Chronic otitis media with effusion in children with adenoidal hypertrophy: Development of a diagnostic prediction model
Yu Wu, Yuan Jiang, Yan-Xun Han, Da-Ming Wang, Chang-Yu Yao, Ye-Hai Liu

TL;DR
This study creates a prediction model to help doctors diagnose chronic ear infections in children with enlarged adenoids.
Contribution
A novel clinical prediction nomogram for COME in children with AH, incorporating four key risk factors and validated for high accuracy.
Findings
The predictive model achieved a high C-index of 0.945, indicating strong predictive accuracy.
Key risk factors include young age, vitamin D3 deficiency, degree of adenoidal hypertrophy, and tympanometry results.
The model showed good calibration and net benefit across a wide range of clinical thresholds.
Abstract
Chronic otitis media with effusion (COME) is a prevalent condition that poses significant risks to the growth and development of children with adenoidal hypertrophy (AH). This study investigates the risk factors associated with COME in children diagnosed with AH and establishes a clinical prediction nomogram to enhance diagnostic accuracy. The study included 311 children with AH, diagnosed through lateral nasopharyngeal radiographs, from the Department of Otorhinolaryngology Head and Neck Surgery at the First Affiliated Hospital of Anhui Medical University. Risk factors were identified using the least absolute shrinkage and selection operator (LASSO), while Firth’s penalized logistic regression analysis was employed to further refine the variables and develop a predictive model. The model’s performance was assessed using the C-index, calibration curve, and decision curve analysis, with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
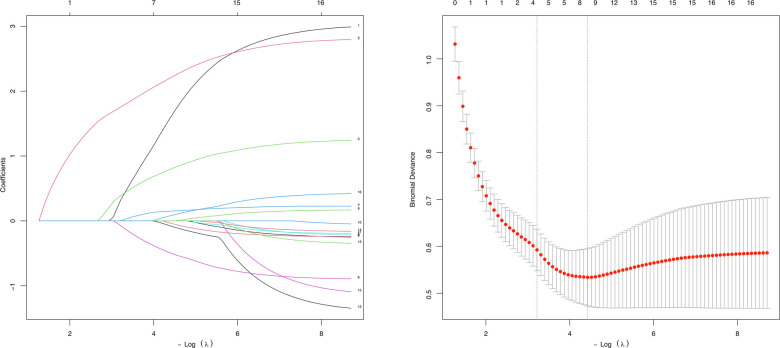 Figure 1
Figure 1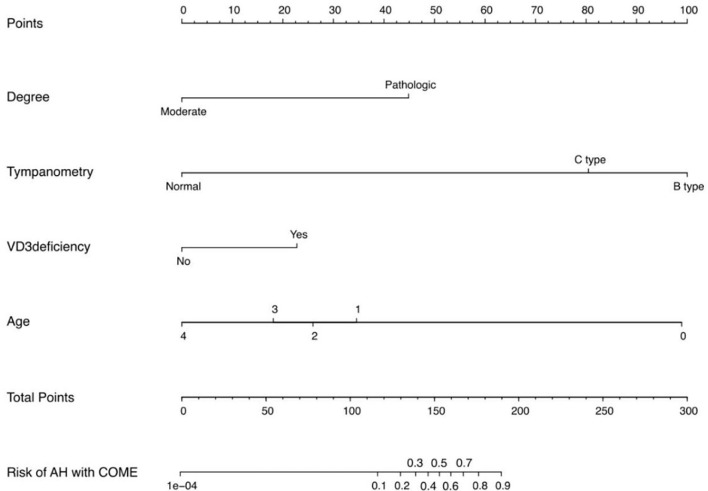 Figure 2
Figure 2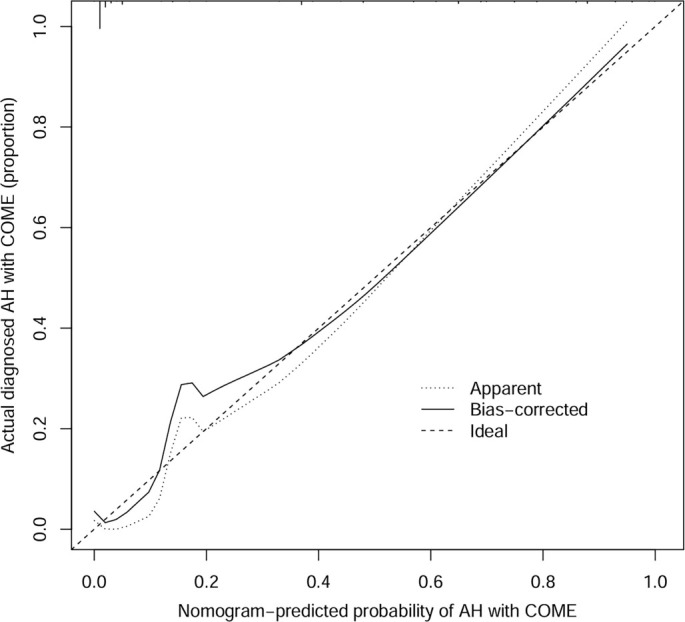 Figure 3
Figure 3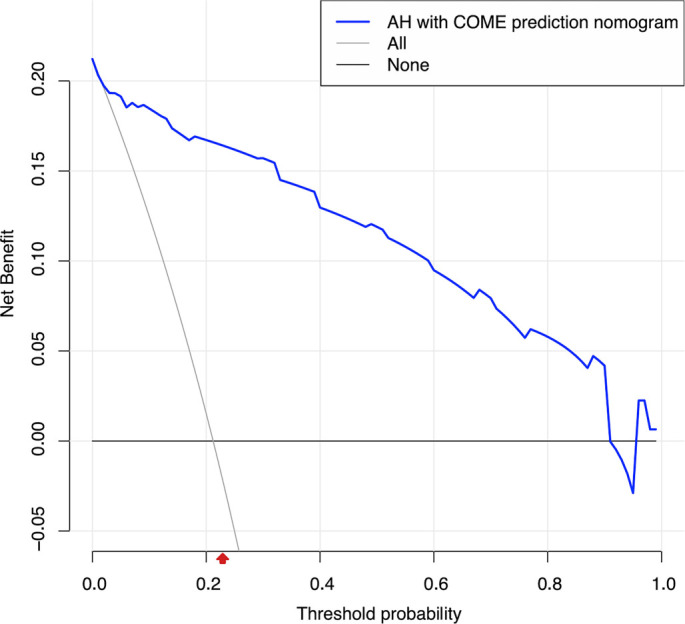 Figure 4
Figure 4|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|
| Age (year) | 6 (5, 8) | 6 (4, 8) | 6 (4, 8) | 0.223 | ||
| Sex | χ2 ═ 0.022 | 0.881 | ||||
| Male | 40 (60.6%) | 146 (59.6%) | 186 (59.8%) | |||
| Female | 26 (39.4%) | 99 (40.4%) | 125 (40.2%) | |||
| AH course (month) | 18 (9.75, 36) | 18 (12, 33) | 18 (12, 36) | 0.909 | ||
| Season | χ2 ═ 4.419 | 0.031 | ||||
| Winter and spring | 39 (59.1%) | 87 (35.5%) | 126 (40.5%) | |||
| Summer and autumn | 27 (40.9%) | 158 (64.5%) | 185 (59.5%) | |||
| BMI | χ2 ═ 2.210 | 0.530 | ||||
| Normal | 41 (62.1%) | 150 (61.2%) | 191 (61.4%) | |||
| Underweight | 0 (0.0%) | 7 (2.9%) | 7 (2.3%) | |||
| Overweight | 8 (12.1%) | 33 (13.5%) | 41 (13.2%) | |||
| Obesity | 17 (25.8%) | 55 (22.4%) | 72 (23.1) | |||
