Capacity building for healthcare workers on preventing and managing female genital mutilation: Impact on knowledge, attitudes, skills, and quality of care—A systematic review
Chioma Oringanje, Sidney Oparah, Christina C. Pallitto, Anthony Okoro, Mavis Otonkue, Faithman Ovat, Ogonna Nwankwo, Martin Meremikwu

TL;DR
Training healthcare workers on FGM, along with resources like job aids, improves their knowledge, skills, and care for women affected by FGM.
Contribution
This study is the first systematic review to assess the impact of training and capacity-building resources on healthcare workers' FGM-related knowledge and care.
Findings
Training plus IEC materials significantly improved knowledge and care practices compared to IEC materials alone.
Point-of-care flip charts helped providers communicate more effectively with clients.
Observational studies showed similar trends but with very low-quality evidence.
Abstract
Despite declining prevalence in some regions, female genital mutilation (FGM) remains a major public health issue, causing both immediate and long‐term health complications. The objective of this present study was to determine the effect of training healthcare workers, providing access to resources for capacity‐building, such as job aids, and its impact on knowledge, skills, and attitudes toward FGM and the quality of healthcare service delivery. The following major databases were searched from inception to May 2023: CINAHL Plus, IRIS, MEDLINE, PsycINFO, SCOPUS, and Web of Science, without language restrictions. Controlled studies based on predefined objectives. Studies were independently assessed for eligibility and risk of bias. Data were extracted for meta‐analyses and the evidence assessed using the GRADE approach. Eight studies, including one cluster randomized controlled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
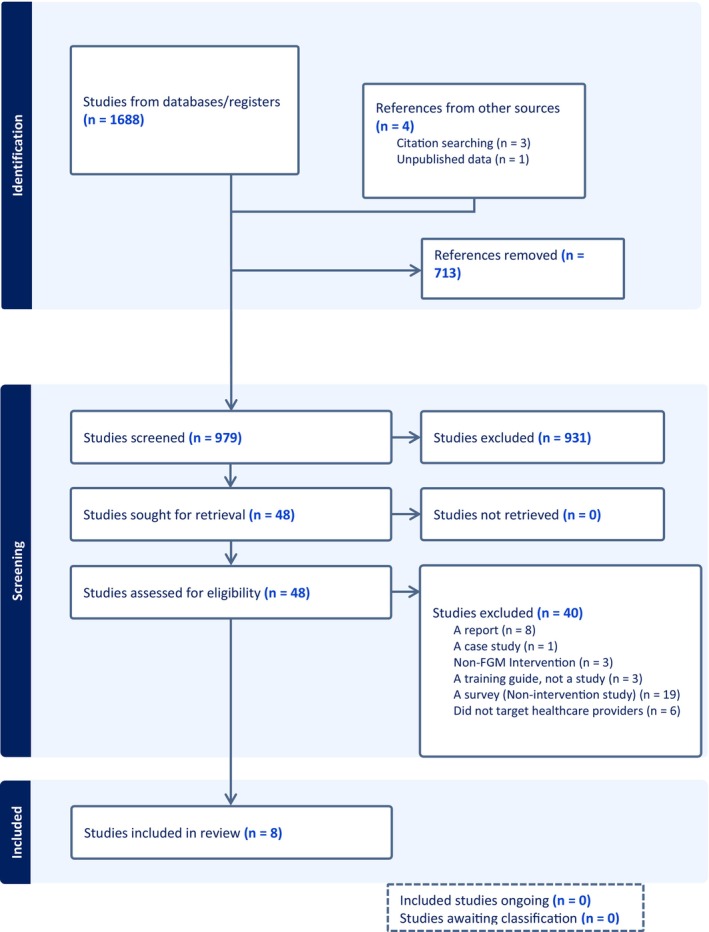 FIGURE 1
FIGURE 1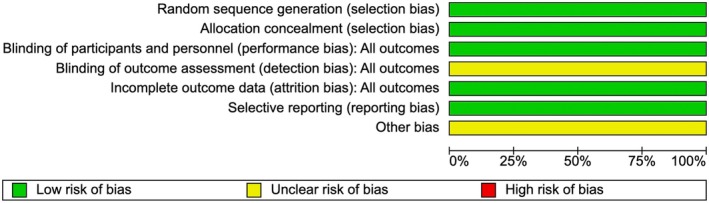 FIGURE 2
FIGURE 2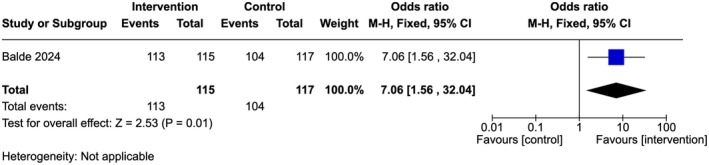 FIGURE 3
FIGURE 3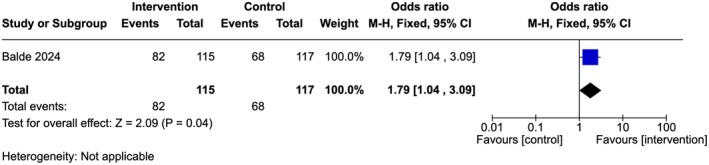 FIGURE 4
FIGURE 4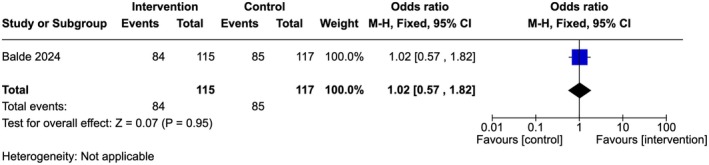 FIGURE 5
FIGURE 5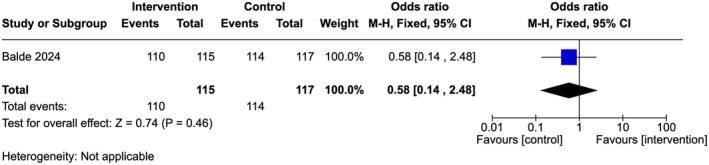 FIGURE 6
FIGURE 6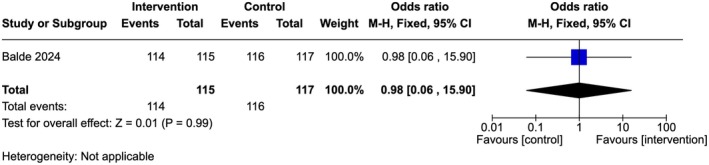 FIGURE 7
FIGURE 7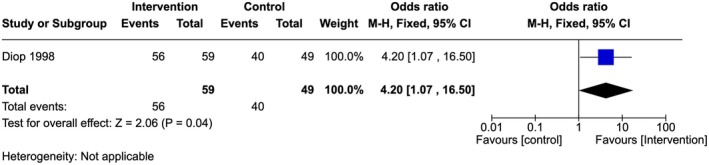 FIGURE 8
FIGURE 8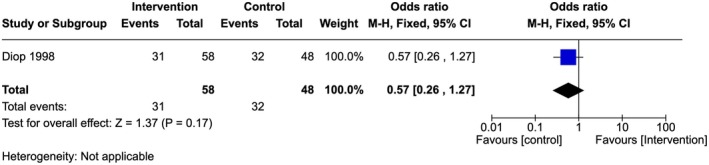 FIGURE 9
FIGURE 9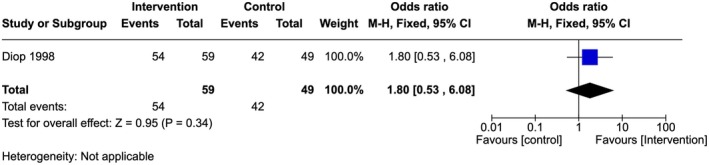 FIGURE 10
FIGURE 10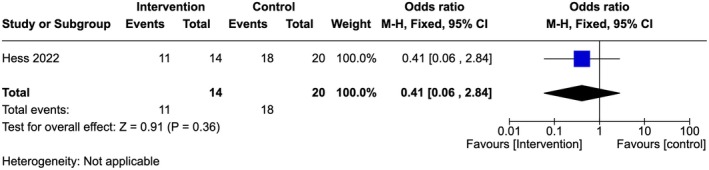 FIGURE 11
FIGURE 11| Study ID | Method | Participants | Intervention | Outcome reported |
|---|---|---|---|---|
| Balde et al. (2024) | Cluster RCT |
