17.6% of patients in a German cohort with exocrine pancreatic cancer were diagnosed with a genetic tumor syndrome—a case for universal genetic testing?
D. William, M. Bermúdez, A. Kübler, C. Kahlert, M. Distler, J. Weitz, S. Uhrig, M. Fröhlich, B. Hutter, D. Aust, G. Baretton, P. Wimberger, K. Kast, C. Meisel, L. Gieldon, J. Porrmann, J. Wagner, M. Arlt, M. Franke, J. Fischer, K. Hackmann, S. Kreutzfeldt, A. Mock, C.E. Heilig

TL;DR
About 18% of pancreatic cancer patients in Germany had a genetic tumor syndrome, suggesting the need for universal genetic testing.
Contribution
The study shows that existing criteria miss some genetic variant carriers and supports universal genetic testing for pancreatic cancer patients.
Findings
17.6% of patients had a genetic tumor syndrome.
23.8% of pathogenic variant carriers would have been missed by current testing criteria.
A meta-analysis found a 14% median yield of pathogenic germline variants in pancreatic cancer.
Abstract
Yields for (likely) pathogenic germline variants (PGVs) in cancer predisposition genes (CPGs) in pancreatic cancer (PCA) cases range from 5% to 10% in initial literature to 15% to 20% in recent literature. PGVs can impact therapy recommendations and cancer surveillance for individuals and families. We retrospectively evaluated prospective cancer predisposition testing in 125 patients with exocrine PCA from a single-center clinical genetics clinic (n = 41) and a multicenter precision oncology program (n = 84) within 64 genes, including 14 established PCA risk genes. Associations with clinical and somatic molecular parameters, as well as therapy recommendations, were assessed. PGVs were identified in 21.6% of patients (n = 27/125) across 14 CPGs. A genetic tumor syndrome was diagnosed in 17.6% of patients (n = 22/125). Existing inclusion criteria for germline testing [European Society…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
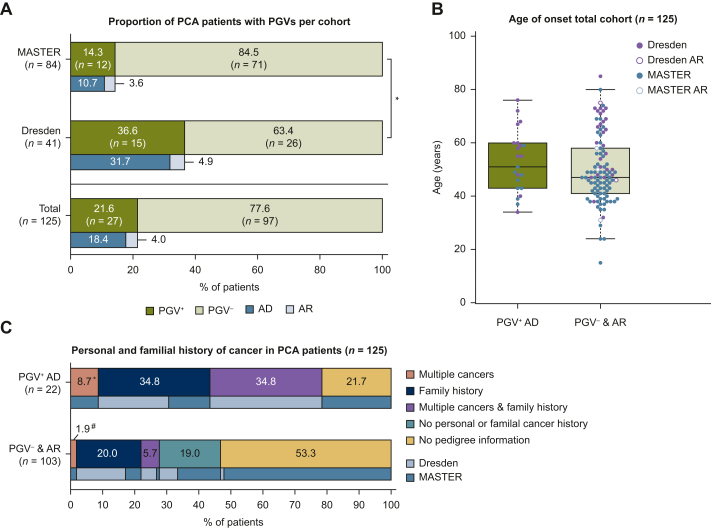 Figure 1
