Molecular and immune characteristics of neuroendocrine bladder carcinoma—Implications for diagnosis, prognosis, and therapy: A review
Tianxiang Zhang, Xi Zhang, Lei Qian, Chunjiang Hu, Jianxing Li

TL;DR
This review summarizes the molecular and immune features of neuroendocrine bladder carcinoma to improve diagnosis and treatment strategies.
Contribution
The paper provides updated insights into the molecular and immune characteristics of NEBC and translates them into clinical guidance.
Findings
NEBC frequently co-occurs with urothelial bladder carcinoma and shares TP53 and RB1 alterations.
NEBC tumors exhibit an immune-cold microenvironment, limiting responses to immunotherapy.
Neoadjuvant chemotherapy followed by cystectomy improves outcomes compared to initial cystectomy alone.
Abstract
Neuroendocrine bladder carcinoma (NEBC) is a rare but highly aggressive histologic subtype of bladder cancer with poor prognosis, often driven by delayed diagnosis and limited therapeutic options; despite widespread use of next-generation sequencing, its cellular origin remains unclear and controversial. We aimed to synthesize up-to-date molecular and immune features of NEBC and translate them into practical guidance for diagnosis and treatment. We performed a narrative review of English-language studies indexed in PubMed and Web of Science (January 2000–August 2025) using predefined keywords, integrating genomic, transcriptomic, immunohistochemical, and clinical outcome data. Key findings indicate frequent co-occurrence and probable common clonal origin with urothelial bladder carcinoma, with hallmark TP53 and RB1 alterations, prevalent APOBEC-driven mutagenesis, and recurrent TERT…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
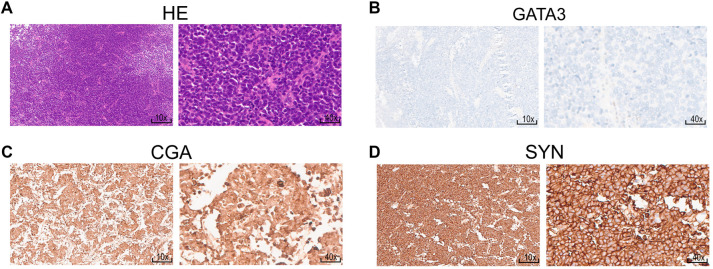 Figure 1
Figure 1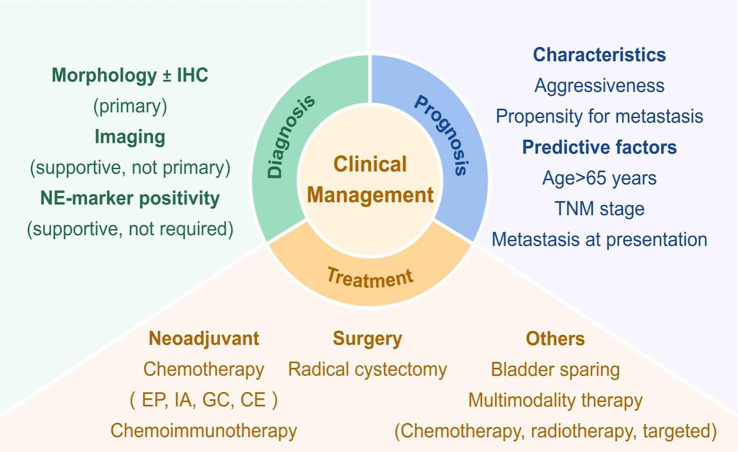 Figure 2
Figure 2|
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|---|
| Siefker-Radtke [ | RC only | 25 | NA | – | 23 (CSS) | 36% | |
| NAC+RC | 21 | IA or EP | 57% | Not reached | 78% | ||
| Siefker-Radtke [ | NAC+RC | 18 | IA or EP | 78% | 58 (OS) | – | |
| Lynch [ | RC only | 47 | NA | – | 18.3 (OS) | 20% | |
| NAC+RC | 48 | IA or EP etc. | 62% | 159.5 (OS) | 79% | ||
| Vetterlein [ | RC only | 144 | NA | – | 17.3 (OS) | – | |
| NAC+RC | 125 | cisplatin-based | 15.2% (pCR) | 34.7 (OS) | – | ||
| Alhalabi [ | RC only | 38 | NA | 21.1% | 20.6 (OS) | 22% | |
| NAC+RC | 141 | EP or IA etc. | 49.5% | 86.1 (OS) | 57% | ||
| Bakaloudi [ | NAC+RC | 29 | EP or CE or GC | – | 46 (OS) | 41% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Cancer Immunotherapy and Biomarkers
Introduction
