients, where a higher supplement score corresponds to a higher intake of anti-inflammatory supplements. This total supplemental micronutrient intake score represents the supplement intake component within the total DIS.
Each component (18 food group components and one supplement intake component) of the DIS was standardized by sex to a mean of 0 and standard deviation of 1, to obtain z-scores. Consequently, all food groups were multiplied by their respective weight (see Table 2). Finally, the sum of the intake of food groups × weights constituted the overall DIS. A higher score means an exposure to a relatively more pro-inflammatory diet.Table 2. Inflammatory weight and descriptives of the components of the dietary and lifestyle inflammation scores (DIS and LIS), stratified by cases and matched controlsCasesMatched controlsInflammatory weightN167668DIS0.33 (−1.23 to 1.87)0.16 (−1.37 to 1.58)LIS0.23 (−0.18 to 0.89)0.05 (−0.41 to 0.73) Unknown534Intake of food groupsaLeafy greens and cruciferous vegetables−0.1432 (18-48)28 (16-45)Tomatoes−0.784 (1-12)5 (2-14)Apples and berries−0.6576 (36-119)84 (38-150)Yellow vegetables and fruits−0.5712 (5-21)11 (5-20)Other fruits and real fruit juices−0.16131 (63-214)115 (53-195)Other vegetables−0.1617 (7-32)18 (9-34)Legumes−0.0420 (8-36)20 (9-32)Fish−0.089 (4-15)10 (5-17)Poultry−0.4510 (4-18)11 (6-21)Red and organ meats0.0238 (19-56)38 (22-56)Processed meats0.6823 (12-39)24 (11-39)Products high in added sugars0.5622 (7-62)22 (8-56)High-fat dairyb−0.1479 (42-162)66 (32-121)Low-fat dairy−0.12145 (60-257)175 (64-291)Coffee and tea−0.25580 (435-779)580 (464-813)Nuts−0.446 (1-16)9 (3-20)Other fats0.3118 (9-30)20 (10-29)Refined grains and starchy vegetables0.72253 (190-322)260 (196-322)Energy (kcal/day)1.775 (1.427-2.133)1.827 (1.525-2.168)Any supplement use (yes)−0.8065 (39)326 (50) Unknown319Alcohol5 (0-20)5 (0-20)Alcohol categoricalc Heavy0.3027 (16)129 (19) Moderate−0.6683 (49)348 (52) None58 (35)194 (29)Moderate to vigorous physical activity (hours/week)10 (5-20)12 (5-21) Unknown533BMI Continuous27.0 (24.2-29.4)25.9 (23.7-29.0) **Normal (<25 kg/m^2^)**58 (35)277 (41) **Overweight (25-30 kg/m^2^)**0.8937 (22)119 (18) Obese (>30 kg/m^2^)1.5773 (43)274 (41) Unknown01Smoking status****Current0.5016 (9.6)43 (6.5)Former and never151 (90)620 (94) Unknown05Values presented are median (Q1-Q3) or n (%).BMI, body mass index.aThe intake of food groups is in g/day.bCream butter is included in the other fat food group.cAlcohol intake, assessed by the food frequency questionnaire, was divided over the categories ‘none’ (<1 g/day), ‘moderate’ (>1 and ≤14 g/day for women and >1 and ≤28 g/day for men)’, or ‘heavy’ (>14 g/day for women and >28 g/day for men).
LIS components and calculation
The LIS consists of four items: physical activity, smoking status, body mass index (BMI) and alcohol consumption.36 In the SQUASH questionnaire, participants were asked to report their average time per week spent on community activities, activity at work, household activities and leisure time activities. Physical activity level was quantified by assigning a metabolic equivalent of task (MET) value to each activity, using the Ainsworth compendium of physical activity, in combination with self-reported intensity.34 Tertiles of moderate-to-vigorous activity in hours per week were calculated. Smoking status was classified as current, former and never smokers. All former smokers stopped >1 year ago; if they stopped <1 year ago, they would be classified as current smokers. Self-assessed anthropometric measurements (height and weight) were used to calculate BMI (kg/m^2^). A BMI of ≤25 is considered ‘normal’, from >25 to <30 ‘overweight’ and ≥30 considered ‘obese’. Only seven people (1%) were underweight (BMI ranging between 17.4 and 18.4 kg/m^2^). Given the limited numbers, these people were categorized within the normal weight group for the construction of the score. Alcohol intake, assessed by the FFQ, was divided over the categories ‘none’ (<1 g/day), ‘moderate’ (>1 and ≤14 g/day for women and >1 and ≤28 g/day for men)’ or ‘heavy’ (>14 g/day for women and >28 g/day for men).
