A Case of Metachronous Prostate Adenocarcinoma and Chromophobe Renal Cell Carcinoma in a Nigerian Male Patient: Diagnostic and Therapeutic Challenges
Olurotimi J Badero, Christiana Ogunlana, Adewumi Alabi, Victor Isibor

TL;DR
A 69-year-old man developed prostate cancer and later chromophobe renal cell carcinoma, highlighting the need for careful diagnosis and follow-up in complex urologic cases.
Contribution
This case report highlights the rare co-occurrence of two distinct urologic cancers and emphasizes the importance of immunohistochemistry in accurate diagnosis.
Findings
The patient was diagnosed with acinar adenocarcinoma of the prostate (Gleason 4+3) and later with chromophobe renal cell carcinoma.
Immunohistochemistry confirmed the renal tumor as the eosinophilic subtype of ChRCC, underscoring its diagnostic value.
The case underscores the need for thorough histopathologic evaluation and long-term follow-up in patients with complex urologic histories.
Abstract
Prostate adenocarcinoma and chromophobe renal cell carcinoma (ChRCC) are two distinct urologic malignancies with different prognoses and treatment approaches. The occurrence of both tumors in the same individual is highly unusual. We describe the case of a 69-year-old man with a long-standing history of hypertension who had previously undergone prostatectomy for benign prostatic hyperplasia. In 2022, he re-presented with recurrent lower urinary tract symptoms. Biopsy confirmed acinar adenocarcinoma of the prostate (Gleason 4+3), and magnetic resonance imaging (MRI) staged the disease as T3aN0M0. He was treated with high-dose-rate (HDR) brachytherapy followed by external beam radiotherapy (EBRT). Two years later, a right renal mass was detected. While the initial histology favored oncocytoma, immunohistochemistry revealed strong cytokeratin (CK)7 expression with focal CD117 staining,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
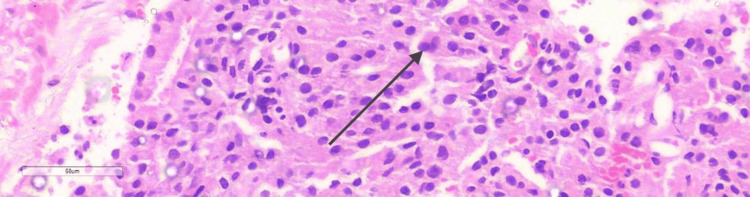 Figure 1
Figure 1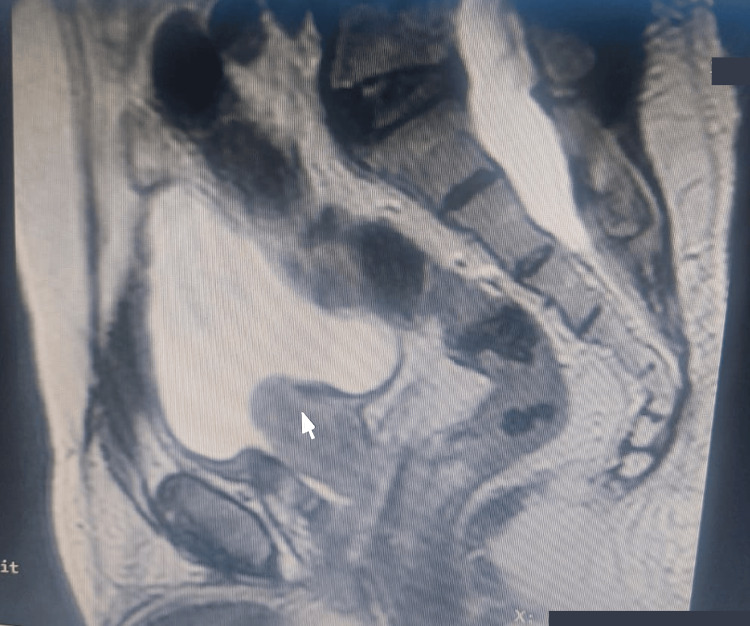 Figure 2
Figure 2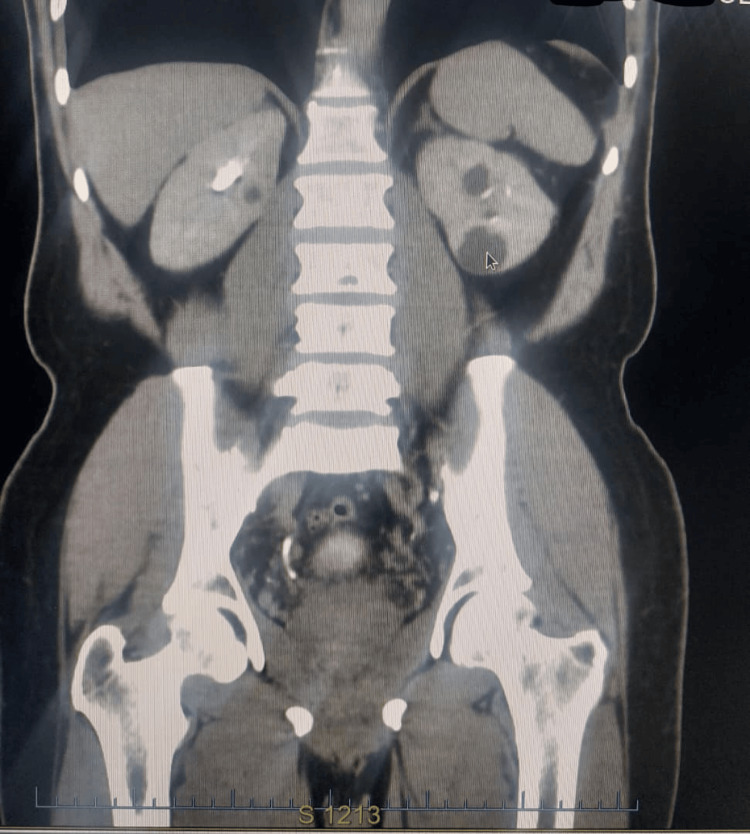 Figure 3
Figure 3| Date | Investigation | Result |
| Three years prior to presentation | Prostate biopsy | Adenocarcinoma, Gleason 4+3=7, ISUP Grade 3 |
| At presentation | Pelvic MRI | Extra-prostatic extension |
| At presentation | Abdominopelvic CT | No liver or bone metastases |
| At presentation | Bone scan | No osteoblastic metastases |
| At presentation | Renal histology and Immunohistochemistry | CK7: Strongly positive CD117: Rare foci |
| Date | Malignancy | Treatment given |
| A year prior to presentation | Renal cancer | Right nephrectomy |
| Two months prior to presentation | Prostate cancer | High Dose Rate Brachytherapy: 27 Gray in 2 fractions |
| Ongoing at the time of the report | Prostate cancer | External Beam Radiation Therapy: 50 Gray in 25 fractions |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Renal cell carcinoma treatment · Prostate Cancer Diagnosis and Treatment
Introduction
