Epidemiology and burden of alopecia areata in Taiwan: a systematic review
Chao-Chun Yang, Sheng-Hsiang Ma, Pei Jung Yen, Hung-Wei Lin, Kuei-An Chen, Chih-Chiang Chen

TL;DR
This paper reviews the epidemiology and health impact of alopecia areata in Taiwan, finding it affects about 0.01% of the population annually with autoimmune and mental health risks.
Contribution
The study provides updated epidemiological data and risk factors for alopecia areata in Taiwan using a systematic review of recent literature.
Findings
Annual incidence of alopecia areata in Taiwan is estimated at 0.011%.
Autoimmune diseases and psychiatric disorders are significant risk factors.
More research is needed on validated diagnostic criteria and systemic comorbidities.
Abstract
Alopecia areata (AA) is a common autoimmune disorder characterized by nonscarring hair loss on the scalp and/or body, affecting individuals of all genders, ages, and races. AA can occur alongside various autoimmune, atopic, and psychiatric conditions, affecting patients’ quality of life. Although AA is a relatively common condition, recent epidemiological data regarding this condition in Taiwan are lacking. This systematic literature review aimed to assess the epidemiology, risk factors, and comorbidities associated with AA in Taiwan by analyzing articles published from January 2010 to June 2024. A total of 37 studies were included, with most using the National Health Insurance Research Database (NHIRD) as the data source. The annual incidence and prevalence of AA in Taiwan were estimated at 0.011 and 0.014–0.016%, respectively. The mean age of AA onset ranged from 32 to 41.2 years,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
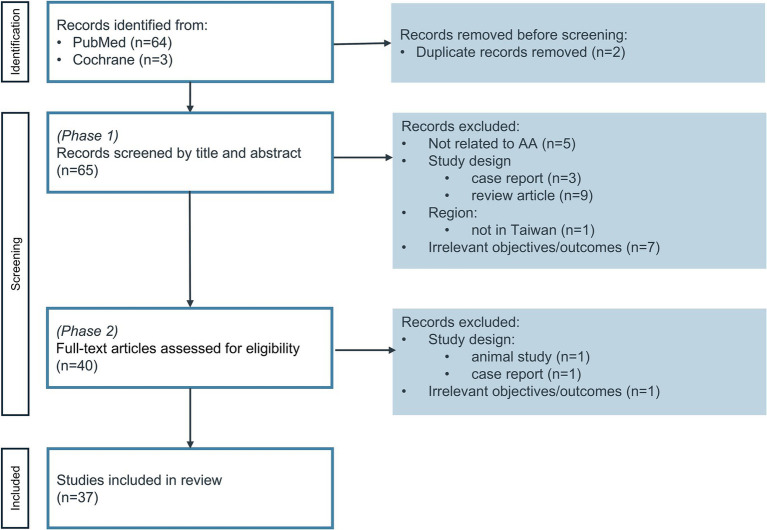 Figure 1
Figure 1| Study number | References and year | Data source† | Study design | Data period‡ | Study population | Outcomes of interest |
|---|---|---|---|---|---|---|
| 1. Epidemiology, patient characteristics and/or treatment patterns of AA in Taiwan | ||||||
| ( | Wu 2013 | Medical records from 2 sites in Taiwan | Longitudinal analysis | 1987–2010 | Late-onset AA (onset age at 50 years or above) | Patient characteristics and disease severity using guideline from US National Alopecia Areata Foundation (1999) |
| ( | Weng 2016 | NHIRD | Longitudinal analysis | 2000–2011 | Psoriasis with/without comorbidities (including AA) | Traditional Chinese Medicine Use |
| ( | Wong 2022 | Taiwan maternal and child health database | Longitudinal analysis | 2004–2017 | AA | Heritability of alopecia areata |
| ( | Tsai 2024 | NHIRD | Analysis 1: cross-sectional analysis | 2016–2021 | AA (severe and mild/moderate AA based on a claims-based algorithm)§ | Prevalence and incidence of AA, demographics and treatment patterns |
| 3. Comorbidities associated with AA patients | ||||||
| ( | Tsai 2011 | NHIRD | Cohort study | 2005–2008 | Psoriasis | Comorbidities including AA |
| ( | Chung 2015 | NHIRD | Case–control study | 1996–2011 | Lichen planus patients | Autoimmune comorbid diseases including AA |
| ( | Chen 2015 | NHIRD | Cohort study | 1996–2011 | Vitiligo | Comorbidities including AA |
| ( | Chiu 2017 | NHIRD | Case control study | 1997–2010 | Sarcoidosis | Autoimmune diseases including AA |
| ( | Liu 2019 | NHIRD | Cohort study | 2006–2013 | Prostate cancer patients with androgen deprivation therapy | Autoimmune comorbid diseases including AA |
| ( | Dai 2020 | NHIRD | Cohort study | 2001–2011 | Major depressive disorder | Autoimmune skin diseases including AA |
| ( | Dai 2020 | National health interview survey + NHIRD | Cohort study | 2001, 2005, 2009, 2013 | Smoker (current, former, never) | AA |
| ( | Chang 2020 | NHIRD | Cohort study | 2000–2012 | Rheumatoid arthritis | Alopecia |
| ( | Li 2020 | NHIRD | Nested Case–control study | 1998–2013 | Proton pump inhibitors users | AA |
| ( | Ma 2021 | NHIRD | Cohort study | 1998–2013 | Hepatitis C virus infection | Chronic inflammatory skin disease |
| ( | Tu 2021 | NHIRD | Cohort study | 1997–2013 | Human papillomavirus symptomatic infection | AA |
| ( | Ho 2021 | Taiwan Maternal and Child Health Database | Cohort study | 2004–2017 | Attention-Deficit/Hyperactivity Disorder with or without Methylphenidate Use | AA |
| ( | Chang 2021 | NHIRD | Cohort study | 1998–2013 | Polycystic ovary syndrome | AA |
| ( | Dai 2021 | NHIRD | Cohort study | 2001–2011 | Posttraumatic stress disorder | Autoimmune skin diseases including AA |
| ( | Hsieh 2022 | NHIRD | Cohort study | 1999–2013 | Ankylosing spondylitis | AA¶ |