| A/N ratio | 0.82 (0.76, 0.88) | 0.79 (0.72, 0.86) | 0.80 (0.72, 0.86) | 0.024 | ||
| Degree | χ2 ═ 2.417 | 0.116 | ||||
| Moderate | 9 (13.6%) | 55 (22.4%) | 64 (20.6%) | |||
| Pathologic | 57 (86.4%) | 190 (77.6%) | 247 (79.4%) | |||
| Tympanometry | χ2 ═ 106.857 | <0.001 | ||||
| Normal | 2 (3.0%) | 178 (72.6%) | 180 (57.9%) | |||
| C type | 24 (36.4%) | 34 (13.9%) | 58 (18.6%) | |||
| B type | 40 (60.6%) | 33 (13.5%) | 73 (16.7%) | |||
| VD3 | χ2 ═ 37.851 | <0.001 | ||||
| Normal | 23 (34.8%) | 184 (75.1%) | 211 (67.8%) | |||
| VD3 deficiency | 43 (65.2%) | 61 (24.9%) | 100 (32.3%) | |||
| Allergen test | χ2 ═ 0.017 | 0.896 | ||||
| Normal | 34 (51.5%) | 124 (50.6%) | 158 (50.1%) | |||
| Positive | 32 (48.5%) | 121 (49.4%) | 153 (49.9) | |||
| Total IgE | 60.25 (27.80, 166.00) | 56.30 (23.40, 134.00) | 56.40 (25.30, 135.00) | 0.617 | ||
| NEUT% | 44.90 (37.15, 53.15) | 43.80 (35.10, 51.50) | 44.00 (36.00, 52.20) | 0.160 | ||
| LY% | 43.29±9.91 | 45.46±11.46 | 45.00±11.17 | 0.162 | ||
| MONO% | 5.90 (4.90, 7.03) | 6.10 (5.10, 6.90) | 6.0 (5.10, 7.00) | 0.977 | ||
| EOS% | 2.95 (1.80, 5.90) | 3.10 (2.10, 5.35) | 3.10 (2.00, 5.40) | 0.465 | ||
| BASO% | 0.50 (0.30, 0.80) | 0.50 (0.40, 0.70) | 0.50 (0.40, 0.70) | 0.927 |
|
|
|
|
|
|
|---|---|---|---|---|
| Age (year) | 3 | 5 | 7 | 11 |
| AH course (month) | 4 | 12 | 24 | 60 |
| A/N ratio | 0.636 | 0.760 | 0.830 | 0.920 |
| Total IgE | 5.485 | 34.760 | 99.280 | 510.600 |
| NEUT% | 26.66 | 38.72 | 48.70 | 63.08 |
| LY% | 26.50 | 41.20 | 49.90 | 62.34 |
| MONO% | 4.00 | 5.50 | 6.60 | 8.62 |
| EOS% | 1.1 | 2.4 | 4.1 | 9.5 |
| BASO% | 0.2 | 0.4 | 0.6 | 1.0 |
|
|
|
| ||
|---|---|---|---|---|
|
|
|
| ||
| Age (year) | Age=<3 (Reference) | |||
| 3<Age=<5 | --3.880 | 0.021 (0.002, 0.176) | <0.001 | |
| 5<Age=<7 | --3.744 | 0.024 (0.002, 0.183) | <0.001 | |
| 7<Age=<11 | --4.335 | 0.013 (0.001, 0.110) | <0.001 | |
| Age>11 | --4.643 | 0.010 (0.000, 0.156) | <0.001 | |
| Tympanometry | Normal (Reference) | |||
| Type C | 3.870 | 47.93 (13.54, 169.74) | <0.001 | |
| Type B | 5.004 | 148.94 (40.54, 547.43) | <0.001 | |
| VD3 deficiency | No (Reference) | |||
| Yes | 1.431 | 4.18 (1.49, 11.75) | 0.006 | |
| Degree | Moderate (Reference) | |||
| Pathologic | 2.682 | 14.61 (1.93, 110.40) | 0.008 | |
| Intercept | --6.731 | 0.001 (0.000, 0.20) | 0.007 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Vestibular and auditory disorders · Sinusitis and nasal conditions
Introduction