232 ANC providers: 193 (83%) were women, mean years of professional experience 8 ± 7 years; 21 (5%) had a certificate, 158 (68%) had a diploma, 44 (19%) had a Bachelors degree, 1 (0.4%) had a Masters degree and above. 103 (44%) providers were midwives, 51 (22%) were nurses, 54 (23%) were nurse‐midwives, 24 (10%) were others. 37% had received formal training on FGM during clinical training and 54% had undergone FGM. Setting: Antenatal clinics in Guinea, Kenya, Somalia |
Experimental group: Intervention was provided at two levels Level 1: Passive distribution of Ministry of Health directives or policy to health facilities on FGM prevention and care, WHO FGM clinical guidelines, a clinical handbook on FGM, and information and educational material in the form of posters to be hung at the health facilities. The materials were distributed without any capacity building to accompany their distribution. Level 2: A PCC training package on FGM prevention. This is an interactive training specifically targeting ANC providers to build their knowledge of FGM, enable them to question their FGM‐related values and attitudes, and build their skills in counseling for FGM prevention using a PCC approach, which is a component of person‐centered care that ensures that the perspectives and preferences of individuals, carers, families, and communities are at the center of decisions and that they have the information and support needed to make decisions. ANC providers were trained to apply a series of structured steps in which they would: “Assess” their client's views on FGM, address and challenge her “Beliefs”, encourage “Change”, and together with the client, “Discuss and Decide” (ABCD).
|
Provide appropriate FGM‐related prevention and care services Correct FGM‐related knowledge responses (ANC providers' mean knowledge score) Appropriate interpersonal communication skills (ANC providers' mean communication skills score) Attitude towards FGM (ANC providers' mean FGM attitude score) Support FGM Support medicalized FGM |
| Diop et al. (1998) | Pre‐ and post‐intervention study with control arm |
Service providers at health centers (nurses‐in‐training or nurse aides, midwives, traditional birth attendants, and health technicians).
Setting: Health centers in Mali (8 = experimental; 6 = control) |
Recall of female anatomy and FGM, its context and local rationale, prevalence in Mali and other regions, and the different types of cutting. Emphasis on health‐related FGM complications and their treatment. It also involved supervision of experimental sites by representatives of other organizations directing the research: DSFC, DRSP, and ASDAP and exposing clients at experimental sites to FGM‐related IEC sessions or counseling. The introduction of FGC‐related IEC activities (the use of IEC visual aids such as flip charts, posters, dummies, AV tools) within health talks and consultations at the clinics and during individual consultations with clients.