Figure 1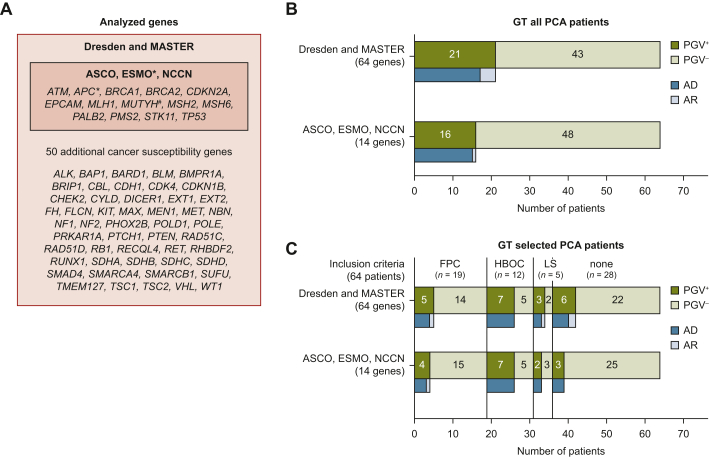 Figure 2
Figure 2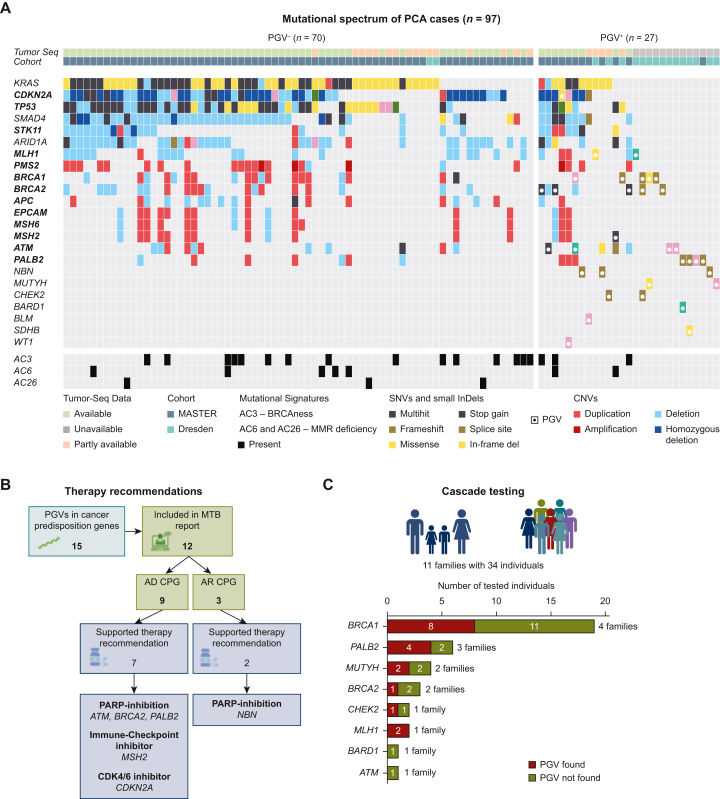 Figure 3
Figure 3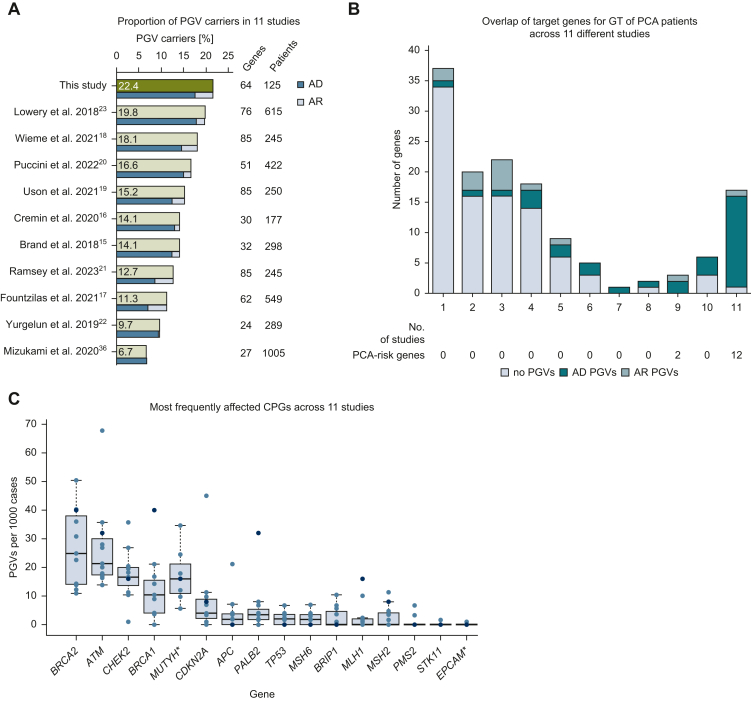 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cancer Genomics and Diagnostics · BRCA gene mutations in cancer
Introduction
Exocrine pancreatic cancer (PCA) is the third most common gastrointestinal cancer and is projected to become the second leading cause of cancer-related deaths in Western countries by 2030.1^,^2 The disease typically peaks in incidence at 65-69 years for men and 75-79 years for women, with a poor overall 5-year survival rate of only 8%.3 Despite general advances in cancer treatment, targeted therapy options for PCA patients are scarce. The poly (ADP-ribose) polymerase (PARP) inhibitor olaparib was approved as maintenance therapy for germline BRCA1/2-mutated, platinum-sensitive metastatic PCA, based on the POLO trial, which demonstrated prolonged progression-free survival (PFS) in these patients, and is under investigation as a potential treatment of PCA patients with (likely) pathogenic germline variants (PGVs) in other DNA damage repair-associated genes.4^,^5
Early detection of PCA and identification of high-risk individuals are crucial for improving the overall survival rate.6 The genetic risk factors for PCA are not yet fully understood. A proportion of PCA cases are associated with PGVs, particularly in BRCA1/2 in the European population (5%-7%).6^,^7 The increased risk may manifest as familial PCA (FPC), which is defined as having at least two first-degree relatives with PCA, without other hereditary (tumor) syndromes associated with increased PCA risk.7
It is important to note that the absence of familial PCA clustering does not exclude a PGV in PCA patients. Thus, diagnostic testing for PGVs in PCA patients may be of benefit to patients and their families at risk for familial PCA or for other genetic tumor syndromes.