Otitis media with effusion (OME) is characterized by the presence of fluid in the middle ear without acute inflammation. A duration of OME exceeding three months is classified as chronic OME (COME) [1]. COME is among the most prevalent conditions affecting early childhood. Epidemiological studies have reported incidence rates of COME in adolescents ranging from approximately 15% to 30% in the United States, 32.3% in India, 16.5% in children attending primary clinics in South Africa, and between 1.16% and 30.7% in various regions of China [1–4]. Research by Tos [5] indicated that children experience OME at least once during their early years. COME is a significant contributor to hearing loss in children and can adversely impact speech and social development [6]. Additionally, prolonged negative pressure in the middle ear may influence vestibular function, leading to varying degrees of balance disorders in children during daily activities [7].
Research has identified multiple etiological factors associated with COME, including respiratory tract infections, adenoidal hypertrophy (AH)—influenced by the degree and location of the adenoid—maxillofacial deformities, allergic and immune responses, family environment, and breastfeeding practices [8–12]. Adenoids, functioning as immune lymphoid tissues in the nasopharynx, play a crucial role in preventing upper respiratory infections during infancy. However, the lymphoid tissues of young children may undergo hyperplastic changes due to repeated exposure to various pathogens, such as bacteria and viruses, leading to mouth breathing. Prolonged mouth breathing can contribute to maxillofacial deformities. Austin demonstrated that hyperplastic adenoids can mechanically obstruct the pharyngeal ostium of the Eustachian tube, resulting in sustained negative pressure in the middle ear and tympanic cavity, a common cause of COME in young children [13, 14].
Tympanometry serves as an effective, non-invasive method for assessing middle ear pressure, although it requires a certain level of cooperation from children. However, traditional tympanometry lacks 100% accuracy in diagnosing the presence of fluid in the middle ear [15, 16], particularly in type C tympanograms at 226 Hz [11]. Myringotomy and tympanocentesis are regarded as gold standards for diagnosing middle ear effusion but also necessitate high levels of cooperation from both the child and parents. These procedures must be performed under general anesthesia in pediatric patients and carry operational risks, such as poor healing of the tympanic membrane and damage to the auditory ossicles. Consequently, there is a need for a non-invasive and accurate diagnostic method for COME that integrates tympanometry with additional clinical factors. Nomograms, as visualization tools for statistical models, can consolidate multiple clinical variables, thereby enhancing the interpretability of predictive models.