| ( | Chou 2022 | NHIRD | Cohort study | 2001–2011 | Obsessive-compulsive disorder | AA |
| ( | Wang 2023 | Taiwan/China | Case–control study | 2021–2022 | COVID-19 vaccinations | Clinical characteristics and immune profiles of Immune-mediated alopecia |
| 3. Assessment of risk factors of developing AA | ||||||
| ( | Chu 2011 | NHIRD | Cohort study | 1996–2008 | AA | Comorbidity profiles |
| ( | Chu 2012 | NHIRD | Case–Control study | 2000–2009 | AA | Psychiatric comorbidities |
| ( | Kang 2015 | NHIRD | Cohort study | 2004–2011 | AA | Stroke |
| ( | Chen 2015 | NHIRD | Cohort study | 2001–2012 | AA | Herpes zoster |
| ( | Chen 2016 | NHIRD | Cohort study | 2003–2009 | AA | Autoimmune diseases |
| ( | Chen 2018 | NHIRD | Cohort study | 1997–2013 | AA | Cancer |
| ( | Ma 2020 | NHIRD | Cohort study | 1998–2011 | AA | Hearing loss |
| ( | Li 2021 | NHIRD | Cohort study | 1998–2013 | AA | Dementia |
| ( | Ting 2022 | NHIRD | Cohort study | 1997–2013 | AA | Retinal diseases |
| ( | Wang 2023 | NHIRD | Cohort study | 1997–2013 | AA | Suicide Attempt |
| 4. Bi-directional analysis of risk factors/comorbidities | ||||||
| ( | Wei 2020 | NHIRD | Cohort study | 1998–2011 | Bidirectional association between AA and atopic dermatitis | |
| ( | Dai 2020 | NHIRD | Cohort study | 1996–2011 | Bidirectional association between AA and major depressive disorder (proband and unaffected siblings, born before 1990) | |
| ( | Dai 2020 | NHIRD | Cohort study | Not mentioned; follow up until end of 2011 | Bidirectional association between AA and sleep disorders | |
| ( | Dai 2021 | NHIRD | Cohort study | 1998–2011 | Bidirectional association between AA and migraine | |
| ( | Dai 2022 | NHIRD | Cohort study | 1998–2013 | Bidirectional association between AA and irritable bowel syndrome | |
| ( | Dai 2021 | NHIRD | Cohort study | 1998–2011 | Bidirectional association between AA and thyroid diseases | |
| Study no. and references | Study type | Data source | Cohort identification period | Definition of AA† | AA cohort ( | Age at first diagnosis (years) | Sex |
|---|---|---|---|---|---|---|---|
| ( | Cohort study | 1 Mn NHIRD sample | 1996–2008 |
ICD-9-CM: 704.01 by dermatologist | 4,334 | Mean (SD): 32.2 (14.8) | 49% |
| ( | Cohort study | 1 Mn NHIRD sample | 2000–2009 |
ICD-9-CM: 704.01 outpatient visit by dermatologist | 5,117 | Median: 31 | 49% |
| ( | Cohort study | 1 Mn NHIRD sample | 2004–2011 |
ICD-9-CM: 704.01 during ambulatory care visit | 4,065 (all AA) | Mean: 36.1 | 49.2% |
| ( | Cohort study | 1 Mn NHIRD sample | 2003–2009 |
ICD-9-CM: 704.01 during ambulatory care visit | 4,665 (all AA) | NR | NR |
| ( | Cohort study | NHIRD§ | 1997–2003 |
Primary diagnosis of ICD-9-CM: 704.01 by dermatologists Without previously cancer | 162,499 | Mean (SD): 32.3 (14.8) | 47.97% |
| ( | Cohort study | NHIRD§ | 1998–2011 |
ICD-9-CM: 704.01 by dermatologists | 5,002 | Mean (SD): 37.4 (12.2) | 49.1% |
| ( | Cohort study; | 3 Mn NHIRD sample | 1998–2008 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists or rheumatologists | 13,931 | Median: 30.8 | 48.9% |
| ( | Cohort study; | 1 Mn NHIRD sample | 1996–2011 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists Born before 1990 | 2,123 | Median: 31.3 | 44.8% |
| ( | Cohort study; | NHIRD§ | Not mentioned; follow up until end of 2011 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists ≥20 years Without previous sleep disorders | 5,648 | Median: 34.1 | 52.2% |
| ( | Cohort study | NHIRD§ | 1998–2011 |
ICD-9-CM: 704.01 ≥2 visits by dermatologists Age ≥45 Without previous dementia | 2,534 | Mean (SD): 53.9 (7.5) | 42.4% |
| ( | Cohort study; | NHIRD§ | 1998–2011 |
ICD-9-CM: 704.01 by dermatologist | 5,608 | Median: 32.7 | 50.1% |
| ( | Cohort study; | NHIRD§ | 1998–2011 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists Excluded patients with thyroid diseases | 5,929 | Median: 32.6 | 51.9% |
| ( | Cohort study | NHIRD§ | 1997–2012 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists ≥3 years | 9,909 | Median: 31.6 | 48.5% |
| ( | Cohort study; | NHIRD§ | 1998–2011 |
ICD-9-CM: 704.01 ≥3 visits by dermatologists Excluded previous IBS | 5,446 | Mean (SD): 34.1 (13.5) | 49.5% |
| ( | Cohort study | NHIRD Sampling database | 1997–2013 |
ICD-9-CM: 704.01 ≥3 outpatient or 1 inpatient visit by dermatologists | 10,515 | Median: 33 | 48.8% |
| ( | Cohort study (Longitudinal analysis) | NHIRD full population dataset | 2017–2018 |
ICD-10-CM: L63 ≥3 visits by dermatologists or rheumatologists With at least 90 days between first and last claim Without other hair loss disorders¶ | Before matching: | Mean (SD):41.2 (14.17)†† | 53.4% |