Bladder cancer (BC) is the most prevalent malignant tumor of the urinary system, accounting for over 570,000 new cases and more than 210,000 deaths globally each year [1, 2]. BC is a heterogeneous disease characterized by various histological subtypes, including urothelial carcinoma, adenocarcinoma, squamous cell carcinoma, and neuroendocrine carcinoma [3]. Neuroendocrine tumors can develop in several anatomical sites, such as the sympathetic nervous system, adrenal gland, lung, pancreas, bladder, and prostate [4]. Regardless of their origin, neuroendocrine tumors consist of neuroendocrine cells that secrete bioactive substances and proteins, including somatostatin, insulin, gastrin, serotonin, and synaptophysin [5]. Histologically, neuroendocrine bladder carcinoma (NEBC) is classified as small cell carcinoma, large cell carcinoma, or mixed neuroendocrine carcinoma [6, 7]. Although NEBC is rare, representing less than 2% of BC diagnoses, it is an exceedingly aggressive disease [8]. NEBC is often diagnosed at an advanced stage, associated with a high metastatic potential and a 5-year survival rate of less than 10% [9, 10]. Consequently, early diagnosis and multimodal treatment strategies are crucial for managing NEBC [11–13]. Currently, NEBC diagnosis lacks a gold standard, relying primarily on morphological findings supplemented by immunohistochemical stains [7]; imaging serves only as an adjunctive tool and is not essential for definitive diagnosis [14].
Therapeutically, clinical guidelines for NEBC predominantly draw from management strategies for urothelial carcinoma and other neuroendocrine carcinomas (e.g., small cell lung cancer), supported by limited high-quality evidence [15]. The scarcity of NEBC cases in clinical trials further hampers the development of innovative therapeutic approaches [10]. In recent years, immunotherapy has emerged as a significant advancement in the treatment of urothelial cancer and other neuroendocrine carcinomas [16]. Among these therapies, immune checkpoint inhibitors (ICIs), particularly those targeting the PD-L1/PD-1 pathway, enhance T-cell-mediated tumor cytotoxicity, thereby exerting anti-tumor effects [17]. Our recent study has also demonstrated the superior efficacy of combined chemoimmunotherapy in NEBC [18]. However, a comprehensive understanding of the molecular and immune mechanisms underlying NEBC remains incomplete.
This review aims to synthesize current knowledge regarding the molecular and immune landscape of NEBC and provide translational insights for implementing these findings in personalized clinical management.
Literature search strategy
This literature review explores recent advancements in the molecular and immune characteristics of NEBC and their implications for diagnosis and treatment. We conducted a search in the PubMed and Web of Science databases for published English-language articles from January 2000 to August 2025. The search strategy employed a combination of keywords, including “neuroendocrine bladder carcinoma,” “bladder cancer,” “immune microenvironment,” “molecular features,” “immune checkpoint inhibitors,” and “neuroendocrine cancer.” Boolean operators (AND/OR) were utilized to refine search results.