This study aims to analyze and identify the risk factors for COME in children with AH, develop a diagnostic prediction model, and present it as a nomogram. The model is designed to provide a supplementary diagnostic tool for clinical settings in primary hospitals in China while minimizing the risks associated with invasive procedures.
Materials and methods
This study included children who exhibited persistent nocturnal mouth breathing and underwent surgical treatment between October 2021 and September 2022 at the Department of Otorhinolaryngology, Head and Neck Surgery, The First Affiliated Hospital of Anhui Medical University. All participants presented with symptoms of consistent mouth breathing and were diagnosed with AH through lateral nasopharyngeal radiographs, with or without accompanying hearing loss. Prior to surgery, all children received conservative treatment for a minimum of three months, which included intranasal steroid therapy and oral montelukast sodium, among other interventions. The children in this study showed inadequate improvement following these conservative measures. All pediatric patients underwent fasting blood sampling within 24 h of admission and, barring any contraindications, received surgical intervention within 72 h. Exclusion criteria encompassed a history of trauma to the head, middle, or inner ear; nasopharyngeal tumors; Down syndrome; mental illness; intellectual disabilities; congenital hearing impairment; significant comorbidities (e.g., heart, liver, kidney, or hematopoietic disorders); severe malnutrition; severe rickets; congenital cleft palate; craniofacial abnormalities; or developmental disorders of the nervous system. Family members of the patients provided informed consent and understanding regarding the study.
Invasive examinations often provoke resistance and distress in children, complicating the subjective assessment of AH classification. Given that lateral nasopharyngeal projection is more readily accessible in Chinese primary hospitals and more acceptable to children, this study utilized lateral nasopharyngeal projection results instead of electronic laryngoscopy to ascertain the presence of AH [17, 18]. The adenoid/nasopharyngeal (A/N) ratio served as the metric for evaluating the degree of AH. The thickness of the adenoid (A) was defined as the vertical distance from the most prominent point of the inferior margin of the adenoid to the tangent line of the occipital clivus. The width of the nasopharyngeal cavity at the most prominent part of the adenoid (N) was determined as the vertical distance from the posterior end of the hard palate to the intersection of the pterygoid plate and the skull base. The A/N ratio was calculated by dividing these two measurements. Various diagnostic methods for AH in children using lateral nasopharyngeal projection have been proposed both domestically and internationally, including the Fujioka diagnostic criteria [19]. After careful consideration of multiple standards, we selected the criterion most appropriate for the Chinese context. Based on a literature review [19–23], AH was classified into three categories: normal (A/N ≤ 0.60), moderate (0.60 < A/N ≤ 0.70), and pathological (A/N > 0.70). Two senior attending physicians independently interpreted the lateral nasopharyngeal radiographs. In cases where discrepancies in A/N ratio measurements arose, a chief physician made the final determination. Otherwise, the measurement from the more experienced senior attending physician was used. All physicians were blinded to the clinical data. The A/N ratios for the children in this study were found to be >0.60. Tympanometry was conducted using the AT235 device by Interacoustics in a quiet environment with a 226 Hz probe tone, and results were classified according to the Liden–Jerger classification system. Each patient underwent tympanometry twice: first during the initial clinic visit and again within 24 h of hospital admission. The tympanometry results obtained during hospitalization were used for data analysis. For further statistical analysis, patients were divided into three groups based on tympanometry results: Group A included children with tympanogram A in both ears (AA), Group C included children with tympanogram C (CC, AC, CA), and Group B included children with tympanogram B (BB, BC, CB, AB, BA) [24]. All participants underwent adenoidectomy and tympanocentesis under general anesthesia. If clinically indicated, these pediatric patients may subsequently receive myringotomy with or without grommet insertion. Patients were further categorized based on the presence or absence of middle ear effusion: AH with and without COME.
Relevant demographic data were extracted from medical records, including sex, age, duration of AH, height, weight, and the season of hospitalization as defined by the astronomical division method. Nutritional status was assessed using age- and sex-adjusted body mass index (BMI). According to the World Health Organization (WHO) 2006 child growth standards, subjects with a BMI below the 5th percentile for their sex and age group were classified as underweight, those with a BMI between the 85th and 95th percentiles were categorized as overweight, and those with a BMI at or above the 95th percentile were considered obese [25, 26]. Serum vitamin D3 levels were measured using a chemiluminescence immunoassay (CLIA) platform (CL-8000i, Mindray), with a coefficient of variation of ≤10%. Vitamin D3 deficiency was defined as a serum level of ≤20 ng/mL [27]. The percentages of neutrophils, lymphocytes, eosinophils, monocytes, and basophils were recorded during routine blood examinations. Additionally, allergen test results and total immunoglobulin E (IgE) levels were included.