| Risk factors | AA cases ( | AA cases ( | Relative risk estimation | Results (95% CI) | References |
|---|---|---|---|---|---|
| Chronic inflammatory dermatoses | |||||
| Psoriasis | 43/51,800 | 44/207,200 | aRR | 4.71 (2.98–7.45) | Tsai ( |
| Psoriasis | 7/5,179 | 194/320,415 | aHR | 2.44 (1.14–5.21) | Tu ( |
| Lichen planus | 126/12,427 | 145/49,708 | aOR | 2.82 (2.20–3.62) | Chung ( |
| Vitiligo | 270/14,883 | 179/59,532 | aOR | 5.11 (4.20–6.21) | Chen ( |
| Atopic dermatitis | 327/40,307 | 214/161,228 | aHR | 6.00 (5.04–7.14) | Wei ( |
| Autoimmune diseases | |||||
| Rheumatoid arthritis | 37/22,276 | 16/25,792 | aHR | 2.64 (1.47–4.76) | Chang ( |
| Ankylosing spondylitis | 5/28,825†† | 20/113,637†† | aHR | 0.98 (0.37–2.62) | Hsieh ( |
| Mental disorders | |||||
| All mental disorders† | 48/67,921†† | 153/257,673†† | aHR | 1.47 (1.05–2.06) | Tu ( |
| Major depressive disorder | 694/222,522 | 213/890,088 | aHR | 11.61 (9.92–13.59) | Dai ( |
| Major depressive disorder | 75/16,543 | 160/69,408 | aHR | 1.66 (1.24–2.22) | Dai ( |
| Unaffected siblings of MDD patients | 65/17,352 | 160/69,408 | aHR | 1.64 (1.27–2.12) | |
| Attention-deficit/hyperactivity disorder | 88/90,016 | 1191/1,660,440 | aHR | 1.30 (1.04–1.64) | Ho ( |
| Posttraumatic stress disorder | 24/10,967 | 30/43,868 | aHR | 4.77 (2.47–9.20) | Dai ( |
| Obsessive-compulsive disorder | 154/44,324 | 41/177,296 | aHR | 13.69 (9.38–19.98) | Chou ( |
| Infectious diseases | |||||
| hepatitis C virus infection | NR | NR | aHR | 6.69 (4.28–10.44) | Ma ( |
| Human papillomavirus infections | 57/30,001 | 144/30,001 | aHR | 2.55 (1.88–3.47) | Tu ( |
| Thyroid diseases | |||||
| Rheumatoid arthritis patients with thyroid diseases‡ | 5/1,764 | NR | aHR | 3.53 (1.38–9.05) | Chang ( |
| Thyrotoxicosis | 107/35,071 | 116/350,710 | aHR | 9.29 (7.11–12.14) | Dai ( |
| Graves’ disease | 57/19,227 | 66/192,270 | aHR | 8.66 (6.03–12.42) | |
| Thyroiditis | 13/5,460 | 20/54,600 | aHR | 6.42 (3.15–13.11) | |
| Hashimoto thyroiditis | 3/3,352 | 12/33,520 | aHR | 2.70 (0.75–9.70) | |
| Other diseases | |||||
| Migraine | 29/16,650 | 37/66,600 | aHR | 1.96 (1.15–3.32) | Dai ( |
| Polycystic ovary syndrome | 24/10,967 | 30/43,868 | aHR | 3.12 (1.81–5.40) | Chang ( |
| Combined sleep disorders | 308/93,130 | NR/372,520 | aHR | 4.70 (3.99–5.54) | Dai ( |
| Obstructive sleep apnea | 20/93,130 | NR/372,520 | aHR | 3.89 (2.46–6.16) | |
| Non-apnea insomnia | 288/93,130 | NR/372,520 | aHR | 4.77 (4.03–5.64) | |
| Irritable bowel syndrome | 116/56,429 | 86/255,716 | aHR | 5.38 (3.95–7.34) | Dai ( |
| Other risk factors | |||||
| Smoking (current smoker)§ | 42/12,964 | 106/44,275 | aHR | 1.88 (1.22–2.88) | Dai ( |
| Smoking (former smoker) | 6/2,816 | 106/44,275 | aHR | 1.61 (0.68–3.83) | |
| Alcohol (social) | 34/15,611 | 108/36,888 | aHR | 0.65 (0.43–0.98) | |
| Alcohol (regular) | 12/7,556 | 108/36,888 | aHR | 0.49 (0.26–0.93) | |
| PPI (cDDD = 31–120)¶ | 7,561‡‡ | 7,605§§ | aOR | 1.12 (1.06–1.18) | Li ( |
| PPI (cDDD = 121–365)¶ | 4,651‡‡ | 4,914§§ | aOR | 1.22 (1.15–1.29) | |
| PPI (cDDD > 365)¶ | 1,160‡‡ | 948§§ | aOR | 1.40 (1.27–1.54) | |
| Comorbidities | Cases ( | Cases ( | Relative risk estimation | Results (95% CI) | References |
|---|---|---|---|---|---|
| Chronic inflammatory dermatoses | |||||
| Atopic dermatitis | 487/12,022 | 355/48,088 | aHR | 5.47 (4.76–6.28) | Wei ( |
| Atopic dermatitis | 218/4,334 | 14654/784,158 | aOR | 2.24 (1.95–2.58)‡ | Chu ( |
| Psoriasis | 13/3,448 | 35/17,240 | aHR | 2.02 (1.06–3.83) | Chen ( |
| Psoriasis | 81/4,334 | 5184/784,158 | aOR | 2.80 (2.24–3.50)‡ | Chu ( |
| Vitiligo | 14/4,334 | 430/784,158 | aOR | 5.23 (3.06–9.00)‡ | |
| Autoimmune diseases | |||||
| Autoimmune disease | 52/3,448 | 137/17,240 | aHR | 1.86 (1.32–2.63) | Chen ( |
| Rheumatoid arthritis | 20/3,448 | 55/17,240 | aHR | 1.79 (1.07–3.00) | |
| Rheumatoid arthritis | 45/4,334 | 6329/784,158 | aOR | 1.69 (1.26–2.28)† | Chu ( |
| 1.27 (0.94–1.72)‡ | |||||
| Lupus erythematosus | 64/4,334 | 2468/784,158 | aOR | 3.95 (3.05–5.11)‡ | |
| Systemic lupus erythematosus | 10/3,448 | 10/17,240 | aHR | 5.01 (2.08–12.05) | Chen ( |
| Atopic diseases | |||||
| Asthma | 245/4,334 | 43983/784,158 | aOR | 1.24 (1.09–1.41)† | Chu ( |
| aOR | 1.07 (0.93–1.22)‡ | ||||
| Allergic rhinitis | 618/4,334 | 87064/784,158 | aOR | 1.29 (1.18–1.41)‡ | |
| Mental disorders | |||||
| Any psychiatric disease | 412/5,117 | 1246/20,468 | aOR | 1.36 (1.21–1.53) | Chu ( |