The origin of NEBC
Common clonal origin hypothesis
Emerging evidence suggests that NEBC and urothelial bladder carcinoma (UBC) share a common cellular origin. In 2005, Cheng et al. [19] first proposed this common clonal origin of small cell carcinoma of the bladder (SCBC) and UBC at the molecular genetic level. They identified similar patterns of allelic imbalance and X-chromosome inactivation between SCBC and coexisting UBC, indicating that these tumors may arise from undifferentiated, multipotent progenitor cells within the urothelium [7, 19]. The heterogeneity of NEBC presents significant challenges to the accurate immunohistochemical identification of large cell NEBC [20]. NEBC and UBC are frequently observed together during histopathological examinations [7]. Approximately 40% of SCBC cases have been documented to exhibit mixed histological components of small cell and urothelial carcinomas [13]. Furthermore, NEBC and UBC often share similar somatic mutations within the same lesion, suggesting a clonal relationship between the two cancer types [19, 21]. Studies utilizing comparative genomic hybridization, next-generation sequencing, and immunohistochemistry have indicated that urothelial carcinoma may transform into NEBC through the accumulation of genetic mutations [22, 23]. Shen et al. [24] later demonstrated that the genomic profiles of NEBC are comparable to those of conventional UBC. Notably, both NEBC and UBC exhibit similar carcinogenic pathways driven by age-related and APOBEC-mediated mutational processes. By comparing genomic data from tumor samples of 87 SCBC cases to those of 303 high-grade UBC and 149 small cell lung cancers, Chang et al. [22] identified a similar histology-specific mutational pattern of somatic RB1 and TP53 driver mutations in SCBC and UBC, which were absent in small cell lung cancers. A comparative analysis of 25 BC cases coexisting with SCBC and non-small-cell phenotypes in the urothelium revealed an identical somatic mutation in the TERT promoter across both components [21]. Experimentally, Wang et al. [25] constructed a patient-derived xenograft model demonstrating that genetically engineered urothelial cells can give rise to mixed histological subtypes of NEBC and UBC. Additionally, another study suggested that miR-145 could induce a stem cell-like phenotype in urothelial carcinoma cells, promoting their differentiation into neuroendocrine cells by inhibiting syndecan-1 [26]. A case report from Robert-Bosch Hospital further illustrated that an invasive tumor developed within classical urothelial carcinoma in situ, comprising a mixed tumor of urothelial carcinoma in situ, NEBC, and an adenocarcinomatous component, with concurrent upregulation of p53 and strong cytoplasmic and membranous β-catenin staining [27]. Collectively, this evidence supports the hypothesis of a common origin between NEBC and UBC. However, further preclinical experimental models, particularly organoid models, warrant exploration to validate this hypothesis, as seen in studies involving small cell lung carcinoma and neuroendocrine prostate cancer [28–32].
Other hypotheses
While considerably less common, alternative theories regarding the origins of NEBC have been proposed. A study utilizing lineage tracing in a murine model of BC indicated that fundamental differences in the cell of origin may account for variations in clinical course, prognosis, and histological morphology, potentially explaining the distinctions between NEBC and UBC [33]. Additionally, a case study by Olivieri et al. found that UBC expressed cytokeratin but lacked synaptophysin expression, while NEBC co-expressed both markers. This led them to propose that NEBC may originate from the neuroendocrine system rather than from urothelial cells [34].
Molecular characteristics of NEBC
Emerging evidence suggests that BC ranks among the most frequently mutated human tumors, following lung and skin cancers in mutation frequency [35, 36]. This section examines the critical molecular alterations in NEBC and their potential implications.