| Knowledge of FGM types; knowledge of FGC immediate and long‐term complications; providers' attitudes towards FGM; providers' opinion on FGM/C and health (does FGM poses health risk if carried out in a hygienic environment); providers' communication skills and confidence to provide FGM prevention and care to their clients |
| Newman and Nelson (2003) | Pre‐ and post‐intervention study |
RH providers Setting: Hospital in Maine, USA | PRIME II assisted a Ministry of Health (MOH) and local NGO technical working group in developing and field‐testing a national FGC curriculum (the curriculum is part of a FGC resource package for providers, which includes job aids and a 35‐min video that helps providers understand and identify complications from FGC), which was used to train 120 RH providers in Koulikoro and Bougouni districts and Bamako Commune I | Providers' knowledge about prevention and management of FGC complications; providers' attitude towards FGM; providers' confidence in patient counseling |
| Jacoby and Smith (2013) | Pre‐ and post‐intervention study |
All member midwives (CNMs) of the Maine Chapter of the ACNM in active practice ( Setting: USA |
An education program was developed that included didactic information, case studies, a cultural roundtable, and a hands‐on skills laboratory of deinfibulation and repair. A laminated procedure card describing the procedure was given to each study participant | Knowledge of FGM; providers' confidence in patient's counseling; confidence to practice deinfibulation and repair (either open or reinfibulation); providers' confidence in identifying factors that are contraindications in performing deinfibulation and repair (either open or reinfibulation); understanding implications of FGM/C |
| Elliot et al. (2016) | Pre‐ and post‐intervention group |
Psychosexual therapists attending the College for Sex and Relationship Therapist (COSRT) 2‐day annual conference ( Setting: England |
The 90‐min interactive group workshop with the aim to increase FGM‐related knowledge and skills in the participants. It deliberately moved away from didactic methods and favored skills acquisition through questions, comments, discussion, and debate. The workshop was repeated on four separate occasions during the 2‐day conference to maximize attendance at parallel conference events The intervention began with a small group exercise inviting diverse reactions and questions relating to FGM. This was followed by a brief slide presentation to the entire group, with pauses between the following segments for questions and reactions. It ended with a plenary discussion to draw out key learning points. A handout based on the teaching slides and a resource list including useful websites, training videos, books, and articles accompanied the workshop, and participants were encouraged to look further into the topic, discuss their learning with colleagues, and identify further needs for training and supervision | Knowledge of FGM types; providers' attitude towards FGM; understanding implications of FGM/C |
| Barnawi (2018) | Quasi‐experimental quantitative approach with a non‐randomized, one‐group, pre‐/post‐test design. | Undergraduate nursing students who enrolled in the Bachelor's degree nursing program enrolled as full‐time students in Decker School of Nursing (DSON) at Binghamton University, USA ( | To examine the impact of the FGC digital e‐book on the level of attitude, knowledge, and self‐efficacy among the undergraduate nursing students. They had to watch the FGC digital e‐book and their knowledge was assessed before and after | Impact of the FGC digital e‐book (the intervention) on the level of attitude towards FGM among undergraduate nursing students; impact of the FGC digital e‐book on the level of perception/knowledge among undergraduate nursing students; impact of the FGC digital e‐book on the level of self‐efficacy among undergraduate nursing students |
| Kimani et al. (2018) | Pre‐ and post‐ intervention study |
Nurse‐midwives ( Setting: Kenya |
Training was conducted using content on FGM/C extracted from the UNFPA training modules e‐tool for midwives for 3 days. Training sessions using interactive, trainer‐guided questions and group discussions through moderated plenaries were adopted. The session facilitators included researchers of diverse background relevant to FGM/C, notably Gynecologic/Obstetric, Nursing/Midwifery, Social Sciences, and Sexual Medicine affiliated to Africa Coordinating Centre for Abandonment of FGM/C (ACCAF). Training tool had in‐built electronic‐derived paper‐based pre‐ and post training quiz comprising 12 questions. The quiz assessed the following factors: definition, classification, determining factors, epidemiology, medicalization, prevention, health consequences, and nurse‐midwives' roles in FGM/C prevention themes | Knowledge of FGM types; knowledge of FGC immediate and long‐term complications; providers' confidence in patient counseling; confidence to practice deinfibulation and repair; perception about FGM; benefit of FGM; medicalization of FGM/C |
| Hess et al. (2022) | A quasi‐experimental pre‐/post‐test study with a convenience sample (a control arm) |
3rd‐year nursing students ( Setting: Nursing schools in the Midwestern USA | Students took a pre‐test, did a reading assignment and then attended a virtual, dramatization simulation session with a standardized patient; a Muslim woman with a personal history of FGC; then took the post‐test within the next week | Knowledge of FGM and its complications; understanding implications of FGM/C |
| Study ID | Reason for exclusion |
|---|---|
| ACOG (2020) | A report |
| Adekanle (2011) | A survey (non‐intervention study) |
| Ali (2012) | A report |
| Ashimi (2014) | A survey (non‐intervention study) |
| Bankolé Sanni (1997) | Wrong study population |
| Calvert (2020) | A survey (non‐intervention study) |
| Chelala (1998) | Wrong study population |
| Deane (2022) | A survey (non‐intervention study) |
| Diop (2004) | Wrong study population |
| Diop (2008) | Wrong study population |
| El‐Gibaly (2019) | Non‐FGM intervention |
| Eyega (1997) | A survey (non‐intervention study) |
| Fay (2022) | A survey (non‐intervention study) |
| Galal (2022) | A survey (non‐intervention study) |
| Galukande (2015) | Wrong study population |
| Hess (2010) | A survey (non‐intervention study) |
| Jones (2023) | A survey (non‐intervention study) |
| Jorgensen (1998) | A report |
| Kangoum (1992) | Wrong study population |
| Kaplan (2013) | A survey (non‐intervention study) |
| Kaplan‐Marcus (2010) | A survey (non‐intervention study) |
| Kouta (2023) | A survey (non‐intervention study) |
| Leye (2006) | A report |
| Nybro (1998) | A case study |
| Refaat (2009) | A survey (non‐intervention study) |
| Relph (2013) | Non‐FGM intervention |
| Rogowska‐Szadkowska (2009) | A report |
| Tantet (2018) | A survey (non‐intervention study) |
| Thomas (2022) | A survey (non‐intervention study) |
| Thompson (2013) | A report |
| Ventura (2021) | A survey (non‐intervention study) |
| WHO (2001a) | Non‐FGM intervention |
| WHO (2001b) | A training guide |
| WHO (2006) | A survey (non‐intervention study) |
| WHO (2010) | A report |
| WHO (2011) | A report |