| Anxiety | 257/5,117 | 672/20,468 | aOR | 1.52 (1.30–1.78) | |
| Attention deficit disorder | 19/5,117 | 74/20,468 | aOR | 0.98 (0.59–1.63) | |
| Bipolar | 29/5,117 | 103/20,468 | aOR | 0.91 (0.58–1.43) | |
| Depression | 146/5,117 | 444/20,468 | aOR | 1.16 (0.94–1.42) | |
| Manic | 11/5,117 | 32/20,468 | aOR | 1.36 (0.66–2.83) | |
| Obsessive-compulsive disorder | 24/5,117 | 56/20,468 | aOR | 1.58 (0.96–2.60) | |
| Phobia | 12/5,117 | 33/20,468 | aOR | 1.11 (0.56–2.18) | |
| Personality disorder | 22/5,117 | 60/20,468 | aOR | 1.29 (0.78–2.13) | |
| Schizophrenia | 35/5,117 | 227/20,468 | aOR | 0.54 (0.37–0.78) | |
| MDD in AA proband | 167/2,123 | 94/9,192 | aHR | 8.22 (6.41–10.54) | Dai ( |
| MDD in AA unaffected siblings | 64/2,298 | 94/9,192 | aHR | 2.55 (1.91–3.40) | |
| Suicide Attempt | 61/10,515 | 81/105,150 | aHR | 6.28 (4.47–8.81) | Wang ( |
| Neurological diseases | |||||
| Hemorrhagic stroke | NR/3,231 | NR/16,155 | aHR | 2.18 (1.01–4.84) | Kang ( |
| Ischemic stroke | NR/3,231 | NR/16,155 | aHR | 1.58 (1.00–2.45) | |
| Unspecified stroke | NR/3231 | NR/16,155 | aHR | 2.27 (1.19–4.31) | |
| Any dementia | 32/2,534 | 83/25,340 | aHR | 3.24 (2.14–4.90) | Li ( |
| Alzheimer’s dementia | 5/2,534 | 10/25,340 | aHR | 4.34 (1.45–12.97) | |
| Vascular dementia | 4/2,534 | 14/25,340 | aHR | 2.05 (0.64–6.63) | |
| Other dementia | 23/2,534 | 59/25,340 | aHR | 3.36 (2.06–5.48) | |
| Migraine | 45/5,608 | 40/22,432 | aHR | 3.26 (2.12–5.01) | Dai ( |
| Thyroid diseases | |||||
| Hashimoto’s thyroiditis | 5/3,448 | 10/17,240 | aHR | 2.47 (0.84–7.26) | Chen ( |
| Hashimoto’s thyroiditis | 8/5,929 | 18/59,290 | aHR | 4.35 (1.88–10.04) | Dai ( |
| Toxic nodular goiter | 19/5,929 | 18/59,290 | aHR | 10.17 (5.32–19.44) | |
| Nontoxic nodular goiter | 54/5,929 | 102/59,290 | aHR | 5.23 (3.76–7.28) | |
| Hyperthyroidism | 89/5,929 | 112/59,290 | aHR | 7.96 (6.01–10.54) | |
| Graves’ disease | 47/5,929 | 57/59,290 | aHR | 8.36 (5.66–12.35) | |
| Thyroiditis | 13/5,929 | 32/59,290 | aHR | 4.04 (2.12–7.73) | |
| Cancer | |||||
| Overall cancer | 2,099/162,499 | Chen ( | |||
| Nonhematologic cancer | 1,993/162,499 | NR | SIR§ | 1.10 (1.05–1.15) | |
| Upper GI cancer | 136/162,499 | NR | SIR§ | 0.70 (0.58–0.82) | |
| Liver cancer | 192/162,499 | NR | SIR§ | 0.82 (0.71–0.94) | |
| Nonmelanoma skin cancer | 30/162,499 | NR | SIR§ | 0.59 (0.38–0.80) | |
| Female breast cancer | 395/162,499 | NR | SIR§ | 2.93 (2.64–3.22) | |
| Uterine and cervix cancer | 150/162,499 | NR | SIR§ | 0.84 (0.70–0.97) | |
| Kidney and urinary bladder cancer | 113/162,499 | NR | SIR§ | 2.95 (2.41–3.50) | |
| Hematologic cancer | 112/162,499 | NR | SIR§ | 1.19 (0.97–1.41) | |
| Lymphoma cancer | 75/162,499 | NR | SIR§ | 1.55 (1.20–1.90) | |
| Other diseases | |||||
| Obstructive Sleep Apnea | 45/5,648 | NR/22,592 | aHR | 3.80 (2.53–5.71) | Dai ( |
| Non-apnea insomnia | 438/5,648 | NR/22,592 | aHR | 4.20 (3.68–4.79) | |
| Retinal disease (Total) | 61/9,909 | 175/99,090 | aHR | 3.10 (2.26–4.26) | Ting ( |
| Retinal detachment | 13/9,909 | 33/99,090 | aHR | 3.98 (2.00–7.95) | |
| Other retinopathy | 42/9,909 | 108/99,090 | aHR | 3.24 (2.19–4.81) | |
| Retinal vascular occlusion | 11/9,909 | 44/99,090 | aHR | 2.45 (1.22–4.92) | |
| Herpes Zoster | NR | NR | aOR | 3.74 (3.28–4.27) | Chen ( |
| Irritable bowel disease | 128/5,446 | 90/21,784 | aHR | 5.20 (3.97–6.82) | Dai ( |
| Hearing loss | 33/5,002 | 75/50,020 | aHR | 4.18 (2.78–6.31) | Ma ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHair Growth and Disorders · Acne and Rosacea Treatments and Effects · Facial Rejuvenation and Surgery Techniques
Introduction
1
Alopecia areata (AA) is one of the most prevalent dermatological diseases and is characterized by autoimmune, inflammatory, nonscarring hair loss on the scalp and/or body (1), affecting individuals of all genders, ages, and races. AA can coexist with other clinical conditions such as atopic dermatitis, thyroid disease, systemic lupus erythematosus (SLE), and other autoimmune diseases (2). Additionally, the clinical manifestations of AA may remain limited to either single or multiple patches with well-defined borders (localized AA) which may progress to complete scalp hair loss (alopecia totalis) or to total body hair loss (alopecia universalis) (2–5). AA also has a substantial psychological impact on patients in terms of anxiety and depression, and patients with AA also experience a decrease in quality of life in multiple domains, including health-related, social, and emotional (2, 4, 6, 7).