TP53 and RB1
The inactivation of TP53 and RB1 serves as a significant biomarker for NEBC [37]. Alterations in these genes are present in nearly 80% of poorly differentiated neuroendocrine carcinomas [38]. Dysfunction of TP53 and RB1 is associated with histological progression to neuroendocrine carcinoma in lung and prostate cancers [39–42]. Recent studies have reported high mutation frequencies of TP53 and RB1 in NEBC. For instance, a study involving 61 SCBC patients indicated mutation frequencies of up to 90% for both genes [22]. Additionally, 80% of SCBC patients exhibited double mutations in TP53 and RB1. Similar findings emerged from research conducted by the Johns Hopkins Greenberg Bladder Cancer Institute, which documented mutation frequencies of 92% for TP53, 75% for RB1, and 72% for concurrent TP53/RB1 mutations in 132 SCBC patients [43]. Another study identified genetic alterations in TP53 and RB1 linked to reduced responsiveness to targeted therapies [24]. Notably, integrative analyses of muscle-invasive BC identified a neuronal subtype where 10 of 20 (50%) tissues displayed either both RB1 and TP53 alterations or E2F3 amplification [37]. Furthermore, 17 out of 20 (85%) tumor samples harbored somatic mutations in the p53/cell-cycle signaling pathway. Interestingly, in cases of UBC, inactivating mutations in TP53 and RB1 were reported in 12% of cases, suggesting these mutations may be sufficient, but not necessary, for the transformation into NEBC [44].
APOBEC
The apolipoprotein B mRNA editing enzyme, catalytic polypeptide (APOBEC) family comprises a group of cytosine deaminases [45]. Analyses of The Cancer Genome Atlas (TCGA) data indicate that APOBEC-mediated mutagenesis significantly contributes to BC carcinogenesis [44]. Conversely, another study integrating whole-exome sequencing, next-generation sequencing, and transcriptome analysis suggested that high APOBEC activity correlates with favorable prognosis, immune activation, and response to immune-checkpoint blockade in BC [46]. Specifically, in NEBC, APOBEC-driven mutational events occur in 95% of SCBC patients, potentially resulting in a high mutation burden [22]. Our previous study identified a prevalent APOBEC-mediated subtype characterized by distinct mutational signatures in NEBC patients [18, 24, 47]. Additionally, Robertson et al. identified a neuronal subtype in muscle-invasive BC associated with genes mutated alongside APOBEC activity [37, 47].
TERT promoter
Mutations in the TERT promoter represent a frequent molecular characteristic of NEBC. One study detected TERT promoter mutations in 55% (29 of 53) of SCBC cases [21]. Another study reported that 100% (10 of 10) of NEBC cases exhibited the TERT promoter C228T mutation [23]. Notably, SCCs from other cancer types, including prostate, lung, cervix, esophagus, and skin, did not harbor TERT promoter mutations, highlighting its potential as a diagnostic biomarker [23, 48]. Furthermore, the common allele rs2853669 within the TERT promoter mutation was associated with reduced overall survival and an elevated risk of tumor recurrence in BC [49, 50].
Immune features of NEBC
The bladder urothelium is continuously exposed to urinary carcinogens, such as tobacco-derived compounds, microbiota, and aromatic hydrocarbons. This ongoing exposure renders BC a highly immunogenic disease, often characterized by a high somatic mutation rate and an abundance of tumor neoantigens [51, 52]. Consequently, BC is particularly amenable to immunotherapy, resulting in the approval of multiple ICIs for clinical use [53]. However, the efficacy of immunotherapy remains limited in a subset of BC patients. Urgent investigation is warranted to comprehensively characterize the immune microenvironment of NEBC, identify responsive patient subgroups, and develop optimized therapeutic strategies.
Hematoxylin–eosin and immunohistochemistry staining of representative markers for the diagnosis of NEBC. (A) Hematoxylin–eosin staining of NEBC tissues. Immunohistochemistry staining of GATA3 (B), CGA (C) and SYN (D) in NEBC samples. 10× corresponds to 200 um, and 40× corresponds to 50 um. The images and stains were done following the approval from the Ethics Committee of Ren Ji Hospital (approval code: KY2022-038-B). The following primary antibodies were used: Anti-CGA (Proteintech, catalog no. 10529-1-AP, 1:500), anti-GATA3 (Proteintech, catalog no. 66400-1-Ig, 1:100), and anti-SYN (Proteintech, catalog no. 17785-1-AP, 1:1000). Abbreviations: NEBC: Neuroendocrine bladder cancer; GATA3: GATA-binding protein 3; CGA: Chromogranin A; SYN: Synaptophysin.