Screening protocols involving endoscopic ultrasound or magnetic resonance imaging have shown benefits in resectability and survival.8^,^9 Enhancing our understanding of genetic risk factors and implementing effective screening protocols can significantly impact early detection and management of PCA.
Despite the therapeutic relevance and potential for cancer screening in patients and high-risk individuals, routine germline testing for all PCA patients has not yet been universally implemented, with varying guideline recommendations across organizations. The National Comprehensive Cancer Network (NCCN) and the American Society of Clinical Oncology (ASCO) recommend germline testing for all PCA patients, regardless of family history or disease stage.10^,^11 This recommendation is based on recent research showing that germline mutations can occur at similar rates in PCA patients with or without a family history of cancer.12
The European Society for Medical Oncology (ESMO) has more restrictive recommendations. They suggest genetic testing only for patients with metastatic PCA who are eligible for platinum-based chemotherapy or PCA patients who meet FPC criteria.13 These differing recommendations highlight the ongoing debate in the medical community regarding the optimal approach to germline testing in PCA patients.
Furthermore, there is a lack of consensus regarding which specific genes should be included in genetic testing panels for PCA patients.
Cancer predisposition genes (CPGs) associated with increased PCA risk encompass several categories. The genes primarily associated with hereditary breast and ovarian cancer (HBOC) include ATM, BRCA1/2, and PALB2. Lynch syndrome (LS) genes comprise MLH1, MSH2/6, PMS2, and EPCAM. Other genes associated with increased PCA risk are CDKN2A [familial atypical multiple mole melanoma (FAMMM)], STK11 [Peutz–Jeghers syndrome (PJS)], TP53 [Li–Fraumeni syndrome (LFS)], APC [familial adenomatous polyposis (FAP)], and various hereditary pancreatitis genes.7^,^14 The yield of PGVs in PCA patients varies widely, ranging from 4% to nearly 20%, depending on the gene panel used, variability in variant evaluation, and patient selection criteria.15, 16, 17, 18, 19, 20, 21, 22, 23
In this study, we conducted a retrospective analysis of PGVs in 64 CPGs across two German PCA cohorts. The cohorts, comprising 125 patients in total, were drawn from a clinical genetics clinic and a precision oncology program. Our analysis revealed that 17.6% of patients (n = 22/125) in the combined cohort carried a PGV in a dominant CPG. We evaluated various inclusion criteria for germline testing and examined the associations between PGVs and clinical and molecular parameters, as well as their clinical implications. Our findings aim to inform and improve genetic testing strategies and personalized care for PCA patients.
Materials and methods
Patients and clinical data
The retrospective analysis included 125 patients with PCA diagnosed between 2013 and 2021. Eighty-four were part of the National Center for Tumor Diseases (NCT)/German Cancer Research Center (DKFZ)/German Cancer Consortium (DKTK)-Molecularly Aided Stratification for Tumor Eradication (MASTER) precision oncology program (MASTER cohort), which focuses on advanced cancers in young patients (<51 years) and rare subtypes, providing molecular profiling, therapy recommendations, and genetic counseling.24^,^25 Forty-one patients were referred to genetic counseling at Dresden’s Institute for Clinical Genetics (Dresden cohort), primarily for high-risk screening or hereditary cancer evaluation. One Dresden cohort patient later joined MASTER. Patients with hereditary pancreatitis and endocrine PCA were excluded. Family cancer histories were documented for 64 patients. Protocols followed the Declaration of Helsinki, with ethics approvals from Heidelberg (S-206/2011, MASTER) and Dresden (EK-495112022) institutions, and written consent obtained for anonymized data use. Clinical and familial cancer data were extracted from medical records (Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218).