Epidemiological data are crucial for evaluating the overall disease burden and helping effective disease management. Although AA is a relatively common condition, there is a paucity of robust and recent epidemiological data (8). The prevalence of AA is 1 in 1000, with a lifetime incidence of about 2% worldwide (9). One recent study found that the total number of patients with AA in Taiwan increased over the years, highlighting the growing disease burden and potential unmet needs for AA patients in Taiwan (10). Racial differences regarding the epidemiology of AA have been reported in previous studies, showing that the Asian population has a higher prevalence of AA compared to individuals with a white ethnicity (8, 11, 12). It is therefore imperative to review currently published data from Taiwan to improve our understanding of the characteristics and disease burden of patients with AA.
This systematic review was carried out to (1) assess the epidemiology data on the prevalence and incidence of AA in Taiwan based on articles published between January 2010 and June 2024, and (2) investigate the disease burden of AA in Taiwan by identifying AA risk factors and comorbidities.
Methods
2
Search strategy
2.1
Literature screening following PRISMA guidelines was initiated for articles in PubMed and Cochrane databases published between January 1st, 2010 and June 14th, 2024 to identify relevant studies on AA from Taiwan. The PRISMA checklist is provided in Supplementary Material 1. A comprehensive search string was used by combining different terms to search across both databases.
Inclusion and exclusion criteria
2.2
Included studies were defined according to the Population, Intervention, Comparator(s), Outcomes, and Study design (PICOS) strategy (Supplementary Table S1). Case reports, review articles, and in-vitro studies were excluded. Review articles were excluded since the results may include findings from non-Taiwanese populations. Publications were excluded if PICOS criteria were not matched. The search strings used for the study were summarized in Supplementary Table S2.
Two independent reviewers (Lin and Chen) were involved in a two-phase literature screening. In Phase 1, titles and abstracts were reviewed. Full-text manuscripts retained after Phase 1 were further reviewed in Phase 2. Following initial searches, publications were combined, and duplicates were removed (Figure 1). If two reviewers did not agree on inclusion, the third reviewer (Shau) was involved to reach a consensus.
Diagram of study selection.
Relevant articles on AA were screened, and studies reporting epidemiology, patient characteristics or risk factors were included. Articles in languages other than English were excluded. The validated Joanna Briggs Institute (JBI) critical appraisal checklists corresponding to the respective study designs were used by the reviewers to assess quality, and consensus was reached on the risk-of-bias rating. Detailed information is summarized in Supplementary Table S3.
The following information was extracted from the included articles: reference details, type of study, study period, number of cases, sample size, sex distribution, diagnosis criteria, severity classification criteria, mean/median age, age of onset, severity, prevalence/incidence, comorbidities, and risk factors.
Results
3
Search results
3.1
A total of 67 publications were identified (64 from PubMed and 3 from Cochrane). After applying the inclusion and exclusion criteria during the two-phase review, 37 studies were included for full-text review (Figure 1). Studies included in the review demonstrated acceptable methodological quality (Supplementary Table S3). All studies were considered to have a low (31 studies, 83.8%) to moderate (6 studies, 16.2%) risk of bias. Although many of the cohort studies lacked information on completion of follow-up (i.e., Q9 and Q10 of the JBI checklist), bias was considered minimal given the nature of the data source (i.e., NHIRD), as approximately 99% of the population was covered by Taiwan’s National Health Insurance system and had longitudinal follow-up until death or the end of the data period.
Publications were further classified into four categories: four publications reported the epidemiology, patient characteristics and/or treatment patterns of AA in Taiwan; 17 studies assessed the risk factors for developing AA; 10 studies investigated the comorbidities of patients with AA in Taiwan; and six studies performed a bi-directional analysis, which investigated both AA risk factors and comorbidities of AA in one study. (Table 1).
Among the 37 included publications, the National Health Insurance Research Database (NHIRD) was the most commonly used data source (n = 33). NHIRD is a claims database which covers 99% of the population in Taiwan.