Ethical statement
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the ethics committee of The First Affiliated Hospital of Anhui Medical University (Approval No. PJ 2023-13-30). Informed consent was obtained from the parents of all participants.
Statistical analysis
Descriptive statistics were performed using IBM SPSS Statistics for Windows, version 26.0. Continuous data with normal distributions were expressed as means ± standard deviation, while continuous data with skewed distributions were presented as medians (p25, p75), and discrete data were reported as N (%). Prior to data filtering, continuous variables were categorized based on the 5th, 35th, 65th, and 95th percentiles [28]. The least absolute shrinkage and selection operator (LASSO) method, suitable for high-dimensional data reduction, was employed to select optimal predictive features among the risk factors associated with AH in children [29, 30]. A Firth’s penalized logistic regression was conducted for final variable selection and predictive model development, utilizing the selected features to estimate the probability of outcome occurrence [31]. A two-sided P value of <0.05 was considered statistically significant. The predictive model was represented as a nomogram.
Results
This study involved 311 children diagnosed with AH. The male-to-female ratio among participants was approximately 3:2, with 186 male and 125 female patients categorized into two groups based on tympanocentesis findings: those with COME and those without. Table 1 summarizes the demographic and clinical characteristics of the participants.
To address the limitations of linear assumptions, this study opted not to construct a full restricted cubic spline (RCS) model. Instead, we utilized four recommended knot positions (p5, p35, p65, p95) to convert continuous variables into multi-categorical variables (Table 2), thereby simplifying the analytical process while still capturing potential nonlinear trends [28]. Employing LASSO regression, we identified eight key features from the 311 children: age, preoperative tympanometry results, vitamin D3 deficiency, A/N ratio, degree of AH, season of hospitalization, and the percentages of lymphocytes and basophils (Figure 1). These variables were analyzed using Firth’s penalized logistic regression (Table 3), resulting in four independent risk factors that were statistically significant: preoperative tympanometry results, vitamin D3 deficiency, degree of AH, and age. A predictive model incorporating these four factors was developed and presented as a nomogram (Figure 2). The calibration curve of the nomogram for predicting the risk of COME in children with AH indicated a strong fit between the apparent and ideal lines (Figure 3). The C-index for the prediction nomogram was 0.945 (95% confidence interval [CI] 0.941, 0.949). Bootstrap validation, which recalibrated the coefficients for the final set of predictors, yielded a C-index of 0.934, further confirming the nomogram’s high discriminative power. The incidence of AH with COME in this predictive model was 21.2% (66/311), comparable to the findings of Niedzielski et al. (20.4%, 110/539) [32]. Within this threshold, the decision curve was consistently above the none and all lines (Figure 4), indicating that all patients could benefit from this predictive model within a threshold range of 10%–90%. Thus, this model demonstrates significant clinical applicability.
Factor selection utilizing LASSO regression analysis. LASSO regression in 311 children with adenoidal hypertrophy produced coefficient profiles for all candidate variables across log(λ) (left) and the cross-validated deviance curve (right). At the optimal value of λ, eight predictors had non-zero coefficients: age, preoperative tympanometry results, vitamin D3 deficiency, A/N ratio, degree of adenoidal hypertrophy, season of hospitalization, percentage of lymphocytes, and percentage of basophils. Abbreviation: LASSO: Least absolute shrinkage and selection operator.
Discussion
This study developed a noninvasive diagnostic tool for COME in children with AH. Traditional diagnostic methods for COME include physical examinations and tympanometry. Physical examination of the ear is conducted using standard otoscopy or the maneuver method, wherein the presence of fluid in the middle ear is assessed through visual inspection of the tympanic membrane and tympanic cavity. However, electronic otoscopy may induce anxiety in children, leading to crying, which can obscure the examiner’s judgment. Consequently, cases of COME may be missed or misdiagnosed. Watters et al. [16] demonstrated that endoscopy alone is insufficient for reliably detecting middle ear effusion. Additionally, Ma et al. [33] reported that only 63.75% of children with COME exhibited middle ear effusion during examination. In our study, all children underwent a comprehensive physical examination prior to surgery, revealing a diagnostic rate of middle ear effusion of 65.2% (43/66) in the AH with COME group. The missed diagnoses may stem from the subjective nature of otoscopic judgments, which can vary based on examiner experience.