To calculate the LIS, all items were multiplied by their respective weight (see Table 2). Finally, the sum of the intake of lifestyle components × weights constituted the overall LIS. A higher score represented a more pro-inflammatory lifestyle.
Clinical information
Clinical information regarding stage of disease, tumour location and presence of comorbidities was derived from the Dutch ColoRectal Audit for the COLON study38 or the Dutch Cancer Registry for the PLCRC-PROTECT study.
Data analysis
Baseline characteristics presented for cases and matched controls are shown in Table 1. The data were described by medians and IQR, or percentages and frequencies. Table 2 shows the baseline descriptives of the DIS and LIS components, presented for cases and controls. The inflammatory weights of each item (derived from Byrd et al.36) are also included in this table.Table 1. Baseline characteristics of colon cancer patients, stratified by cases and matched controlsCases, n (%)Matched controls, n (%)N167668Sex (female)58 (35)221 (33)Age at diagnosis, years (median[Q1-Q3]****)67 (60-73)66 (60-73)Education levela Low63 (38)267 (40) Medium50 (30)176 (27) High54 (32)220 (33) Unknown05Regular use of NSAIDb Yes17 (10)62 (9.4) Unknown09ASA physical status classification 140 (25)186 (29) 295 (59)386 (60) 323 (14)72 (11) 42 (1.3)1 (0.2) Unknown723Location primary tumour Proximal colon75 (45)297 (44) Distal colon92 (55)371 (56)Stage of disease I10 (6.0)47 (7.0) II51 (31)200 (30) III106 (63)421 (63)Type of treatment Only surgery71 (43)291 (44) Adjuvant chemotherapy95 (57)372 (56) Other1 (1)5 (1)Tumour characteristics MSI15 (9)85 (13) Unknown757 KRAS mutated77 (48)246 (39) Unknown538 BRAF mutated29 (18)104 (17) Unknown538 TP53 mutated108 (67)410 (65) Unknown538 PIK3CA mutated27 (17)133 (21) Unknown538 APC mutated120 (76)492 (80) Unknown954Cohort COLON128 (77)521 (78) PLCRC39 (23)147 (22)Values presented are median (Q1-Q3) or n (%).ASA, American Society of Anesthesiologists; BMI, body mass index; MSI, microsatellite instability; NSAID, nonsteroidal anti-inflammatory drug.aEducation: Low education is defined as primary school and general lower secondary school; medium as lower vocational training and higher general secondary education; high as high vocational training and university.bRegular NSAID use: use of NSAID more than once a week.
An incidence rate ratio (IRR), which is the interpretation of an odds ratio in an incidence density sampling design,39 and 95% confidence interval (95% CI) for the associations between the DIS and LIS (continuously per one unit increase) and colon cancer recurrence were estimated using conditional logistic regression.40 These analyses were first stratified by MSI and MSS tumours (86%) and subsequently by other molecular tumour characteristics (i.e. KRAS, BRAF, PIK3CA, TP53, APC mutation status) (Table 3). As matching could introduce confounding,41 all matching variables (sex, age, disease stage) and cohort were included in the models. Although hospital was used as a matching variable in the COLON study, this was not added to the crude model a priori, because of the limited power. The effect of including hospital as a covariate into the model was tested in a sensitivity analysis. Also, energy intake was included in model 1. Model 2 was additionally adjusted for either lifestyle for the DIS model or diet for the LIS model. Adjusting for lifestyle was done by including the individual components of the LIS. Adjusting for diet was done by calculating an equally weighted DIS where, instead of the inflammatory weights from Table 2, either −1 (healthy food) or +1 (unhealthy food) was