Atrial Flow Regulator: Bridging Pediatric Patients With Pulmonary Arterial Hypertension to Lung Transplantation
Julia Moosmann, Anastasia Schleiger, Felix Berger, Peter Kramer

TL;DR
A new device called an atrial flow regulator helps stabilize pediatric patients with severe pulmonary hypertension before lung transplantation, improving outcomes and allowing for safer surgery.
Contribution
The study demonstrates the effectiveness of atrial flow regulators as a bridging strategy for pediatric PAH patients awaiting lung transplantation.
Findings
AFR implantation stabilized two pediatric patients with severe PAH, enabling successful listing for lung transplantation.
Post-transplant percutaneous closure of the AFR fenestration minimized long-term complications.
AFR use allowed for complete cardiac remodeling in both patients after lung transplantation.
Abstract
Pulmonary arterial hypertension (PAH) in pediatric patients remains challenging, particularly in symptomatic patients with right heart failure despite optimal medical therapy. The use of an atrial flow regulator (AFR) to decompress the right ventricle has offered a new therapeutic approach for those patients and allows bridging for lung transplantation (LTX). Data on pretransplant decision-making, perioperative considerations, and post-transplant management in pediatric patients undergoing LTX are limited. We report 2 pediatric patients with severe symptomatic PAH and right heart failure in whom an AFR was implanted before LTX. In both patients, AFR implantation resulted in clinical stabilization, allowing for successful listing and subsequent LTX. After LTX, both patients showed complete cardiac remodeling, and the AFR fenestration was closed percutaneously to minimize long-term…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
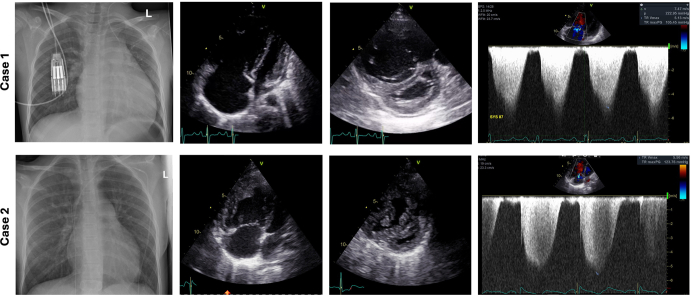 Figure 1
Figure 1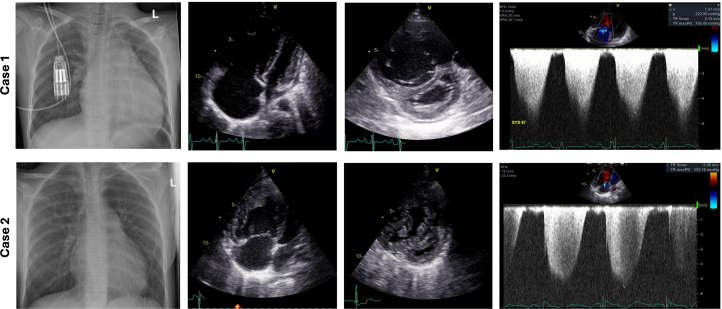 Figure 2
Figure 2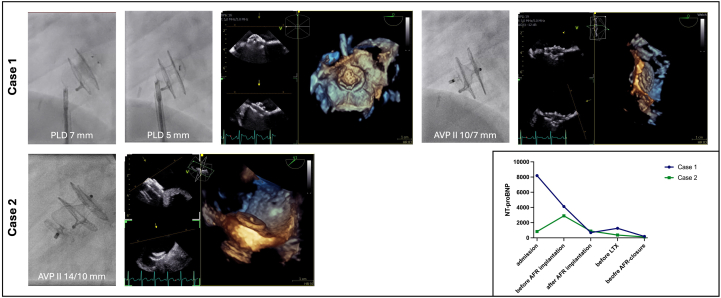 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiovascular and Diving-Related Complications · Cardiac Arrhythmias and Treatments
The atrial flow regulator (AFR, Occlutech) is a self-expandable percutaneously delivered double-disk device with a central fenestration, designed to create an interatrial shunt. This device was initially approved for adult patients with heart failure and reduced ejection fraction. In the pediatric population, its use has been successfully described in patients with congenital heart disease, including failing Fontan patients to create a right-to-left shunt, or in patients with cardiomyopathy and in patients with therapy-resistant pulmonary arterial hypertension (PAH).1^,^2 Clinical improvement or stabilization can be achieved after AFR implantation in patients with PAH by decompressing the right ventricle (RV), improving cardiac output and therefore end-organ function.3^,^4 In patients with RV failure refractory to optimal medical therapy, implantation of an AFR may serve as a feasible bridging strategy to lung transplantation (LTX).5 This report presents 2 pediatric cases of AFR implantation before LTX, focusing on pretransplant management, perioperative considerations, and post-transplant outcomes.Take-Home Message
- •In patients with severe PAH, atrial flow regulator implantation improves clinical symptoms and optimizes transplant candidacy, allowing for a safer bridge to lung transplantation.