Tympanometry, a noninvasive and objective method for detecting pressure changes in the middle ear, is frequently employed to assist in diagnosing COME. Wu et al. [34] indicated that the preoperative tympanometric B-type curve pattern has a higher diagnostic rate for middle ear effusion. Despite this, traditional otological examination methods still exhibit room for improvement regarding their detection rates for COME. During our investigation, we considered including audiological factors; only auditory brainstem response (ABR) testing can accurately assess hearing loss across all pediatric age groups [10]. However, this diagnostic tool is not readily available in primary healthcare settings in China.
Recent guidelines in various countries have strongly advocated for pneumatic otoscopy as a critical examination method for diagnosing OME [10, 35, 36]. However, since pneumatic otoscopy requires significant cooperation from pediatric patients and has not been widely adopted, the proportion of diagnosed middle ear effusion cases remains low. In primary healthcare, only 7%–33% of physicians utilize pneumatic otoscopy for diagnosing middle ear effusion [10]. Some researchers have reported high specificity and sensitivity for routine middle ear and mastoid scans in diagnosing middle ear effusion [37]; however, due to radiation exposure, these scans are not recommended for younger patients.
In conclusion, the present study developed an accessible noninvasive tool by analyzing independent risk factors for COME in children with AH and evaluating its efficacy and clinical significance. The nomogram integrates traditional otological examinations with easily obtainable clinical data, enabling clinicians to calculate the probability of COME for children with AH based on outpatient examination results.
The risk factors for COME in children with AH have been extensively studied [38]. While the pathogenesis of COME remains unclear, multiple factors contribute to its development. These factors include respiratory tract infections, AH, maxillofacial deformities, allergic and immune responses, family environment, breastfeeding practices, family economic status, and parental education levels [8–10]. However, previous studies have yielded varying results. This study identified independent risk factors for COME in children with AH, including the degree of AH, vitamin D3 deficiency, age, and preoperative tympanometry results.
To assess the severity of AH, the study utilized lateral nasopharyngeal radiographs. Findings indicated that the degree of AH correlates with the development of COME; specifically, more severe AH increases the risk of COME. The Eustachian tube, an essential anatomical structure, regulates air pressure in the middle ear. Hypertrophic adenoid tissue can mechanically obstruct the pharyngeal orifice of the Eustachian tube, leading to negative pressure in the middle ear and the accumulation of effusion [13]. Additionally, hypertrophic adenoids serve as reservoirs for bacteria that form biofilms. Microorganisms from the upper respiratory tract may ascend through the Eustachian tube mucosa to the middle ear, resulting in retrograde infections [39]. Although lateral nasopharyngeal radiographs provide only a two-dimensional assessment of AH and may not fully illustrate the specific anatomical relationship of adenoid tissue obstructing the Eustachian tube’s pharyngeal opening, numerous studies have demonstrated a significant correlation between measurements from lateral radiographs and those obtained via endoscopic evaluation [40, 41]. Thus, lateral nasopharyngeal radiography remains a valuable tool for estimating adenoid size and guiding surgical decisions.
Nomogram for predicting adenoid hypertrophy (AH) in patients with chronic otitis media with effusion (COME). This nomogram is constructed using variables including age, tympanometry results, vitamin D3 deficiency, and the degree of adenoid hypertrophy. The age variable is encoded as follows: 0 indicates ≤3 years; 1 indicates >3 to ≤5 years; 2 indicates >5 to ≤7 years; 3 indicates >7 to ≤11 years; and 4 indicates >11 years.