Tumor mutation burden (TMB)
TMB, defined as the number of mutations present in a tumor, reflects the level of neoantigens and the likelihood of T-cell recognition [54, 55]. A significant association between TMB and response to immunotherapy has been reported across various tumor types, including non-small cell lung cancer, melanoma, and urothelial carcinoma [56–58]. NEBC exhibits heterogeneous TMB levels. A study of 132 cases of small cell carcinoma of the bladder and upper urinary tract found that 26% of SCBC samples exhibited TMB ≥ 10 mutations/Mb, 3% had TMB ≥ 20 mutations/Mb, and the median TMB value was 6.2 mutations/Mb [43]. Another study involving 17 SCBC patients reported a median TMB of 10.7 (ranging from 1.2 to 41.1) mutations/Mb, significantly higher than observed in other genitourinary tumors [22]. Furthermore, Shen et al. reported an average mutation rate of 12.91 (ranging from 0.6 to 41.4) mutations/Mb in 12 resected genitourinary neuroendocrine neoplasms derived from the bladder [24]. A meta-analysis encompassing 27 tumor types demonstrated that the average response rate positively correlates with the logarithm of TMB [59]. Importantly, BC with a neuroendocrine-like molecular subtype is among the most sensitive tumors to ICIs, suggesting promising therapeutic efficacy for immunotherapy in NEBC [60, 61].
Immune infiltration
The tumor immune microenvironment—particularly the infiltration of CD8+ T cells associated with anti-tumor effects—enables the classification of NEBC into two (immune-cold and immune-hot) or three primary immunophenotypes (immune-inflamed, immune-excluded, and immune-desert) [62–64]. Despite high TMB, NEBC predominantly exhibits an immune-cold phenotype. Based on transcriptome sequencing of 24 SCBC cases and 51 UBC cases, Jean Hoffman-Censits et al. demonstrated that the expression of T-cell-related markers and inflammatory signaling pathways was suppressed in SCBC [43]. Another study comparing potential predictors between 12 SCBC and 69 UBC by immunohistochemistry concluded that SCBC primarily exhibited an immune-excluded subtype, which is characterized by the absence of PD-L1 expression and few tumor-infiltrating lymphocytes in the center of the cancer [65]. Similar findings were reported in small cell lung cancer research [66]. Chan et al. [67] identified an immunosuppressive tumor microenvironment in small cell lung cancer through single-cell sequencing, characterized by CD8+ T cell exhaustion. The distinct immune-excluded phenotype of NEBC may compromise the therapeutic efficacy of monotherapy with ICIs.