| WHO (2022a) | A training manual |
| WHO (2022b) | A training manual |
| Wyss (2022) | No control arm and not pre‐post design |
| Ziyada (2023) | A survey (non‐intervention study) |
| Study ID | Is confounding of the effect of intervention unlikely in this study? | Bias in selection of participants into the study | Bias in measurement of intervention | Bias due to departures from intended interventions | Bias due to missing data | Bias in measurement of outcomes | Bias in selection of the reported result | Overall bias | Did authors employ matching or restriction at design stage? | Did authors employ stratification or regression modeling in their analysis? |
|---|---|---|---|---|---|---|---|---|---|---|
| Diop et al. (1998) | Moderate | Moderate | Low | Low | Moderate | Low | Moderate | Moderate | No | No |
| Limited information to assess this domain | All health personnel (focused on OB‐GYN practitioners) were said to be included in the different sites. No detail on how the recruitment or selection of the sites was carried out | The different interventions were well defined | Intervention was implemented over a short period of time; switches were unlikely as experimental and control sites are in different communities | 4 people were said to be missing during the analysis, but it was not specified if they were from the experimental or control sites; also, for some of the post‐test data, some of the questions were not completed by the participant | Method of outcome assessment was comparable across groups and not likely to be influenced by knowledge of the intervention received | Study did not report comparison between the intervention and control groups regarding some of their stated objectives, thus not free of selective reporting | ||||
| Hess et al. (2022) | Low | Low | Low | Low | Low | Low | Moderate | Moderate | No | No |
| Bias due to confounding is unlikely | Baseline characteristics were similar between groups. The same participant included in pre‐ and post‐surveys | The different interventions were well defined | No deviations from the intended intervention | The data were reasonably complete. One student did not complete the pre‐test, the other student did not complete the post‐test; both were in the control group | The method of outcome assessment was comparable across groups; researchers were blinded to the participants' completed tests | Unable to access this as we did not have access to protocol | ||||
| Newman and Nelson (2003) | Low | Low | Low | Low | No information | Low | Moderate | Moderate | No | No |
| No confounding expected | Study followed the same participants from pre‐intervention to post‐intervention, selection bias unlikely | Intervention status was well‐defined | Unlikely because the curriculum was a standardized video recording on FGM prevention |
No information is reported about missing data or the potential for data to be missing | The method of outcome assessment was comparable at the before‐ and after survey | No information was provided to assess this domain | ||||
| Jacoby and Smith (2013) | Low | Low | Low | Low | Low | Low | Moderate | Moderate | No | No |
| No confounding expected | Study followed the same participants from pre‐intervention to post‐intervention, selection bias unlikely | Intervention status was well‐defined | No deviation from the intervention reported | All participants were analyzed | The method of outcome assessment was comparable at the before‐ and after survey | Unable to access this as we did not have access to protocol | ||||
| Elliot et al. (2016) | Low | Low | Low | Low | Low | Low | Moderate | Moderate | No | No |
| No confounding expected | Study followed the same participants from pre‐intervention to post‐intervention, selection bias unlikely | Intervention status was well‐defined | No deviation from the intervention reported | All participants were analyzed | The method of outcome assessment was comparable at the before‐ and after survey | Unable to access this as we did not have access to protocol | ||||
| Barnawi (2018) | Low | Low | Low | Moderate | Moderate | Low | Moderate | Moderate | ||
| No confounding expected (all participants were in the same medical field) | Study followed the same participants from pre‐intervention to post‐intervention, selection bias unlikely | Intervention status was well‐defined. | The study used a FGC digital e‐book. The research relied on the students' skills of using audiovisual technology, which may vary from one student to another. Even though the author provided clear guidelines on how to utilize the FGC digital e‐book, some students may have skipped through some sections, not completing the e‐book content. | It was not clear how many students completed the pre‐test and how many completed the post‐test. The author mentioned 10 participants who dropped out of the post‐test after accessing the FGC digital e‐book. Reference was made to “the loss of study subjects due to the limited time and students' commitment to other coursework.” | The method of outcome assessment was comparable at the before‐and‐after survey. | Unable to access this as we did not have access to protocol. | No | No | ||
| Kimani et al. (2018) | Moderate | Low | Low | Low | Low | Moderates | Moderate | Moderate | No | No |
| Difference in the educational qualifications of participants: 19 had a diploma, two had a certificate, five participants had a Bachelors degree and two had a Masters degree | The same participants from pre‐intervention to post‐intervention, selection bias unlikely | Intervention status was well‐defined | No deviation from the intervention reported | All participants were analyzed | Study reported that “the tool had an inbuilt electronic‐supported quiz programmed in such a way that one must correctly answer the preceding questions before proceeding to the next. The tool enabled participants to retake questions until the correct response was achieved.” Unclear if this was pre‐ or post‐survey | Unable to access this as we did not have access to protocol |
- —Government of Norway and the UNDP‐UNFPA‐UNICEF‐WHO‐World Bank Special Programme of Research, Development, and Research Training in Human Reproduction (HRP), a cosponsored programme executed by the Wor
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFemale Genital Mutilation/Cutting Issues · Genital Health and Disease · Ureteral procedures and complications
INTRODUCTION
1
Background
1.1
Female genital mutilation (FGM) involves altering female genitalia for cultural or nonmedical reasons.1 Recent evidence shows a decline in FGM prevalence among girls aged 16–19 years in many affected regions, especially in parts of West and East Africa and some countries in the Middle East and South Asia.2 However, FGM remains a major public health issue, with over 230 million girls and women in 31 countries having undergone the practice.2, 3 It is also reported in high‐income countries due to international migration.4 FGM is typically performed with sharp objects by individuals such as elderly women and traditional birth attendants.5, 6 Some healthcare providers also perform FGM, citing harm reduction, better hygienic conditions, social pressure from families, or financial gain.3, 7, 8