Next-generation sequencing
DNA from Dresden cohort patients was isolated from blood and ultrasonically sheared to 180-250 bp fragments (Covaris, LLC, Woburn, MA), with size verification via Fragment Analyzer (Agilent Technologies, Santa Clara, CA). Libraries were prepared using the TruSeq Nano DNA Kit and sequenced on a NextSeq500/550 (2 × 150 bp) after targeting 94 or 113 CPGs (TruSight Cancer panels, Illumina Inc., San Diego, CA). Fastq files were aligned to hg19 using Qiagen Biomedical Genomics Workbench 5.0 (Qiagen, Hilden, Germany), with variants detected via CLC BMW’s low-frequency tool (minimum variant allele frequency of 10%, target regions only). The MASTER cohort provided germline/somatic variant data and mutational signatures from tumor/control whole exome sequencing/whole genome sequencing.24, 25, 26
Bioinformatics gene panel
The available sequencing data (Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218) were filtered for variants in a core set of 14 genes recommended by ASCO and NCCN for genetic testing in PCA patients (APC, ATM, BRCA1/2, CDKN2A, EPCAM, MLH1, MSH2/6, MUTYH, PALB2, PMS2, STK11, TP53) and 50 additional hereditary cancer-associated genes (ALK, BAP1, BARD1, BLM, BMPR1A, BRIP1, CBL, CDH1, CDK4, CDKN1B, CHEK2, CYLD, DICER1, EXT1, EXT2, FH, FLCN, KIT, MAX, MEN1, MET, NBN, NF1, NF2, PHOX2B, POLD1, POLE, PRKAR1A, PTCH1, PTEN, RAD51C, RAD51D, RB1, RECQL4, RET, RHBDF2, RUNX1, SDHA, SDHB, SDHC, SDHD, SMAD4, SMARCA4, SMARCB1, SUFU, TMEM127, TSC1, TSC2, VHL, WT1).7^,^10^,^11^,^25 Of note, BARD1 was not included in the TruSightCancer94 panel (Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218). Genes associated with hereditary pancreatitis were excluded. Variant classification was carried out in accordance with the standards and guidelines of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology (ACMG-AMP) and further ClinGen specifications.27^,^28
Inclusion criteria for germline testing of PCA patients
Medical records and family cancer histories were reviewed to identify patients meeting germline testing criteria. Families fulfilled criteria for familial pancreatic cancer (two or more first-degree relatives or one first-degree relative plus another relative with PCA), familial breast/ovarian cancer, or LS (Amsterdam-II), as detailed in Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218.7^,^29^,^30 No cases met criteria for PJS, FAMMM, or LFS.31, 32, 33 German guidelines restricting germline testing to BRCA1/2 in metastatic PCA patients for PARP inhibitors were excluded from this analysis.
Statistics
To assess whether two population proportions significantly differ on a single, categorical characteristic, the z-score test for two population proportions was used. The Kolmogorov–Smirnov test was used to determine if a sample distribution matches the characteristics of a normal distribution. For comparisons of numerical variables between two groups the t-test for two independent means was used.
Results
Likely pathogenic or pathogenic germline variants were identified in 21.6% (27/125) of patients in two cohorts
The study included 125 PCA patients: 84 from the multicenter MASTER precision oncology program and 41 from the Dresden genetics clinic (Table 1, Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218).24^,^25 The MASTER cohort had a younger median age of onset (45.5 years versus 60.0 years) due to its inclusion criterion of age <51 years, while the Dresden cohort had more prior cancer diagnoses (31.7% versus 6.0%, P < 0.001) and greater family cancer history availability (97.6% versus 28.6%). Dresden patients more often had a first-degree relative with cancer (82.9% versus 37.5%, P < 0.001) or PCA (50.0% versus 8.3%, P < 0.001). Germline variant analysis of 64 CPGs was carried out for most patients, except for 20 analyzed with the TruSight Cancer 94 panel, which excluded BARD1. Tumor sequencing was available for most MASTER patients (95.2% versus 7.3% in Dresden, Table 1).Table 1. Patient characteristicsTotal cohortN = 125 (%)Dresden cohortn = 41 (%)MASTER cohortn = 84 (%)Sex, n (%) Male61 (48.8)18 (43.9)43 (51.2) Female64 (51.2)23 (56.1)41 (48.8)Age, years Median486045.5 Range15-8534-8515-80Previous cancer diagnosis, n (%) Yes18 (14.4)13 (31.7)5 (6.0) No106 (84.4)27 (65.9)79 (94.0) N/A1 (0.8)1 (2.4)—Pedigree information available, n (%) Yes64 (51.2)40 (97.6)24 (28.6) No61 (48.8)1 (2.4)60 (71.4)History of cancer in at least one FDR, n (%) Yes, any entity including PCA43 (34.4)34 (82.9)9 (10.7) Yes, PCA22 (17.6)20 (48.8)2 (2.3) No21 (16.8)6 (14.6)15 (17.9) Unknown61 (48.8)1 (2.4)60 (71.4)Tumor sequencing available, n (%) Yes88 (70.4)4 (9.8)84 (100.0) No37 (29.6)37 (90.2)0 (0.0)FDR, first-degree relative; N/A, not available; PCA, pancreatic cancer.