Prostate adenocarcinoma is the most frequently diagnosed non-cutaneous malignancy in men. By contrast, chromophobe renal cell carcinoma (ChRCC) accounts for only 5-7% of renal cell carcinomas [1]. Their coexistence in the same patient is rare and creates additional diagnostic and therapeutic challenges. We present a case of sequential prostate adenocarcinoma and chromophobe RCC in a Nigerian male patient, emphasizing the role of immunohistochemistry and the relevance of multimodal treatment.
Case presentation
A 69-year-old man with hypertension diagnosed three decades earlier was referred for external beam radiation therapy (EBRT) after already receiving high-dose rate (HDR) brachytherapy for prostate cancer. He denied smoking, alcohol use, or a family history of cancer. His past medical record was negative for diabetes, asthma, seizure disorders, or sickle cell disease. He had remained generally well until 10 years earlier, when he developed bladder outlet obstruction (BOO). A simple prostatectomy performed at that time reportedly demonstrated benign histology, with no evidence of malignancy on histopathological examination.
Seven years later, in 2022, he again developed BOO symptoms. A prostrate biopsy revealed acinar adenocarcinoma with a Gleason score of 4+3 (International Society of Urological Pathology (ISUP) grade group 3), as shown in Figure 1.
Photomicrograph of prostatic tissue showing tumour composed of malignant glands of varying shapes and sizes forming cribriform patterns. The glands are lined by single layer of mildly atypical cells with enlarged hyperchromatic nuclei (black arrow).Magnification: 4x 400; Stain used: hematoxylin and eosin
Magnetic resonance imaging (MRI) of the pelvis revealed extra-prostatic extension without nodal disease (T3aN0M0) as shown in Figure 2. Computed tomography (CT) scan of the abdomen and pelvis excluded liver metastases, and a bone scan ruled out skeletal involvement.
Pelvic MRI showing enlarged prostate (white arrow)
Two months prior to presentation, he received HDR brachytherapy to the prostatic bed, 27 Gy in two fractions (13.5 Gy each). At presentation, he was then scheduled for EBRT to the prostate, 50 Gy in 25 fractions.
Approximately one year before the current presentation for prostate cancer radiotherapy, the patient underwent a right nephrectomy for a renal mass. Abdominopelvic CT scan done at the time showed a renal mass (Figure 3). The initial histopathology suggested oncocytoma, but immunohistochemistry revealed cytokeratin (CK)7 positivity with focal CD117 expression, leading to a final diagnosis of eosinophilic variant ChRCC. There were no adverse histologic features such as sarcomatoid change, microscopic necrosis, or vascular invasion. Table 1 shows a list of the investigations carried out.
Abdominopelvic CT scan prior to nephrectomy
A diagnosis of prostate adenocarcinoma coexisting with chromophobe RCC was made. The treatments administered for the respective malignancies are listed in Table 2.