used. Additional potential confounders were added to the models when they changed the IRR substantially (>10%). Potential confounders considered were education level (low, medium, high), adjuvant chemotherapy (yes, no), daily nonsteroidal anti-inflammatory drug use (yes, no) and comorbidities (overall yes, no; cardiovascular diseases yes, no; diabetes yes, no; American Society of Anesthesiologists (ASA) score I, II, III, IV). None of these factors influenced the association and they were therefore not included in the models.Table 3. Associations of the dietary and lifestyle inflammation scores (DIS and LIS) with recurrence in colon cancer patients, overall and by molecular tumour characteristicsDISLISTotal populationRecurrence (local-regional and metastasis)N cases/controls167/668162/634Model 1a IRR (95% CI)1.05 (0.98-1.14)1.23 (0.98-1.53)Model 2b IRR (95% CI)1.04 (0.96-1.12)1.21 (0.97-1.52)Stratified microsatellite stability****MSIN cases/controls15/8514/78Model 1 IRR (95% CI)0.94 (0.71-1.26)1.16 (0.56-2.42)Model 2 IRR (95% CI)0.90 (0.63-1.27)1.69 (0.70-4.01)MSSN cases/controls145/526142/504Model 1 IRR (95% CI)1.05 (0.97-1.14)1.22 (0.95-1.55)Model 2 IRR (95% CI)1.03 (0.95-1.12)1.21 (0.95-1.55)Further stratified for other mutations in MSS tumourscKRAS mutatedN cases/controls74/22572/212Model 1 IRR (95% CI)1.03 (0.91-1.15)1.08 (0.77-1.52)Model 2 IRR (95% CI)1.03 (0.91-1.16)1.08 (0.77-1.52)KRAS wild typeN cases/controls69/29768/288Model 1 IRR (95% CI)1.09 (0.97-1.23)1.32 (0.91-1.90)Model 2 IRR (95% CI)1.05 (0.92-1.18)1.31 (0.90-1.90)BRAF mutatedN cases/controls16/4416/42Model 1 IRR (95% CI)1.12 (0.83-1.52)1.32 (0.58-3.01)Model 2 IRR (95% CI)1.21 (0.85-1.72)1.33 (0.58-3.04)BRAF wild typeN cases/controls127/478124/458Model 1 IRR (95% CI)1.04 (0.95-1.14)1.20 (0.92-1.56)Model 2 IRR (95% CI)1.02 (0.94-1.12)1.19 (0.92-1.55)PIK3CA mutatedN cases/controls22/10622/100Model 1 IRR (95% CI)0.96 (0.78-1.18)0.78 (0.42-1.44)Model 2 IRR (95% CI)0.97 (0.79-1.20)0.79 (0.42-1.46)PIK3CA wild typeN cases/controls121/416118/400Model 1 IRR (95% CI)1.07 (0.98-1.17)1.30 (0.99-1.72)Model 2 IRR (95% CI)1.05 (0.96-1.16)1.30 (0.98-1.71)TP53 mutatedN cases/controls102/373101/359Model 1 IRR (95% CI)1.05 (0.95-1.17)1.20 (0.89-1.62)Model 2 IRR (95% CI)1.03 (0.93-1.15)1.20 (0.88-1.62)TP53 wild typeN cases/controls41/14939/141Model 1 IRR (95% CI)1.06 (0.92-1.24)1.21 (0.78-1.89)Model 2 IRR (95% CI)1.05 (0.90-1.23)1.20 (0.77-1.88)APC mutatedN cases/controls111/466109/426Model 1 IRR (95% CI)1.05 (0.96-1.15)1.24 (0.94-1.64)Model 2 IRR (95% CI)1.02 (0.93-1.13)1.24 (0.93-1.64)APC wild typeN cases/controls28/6227/60Model 1 IRR (95% CI)1.20 (0.94-1.53)1.15 (0.63-2.10)Model 2 IRR (95% CI)1.21 (0.94-1.57)1.16 (0.63-2.12)Associations were assessed using conditional logistic regression analyses. DIS and LIS were added to the models as continuous variables, so IRRs are reflecting associations for a one unit increase in the DIS or LIS.CI, confidence interval; IRR, incident rate ratio; MSS, microsatellite stable.aModel 1 is adjusted for the matching factors; age at diagnosis (years), sex (male, female), stage of disease (I, II, III) and cohort (COLON/PLCRC), as well as for energy intake.bModel 2 additionally adjusted for smoking status (current, former and never), physical activity level (hours/week moderate to vigorous activity), body mass index (kg/m^2^) and alcohol intake (g/day) for the DIS and diet quality (equally weighted DIS) for the LIS. The cases/controls of model 2 are equal to the cases/controls for the LIS model 1 models.cGiven the low number of microsatellite instable (MSI) tumours, we could not further stratify in MSI tumours.