Germline analysis identified 33 PGVs in 27/125 patients (21.6%), with a significantly higher rate in the Dresden cohort (36.6% versus 14.3%, P = 0.0045, Figure 1A). Most PGVs (81.8%, n = 27/33) were in autosomal dominant CPGs, diagnosing genetic tumor syndromes in 22/125 patients (17.6%, Supplementary Table S2, available at https://doi.org/10.1016/j.esmogo.2025.100218). Only heterozygous PGVs in autosomal recessive CPGs were detected. There was no significant difference in median age of onset between PGV carriers and noncarriers (51.0 years versus 47.0 years, P = 0.16, Figure 1B). Among patients with prior cancer diagnoses, 55.6% (n = 10/18) had a PGV in an autosomal dominant CPG, as did 37.2% (n = 16/43) with a family cancer history (Figure 1C). Pedigree data were unavailable for 48.8% of patients (n = 61/125).Figure 1Characterization of pancreatic cancer (PCA) patients across cohorts. (A) Percentage of pathogenic germline variant (PGV) carriers in all patients (n = 125), the MASTER cohort (n = 84), and the Dresden cohort (n = 41). blue bars: patients with PGVs in autosomal dominant (AD) cancer predisposition genes (CPGs); light blue bars: patients with PGVs in autosomal recessive (AR) CPGs. ∗P < 0.01. (B) Age of onset in PGV-negative and AD-PGV-positive PCA patients (n = 125), Green bar: patients with PGVs in AD CPGs (n = 22), light green bar: patients with no identified PGVs (n = 98) or PGVs in AR CPGs (n = 5); Blue dots: MASTER patients; purple dots: Dresden patients. (C) Previous cancer diagnoses and family history of cancer in patients with PGVs in AD CPGs (n = 22, upper bar) and patients with no identified PGVs (n = 98) or PGVs in AR CPGs (n = 5, lower bar), Light blue bars: patients from Dresden, blue bars: patients from MASTER. ∗One patient with multiple cancers and unavailable pedigree information. ^#^Two patients with multiple cancers and unavailable pedigree information.
Up to 23.8% of PGV carriers would have been missed by applying strict guidelines for germline testing in 64 PCA patients with available clinical information
International guidelines recommend germline testing for all PCA patients, with varying gene sets. ASCO and NCCN suggest testing 13 PCA risk genes, while ESMO advises BRCA1/2 testing for metastatic PCA and expanding to 14 genes for familial clustering (Figure 2A).10^,^11^,^13^,^34 In a group of 64 patients with sufficient clinical data, analysis of 64 genes identified 26 PGVs in 21/64 patients (32.8%). Testing only the 14 recommended genes would detect PGVs in 16/64 patients (25.0%), missing additional PGVs in CHEK2, SDHB, BARD1, WT1, and NBN (Figure 2B, Supplementary Table S1, available at https://doi.org/10.1016/j.esmogo.2025.100218). Applying germline testing criteria (HBOC, LS, FPC) would test only 36/64 patients (56.3%), identifying PGVs in 15/36 (41.7%), while missing PGVs in CHEK2 and NBN.7^,^29^,^30 Among the remaining 28 patients not meeting criteria, 6 had PGVs in autosomal dominant CPGs (PALB2, BRCA2, BARD1, SDHB, WT1) and 2 in NBN (Figure 2C). Testing only BRCA1/2 as per ESMO guidelines would identify 6/64 patients (13.3%) but miss 9 others with PGVs in autosomal dominant or autosomal recessive CPGs.13Figure 2Analyzed gene panels and fulfillment of genetic testing (GT) criteria by pancreatic cancer (PCA) patients. (A) List of all tested genes (64 genes, red box) including PCA risk genes recommended for testing by European Society for Medical Oncology (ESMO), American Society of Clinical Oncology (ASCO), and National Comprehensive Cancer Network (NCCN) (14 genes, blue box). ESMO∗ recommends testing at least BRCA1/2 for metastatic PCA and 14 CPGs in cases with familial clustering. ∗APC is only included in the ASCO and ESMO recommendations, ^#^MUTYH is only included in the ESMO recommendation.10^,^13^,^34 (B) Number of patients with PGVs in 64 genes (upper bar) or 14 genes (lower bar, ESMO, ASCO, NCCN recommendation) of all PCA patients. (C) Analysis of 64 genes or 14 genes of PCA patients who met the ESMO GT inclusion criteria for either familial PCA (FPC), Lynch syndrome (LS), or hereditary breast or ovarian cancer (HBOC), and patients not meeting any of the criteria (‘none’).