FGM is practiced on girls aged 4–12 years but may occur days after birth to just before marriage, depending on local traditions.6 It is driven by social pressures, religious beliefs, and the belief that it reduces sexual desire. Despite having no health benefits, FGM poses immediate risks, such as pain and bleeding, and long‐term complications, including gynecological and obstetric issues, urinary problems, psychological trauma, and sexual dysfunction,3 underscoring the urgent need to eliminate the practice.9, 10
FGM poses both short‐ and long‐term challenges, complicating the provision of care services for affected women and adolescents. Healthcare providers often struggle to discuss FGM, and some may lack the clinical skills needed, particularly for managing cases involving deinfibulation.11 Studies highlights the challenges healthcare workers face in caring for women with infibulation during childbirth, including the need for deinfibulation and managing related complications.12, 13 In both high‐ and low‐prevalence countries with affected populations, including the United Kingdom, Spain, and the United States, healthcare workers often have significant gaps in theoretical knowledge and practical skills. Some report fear, limited experience, and discomfort discussing FGM.14 To address this, WHO has supported priority countries in developing comprehensive action plans, including capacity building for healthcare workers based on evidence‐based resources.15
Various activities implemented by ministries of health, international organizations, educators, and nongovernmental organizations have focused on capacity building of healthcare workers to address FGM‐related complications. These include training on legal frameworks, evidence‐based management of sexual, obstetric, and psychosocial complications, and developing competencies in person‐centered communication (PCC) and respectful care.16, 17, 18 Educational approaches range from health talks, visual aids, role‐plays, case studies, and group discussions to hands‐on demonstrations, storytelling, and mobile apps.17, 18, 19 WHO has also developed tools, such as training materials, guidelines, and a clinical handbook to strengthen healthcare capacity and improve care for at‐risk or affected individuals.19, 20
These resources aim to enhance healthcare workers' knowledge, skills, and confidence in FGM prevention and care, empowering them to engage in informed PCC and influence clients to abandon the practice. In addition, tools such as structured interview guides, infographics, and counseling checklists can help bolster the retention of information among healthcare workers and serve as practical reminders during service delivery.21
This review sought to determine the impact of providing FGM training and education to healthcare workers and/or provision of capacity‐building resources such as job aids, information, education, and communication (IEC) materials, clinical guides/handbooks, and other training materials on FGM to healthcare providers on their knowledge, attitudes to FGM, and their skills in providing care for girls and women living with FGM.
METHODS
2
The review was conducted in line with the Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0,22 and the findings were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines.23 The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO; ID: CRD42023426370).
Literature search
2.1
A systematic search was carried out of the following electronic databases from inception to May 2023: CINAHL Plus, IRIS, MEDLINE, PsycINFO, SCOPUS, and Web of Science. The full details of the search are detailed in Table S1. We also reviewed the reference lists of relevant studies, including contacts of experts in women's health for additional references. No language restrictions were applied.
Study selection
2.2
Two authors independently screened titles, abstracts, and full texts of relevant articles using the Covidence software.24 Discrepancies were resolved through team discussion. We considered randomized, non‐randomized studies, cohort studies, case–control studies, and pre‐ and post‐test studies with/without comparative analysis. Any intervention providing information on FGM practices, risks, and care, regardless of delivery mode among healthcare workers, was considered. Outcomes assessed included improved FGM knowledge, communication skills, complication management, attitude change, community education, reduced stigma, and increased reporting.
Data collection
2.3
Three authors independently extracted data using a template developed in Microsoft Excel. Where available, we extracted information on location, race, occupation, gender, religion, education, and socioeconomic status, along with healthcare providers' categories. Details included the nature of intervention including job aids provided, delivery method, duration, follow‐up length, and outcomes. Two review authors independently assessed study bias using the Cochrane Risk of Bias tool for Randomized Controlled Trials (RCTs)22 and the Cochrane Risk Of Bias In Non‐randomized Studies of Interventions (ROBINS‐I) for non‐randomized studies.25 Judgments of “yes”, “no”, and “unclear” were used to indicate a low, high, or unclear risk of bias. Disagreements were resolved through discussion between review authors.
Data analysis
2.4
Statistical analyses were performed with Review Manager Web.26 Odds ratios (ORs) were reported with 95% confidence intervals (CIs). When percentages were provided, actual numbers were calculated. Individual outcome findings were illustrated using forest plots. When an analysis was not possible, a narrative summary was presented following Synthesis without Meta‐analysis (SWiM) guidelines.27 Due to variations in study types, populations, durations, and outcome reporting, data pooling was not feasible. The quality of the evidence was evaluated using the GRADE approach and summarized in GRADE evidence tables (Table S2).
RESULTS
3
The search returned 1692 articles. After de‐duplication, the titles and abstracts of 979 records were screened, of which 48 were eligible for full‐text assessment and eight studies were included. The included studies are described in Table 1. The excluded studies and the reasons for exclusion are described in Table 2. Details of the search results are presented in a PRISMA flow diagram (Figure 1).
Flow diagram of included studies.
The included studies were carried out between 1998 and 2022. Five of the studies were noncontrolled pre‐ and post‐test studies,17, 29, 30, 31, 32 two were controlled non‐randomized studies,28, 33 and one was a cluster RCT.34 One study was carried out in Kenya, two in Mali, three in the United States, one in the United Kingdom, and one was a multicenter study carried out in Guinea, Kenya, and Somalia. Participants included different cadres of healthcare workers: obstetrician and gynecologist (n = 1), midwives (n = 2), psychosexual therapists (n = 1), nursing students (n = 2), and antenatal care (ANC) providers, which includes nurses, midwives, and other healthcare workers (n = 2). One study did not specify the cadre of healthcare worker, but targeted reproductive health service providers.