To investigate whether observed associations might be different for locoregional recurrences versus distant metastases, persons with a locoregional recurrence (n = 40) were excluded in a sensitivity analysis.
As supplementary analyses, associations between tumour characteristics and recurrences were investigated using conditional logistic regression models. Similar as for the associations between DIS and LIS and recurrence, the matching factors sex, disease stage and cohort were included in all models. Also treatment with adjuvant chemotherapy (yes/no) was included in the model a priori, because of its influence on recurrence risk and since molecular tumour characteristics seem to be associated with chemotherapy efficacy.42^,^43
Ethics approval
Both studies were performed in line with the principles of the Declaration of Helsinki and were approved by a medical ethics committee (COLON: region Arnhem-Nijmegen, 2009-349; PLCRC-PROTECT: University Medical Center Utrecht, 15-770/C). All study participants provided written informed consent.
Results
Baseline characteristics
In total, 167 cases and 668 matched controls were included in our data analyses. Cases and controls were successfully matched on age, sex and stage of disease (Table 1). In both groups, the medium age was 66 years (IQR 60-73 years), 33%-35% was female, and most participants had stage III disease at diagnosis (63%), followed by stage II (30%-31%) and stage I (6%-7%).
Compared with controls, cases had a slightly higher pro-inflammatory diet and lifestyle score (Table 2). In addition, cases had a higher intake of high-fat dairy and a lower intake of low-fat dairy and less often used dietary supplements. Cases had a higher BMI and were more often current smokers compared with matched controls (Table 2).
The inflammatory potential of diet and lifestyle in relation to recurrence in subgroups of patients based on molecular tumour characteristics
A higher DIS, corresponding to a more pro-inflammatory diet, was not associated with the risk of colon cancer recurrence (IRR 1.04, 95% CI 0.96-1.12), while a higher LIS, corresponding to a more pro-inflammatory lifestyle, seemed to be associated with a higher risk of recurrence (IRR 1.21, 95% CI 0.97-1.52) in the overall study population (Table 3).
Although no statistically significant associations were found, several intriguing trends were observed. Null associations between the DIS and recurrence seemed to be consistent within all subgroups based on tumour characteristics. No differences in association between the LIS and recurrence were observed in subgroups of patients with an MSI versus an MSS tumour. Interestingly, association between LIS and recurrence seemed to be different in MSS PIK3CA wildtype (IRR 1.30, 95% CI 0.98-1.71) versus MSS PIK3CA-mutated tumours (IRR 0.79, 95% 0.42-1.46). Furthermore, associations between the LIS and recurrence seemed to be stronger in patients with an MSS KRAS wildtype tumour compared with patients with an MSS KRAS-mutated tumour (IRR 1.31, 95% CI 0.90-1.90 and IRR 1.08, 95% CI 0.77-1.52, respectively). Associations between the LIS and recurrence were similar in subgroups of MSS BRAF wildtype versus mutated*, TP53* wildtype versus mutated and APC wildtype versus mutated tumours.
In sensitivity analyses with colon cancer metastasis as outcome, associations seemed to be slightly stronger compared with the associations with locoregional recurrences and metastasis combined (Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100202). For example, for the MSS PIK3CA wildtype, a higher LIS was statistically significantly associated with a higher risk of colon cancer metastasis (IRR 1.48, 95% CI 1.09-2.00) compared with for the risk of locoregional recurrences and metastasis combined (IRR 1.30, 95% CI 0.98-1.71).
Supplementary analyses: tumour characteristics and recurrence
MSI compared with MSS tumours seemed to be associated with a lower risk of colon cancer recurrence (IRR 0.60, 95% CI 0.33-1.09) (Supplementary Table S2, available at https://doi.org/10.1016/j.esmogo.2025.100202). Within MSS tumours, a tumour with a KRAS mutation compared with a KRAS wildtype seemed to be associated with a higher risk of colon cancer recurrence (IRR 1.40, 95% CI 0.96-2.04). Within MSS tumours, an APC mutation compared with an APC wildtype was associated with a lower risk of recurrence (IRR 0.56, 95% CI 0.34-0.91). No associations were observed between mutation status of BRAF, PIK3CA and TP53 and colon cancer recurrence.