Two-thirds of PGVs supported treatment recommendations and led to cascade testing in 73% of patients with PGVs
Germline analysis identified 33 PGVs across 14 CPGs, predominantly in 8 PCA risk genes [72.7%; n = 24/33 of PGVs: BRCA1/2 (n = 5 each), ATM (n = 4), PALB2 (n = 4), MLH1 (n = 2), MUTYH (n = 2), MSH2 (n = 1), CDKN2A (n = 1)]. Remaining PGVs occurred in six non-PCA risk genes [27.3%; n = 9/33: BARD1 (n = 1), CHEK2 (n = 2), SDHB (n = 1), WT1 (n = 1, all autosomal dominant), NBN (n = 3), BLM (n = 1, both autosomal recessive)], with four patients harboring multiple autosomal dominant CPG variants (Figure 3A). There was no indication of mosaicism in analyzed genes in our cohort. However, copy number variation calling using panel data in the Dresden cohort was limited, and low-level mosaicism or copy number events below the detection threshold cannot be fully excluded.Figure 3Molecular analysis and clinical management of pancreatic cancer cases. (A) Mutational spectrum of 97 pancreatic cancer (PCA) cases grouped by pathogenic germline variant (PGV) status (left: PGV^−^, right: PGV^+^). PCA risk genes are shown in bold. Alterations marked as both ‘multihit’ and as PGV represent loss of heterozygosity (LOH). (B) Therapy recommendations supported by PGVs in the MASTER cohort. (C) Overview of cascade testing of relatives of individuals with PGVs. AD, autosomal dominant, AR, autosomal recessive; CNV, copy number variation; CPG, cancer predisposition gene; MMR, mismatch repair; MTB, molecular tumor board.
Tumor sequencing data (available for 88/125 cases, 70.4%) revealed frequent and PCA characteristic somatic alterations in KRAS (75.0%, n = 66/88), CDKN2A (65.9%, n = 58/88), TP53 (65.9%, n = 58/88), and SMAD4 (60.2%, n = 53/88, Figure 3A). Technical challenges (e.g. poor DNA quality or low tumor cell content) limited data completeness in 16.8% of cases (n = 21/125). No somatic data were available in 13/125 cases (10.4%).
In the multidisciplinary molecular tumor board, 69.2% of PGV-positive patients (n = 9/13) received therapy recommendations, primarily PARP inhibitors (BRCA1/2 alterations), immune checkpoint inhibitors, or CDK4/6 inhibitors (Figure 3B).25^,^35 Cascade testing of 34 relatives from 11 of 15 Dresden cohort patients with PGVs (73.3%) detected PGVs in 18 relatives (52.9%) from 7 different families, prompting tailored surveillance (Figure 3C).
Broad panel sequencing of PCA patients from 11 different studies yields 6.7%-21.6% of patients with PGVs in autosomal dominant CPGs
Analysis of 11 studies (including ours) with 125-1005 PCA patients (mean 387) assessed 140 CPGs (24-84 per study), revealing PGV yields of 6.7%-21.6% (mean 14.6%, median 14.1%, Figure 4A, Supplementary Table S3, available at https://doi.org/10.1016/j.esmogo.2025.100218).23^,^36 Among 18 CPGs analyzed in all studies (12 PCA risk genes), 80.3% of PGVs (n = 468/583) were detected in 11% of patients (Figure 4B). BRCA2 (19.9%), ATM (16.6%), CHEK2 (11.0%), and BRCA1 (8.4%) were most frequent (Figure 4C). MUTYH and EPCAM were analyzed in 9/11 studies. MUTYH had high yields in two studies, though inconsistent reporting of monoallelic variants limited comparisons.17^,^18^,^20, 21, 22^,^36 Our cohort showed elevated BRCA1, PALB2, and MLH1 PGV rates, potentially due to smaller size or enrichment for HBOC/LS families.Figure 4Meta-analysis of pathogenic germline variants (PGVs) in pancreatic cancer across 11 studies. (A) Percentage of pathogenic germline variant (PGV) carriers identified in different cohorts (green bars) in autosomal dominant (AD) cancer predisposition genes (CPGs) (blue bars) and autosomal recessive (AR) CPGs (Light blue bars). (B) Overlap of target genes across 11 studies with germline sequencing of pancreatic cancer (PCA) patients. Numbers of studies that nominated a specific gene and the PGV counts in AD and AR CPGs is depicted. (C) Most frequently affected CPGs across 11 studies, including PGV yields in 14 PCA risk genes (bold). Blue dots: this study. ∗MUTYH was analyzed in nine studies and heterozygous PGVs reported in seven studies. EPCAM was analyzed in nine studies. GT, genetic testing.