At the time of reporting, the patient was clinically stable, still undergoing EBRT, and showed no evidence of metastatic spread on imaging. He remains under active follow-up.
Discussion
The development of synchronous or metachronous tumors within the genitourinary tract is unusual, and such cases can present diagnostic dilemmas. Our patient first developed prostate adenocarcinoma, followed later by ChRCC; two biologically distinct tumors requiring different management strategies.
Prostate cancer is the most common solid tumor in men, and prognosis is closely linked to Gleason grading. Gleason 7 cancers, especially 4+3 patterns, carry a worse prognosis than 3+4 disease, necessitating more aggressive treatment [2]. In this patient, extra-prostatic extension warranted multimodal therapy, and he was managed with HDR brachytherapy followed by EBRT. HDR brachytherapy has demonstrated excellent local control and survival benefits both as primary and salvage therapy [3,4]. Combined modality approaches have further improved outcomes in high-risk disease [5].
ChRCC, though uncommon, generally has a more favorable prognosis than clear cell RCC provided that high-risk features such as sarcomatoid differentiation or necrosis are absent [6,7]. Accurate diagnosis is critical because management and prognosis differ significantly from those of other renal tumors. The eosinophilic variant of ChRCC can resemble renal oncocytoma on routine hematoxylin and eosin (H&E) staining, making diagnosis difficult. Immunohistochemistry, particularly CK7 positivity and variable CD117 expression, is extremely helpful in distinguishing the two [7,8]. This distinction has major clinical implications: oncocytoma is benign, whereas ChRCC requires surgical excision and long-term surveillance.
The ISUP grading system has refined prognostic classification for certain subtypes of RCC, while the World Health Organization (WHO) classification further integrates molecular and immunohistochemical features [9,10].
This case highlights several learning points. Recurrent urinary obstruction in a patient with prior prostate surgery should prompt reevaluation with biopsy, as earlier histologic testing may have missed malignancy. Second, multimodal therapy offers effective disease control in high-risk prostate cancer. Finally, the accurate diagnosis of renal tumors relies on following up histology with immunohistochemistry to avoid misclassification and inappropriate management [10].
Conclusions
This case highlights the importance of maintaining vigilance in patients with previous urologic interventions who develop new or recurrent symptoms. Beyond histology, the variation between oncocytoma and ChRCC requires immunohistochemical confirmation, as management differs significantly. For prostate cancer with extra-prostatic spread, timely multimodal therapy remains crucial for disease control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chromophobe renal cell carcinoma - a rare kidney cancer with limited therapy options: a narrative review BMC Urol Pashai Fakhri M Serth J Bräsen JH Ivanyi P Kuczyk MA Tezval H 1472520254045727210.1186/s 12894-025-01816-5PMC 12131663 · doi ↗ · pubmed ↗
- 2Gleason score and lethal prostate cancer: does 3 + 4 = 4 + 3?J Clin Oncol Stark JR Perner S Stampfer MJ 345934642720091943368510.1200/JCO.2008.20.4669 PMC 2717753 · doi ↗ · pubmed ↗
- 3GEC/ESTRO recommendations on high dose rate afterloading brachytherapy for localised prostate cancer: an update Radiother Oncol Hoskin PJ Colombo A Henry A Niehoff P Paulsen Hellebust T Siebert FA Kovacs G 32533210720132377340910.1016/j.radonc.2013.05.002 · doi ↗ · pubmed ↗
- 4High-dose-rate brachytherapy boost for prostate cancer: rationale and technique J Contemp Brachytherapy Morton GC 323330620142533713810.5114/jcb.2014.45759 PMC 4200189 · doi ↗ · pubmed ↗
- 5Editorial: optimizing local therapy for high-risk prostate cancer: evidence and emerging options Front Oncol Zaorsky NG Spratt DE Kishan AU Culp SH Showalter TN 16161020203298402810.3389/fonc.2020.01616 PMC 7481351 · doi ↗ · pubmed ↗
- 6Chromophobe renal cell carcinoma (RCC): oncological outcomes and prognostic factors in a large multicentre series BJU Int Volpe A Novara G Antonelli A 768311020122204451910.1111/j.1464-410X.2011.10690.x · doi ↗ · pubmed ↗
- 7Combined immunohistochemistry for the "Three 7" markers (CK 7, CD 117, and Claudin-7) is useful in the diagnosis of chromophobe renal cell carcinoma and for the exclusion of mimics: diagnostic experience from a single institution Dis Markers Zhou J Yang X Zhou L Zhang P Wang C 4708154201920193173712710.1155/2019/4708154 PMC 6815563 · doi ↗ · pubmed ↗
- 8Multilocular cystic renal cell carcinoma with focus on clinical and pathobiological aspects Histol Histopathol Kuroda N Ohe C Mikami S 9699742720122276387010.14670/HH-27.969 · doi ↗ · pubmed ↗