Discussion
Our study is the first study to investigate associations between the inflammatory potential of diet and lifestyle in relation to colon cancer recurrence in subgroups based on common molecular tumour characteristics. A more pro-inflammatory diet was not associated with recurrence in the overall study population, nor in different subgroups based on molecular tumour characteristics. Persons with a more pro-inflammatory lifestyle seemed to have a higher risk of recurrence, although the association did not reach statistical significance. Associations between the LIS and recurrence appeared to be stronger in persons with an MSS KRAS or MSS PIK3CA wildtype tumour, compared with an MSS KRAS- or MSS PIK3CA-mutated tumour, respectively.
A more pro-inflammatory lifestyle, but not a more pro-inflammatory diet, seemed to be associated with a higher risk of recurrence in this nested case-control study. This is in line with our previous work in the overall COLON and PLCRC cohorts, where we observed a nonstatistically significantly higher risk of recurrence with a higher LIS (HR 1.10, 95% CI 0.91-1.35), but not with a higher DIS (0.95, 95% CI 0.89-1.02) in 2738 persons with stage I-III CRC.35 Since the COLON and PLCRC cohorts were the first studies in which associations between diet and lifestyle inflammation scores and colon cancer recurrence were investigated, our results should be confirmed in future studies.
Our results provide indications that associations between the LIS and colon cancer recurrence might be stronger in persons with KRAS or PIK3CA wildtype tumours. This would mean that adapting a less pro-inflammatory lifestyle might be especially beneficial for patients with a KRAS wildtype and/or PIK3CA wildtype tumour. While KRAS mutations are hypothesized to drive a pro-inflammatory tumour environment, KRAS wildtype tumours have a less aggressive inflammatory profile, leading to an environment that promotes immune activation against the tumour.14^,^16^,^18 Therefore, we hypothesize that KRAS wildtype tumours, compared with tumours with a KRAS mutation, might be more sensitive to the effects of lifestyle-induced inflammation. A similar mechanism can be hypothesized for PIK3CA-mutated versus wildtype tumours. PIK3CA-mutated tumours have a more pro-inflammatory and immune-suppressive profile, compared with PIK3CA wildtype tumours.20 As with KRAS wildtype tumours, PIK3CA wildtype tumours might better engage the immune system.20 Patients whose tumours are more sensitive to immune activation may be more likely to benefit from adopting a less pro-inflammatory lifestyle. In contrast, when the tumour microenvironment is predominantly immunosuppressive, it may override the potential beneficial effects of anti-inflammatory dietary and lifestyle changes. This suggests that the impact of lifestyle factors on recurrence could be modulated by tumour-intrinsic immune characteristics. An anti-inflammatory lifestyle includes becoming more physically active, reducing alcohol consumption, achieving a healthy BMI and stopping smoking. These lifestyle changes are not only potentially beneficial for cancer-related outcomes, but can also improve overall health and lower the disease burden of other chronic diseases, such as cardiovascular diseases, which are common in cancer survivors.44^,^45
In this study, association between tumour characteristics and recurrence, although not always statistically significant, was generally in line with results of previous studies.43^,^46, 47, 48, 49, 50, 51, 52 Associations between specific mutations and colon cancer recurrence often rely on the presence of co-existing mutations.53^,^54 However, analysing combinations of tumour mutations, especially within the context of lifestyle factors and recurrence, requires larger study populations.
More research is needed before recommendations regarding lifestyle based on molecular tumour characteristics can be provided. Firstly, our findings should be replicated in other study populations. Considering that analysing molecular tumour characteristics is both time consuming and costly, leveraging existing studies or datasets would be a preferable approach. Secondly, a larger population would allow for more robust analyses of how lifestyle interacts with combinations of mutations and other factors, such as cancer treatment, immune-related tumour characteristics such as immune cell infiltration and expression of inflammatory markers and germline genetics in the context of colon cancer recurrence. This level of detail could help refine personalized therapy approaches, including but not limited to lifestyle interventions, and could hopefully result in better patient outcomes.