Discussion
This study detected (likely) PGVs in 21.6% (17.6% autosomal dominant) of PCA patients, exceeding previously reported yields (5%-10%).11^,^13 This higher prevalence likely reflects cohort inclusion biases: Dresden cohort patients were primarily referred based on personal/familial cancer history (nearly half had a first-degree relative with PCA), while MASTER cohort patients were selected for advanced cancers diagnosed before age 51 years. Consistent with referral patterns, autosomal dominant CPG PGVs were significantly more frequent in the Dresden cohort (31.7%, n = 13/41) than in MASTER (10.7%, n = 9/84), independent of age. A meta-analysis of 11 studies (4264 PCA patients) revealed a median PGV yield of 14.1% across 140 CPGs.
Current guidelines (ASCO, ESMO, NCCN) show inconsistencies in testing criteria and gene panels. ESMO’s recommendation to test metastatic PCA patients for BRCA1/2 variants risks missing other autosomal dominant CPG PGVs in cohorts enriched for FPC. Restricting testing to patients meeting FPC, LS, or HBOC criteria would have missed 23.8% of PGVs in our cohort. Among 21 autosomal dominant CPG PGVs detected in 64 patients, only 4 (19%) occurred in individuals meeting FPC criteria (BRCA1, PALB2, ATM, CHEK2).
Guideline discrepancies extend to gene selection, with variations in recommendations for APC, CDK4, MUTYH, and chronic pancreatitis genes.10^,^11^,^13^,^34 Limiting testing to 14 PCA risk genes would have missed 27%-28% of PGVs in this cohort. For example, CHEK2—a gene frequently altered in PCA (second to BRCA2 and ATM in 4264 patients across 11 cohorts)—is excluded from many panels.19, 20, 21, 22, 23, 24, 25, 26, 27^,^33^,^37 Notably, among 29/64 patients (45.3%) not meeting FPC/LS/HBOC criteria, 4 (13.8%) harbored 6 autosomal dominant CPG PGVs (BRCA2, BARD1, WT1, SDHB, 2x PALB2), and 2 had NBN variants. While not part of international guideline recommendations, BARD1 and WT1 are recommended to be included for germline testing in the German S3-Guideline for exocrine PCA. The contribution of SDHB to PCA is unclear, but in our cohort, the PGV in SDHB occurred in a patient that also had a PGV in PALB2, which has a clear PCA association. However, SDHB is included in the ACMG recommendations for secondary findings and was thus included in the report.38 Strict adherence to guidelines would have denied four patients a hereditary cancer diagnosis and five patients the opportunity for targeted therapies (e.g. PARP inhibitors for BRCA2/PALB2 alterations, immune checkpoint inhibitors for an microsatellite instability high case with MSH2 PGV, CDK4/6 inhibitors for CDKN2A).5^,^35 The benefit of PARP inhibitors for non-BRCA DNA repair genes or autosomal recessive CPG carriers remains unclear.5^,^6
These findings underscore the underestimation of genetic risks in PCA and advocate universal large-panel germline testing, given the broad spectrum of implicated genes.15, 16, 17, 18, 19, 20, 21, 22, 23^,^36 Harmonizing guidelines to include all actionable CPGs—irrespective of established PCA associations—is critical. Where tumor-only sequencing is used, germline confirmation should be prioritized.5^,^25^,^39^,^40
Despite the considerable benefits of broad genetic testing, challenges remain in integrating this approach into routine clinical practice. Cascade testing in 73.3% of patients identified PGVs in 47.4% of relatives, aligning with reports from centers using universal testing.37^,^41 Barriers include advanced disease, older age, and lack of social support.37 NCCN emphasizes rapid germline testing due to PCA’s poor prognosis, yet 16 families were excluded when index patients died before testing.10 Among these, six families had PGVs (BRCA2, BRCA1, CDKN2A, CHEK2, NBN). In one case, a CDKN2A PGV was identified in a relative only after a melanoma diagnosis (and the subsequent diagnosis of FAMMM), highlighting missed opportunities when providers deny testing due to restrictive criteria. Another important factor is the cost-effectiveness of universal germline testing. A 2020 economic evaluation comparing population-based BRCA1/2 testing with clinical criteria-based testing for HBOC demonstrated that population-based testing is cost-saving in high-income countries (e.g. UK, USA) and cost-effective in upper-middle-income countries (e.g. China, Brazil).42 However, it was not found to be cost-effective in low-middle-income countries such as India unless the cost of testing is substantially reduced.42 These findings highlight the sensitivity of cost-effectiveness outcomes to the price of genetic testing and underscore the complexity involved in generalizing such conclusions across different settings. Importantly, these results indicate that universal germline testing in PCA patients may be economically justifiable and feasible, supporting its potential value also from a health economics standpoint.