The interventions varied in delivery method, including in‐person presentation, lectures, group discussions, and hands‐on skills building.17, 28, 30, 32 One study used a self‐directed learning female genital cutting (FGC) digital e‐book31 and another conducted a virtual dramatization with a standardized patient who had a history of FGM.33 In‐person sessions typically combined videos and hands‐on techniques. One study incorporated diverse participatory adult learning methods, including value clarification exercises, storytelling, interactive games, demonstrations, and role‐plays.34 All interventions included theoretical content on FGM classification, complications, treatments, and prevalence. The duration of the intervention was in the range of 90 min to 2 months. The RCT compared a PCC training for FGM prevention with a health‐system strengthening approach; the control arm received only the latter.34
The Cochrane Risk of Bias tool for RCTs was used to assess the RCT, which was judged low risk in all domains except for detection bias for self‐reported outcomes, which was judged unclear as it was not reported in the article.34 In addition, the study was judged as unclear for other bias, as the authors reported possible selection bias in provider enrollment due to the use of clinical rotation schedules (Figure 2).
Risk of bias (Balde 2024). Source: Review Manager (RevMan) Web.
The risk of bias for the observational studies was assessed using the ROBINS‐I (Table 3).25 Overall, the studies were judged to have a “moderate” risk of bias. The studies were judged to be of moderate risk on the following domains: confounding,28, 32 selection bias,28 deviation from intended intervention,31 missing data,28 and outcome measurement.32 All the studies lacked a published protocol and were therefore judged as moderate for reporting bias. The use of interviewers posed a risk of interviewer bias, due to potential influence of preconceptions.28 Self‐report instruments are prone to biases, as participants may provide socially acceptable answers or may interpret the questions incorrectly. In one study, an electronic quiz allowed repeated attempts, but it was unclear if this applied to both pre‐ and post‐tests, possibly biasing reported outcomes.32 Two other studies used voluntary participant sampling to select participants, introducing potential sampling bias.31, 33
Effect of intervention
3.1
Training of healthcare providers plus provision of IEC materials compared to provision of IEC materials only (RCT)
3.1.1
Knowledge of FGM
3.1.1.1
Moderate‐quality evidence showed that ANC providers in the intervention arm had higher mean scores of FGM‐related knowledge (2.5, 95% Cl 2.2–2.7) compared to the control arm (1.6, 95% CI 1.5–1.8; P < 0.001).34
Communication skills and confidence to provide FGM prevention and care to their clients
3.1.1.2
The intervention consisted of an interactive training to build ANC providers' knowledge of FGM using a component of PCC, where ANC providers were trained on a step‐by‐step approach to “Assess” the client's views on FGM, address and challenge her “Beliefs”, encourage “Change”, and together with the client, “Discuss and Decide” (ABCD).
Providing appropriate FGM‐related prevention and care services
3.1.1.3
Moderate‐quality evidence showed that ANC providers in the intervention arm had a higher mean score of providing appropriate FGM prevention and care services (6.2, 95% Cl 5.9–6.6) compared to the providers in the control arm (3.7, 95% Cl 3.2–4.1) with a difference in the mean score of 2.5 (95% Cl 2.0–3.2; P < 0.001).34
In addition, clients reported that compared to ANC providers in the control group, those in the intervention group were more likely to implement components of PCC when addressing FGM prevention. Those in the intervention group were nearly nine times more likely to ask clients about FGM (adjusted odds ratio [AOR] 8.9, 95% CI 6.9–11.5; P < 0.001), nearly 10 times more likely to ask about clients' personal beliefs on FGM (AOR 9.7, 95% CI 7.5–12.5; P < 0.001), over nine times more likely to discuss the reasons for preventing FGM (AOR 9.2, 95% CI 7.1–11.9; P < 0.001), and nearly eight times more likely to talk about how FGM could be prevented (AOR 7.7, 95% CI 6.0–9.9; P < 0.001) compared to the ANC providers in the control group.34
Confident in the knowledge to provide FGM prevention and care services
3.1.1.4
Moderate‐quality evidence showed that ANC providers in the intervention arm had higher odds of being confident in their knowledge to provide FGM prevention and care services compared to those in the control arm (OR 7.06, 95% Cl 1.56–32.04; one study, 232 participants) (Figure 3).34
Confident in the knowledge to provide FGM prevention and care services.
Appropriate interpersonal communication skills
3.1.1.5
Moderate‐quality evidence showed that there was no statistically significant difference between the number of healthcare providers in the intervention arm compared to the control arm regarding appropriate interpersonal communication skills (OR 1.79, 95% Cl 1.04–3.09; one study, 232 participants) (Figure 4).34
Appropriate interpersonal communication skills.
Change in attitude about support for FGM, FGM medicalization, and reinfibulation
3.1.1.6
Low‐quality evidence showed that there is no significant difference between the groups (OR 1.02, 95% Cl 0.57–1.82; one study, 232 participants) (Figure 5). A similar trend was observed among the providers in both groups reporting that they did not support FGM (96% in the intervention arm compared to 97% in the control arm [OR 0.58, 95% Cl 0.14–2.48; one study, 232 participants]) (Figure 6) and/or medicalized FGM (99% in both arms [OR 0.98, 95% Cl 0.06–15.9; one study, 232 participants]) (Figure 7).34
Less supportive attitude towards FGM.
Not supportive of FGM.
Not supportive of medicalized FGM.
Educational intervention (face‐to‐face, group discussion, hands‐on demonstration) compared to no intervention control arm (non‐randomized)
3.1.2
Knowledge of FGM
3.1.2.1
Very low‐quality evidence showed that there was a significant difference between the number of providers that could recognize the different types of FGM in the intervention compared to the control arm. Providers in the intervention arm had higher odds of recognizing the different types of FGM compared to providers in the control sites (OR 4.20, 95% CI 1.07–16.50; one study, 108 participants) (Figure 8).28
Knowledge of the different types of FGM.
Very low‐quality evidence showed that when asked whether FGM posed no health risk when carried out in a hygienic environment; there was no statistically significant difference between the providers (54%) in the intervention site compared to 66% of providers in the control sites who disagreed (OR 0.57, 95% CI 0.26–1.27; one study, 106 participants) (Figure 9).28
Number of providers who disagree that FGM posed no health risk in a hygienic environment.