Incidence and prevalence of AA in Taiwan
3.2
In the latest study using the full-population NHIRD in Taiwan, the total number of patients with AA in Taiwan increased from 3,221 in 2016 to 3,855 in 2020 (with a prevalence of 0.14–0.16 per 1,000), with about 8% of patients having severe AA and most were newly diagnosed. During 2017–2020, there was an average of 2,659 incident patients with AA in Taiwan annually, with a crude incidence rate of about 0.11 per 1,000 (10). In earlier studies using the data from 1997 to 2011, the estimated prevalence were ranged from 4.1 to 7.1 per 1,000 and the estimated incidence rate were 0.36–1.01 per 1,000 (13–19).
Characteristics of patients with AA in Taiwan
3.3
A summary of studies that identified AA cohorts is presented in Table 2. In the study cohort identified from the NHIRD before 2013, the mean age of initial AA diagnosis was around 32 years, and the proportion of male patients was around 50% (13, 15–17, 19–23). In a recent cohort (2017–2018) identified by Tsai et al. (10), the mean age of patients with AA was 41.2 years, with a slight male predominance (male: 53.4%; female: 46.6%). In contrast, there was a female predominance in cohorts with older age: 67% of patients were female in a late-onset AA cohort (patients with first onset of AA at 50 years or above) (24). A similar distribution was found in an AA cohort aged 45 years or above (25).
The heritability of AA has also been observed in the Taiwanese population. A study using the Taiwan Maternal and Child Health Database found that children of parents with AA have twice the risk of developing AA compared to offspring of parents who did not have the condition (26).
Treatment patterns of AA in Taiwan
3.4
Topical corticosteroids were the most common treatment for patients with AA (80% of patients) (10). The treatment patterns varied depending on disease severity, with 48.5 and 12.0% of patients with severe AA receiving systemic glucocorticoids and immunosuppressants, respectively, compared to only 15.7 and 0.7% of patients with mild or moderate AA (10). Traditional Chinese Medicine (TCM) was noted as a potential treatment option in patient with AA. A study assessing the psoriasis treatment patterns found that patients with psoriasis preferred to visit TCM practitioners when they had several comorbidities, including AA (adjusted prevalence rate ratio: 1.36 [95% confidence interval (CI): 1.06–1.75]) (27).
Risk factors for developing AA in the Taiwanese population (Table 3)
3.5
Sixteen studies assessed diseases which could be associated with a higher risk of developing AA. Autoimmune/atopic diseases and psychiatric disorders were the two major disease areas studied.
Patients with chronic inflammatory dermatoses, such as atopic dermatitis (19), psoriasis (28, 29), lichen planus (30), and vitiligo (31) were found to be associated with a higher risk of developing AA. Rheumatoid arthritis also increased the risk of AA (32), but not ankylosing spondylitis. (33)
The association between mental disorders and the risk of AA was also widely investigated. Patients with mental disorders, including major depressive disorder (MDD) (34, 35), attention-deficit/hyperactivity disorder (ADHD) (36), posttraumatic stress disorder (37), and obsessive-compulsive disorder (38) were found to have an increased risk of AA. The study by Dai et al. (35) further investigated the relationship between MDD family history and AA by linking the NHIRD data and birth certificates. The results showed that both MDD probands and their unaffected siblings had a higher risk of AA compared to the control group.
Other identified risk factors for AA include viral infections (Hepatitis C virus and Human papillomavirus) (29, 39), irritable bowel syndrome (21), sleep disorders (22), thyroid disorders (including thyrotoxicosis, Graves’ disease, and thyroiditis) (20, 32), migraine (23), and polycystic ovary syndrome (40).
The association between lifestyle habits or medication use and the risk of AA was studied in the Taiwanese population. Smokers (current of former) were found to have a higher risk of developing AA from a study using National Health Interview Survey database (conducted in 2001, 2005, 2009, and 2013) and the NHIRD (41). Exposure to proton pump inhibitors was found to increase the risk of AA. Compared to a cumulative defined daily dose (cDDD) ≤ 30, patients with a higher cDDD had a higher risk of AA, and a dose-dependent trend was also observed (42). In addition, among patients with ADHD, the use of methylphenidate did not increase the risk of AA compared to patients not using methylphenidate (36).
Risk factors for coronavirus disease 2019 (COVID-19) vaccine-related AA were investigated using Taiwan/China Severe Cutaneous Adverse Reaction consortium data, with 27 cases of COVID-19 vaccine-related AA and 106 vaccine-tolerant controls included. Underlying chronic urticaria and nail dystrophy were found to be associated with COVID-19 vaccine-related AA. Additionally, laboratory findings such as increased antinuclear antibody level, total IgE level, and eosinophil count were also risk factors for developing COVID-19 vaccine-related AA (43).
AA-related comorbidities in the Taiwanese population
3.6
Studies investigating AA-related comorbidities are summarized in Table 4. Tsai et al. (10) identified a study cohort of 6,016 patients with AA in Taiwan during 2017–2018, with 477 cases of severe AA and 5,539 cases of mild/moderate AA. Baseline comorbidities of AA (i.e., at first diagnosis of AA) were analyzed. Allergic rhinitis (6.13%) and allergic conjunctivitis (3.21%) were the two major coexisting atopic conditions at baseline. Within conditions included in the Charlson Comorbidities Index, diabetes (with or without complications, 4.54%), peptic ulcer (3.27%), and mild liver disease (3.27%) were the three main comorbidities at baseline. The prevalence of comorbidities was similar between patients with severe or mild/moderate AA except for allergic urticaria (2.31% in severe AA and 0.54% in mild/moderate AA).
Similar to studies on risk factors of AA, publications investigating the association between comorbidities and AA mainly focused on chronic inflammatory dermatoses, atopic diseases, autoimmune diseases, and mental disorders. AA was associated with an increased risk of atopic dermatitis, allergic rhinitis, psoriasis, vitiligo, rheumatoid arthritis, and lupus erythematosus (14, 15, 19). However, the risk of asthma in patients with AA was not significantly different from that of patients without AA after adjusting for age, sex, and other comorbid diseases (15). Patients with AA were also found to have an increased risk of mental disorders and neurological diseases. The risk of any psychiatric diseases, anxiety, schizophrenia (16), major depression disorder (35), dementia, and stroke (including hemorrhagic and ischemic stroke) (17) was significantly higher in patients with AA than in the control group.