Case 1
A 9-year-old girl was diagnosed with PAH, prompted by the patient's reports of new-onset chest pain during exercise and multiple syncopal episodes during exertion.
The patient had a medical history of symptomatic focal epilepsy, diagnosed in early infancy, and showed mild facial dysmorphism. Previous genetic testing identified a variant in the KCNQ2 gene (c.2068G>A; p.Val690Met), which is associated with early infantile epileptic encephalopathy and is not known to cause PAH. Under antiepileptic therapy, the patient had remained free of seizures and had developed appropriately for her age.
After initial stabilization and confirmation of pulmonary vasoreactivity, the patient was initiated on bosentan, sildenafil, and selexipag. Despite medical therapy, her clinical symptoms persisted, and she required readmission because of fulminant right heart failure in the setting of suprasystemic RV pressure. Echocardiography revealed a structurally normal heart with severe RV failure. The right atrium (RA) and RV were severely dilated. There was moderate tricuspid regurgitation (TR), septal flattening, and suprasystemic RV pressure (Figure 1).Figure 1. Imaging Findings in Patients With Pulmonary Arterial HypertensionRadiographic and echocardiographic imaging for (Top Row) case 1 and (Bottom Row) case 2. Both patients showed cardiomegaly and prominent PA segment, RA and RV dilatation, septal flattening, and suprasystemic RV pressure. PA = pulmonary artery; RA = right atrial; RV = right ventricular.
Clinically, the patient was in reduced general condition and required admission to the pediatric intensive care unit for central line insertion under inotropic support and standby extracorporeal membrane oxygenation (ECMO). The medical treatment was changed to macitentan, sildenafil, and intravenous epoprostenol. Two days after admission, trans-septal puncture followed by implantation of an 8-mm AFR device was performed to decompress the right heart structures. The patient subsequently stabilized and was transferred to the general ward. No further syncopal events occurred, and N-terminal pro–B-type natriuretic peptide (NT-proBNP) levels normalized after AFR implantation (see graph in Figure 2).Figure 2. Closure of the Atrial Flow RegulatorFluoroscopic images and simultaneous 2D and 3D transesophageal echocardiography demonstrate (Top Row) attempted closure with paravalvular leak devices and final closure with the AVPII in case 1 and (Bottom Row) closure with the AVPII in case 2. (Bottom Right) Graph showing NT-proBNP levels at different time points: admission, before and after AFR implantation, before lung transplantation, and before AFR closure. 2D = two-dimensional; 3D = three-dimensional; AFR = atrial flow regulator; AVPII = Amplatzer vascular plug II; LTX = lung transplantation; NT-proBNP = N-terminal pro–B-type natriuretic peptide; PLD = paravalvular leak device.
Owing to an increased gradient across the AFR device as detected on transthoracic echocardiography, the patient underwent an additional cardiac catheterization 1 month after initial implantation. The gradient was successfully reduced by balloon dilatation using an ultra-high-pressure balloon (Conquest).
The patient was subsequently listed for LTX and successfully underwent bilateral LTX 1 month after admission. After LTX and remodeling of the RV, she showed normal mean pulmonary artery and RV pressure and an isolated left-to-right shunt across the AFR. The patient is currently 26 months post-LTX in good condition.
Case 2
A 12-year-old girl presented to the emergency department with an upper airway infection and progressive decline in exercise capacity. She was a refugee and was diagnosed with PAH abroad during an episode of pneumonia 6 months before. She was started on oral pulmonary vasodilator treatment with sildenafil, macitentan, selexipag, and iloprost inhalation. She had experienced worsening of her symptoms in the previous month, including several syncopal events.
Echocardiography revealed a marked dilatation of the RV and RA, with suprasystemic RV pressures and moderate reduced RV systolic function. Moderate TR, interventricular septal flattening, and severe pulmonary artery dilatation was also shown (Figure 1). Genetic testing revealed a rare missense variant c.212C>A(p.Pro71Gln), which is regarded as likely pathogenic in the context of PAH.