Clinical management of NEBC
Diagnosis
NEBC is characterized by an aggressive clinical course, typically presenting at an advanced stage with a high propensity for metastasis, resulting in a low overall 5-year survival rate of 8%–25%. Key negative prognostic factors include age over 65 years, advanced TNM stage, and metastatic disease at diagnosis, with tumor stage being the most significant predictor [3]. The diagnosis of NEBC poses considerable challenges for both pathologists and clinicians [68]. Currently, clinical diagnosis primarily relies on pathological morphology and immunohistochemistry [69]. Small cell neuroendocrine carcinoma is defined histologically by features such as sheets and nests of small cells, scant cytoplasm, speckled nuclei, and indistinct nucleoli [70, 71]. In the urinary bladder, NEBC often presents as a mixed component of SCBC and non-SCBC [12, 72]. Diagnosing large cell NEBC is considered more challenging than that of SCBC due to its morphologic characteristics. Large cell NEBC and mixed NEBC cases frequently exhibit enlarged nuclei, which may lead to misdiagnosis as high-grade urothelial carcinoma and delays in appropriate clinical intervention [6]. Distinguishing features between SCBC and large cell NEBC include larger tumor cells, a lower nuclear-to-cytoplasmic ratio, and prominent nucleoli in large cell NEBC [73]. Traditional neuroendocrine markers for NEBC, such as synaptophysin, chromogranin A (CGA), and CD56, have their limitations. For instance, CGA demonstrates a lack of sensitivity [7, 74], while CD56 exhibits high sensitivity but low specificity [75]. A combination of morphologic features and traditional immunohistochemical markers, including GATA3, CGA, and synaptophysin, is widely employed for NEBC diagnosis in clinical practice (Figure 1) [70, 74]. However, immunohistochemical staining may be focal or weak, and often only a few markers yield positive results. Thus, histomorphology alone may suffice for diagnosis, as neuroendocrine markers can be negative in 10% of cases [76]. There is an urgent need for novel diagnostic methods to enhance accuracy for NEBC. Kim et al. [70] developed a decision tree model based on synaptophysin, CD117, and GATA3, achieving 98.4% accuracy in identifying neuroendocrine differentiation in NEBC. Additionally, insulinoma-associated protein 1 (INSM1) has emerged as a promising diagnostic biomarker for neuroendocrine carcinomas across various anatomical sites, including the uterine cervix, pancreas, prostate, thoracic cavity, and head and neck, demonstrating both high sensitivity and specificity [77–80]. After evaluating INSM1 staining in NEBC, a study demonstrated that INSM1 was positive in 87% (28 of 32) of cases, highlighting its potential as a diagnostic tool for NEBC [81]. Moreover, neuronal markers identified through RNA sequencing or immunohistochemistry can also be utilized to define the neuroendocrine subtype in urothelial carcinoma, as these tumors may not exhibit the classic morphologic features of neuroendocrine neoplasms [37, 82].
Overview of NEBC management: Diagnosis, prognosis, and treatment. Abbreviations: IHC: Immunohistochemistry; NE: Neuroendocrine; EP: Etoposide and cisplatin; IA: Ifosfamide plus doxorubicin; GC: Gemcitabine and cisplatin; CE: Carboplatin and etoposide; TNM: Tumor-node-metastasis.
Treatment
The sensitivity of neoadjuvant chemotherapy (NAC) in NEBC has been confirmed in reports from various institutions [13, 83]. Recent studies have demonstrated significantly improved outcomes in SCBC patients receiving NAC, with 5-year cancer-specific survival rates increasing from 38% to 78% [84]. We summarized prior studies of large NEBC patient cohorts (Table 1), we found that IA (ifosfamide and doxorubicin) or EP (etoposide and cisplatin)-based NAC combined with radical resection resulted in significantly better survival outcomes than those observed in patients who did not receive NAC [84–89]. However, for patients with metastatic NEBC unsuitable for surgery, current treatment options are limited to EP chemotherapy and radiotherapy for metastatic lesions [37, 90]. Although these therapies achieve a relatively favorable response rate, limited progression-free survival and drug resistance remain prevalent [87, 91]. Given the high immunogenic potential of BC, immunotherapy, particularly ICIs, represents a promising therapeutic strategy for various BC subtypes, including NEBC [92]. A study reported that a recurrent metastatic NEBC patient responded favorably to pembrolizumab therapy in the sixth-line setting, with minimal drug toxicity [93]. Conversely, another retrospective study indicated that BC patients with neuroendocrine features exhibited shorter overall survival following ICI therapy compared to those with pure urothelial carcinoma [94]. Furthermore, our real-world experiences with off-label ICI use suggest that chemoimmunotherapy—a combination of chemotherapy and immunotherapy—might provide a therapeutic advantage for certain NEBC patients compared to chemotherapy alone [18]. Building on these promising preliminary findings, we have initiated a prospective clinical trial (ClinicalTrials.gov identifier: NCT06091124; Registration date: November 16, 2023; Registry: Ren Ji Hospital) to formally assess the efficacy and safety of neoadjuvant adebrelimab (anti-PD-L1) plus EP in patients with NEBC. Additionally, novel targeted therapies, particularly antibody-drug conjugates such as rovalpituzumab tesirine and sacituzumab govitecan, have shown preliminary efficacy in small cell lung cancer and NEBC [94–96]. Furthermore, innovative bladder-preserving approaches have been widely applied in the treatment of muscle-invasive BC. For instance, our preliminary findings suggest the safety and efficacy of combining disitamab vedotin with toripalimab and radiotherapy as a multimodal organ-sparing strategy for muscle-invasive BC [97]. As these approaches mature, their future application in bladder-preserving therapy for non-metastatic NEBC appears promising. Overall, compared to other neuroendocrine carcinomas, therapeutic options for NEBC remain limited. Additional novel therapies should be evaluated through prospective clinical trials involving NEBC patients.