The risk of cancer in patients with AA was also assessed in several studies. The overall cancer risk in patients with AA was slightly lower, but there was a slightly higher incidence ratio of certain types of cancer in patients with AA compared to the control group (13). The risk of female breast cancer, kidney and urinary bladder cancer, and lymphoma were elevated in patients with AA, while the risk of nonmelanoma skin cancer, upper GI cancer, liver cancer, and uterine and cervix cancer were lower in patients with AA than in the general population (13).
In addition, patients with AA were also associated with the increased risk of having sensorineural hearing loss (18) and retinal detachment (44).
Discussion
4
To the best of our knowledge, this is the first systematic literature review study on AA epidemiology and disease burden in Taiwan. By reviewing 37 articles, we summarized the epidemiology of AA in Taiwan, risk factors for developing AA, and AA-related comorbidities. In addition, demographics of patients with AA in Taiwan could be understood through the analysis of newly diagnosed AA cohorts reported in studies.
Although the modelling study by Jeon et al. (45) reported that the prevalence estimates tend to be higher in Asian regions, the estimated annual incidence rate and prevalence of AA in Taiwan reported in the latest study (estimated by total population in each year in Taiwan during 2017–2020) were 0.011 and 0.015%, respectively (10), which are lower than data reported in other countries. For instance, the estimated global incidence of AA varies between 0.1 and 3.8%, and the prevalence of AA is 0.1% (9, 45–47). In other Asian countries, the incidence rate in South Korea was 0.2%; and the prevalence ranged from 0.16 to 0.19% in Japan and 0.37% in South Korea (46, 48). A UK study showed a threefold higher AA incidence in people of Asian origin compared to those of white ethnicity (8). The geographic region, social factors, lifestyle and could cause differences in prevalence and incidence rate of AA (45). In addition to these factors, the lower incidence and prevalence of AA in Taiwan might be due to stricter case definition used in the study by Tsai et al. (i.e., ≥3 claims with AA diagnosis by dermatologists or rheumatologists) compared to other studies that used a one-time diagnosis as the inclusion criterion (46, 48); AA patients without persistent medical consultation or treatment could therefore not be captured in the study. Moreover, although the ICD codes used for AA were inconsistent with the codes used in other studies (48, 49), underestimation of the number of patients with AA might exist: for example, a US study also included ICD-9-CM: 704.09 (Other alopecia) to define AA (50), and clinicians might code it with other hair loss disorders.
Chronic inflammatory dermatoses, autoimmune diseases, atopic diseases, and psychiatric diseases were major disease categories when assessing the disease burden of AA in Taiwan, as summarized in Tables 3, 4. We observed that Taiwanese patients with AA showed various systemic and psychiatric comorbidities. This observation aligns with findings from other countries, including Korea, UK, and the US (51–55).
The activation of T helper cell (Th) 2, Th1, Th17 and Th9 cytokines play a vital role in the disease pathogenesis of AA. Since AA shares overlapping immune-mediated and inflammatory pathways with other autoimmune and atopic disorders, such as mediation of T-cells or activation of cytokines (54, 56–58), autoimmune diseases were one of the comorbidities that had the strongest association with AA (54). Consistent with findings in Taiwan, observational studies from the UK reported an increased risk of autoimmune conditions among patients with AA (adjusted HR for combined autoimmune conditions: 1.45 [95% CI: 1.28–1.66] (51). Furthermore, a meta-analysis encompassing 102 studies and including 680,823 patients with AA and 72,011,041 controls demonstrated a significant association between AA and autoimmune diseases (meta-analyzed odds ratio 2.28 [95% CI 1.75–2.97]) (54). In contrast to other autoimmune diseases, a meta-analysis and an observational study reported that ankylosing spondylitis had no association with AA (33, 54) and concluded that no direct association between AA and ankylosing spondylitis can be made (33).
Stressful phenomena may lead to hair loss through immune dysregulation and may trigger the functional equivalent of the hypothalamic–pituitary–adrenal axis in hair follicles, resulting in neurogenic inflammation and inducing premature destruction of the follicle (55, 59–61). Consistent with the study by Chu et al. (16), Okhovat et al. (55) reported that the combined odds ratios of anxiety and depression were 2.5 (95% CI: 1.54–4.06) and 2.71 (95% CI: 1.52–4.82), respectively, in a meta-analysis. Moreover, studies in Taiwan found that patients with AA had a higher risk of developing mental disorders such as bipolar and manic disorders, while attention-deficit/hyperactivity disorder, post-traumatic stress disorder, and obsessive-compulsive disorder were risk factors for developing AA. Bi-directional associations between MDD and AA were both reported by Dai et al. (35) in a Taiwanese population and by Vallerand et al. in the United Kingdom (62).
In addition to autoimmune and psychiatric diseases, ocular disorders (fundus changes, disorders of the sclera, lens changes, inflammation of the eyelid, iridocyclitis, keratitis, lacrimal system disorders, disorders of the choroid or retina and dry eye disorder) were found to have a strong association with AA in previous studies (44, 63, 64). Several hypotheses have been proposed to support the underlying mechanisms linking AA and ocular involvement. T-cell-mediated autoimmune condition may play a major role in the pathogenesis of AA and ocular disease. One key feature of AA pathogenesis is the collapse of hair follicle immune privilege, which normally protects follicular structures from autoimmune attack. Similarly, the anterior chamber of the eye maintains an immune-privileged environment to prevent inflammatory damage. Disruption of this ocular immune privilege may trigger local immune responses, contributing to ocular pathology in patients with AA (64, 65). Based on the studies review, only retinal disease has studied in Taiwan by using claims data. Further research should explore a border range of ocular diseases, ideally the data sources contains results on clinical examinations (e.g., complete ophthalmologic examination involving detailed anterior segment and fundus examination) to better elucidate potential etiological mechanisms.