This study stands out due to its comprehensive approach, integrating data on lifestyle factors, tumour characteristics and disease outcomes. However, this study is not without limitations. Although our study was relatively large, most of our findings did not reach statistical significance and should be interpreted with caution. Given our sample size, we would be able to detect an effect size (IRR) between 1.5 and 3.8 depending on the prevalence of the specific mutation with a power of 80% and an alpha of 0.05. Nevertheless, our results provide a valuable foundation for generating hypotheses and guiding future research. Furthermore, as the DIS and LIS were developed in a United States population, dietary intake and inflammatory weights might be different in our population of colon cancer patients in The Netherlands. We did observe an association between the EDIP score and cancer recurrence in our previous work within the COLON study.11 The EDIP score is a data-driven score, where inflammatory weights of food groups were derived from associations with inflammation markers in our own population of colon cancer patients. Therefore, the EDIP score, compared with the DIS, may better reflect the inflammatory potential of the diet for our specific study population. However, comparison with other studies and replication of results is easier with a standardized score such as the DIS. The associations observed between the DIS and LIS and recurrence in our nested case-control study were consistent with those in the overall COLON and PLCRC cohorts, while associations between molecular tumour characteristics and recurrence were mostly in line with previous literature, suggesting our nested case-control study accurately represents stage I-III colon cancer patients. Nevertheless, the generalizability of these findings to populations other than stage I-III colon cancer with a Western type of diet and lifestyle might be limited. Finally, investigating changes over time would be potentially interesting; based on our previous research, however, we observed that scores reflecting the inflammatory potential of diet and lifestyle remained relatively stable over time.35 Moreover, in longitudinal models within the full cohort, incorporating a slope to account for changes in these scores over time did not improve model performance,35 suggesting that baseline dietary patterns may be representative of the relevant exposure window for recurrence risk. In addition, the majority of cancer recurrences in our cohort occurred within the first 2 years after diagnosis (63%). Therefore, dietary intake 2 years after diagnosis would not be relevant to consider, since the exposure (dietary intake) in these cases is measured after the outcome (recurrent event).
To conclude, our results suggest that associations between the inflammatory potential of lifestyle and cancer recurrence might differ based on common molecular tumour characteristics. Larger studies, facilitated by consortia, are needed to further establish the interactions between lifestyle, tumour characteristics and colon cancer recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Greten F.R.Grivennikov S.I.Inflammation and cancer: triggers, mechanisms, and consequences Immunity 511201927413131503410.1016/j.immuni.2019.06.025PMC 6831096 · doi ↗ · pubmed ↗
- 2Schmitt M.Greten F.R.The inflammatory pathogenesis of colorectal cancer Nat Rev Immunol 211020216536673391123110.1038/s 41577-021-00534-x · doi ↗ · pubmed ↗
- 3Hanahan D.Hallmarks of cancer: new dimensions Cancer Discov 121202231463502220410.1158/2159-8290.CD-21-1059 · doi ↗ · pubmed ↗
- 4Hanahan D.Weinberg R.A.Hallmarks of cancer: the next generation Cell 144520116466742137623010.1016/j.cell.2011.02.013 · doi ↗ · pubmed ↗
- 5Verhagen M.P.Joosten R.Schmitt M.The origin of intestinal cancer in the context of inflammationbio Rxiv 202310.1101/2023.10.02.560432 · doi ↗
- 6Zitvogel L.Pietrocola F.Kroemer G.Nutrition, inflammation and cancer Nat Immunol 18820178438502872270710.1038/ni.3754 · doi ↗ · pubmed ↗
- 7Flynn M.G.Mc Farlin B.K.Markofski M.M.The anti-inflammatory actions of exercise training Am J Lifestyle Med 1320072202352543154510.1177/1559827607300283 PMC 4243532 · doi ↗ · pubmed ↗
- 8Deng F.E.Shivappa N.Tang Y.Mann J.R.Hebert J.R.Association between diet-related inflammation, all-cause, all-cancer, and cardiovascular disease mortality, with special focus on prediabetics: findings from NHANES III Eur J Nutr 5632017108510932682559210.1007/s 00394-016-1158-4 · doi ↗ · pubmed ↗