Conclusion
Given its aggressive nature and unfavorable prognosis, NEBC requires prompt clinical intervention (Figure 2). The origin of NEBC remains unclear and controversial, necessitating further research to elucidate this phenomenon. Notably, the coexistence of high TMB and immune exclusion in the NEBC microenvironment offers novel insights for guiding immunotherapy. A comprehensive understanding of the molecular characteristics and an increased number of well-designed clinical trials are essential for addressing this aggressive subtype of BC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen W Zheng R Baade PD Zhang S Zeng H Bray F Cancer statistics in China, 2015 CA Cancer J Clin 201666211532 https://doi.org/10.3322/caac.213382680834210.3322/caac.21338 · doi ↗ · pubmed ↗
- 2Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 202171320949 https://doi.org/10.3322/caac.216603353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 3Gaisa NT Hartmann A Knüchel-Clarke R Neue WHO-klassifikation 2022: harnblasenkarzinom [new WHO classification 2022: urinary bladder cancer]Pathologie (Heidelb)202344213948 https://doi.org/10.1007/s 00292-023-01183-83682649310.1007/s 00292-023-01183-8 · doi ↗ · pubmed ↗
- 4Caplin ME Ratnayake GM Diagnostic and therapeutic advances in neuroendocrine tumours Nat Rev Endocrinol 2021172812 https://doi.org/10.1038/s 41574-020-00458-x 3333532910.1038/s 41574-020-00458-x · doi ↗ · pubmed ↗
- 5Bodei L Schoder H Baum RP Herrmann K Strosberg J Caplin M Molecular profiling of neuroendocrine tumours to predict response and toxicity to peptide receptor radionuclide therapy Lancet Oncol 2020219 e 43143 https://doi.org/10.1016/S 1470-2045(20)30323-53288847210.1016/S 1470-2045(20)30323-5PMC 8385643 · doi ↗ · pubmed ↗
- 6Kim S Seo J Shin Y Kim M Expression of insulinoma-associated protein 1 in gastric neuroendocrine and non-neuroendocrine neoplasms Discov Oncol 2025161754 https://doi.org/10.1007/s 12672-025-02576-24035885310.1007/s 12672-025-02576-2PMC 12075032 · doi ↗ · pubmed ↗
- 7Kouba EJ Cheng L Understanding the genetic landscape of small cell carcinoma of the urinary bladder and implications for diagnosis, prognosis, and treatment: a review JAMA Oncol 201731115708 https://doi.org/10.1001/jamaoncol.2016.70132833432410.1001/jamaoncol.2016.7013 · doi ↗ · pubmed ↗
- 8Perren A Couvelard A Scoazec JY Costa F Borbath I Delle Fave GENETS consensus guidelines for the standards of care in neuroendocrine tumors: pathology: diagnosis and prognostic stratification Neuroendocrinology 20171053196200 https://doi.org/10.1159/0004579562819001510.1159/000457956 · doi ↗ · pubmed ↗