Ability to identify FGM‐related complications
3.1.2.2
One study reported similar increase in the number of providers in both arms that could mention at least three immediate complications. In the intervention arm, the number of providers increased from 40% to 86%, and knowledge of subsequent complications increased from 49% to 72% at follow‐up. To a lesser degree, respondents from the control sites also registered improvement in their knowledge of FGM‐related complications, with an increase from 61% to 73% at follow‐up.28 The quality of evidence was very low.
Communication skills and confidence to provide FGM prevention and care
3.1.2.3
One study reported that a significant majority (96%) of the healthcare providers who used the flip chart said it helped them communicate messages more effectively. However, some found it constraining, while 38% felt it did not limit their ability to convey information. Among the 63% who thought they were constraining, 56% still found it useful.28 It was not specified how the result applied to the experimental and control sites.
The study also reported that more than half of the health agents who had received IEC training were unwilling to address FGM‐related issues with clients compared to one‐third of those who had not been trained in communication techniques.28
Provider view of their active role in anti‐FGM activities
3.1.2.4
There was no statistically significant difference in the number of providers willing to conduct IEC activities in the intervention sites (91.5%) compared to the control sites (85.7%) (OR 1.80, 95% Cl 0.53–6.08; one study, 108 participants) (Figure 10).28 The quality of evidence was very low.
Provider view of their active role in anti‐FGM activities.
Virtual, dramatization simulation session with a standardized patient with FGM compared to no intervention control arm (non‐randomized)
3.1.3
Knowledge of FGM
3.1.3.1
Very low‐quality evidence showed that training improved knowledge of FGM with a mean score of 9.50 ± 1.345 in the intervention group compared to 6.76 ± 4.640 in the control group (mean difference [MD] 2.74, range 0.59–4.89).33
Knowledge of the consequences of FGM
3.1.3.2
Very low‐quality evidence showed that there was no difference in the number of providers in both arms regarding the knowledge that the consequences of FGM are numerous (OR 0.41, 95% Cl 0.06–2.84; one study, 34 participants) (Figure 11).33
Knowledge on the consequences of FGM.
Change in attitude about support for FGM, FGM medicalization, and reinfibulation
3.1.3.3
One study reported that more participants thought FGM should not be medicalized (26.5% increase) on the post‐test.33 No information was provided for the different arms in both studies and the quality of evidence was very low.
Educational intervention (face‐to‐face, group discussion, hands‐on demonstration) (pre‐ and post‐test study)
3.1.4
Knowledge of FGM
3.1.4.1
All studies that assessed the outcome reported an improvement in knowledge after the intervention. One study reported an increase from a mean of 2.36 to 4.18.17 Another study reported that the number of participants who knew the number of the types of FGM increased from 35% to 85% (χ ^2^ [6, N = 97] = 29.10; P < 0.001).30 One study reported a significant improvement in participants' knowledge after a 3‐day training, from 64% at baseline versus 96.2% after training (t(25) = 7.408; P < 0.001), and knowledge of the types of FGM/C, from 84.6% at baseline versus 100% after training (t(25) = 2.132; P = 0.043).32 The quality of evidence for all the studies was very low.
Confidence and ability to identify FGM‐related complications
3.1.4.2
After training, one study reported improved scores in participants' knowledge of FGM‐related health consequences (immediate physical, P = 0.003; gynecological, P = 0.001; obstetric, P = 0.022; sexual, P < 0.001; and social harms, P < 0.001). There was no statistically significant difference in knowledge scores regarding FGM‐related psychological complication after intervention.32 The quality of evidence for all the studies was very low.
Change in attitude about support for FGM, FGM medicalization, and reinfibulation
3.1.4.3
One study found no significant difference before and after the intervention.30 In another study, all the participants agreed that FGM/C violates women's and girls' human rights (P = 0.043) and that it was not safer if FGM was performed by healthcare workers.32 The study further assessed the capacity of participants to resist reinfibulation if requested by a woman supposedly under pressure from her husband and reported significant improvement on the need for the woman to remain deinfibulated (P < 0.001).32 Participants' knowledge on the importance of the need to leave the woman deinfibulated was reported to be poor to moderate.32 There was also an improvement after training with providers pledging to never perform FGM because it is not medically necessary and causes harm (t(25) = −5.000; P < 0.001). The quality of evidence for all the studies was very low.
Communication skills and confidence to provide FGM prevention and care to their clients
3.1.4.4
One study reported an increase in the mean confidence level from 2.36 to 4.09 among healthcare workers regarding counseling women with type III FGM. The mean confidence level of healthcare provider increased from 1.54 to 3.54 after training on deinfibulation and repair using simulated pelvic models.17 The quality of evidence for all the studies was very low.
Virtual training only (before‐and‐after study)
3.1.5
Knowledge of FGM
3.1.5.1
One study reported that an FGM digital e‐book significantly improved the attitudes of nursing students on FGM, with an increase in mean FGM knowledge scores from 32.95 ± 2.977 at baseline to 38.49 ± 2.895 after the intervention (MD 5.54 ± 4.5, range − 6.495 to −4.583; P < 0.001).31 The quality of evidence for all the studies was very low.
Communication skills and confidence to provide FGM prevention and care to their clients
3.1.5.2
In one study that provided virtual training, after the intervention, providers were three times more likely to ask pregnant women if they have FGC complications that might affect birthing.29 Another study reported an increase in the level of readiness of students to provide competent care to manage FGM from a mean of 15.7629 ± 1.88 at baseline to 18.567 ± 1.89 after the intervention (MD –2.80, range − 3.37 to −2.24; P < 0.001).31 The quality of evidence for all the studies was very low.
Management of patients with FGM‐related complications
3.1.5.3
One study assessed the number of FGM‐related complications that were treated on site and reported that the mean number of such FGM‐related complications increased by 26%.29 The quality of evidence was very low.
Change in attitude about support for FGM, FGM medicalization, and reinfibulation
3.1.5.4
One study reported a significant improvement regarding the attitude toward FGM among nursing students after training. The mean FGM attitude scores increased from 49.42 ± 5.475 at baseline to 54.89 ± 5.902 after the intervention (MD 5.47, SD 8.3, range − 7.18 to −3.77; P < 0.001).31 The quality of evidence was very low.