The patient was admitted and initiated on intravenous epoprostenol therapy. After successful stabilization on epoprostenol, a permanent pump system was implanted 1 month after initial presentation. However, she showed insufficient clinical improvement and progressively deteriorated, presenting with recurrent chest pain, elevated NT-proBNP levels (see graph in Figure 2), and sinus tachycardia. Given the lack of response, the decision was made to create an atrial communication and implant an 8-mm AFR. After successful AFR implantation, the patient stabilized and was listed for LTX. NT-proBNP levels dropped within days after AFR implantation and normalized in the following months. No further syncopal events occurred.
After a 9 months on the transplant list, the patient underwent bilateral LTX, complicated by pneumonia and oxygenation issues requiring postoperative ECMO. Six months after LTX, the patient developed post-transplant lymphoproliferative disorder with B-cell lymphoma, which was successfully treated with rituximab. The patient is currently 14 months post-LTX in clinically stable condition.
Interventional Aspects of the AFR
AFR implantation
Case 1 underwent AFR implantation in our hybrid suite with ECMO on standby, whereas case 2 was treated in our standard catheterization laboratory. This decision was based on the individual clinical stability of each patient. Both procedures were performed under transesophageal echocardiography guidance and fluoroscopy. Trans-septal puncture was achieved using radiofrequency ablation, followed by ballon dilatation of the atrial septum with 8- and 10-mm Conquest balloons to create an atrial communication. Both patients immediately showed bidirectional shunting across the defect. Subsequently, an AFR device (5 and 8 mm) was successfully implanted in both patients without complications. Both patients showed a decrease in their oxygen saturation after implantation (Table 1). The AFR device was well seated in the interatrial septum, without obstructing surrounding structures (see, eg, case 1 in Video 1).Table 1. Overview of Clinical and Interventional Parameters Associated With Perioperative ManagementCase 1Case 2Age (y)912Weight (kg)3133Genetic findingKCNQ2 gene (c.2068G>A; p.Val690Met)SOX17 gene c.212C>A (p.Pro71Gln)Waiting time to LTX (mo)19Medical therapySildenafil, macitentan, epoprostenol i.v., nasal oxygen (2 L/min), milrinoneSildenafil, macitentan, epoprostenol i.v. (pump), nasal oxygen (2 L/min)AFR implantation after hospital admission (d)176Fluoroscopy time (min)3.65AFR size8/58/5Hemodynamics at AFR implantation (mm Hg) RA pressure175 LA pressure14— RA pressure with AFR143Gradient across AFR on TEE (mm Hg)23Saturation before AFR implantation (%)97-9996-98Saturation after AFR implantation (%)88-9391-93Reinterventions before LTXBalloon dilatation of AFR (Conquest balloon)Diagnostic cardiac catheterizationDays in ICU after LTX (d)841Total hospital stay after LTX (d)7678ComplicationsPostoperative bleeding requiring rethoracotomyPostoperative ECMO (4 d), tracheostomy (28 d), sepsis, PTLD 6 mo after LTXAFR closure after LTX (mo)410Device used for AFR closureAVPII 10 × 7 mmAVPII 14 × 10 mmFluoroscopy time (min)167.4Hemodynamics at closure RA pressure46 LA pressure612 RVSP30— Mean PA pressure18— Wedge pressure7— LVEDP513 LVSP140110AFR = atrial flow regulator; AVPII = Amplatzer vascular plug II; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; i.v. = intravenous; LA = left atrium; LTX = lung transplantation; LVEDP = left ventricular end-diastolic pressure; LVSP = left ventricular systolic pressure; PA = pulmonary artery; PTLD = post-transplant lymphoproliferative disorder; RA = right atrium; RVSP = right ventricular systolic pressure; TEE = transesophageal echocardiography.
After the procedure, case 1 continued on intravenous heparin given the need for a permanent intravenous line for intravenous epoprostenol administration, and case 2 was transitioned to oral antiplatelet therapy with aspirin.
AFR closure
Because of the presence of an interatrial shunt, antiplatelet therapy with aspirin was continued after LTX in both patients. However, considering the anticipated need for follow-up bronchoscopies and risk of associated bleeding, as well as the long-term risk for paradoxical embolism, the decision was made to close the AFR in both patients after LTX. Both patients showed marked cardiac remodeling, with normal RV size and function, trivial TR, normal RV pressure, and an isolated left-to-right shunt across the AFR.
In case 1, closure was performed 4 months after LTX. Initial attempts to close the device with the rectangular paravalvular leak device (Occlutech) at both 7 and 5 mm were not successful. The paravalvular leak devices were recommended because of their shape and their supposed ability to perfectly exclude the eccentric ball-connector of the AFR. However, both device configurations were too bulky, particularly the left atrial disk, and they were not released owing to concerns of left-sided thrombus formation (Figure 2). Eventually, the fenestration was closed with a 10-mm Amplatzer vascular plug II (AVPII; Abbott), showing a flat configuration in the left atrium and no residual shunt across the fenestration (Figure 2).