We identified key evidence gaps on AA in Taiwan. First, comprehensive epidemiology data on AA in Taiwan was limited, and validation of AA diagnosis in NHIRD is required. Even though AA cohorts were identified in 12 studies, as listed in Table 2, the heterogeneity of AA diagnostic algorithms makes the results from different studies, especially epidemiological data, difficult to compare. The AA cohorts were identified using the national claims in two different data periods: before 2015 (inclusive, ICD-9-CM era) and after 2016 (inclusive, ICD-10-CM era). Inconsistencies were found in several conditions (66), which highlights that the comparison between studies from two different periods should be discussed with caution. Given the published epidemiological data on AA in Taiwan differ from those reported in other countries, future research should focus on developing and validating the algorithm for defining AA cases in real-world data sources to ensure the accuracy and consistency.
Accurate diagnosis and grading of AA severity are essential for assessing the true disease burden (67, 68). However, only two of the included studies reported disease severity. Wu et al. (24) classified the severity of the AA as S1-S4 based on the guidelines from National Alopecia Areata Foundation. Although NHIRD lacks clinical information, the algorithm proposed by Tsai et al. could be a potential approach to identify moderate-to-severe AA by the presence of advanced treatment (immunosuppressants, topical immunotherapy treatment, topical intralesional injectable steroids, or phototherapy) (28). Further validation studies on the algorithm should be taken by linking the NHIRD to data sources with clinical information.
The studies included in this review shared similar potential biases, and the causality of comorbidities and risk factors could not be confirmed. To elaborate, 33 out of 37 included studies were from the same database (NHIRD), which shares the same limitations. Most epidemiologic and comorbidity analyses were based on overlapping time windows within the same national claims population, meaning these findings do not represent independent cohorts. Beyond autoimmune/atopic and mental disorders, many of the comorbidities/risk factors were reported in a single study. Therefore, randomized controlled studies are required to confirm the causality, and patient-reported outcomes can be assessed to address the burden on patients’ quality of life.
Lastly, several comorbidities have been reported to be associated with AA; however, they have not been well studied in the Taiwanese population. For example, a meta-analysis by Ly et al. (54) reported that patients with AA have a higher risk of developing cardiovascular diseases (pooled odds ratio: 1.31 [95% CI: 1.05–1.63]), particularly coronary artery disease and dyslipidemia. These findings highlight potential directions for future research.
Even though the review followed PRISMA guidelines and used both the term “alopecia areata” and its corresponding MeSH term to capture relevant studies, there remains a potential limitation: some studies indexed under broader hair-loss terms or alternative diagnostic wording may not have been captured. In summary, the current systematic literature review suggests that AA has an overall impact on patients further than an aesthetic concern, causing a significant disease burden and emphasizing the need for effective treatments and the importance of increasing disease awareness. This study also identified key evidence gaps in Taiwan, highlighting the directions for future research, including the need for developing a unified algorithm to define AA and the severity classification in real-world data sources, as well as to have research to investigate other risk factors and comorbidities with AA. Furthermore, with the publication of a local consensus (68) and the introduction of novel treatment options, disease awareness and diagnosis rates are expected to increase, leading to a more comprehensive understanding of AA epidemiology and disease burden worldwide, ultimately improving patient care and treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Juárez-Rendón KJ Rivera Sánchez G Reyes-López M García-Ortiz JE Bocanegra-García V Guardiola-Avila I . Alopecia areata. Current situation and perspectives. Arch Argent Pediatr. (2017) 115:e 404–11. doi: 10.5546/aap.2017.eng.e 404, 29087123 · doi ↗ · pubmed ↗
- 2Chanprapaph K Mahasaksiri T Kositkuljorn C Leerunyakul K Suchonwanit P. Prevalence and risk factors associated with the occurrence of autoimmune diseases in patients with alopecia areata. J Inflamm Res. (2021) 14:4881–91. doi: 10.2147/JIR.S 331579, 34588794 PMC 8473714 · doi ↗ · pubmed ↗
- 3Barton VR Toussi A Awasthi S Kiuru M. Treatment of pediatric alopecia areata: a systematic review. J Am Acad Dermatol. (2022) 86:1318–34. doi: 10.1016/j.jaad.2021.04.077, 33940103 PMC 8556406 · doi ↗ · pubmed ↗
- 4Fukumoto T Fukumoto R Magno E Oka M Nishigori C Horita N. Treatments for alopecia areata: a systematic review and network meta-analysis. Dermatol Ther. (2021) 34:e 14916. doi: 10.1111/dth.1491633631058 · doi ↗ · pubmed ↗
- 5Lai VWY Chen G Gin D Sinclair R. Systemic treatments for alopecia areata: a systematic review. Australas J Dermatol. (2019) 60:e 1–e 13. doi: 10.1111/ajd.12913, 30191561 · doi ↗ · pubmed ↗
- 6Abedini R Hallaji Z Lajevardi V Nasimi M Karimi Khaledi M Tohidinik HR. Quality of life in mild and severe alopecia areata patients. Int J Womens Dermatol. (2018) 4:91–4. doi: 10.1016/j.ijwd.2017.07.001, 29872683 PMC 5986230 · doi ↗ · pubmed ↗
- 7Mostaghimi A Napatalung L Sikirica V Winnette R Xenakis J Zwillich SH . Patient perspectives of the social, emotional and functional impact of alopecia areata: a systematic literature review. Dermatol Ther (Heidelb). (2021) 11:867–83. doi: 10.1007/s 13555-021-00512-0, 33770385 PMC 8163950 · doi ↗ · pubmed ↗
- 8Harries M Macbeth AE Holmes S Chiu WS Gallardo WR Nijher M . The epidemiology of alopecia areata: a population-based cohort study in UK primary care. Br J Dermatol. (2022) 186:257–65. doi: 10.1111/bjd.20628, 34227101 PMC 9298423 · doi ↗ · pubmed ↗