Vitamin D3, the biologically active form of vitamin D in humans, is synthesized in the skin through ultraviolet-induced photoconversion of cholesterol and can also be obtained from dietary sources, such as animal liver. For healthy individuals, sunlight-derived vitamin D3 typically meets physiological requirements. Growing evidence suggests a link between vitamin D3 deficiency and the incidence of COME in children. A randomized controlled trial found that daily supplementation with 1000 IU of vitamin D3 over four months significantly reduced the incidence of OME to 44.8%, compared to 66.5% in the placebo group (P ═ 0.03) among 116 children [42]. This finding is further supported by a cohort study conducted by Walker et al. [43], which indicated that higher serum vitamin D3 levels correlate with a decreased risk of COME. Consistent with these reports, the nomogram developed in our study revealed that lower serum vitamin D3 levels are associated with an increased risk of COME in children with AH. Notably, the prevalence of vitamin D3 deficiency was significantly higher in AH patients with COME compared to those without (65.2% vs 24.9%, P < 0.01). This deficiency may contribute to pathological changes such as squamous metaplasia of the tympanic mucosa and impaired mucociliary clearance [44], facilitating the persistence of effusion. The pathogenic process likely involves colonized bacteria from hypertrophic adenoids migrating via the Eustachian tube, inducing goblet cell hyperplasia in the middle ear epithelium and leading to mucus-rich effusion with elevated mucin content [45]. Importantly, goblet cell proliferation often persists despite months of treatment, indicating potential irreversibility [46]. Vitamin D3 may modulate this process through various mechanisms, as higher serum levels enhance the expression of cathelicidin, an antimicrobial peptide; however, elevated mucin concentrations in middle ear effusion may compromise its efficacy [47, 48]. From an etiopathological perspective, vitamin D plays a critical role in regulating several key processes implicated in COME, including immune cytokine networks, Th1/Th2 balance, pathogen eradication, and Eustachian tube function [49–52]. Dysregulation of Th1/Th2 immunity, particularly Th2-cell overactivation, is a significant mechanism in the development of COME. Experimental studies have demonstrated that vitamin D3 can suppress T-lymphocyte proliferation and cytokine secretion, thereby mitigating immune-mediated tissue injury, inhibiting inflammatory cell activation, and reducing local mucin production [53, 54]. However, the causal relationship between vitamin D3 deficiency and the development of COME remains unclear. Scholars have suggested that the persistence of inflammatory states may affect vitamin D conversion [55–57]. Consequently, the high prevalence of vitamin D3 deficiency in children with COME may be a result of chronic otitis media.
Calibration curves of the nomogram. The bias-corrected line closely aligns with the ideal line, indicating a strong consistency between the model’s predicted probabilities and the observed outcomes. Abbreviations: AH: Adenoid hypertrophy; COME: Chronic otitis media with effusion.
Decision curve analysis of the prediction nomogram of AH with COME. This curve is based on the predicted probabilities derived from the apparent model, represented by the blue line. The figure compares the net benefits of three strategies: (1) the predictive nomogram; (2) the “All” strategy (Treat All), where all children with AH receive routine intervention; and (3) the “None” strategy (Treat None), where no additional intervention is administered to any child. The results indicate that across a broad threshold probability range of 10% to 90%, utilizing our model for clinical decision-making provides a higher net benefit compared to both the “All” and “None” strategies. Across this range of threshold probabilities (10% to 90%), the model provides clinical value by effectively identifying high-risk patients for intervention at any chosen threshold, while avoiding overtreatment of low-risk individuals. The red arrow denotes the incidence rate (21.2%) of COME in children with AH as observed in this study. Abbreviations: AH: Adenoid hypertrophy; COME: Chronic otitis media with effusion.
This study examined the seasonal patterns of hospitalization among children with AH and COME. Notably, 59.1% of children in the AH group with COME were admitted for treatment during the winter and spring months, compared to only 35.5% of those in the AH group without COME. A statistically significant difference in seasonal admissions was observed between the two groups (χ^2^ ═ 4.419, P ═ 0.031). However, this characteristic was not significant in LASSO regression analyses, likely due to the correlation between seasonal variations and serum vitamin D3 levels. LASSO regression effectively mitigates multicollinearity among factors by implementing feature selection. During winter and early spring, shorter daylight hours reduce children’s outdoor activities, leading to decreased vitamin D levels, which are closely associated with sunlight exposure and generally diminish during these seasons [45, 58]. Further research is necessary to explore the relationship between the incidence of COME in children with AH and daily sunshine duration.
The nomogram developed in this study indicated that younger children are at a heightened risk for developing COME. Previous studies, both domestic and international, have shown a correlation between younger age groups and the incidence of COME [59, 60]. The youngest patient in the AH with COME group was just 3 years old. Younger children often exhibit limited verbal skills, reduced attention spans, and difficulty understanding illness concepts or distinguishing between physical symptoms. Consequently, parents of young children with AH should remain vigilant regarding the potential for middle ear effusion.
This study introduced a predictive model for COME in patients with AH, utilizing risk factors and tympanometry results presented in a clinically applicable nomogram. This model serves as a personalized and relatively accurate tool for predicting COME, offering significant clinical value given the challenges in early detection of this condition. Specifically, young children with AH frequently struggle to articulate symptoms, and parental awareness of COME is often insufficient [38]. Consequently, medical intervention is typically sought only when children demonstrate substantial hearing loss or behavioral issues, such as concentration difficulties noted by educators. Additionally, children residing in rural areas face a greater risk of undiagnosed hearing impairments compared to their urban peers [61]. Consistent with previous reports, our study found that only 31.7% of patients with AH and COME actively reported hearing loss, a rate aligned with findings by Brennan-Jones et al. [15].