In case 2, the AFR was closed 10 months after LTX. The delayed closure compared with case 1 was attributed to her significant complications after transplantation. The atrial fenestration was closed with a 14-mm AVPII, which conformed nicely in the left atrium but appeared slightly bulkier within the RA owing to the its length (Figure 2). In both patients, the AVPII demonstrated a flawless, left-sided flat configuration at the site of the AFR, eliminating any residual shunting. The AVPII 10 × 7 mm size configured particularly well to achieve full closure, while the larger device was slightly bulkier on the RA side. Both procedures were performed under conscious sedation, with three-dimensional transesophageal echocardiography guidance and fluoroscopy. Antiplatelet therapy with aspirin was continued for another 6 months to ensure complete endothelialization of the device.
Discussion
The AFR device has been successfully used in pediatric patients with PAH.1^,^3 Our cases demonstrate the effective use of AFR as a bridging strategy to LTX and the closure of the AFR after cardiac remodeling post-LTX.
In both of our patients, AFR implantation resulted in significant clinical improvement and most likely contributed to improved transplant candidacy. This was reflected by no further syncopal events and normalized NT-proBNP (Figure 2, graph). No device-related complications occurred during LTX. We hypothesize that the AFR implantation may also facilitate RV and left ventricular remodeling in the postoperative period. In these patients, the left ventricle is often chronically “deconditioned,” exhibiting diastolic dysfunction as a consequence of longstanding low cardiac output secondary to high pulmonary vascular resistance and reduced preload.6 The AFR might be beneficial in the postoperative phase to unload the left ventricle and enable a more gradual adaption to the increased preload during postoperative recovery.
In contrast to adult patients, where a residual atrial communication post-LTX may be of limited clinical relevance, it may warrant closure in pediatric patients, who have a comparably longer life expectancy. Therefore, closure of the AFR after successful LTX seems reasonable in this patient population. Furthermore, anticoagulation can typically be discontinued at 6 months after device closure, potentially improving long-term medical compliance by reducing daily medication burden.
After LTX, we observed complete remodeling of ventricular function, pressures, and ventricular volumes. This normalization of hemodynamics resulted in shunt reversal to a left-to-right shunt. In cases where atrial fenestration is no longer necessary, closure can be effectively achieved using an AVPII.
Conclusions
The use of AFR represents a valuable therapeutic option in pediatric patients with PAH and RV failure as a bridging strategy to LTX. The achieved clinical stabilization enables safer perioperative management and improved transplant candidacy. Our cases illustrate that the AFR device can be safely managed throughout the transplantation process and closed effectively using an AVPII postoperatively to minimize long-term risks of an atrial shunt.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Butera G.Piccinelli E.Kolesnik A.Implantation of atrial flow regulator devices in patients with congenital heart disease and children with severe pulmonary hypertension or cardiomyopathy-an international multicenter case series Front Cardiovasc Med 102023133239510.3389/fcvm.2023.1332395 PMC 1082298038288053 · doi ↗ · pubmed ↗
- 2Piccinelli E.Testa A.Butera G.Versatility of atrial flow regulator device in congenital heart disease: a case series Pediatr Cardiol 4562024137713833679512110.1007/s 00246-023-03123-y · doi ↗ · pubmed ↗
- 3Sivakumar K.Rohitraj G.R.Rajendran M.Study of the effect of occlutech atrial flow regulator on symptoms, hemodynamics, and echocardiographic parameters in advanced pulmonary arterial hypertension Pulm Circ 1112021204589402198996610.1177/2045894021989966 PMC 786917933614019 · doi ↗ · pubmed ↗
- 4Aregullin E.O.Samuel B.P.Girgis R.Emergency use of occlutech® atrial flow regulator device facilitates weaning from veno-arterial extracorporeal membrane oxygenation in a patient with severe pulmonary arterial hypertension J Intensive Care Med 36620217267283385340210.1177/08850666211007809 · doi ↗ · pubmed ↗
- 5Aregullin O.E.Girgis R.E.Krishnan S.Atrial flow regulators for the treatment of pulmonary arterial hypertension: what does the future hold?Expert Rev Med Devices 211020248898913936461610.1080/17434440.2024.2409769 · doi ↗ · pubmed ↗
- 6Tudorache I.Sommer W.Kühn C.Lung transplantation for severe pulmonary hypertension--awake extracorporeal membrane oxygenation for postoperative left ventricular remodelling Transplantation 99220154514582511912810.1097/TP.0000000000000348 · doi ↗ · pubmed ↗