While the presence of PGVs in PCA patients can inform clinical decisions, PGV interpretation remains complex, particularly for variants in understudied genes. At least 30% of families, especially in the Dresden cohort, have relatives eligible for PCA screening, necessitating multidisciplinary collaboration among geneticists, pathologists, and oncologists.
Our findings suggest that PGVs are more prevalent in PCA than historically recognized. Genetic testing should follow ASCO/NCCN guidelines and expand to all PCA patients, regardless of age or family history. Standardized, comprehensive panels are essential to optimize diagnosis, therapy, and cascade testing. Integrating genetic data into precision oncology is not merely advantageous but imperative for improving outcomes. A study showed significant survival benefits for patients with PGVs in CDKN2A undergoing surveillance for pancreatic cancer compared with those not in surveillance.43 Surveillance led to earlier detection, increased resectability, and a 5-year survival rate of 32.4% compared with 4.3% for nonsurveillance patients, supporting the notion that early detection strategies—including germline testing—can be life-saving when paired with high-quality, guideline-based care in certified centers to ensure low complication rates and the best possible results for all patients.43
Conclusions
PGVs are under-recognized in PCA. Harmonized guidelines should mandate comprehensive gene panels (beyond BRCA1/2) for all patients, irrespective of age/family history, to optimize diagnosis, therapy, and cascade testing. Multidisciplinary collaboration is essential to address clinical complexities and improve outcomes.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work the authors used Perplexity AI in order to refine phrasing and grammar. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Disclosure
Consultancies: AS: Aignostics, Amgen, Astra Zeneca, Bayer, BMS, Eli Lilly, Illumina, Incyte, Janssen, Jazz Pharmaceuticals, Merck, MSD, Novartis, Pfizer, Roche, Servier, Sanofi, Takeda, and Thermo Fisher. TH: Servier and Jazz Pharmaceuticals. SF: Illumina. Honoraria: TH: Astellas Pharma GmbH. Grants or other funding: AS: Bayer, BMS, MSD, Chugai, and Incyte. TH: Roche.
All remaining authors have declared no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rahib L.Smith B.D.Aizenberg R.Rosenzweig A.B.Fleshman J.M.Matrisian L.M.Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States Cancer Res 74112014291329212484064710.1158/0008-5472.CAN-14-0155 · doi ↗ · pubmed ↗
- 2Dyba T.Randi G.Bray F.The European cancer burden in 2020: Incidence and mortality estimates for 40 countries and 25 major cancers Eur J Cancer Oxf Engl 1990157202130834710.1016/j.ejca.2021.07.039PMC 856805834560371 · doi ↗ · pubmed ↗
- 3Stoop T.F.Javed A.A.Oba A.Pancreatic cancer Lancet 405104852025118212024018784410.1016/S 0140-6736(25)00261-2 · doi ↗ · pubmed ↗
- 4Golan T.Hammel P.Reni M.Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer N Engl J Med 381420193173273115796310.1056/NEJ Moa 1903387 PMC 6810605 · doi ↗ · pubmed ↗
- 5Javle M.Shacham-Shmueli E.Xiao L.Olaparib monotherapy for previously treated pancreatic cancer with DNA damage repair genetic alterations other than germline BRCA variants: findings from 2 phase 2 nonrandomized clinical trials JAMA Oncol 7520216936993366210010.1001/jamaoncol.2021.0006 PMC 7934074 · doi ↗ · pubmed ↗
- 6Mc Guigan A.Kelly P.Turkington R.C.Jones C.Coleman H.G.Mc Cain R.S.Pancreatic cancer: a review of clinical diagnosis, epidemiology, treatment and outcomes World J Gastroenterol 24432018484648613048769510.3748/wjg.v 24.i 43.4846 PMC 6250924 · doi ↗ · pubmed ↗
- 7Stjepanovic N.Moreira L.Carneiro F.Hereditary gastrointestinal cancers: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 30102019155815713137880710.1093/annonc/mdz 233 · doi ↗ · pubmed ↗
- 8Overbeek K.A.Levink I.J.M.Koopmann B.D.M.Long-term yield of pancreatic cancer surveillance in high-risk individuals Gut 7162022115211603382075610.1136/gutjnl-2020-323611 PMC 9120399 · doi ↗ · pubmed ↗