The model exhibited robust discriminative ability, achieving a C-index of 0.934 during internal validation, underscoring its potential for broader application in identifying and managing COME in children with AH. To enhance clinical utility, we established a three-tier risk stratification system based on predicted probabilities: low-risk (<20%), intermediate-risk (20%–60%), and high-risk (>60%). Corresponding management strategies were proposed, including watchful waiting with periodic follow-up for low-risk patients, referral for specialized audiological testing for intermediate-risk cases, and consultation with a specialist for high-risk individuals. This framework aims to serve as a clinical decision support tool, with final treatment tailored to individual patient conditions.
This retrospective study has several limitations. The selected risk factors were derived from prior studies and clinical observations. While existing literature has established associations between family socioeconomic status, indoor air pollution, family size, and pet ownership with the occurrence of COME in children [9, 62, 63], these potential socioeconomic factors were not included in our analysis. Additionally, evidence suggests that COVID-19 and its variants may influence the development and persistence of middle ear effusion [64]. Future studies should investigate the extent to which these factors contribute to the development of COME in children with AH. The bootstrap resampling approach was limited to refitting model coefficients for the final set of predictors without repeated variable screening. Furthermore, this single-center retrospective study necessitates validation through larger external datasets to confirm the accuracy and specificity of the nomogram. Given practical constraints, including limited equipment and technical capabilities in Chinese primary hospitals, this study did not analyze hearing loss in children or employ wideband acoustic immittance (WAI) to assess middle ear effusion. Although existing research has demonstrated that WAI offers higher sensitivity and specificity than conventional 226 Hz acoustic immittance in detecting middle ear effusion [65–67], such methods were not feasible in our setting. Future investigations will aim to incorporate more comprehensive audiological assessments to further explore the mechanistic relationships between COME and AH.
Conclusion
This study established a supplemental risk prediction model for COME in children with AH, based on preoperative tympanometry, the degree of AH, age, and serum vitamin D3 levels. Clinicians can utilize this nomogram to estimate the probability of this outcome and provide targeted medical interventions, thereby mitigating the adverse effects of COME on the growth and development of children with AH. The findings of this study require validation through external data, and further research is necessary to confirm the clinical significance of this nomogram.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Editorial Board of Chinese Journal of Otorhinolaryngology H Neck S Subspecialty Group of P[Guideline for the diagnosis and treatment of otitis media with effusion in children (2021)]Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 202156655667 https://doi.org/10.3760/cma.j.cn 115330-20210511-002643425647810.3760/cma.j.cn 115330-20210511-00264 · doi ↗ · pubmed ↗
- 2Baggi E Semino M Bianchini S Fattizzo M Rosazza C Esposito S Middle ear problems in children hospitalised because of lower respiratory tract infections: a comparison between two cohorts in Burundi and Italy Int J Pediatr Otorhinolaryngol 2013771219846 https://doi.org/10.1016/j.ijporl.2013.09.0182416950810.1016/j.ijporl.2013.09.018 · doi ↗ · pubmed ↗
- 3Parmar S Davessar JL Singh G Arora N Kansal L Singh J Prevalence of otitis media with effusion in children with hearing loss Indian J Otolaryngol Head Neck Surg 201971 Suppl_2127681 https://doi.org/10.1007/s 12070-018-1310-y 3175016410.1007/s 12070-018-1310-y PMC 6841788 · doi ↗ · pubmed ↗
- 4Biagio L Swanepoel DW Laurent C Lundberg T Paediatric otitis media at a primary healthcare clinic in South Africa S Afr Med J 201410464315 https://doi.org/10.7196/SAMJ.75342521425410.7196/samj.7534 · doi ↗ · pubmed ↗
- 5Tos M Epidemiology and natural history of secretory otitis Am J Otol 19845645962 https://doi.org/10.1016/S 0196-0709(84)80060-56542752 · pubmed ↗
- 6Vanneste P Page C Otitis media with effusion in children: pathophysiology, diagnosis, and treatment. A review J Otol 2019142339 https://doi.org/10.1016/j.joto.2019.01.0053122329910.1016/j.joto.2019.01.005PMC 6570640 · doi ↗ · pubmed ↗
- 7Li S Huang Y Chen X Wang W Zhang Q Zhang Q[Effect of otitis media with effusion on vestibular function in children: a pilot study]Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 20203432026 https://doi.org/10.13201/j.issn.2096-7993.2020.03.0043279158210.13201/j.issn.2096-7993.2020.03.004PMC 10127851 · doi ↗ · pubmed ↗
- 8Aniansson G Alm B Andersson B Hakansson A Larsson P Nylen OA prospective cohort study on breast-feeding and otitis media in Swedish infants Pediatr Infect Dis J 19941331838 https://doi.org/10.1097/00006454-199403000-00003817762410.1097/00006454-199403000-00003 · doi ↗ · pubmed ↗