Skills on providing FGM‐related education and counseling for communities in outreach services
3.1.5.5
One study reported an improvement in healthcare workers providing counseling on FGM, which was nonexistent at baseline. The study reported that 414 women receiving antenatal care also received counseling on abandoning FGM. In addition, nearly 75% of providers assessed passed the counseling skill performance test. The study also showed that healthcare workers were present as resource persons at 714 of 1187 community outreach sessions and 473 educational sessions where they discussed the negative effects of FGM.29
None of the included studies reported on the reduction of FGM‐related stigma, discrimination, and disrespectful care or the recording of FGM in clinical reports.
DISCUSSION
4
This review sought to determine the impact of FGM education on healthcare providers' knowledge, attitudes, skills, and quality of care for girls and women with FGM. The results showed that the training, whether delivered face‐to‐face or online, improved healthcare workers' knowledge of FGM and its complications. Healthcare workers reported increased confidence in identifying and managing FGM‐related complications, enhanced communication and counseling skills, with some improvement in attitudes toward FGM, its medicalization, and reinfibulation. Some training institutions offer materials such as job aids and handbooks on FGM; however, gaps remain in many countries. Findings from this review indicate that the provision of these materials alone is insufficient to enhance knowledge; however, emphasis should also be placed on capacity building, which involves teaching healthcare workers how to effectively utilize these resources and to build skills and competencies. One study demonstrated a significant increase in resource use of 91% among the intervention group compared to 56% in the control group, who also had access to the resources but did not receive additional training.34 This highlights the importance of capacity building for healthcare workers, suggesting that training and ongoing support play a key role. The same study reported improved healthcare workers' attitudes, making them less supportive of the practice.34
In‐depth interviews with healthcare workers and ANC clients revealed that healthcare workers found the ANC context to be a feasible, acceptable, and appropriate entry point for FGM prevention counseling. Likewise, clients were satisfied with the communication received and trusted their ANC provider as a source of information. Healthcare workers also suggested integrating such discussions at other service delivery points within health facilities and involving different cadres of healthcare workers (e.g., community healthcare workers) to increase the sustainability and impact of the intervention.35
FGM training programs generally enhance theoretical knowledge and confidence, often focusing on classification, complications, and counseling over practical, hands‐on clinical skills.36, 37 This may create a false sense of diagnostic competence, particularly in legal settings where misclassification carries serious consequences.38, 39 Research shows that aside from infibulation, most forms of FGM are difficult to identify, even for experienced clinicians, challenging the assumption that FGM types can be reliably and visibly distinguished through theoretical training alone.40
The included studies on FGM training were conducted in diverse locations, encompassing both low‐ and high‐income countries, suggesting the effectiveness of implementing such education in different settings. However, the varied prevalence of FGM in these countries limits the broad generalization of findings. The mode and duration of intervention delivery varied across studies, ranging from face‐to‐face sessions to virtual simulations lasting 35 min to 4 days. Despite these differences, improvements in reported outcomes were consistent, indicating that the mode of intervention might not significantly impact the results. Most studies had short follow‐up periods, typically concluding at the end of the intervention, making it difficult to reliably assess long‐term changes in knowledge and attitude. Longer follow‐up studies, extending to 1 year or longer, are needed to better understand lasting impacts. In some non‐randomized controlled studies, both the intervention and control groups showed similar improvements in certain outcomes, raising questions about whether changes can be solely attributed to the intervention.28, 33 Participants in the control group may have independently sought information on FGM after the baseline assessments.
Evidence from some studies suggest that although training can improve awareness, it may lead to unintended consequences, such as stigmatization or excessive questioning of women with FGM, potentially resulting in poorer care experiences.41, 42 Although these outcomes were beyond the scope of this review, they underscore the importance of sensitive, person‐centered approaches. One of the included studies reported that PCC improved ANC providers' engagement on FGM prevention. Providers in the intervention group were 9–10 times more likely to initiate discussions on FGM‐related topics, including beliefs, abandonment, and prevention. These findings suggest that capacity building can strengthen both provider knowledge and respectful, effective communication.34
Notably, none of the studies evaluated the impact of FGM training on local health practitioners, such as traditional birth attendants and community healthcare workers who play a role in FGM practices in some settings and can be transformed into advocates against the practice given their proximity to affected communities. Consequently, the influence of these interventions on the knowledge and attitudes of such practitioners remains unclear.
This review aligns with previous research suggesting that FGM‐related training improves provider knowledge and attitudes [43]. It also supports recommendations to include such training during both pre‐licensing and in‐service education for health professionals.43, 44
Strength and limitations
4.1
The review utilized a comprehensive search of relevant databases without restrictions in study type or language. Following Cochrane methodology, it employed a robust approach, including reviewer blinding and a validated screening tool to minimize bias.22, 24 Despite this, few studies met the inclusion criteria, with only one RCT. Some studies had small sample sizes, which limited the ability to determine significance.17, 29, 30, 33 Variation in intervention delivery and duration prevented meta‐analysis. No study assessed the long‐term effects on information retention or changes in providers' attitudes. Only two studies assessed client satisfaction with health services after the intervention.28, 34 Finally, outcomes relied on self‐reports or interviews, potentially introducing self‐report bias.
CONCLUSION
5
This review indicates that training influences healthcare workers' knowledge and attitudes toward FGM. However, the limited number of studies and lack of high‐quality evidence prevent definitive conclusions about the effectiveness of educational interventions or the best ways to implement them. These limitations reduce the reliability and generalizability of the findings. More rigorous, multicentered studies are needed, especially in FGM‐prevalent regions and industrialized countries with large immigrant populations. Future research should consider regional, ethnic, and sociodemographic differences with long‐term follow‐up to assess sustained changes in provider knowledge and attitudes.
AUTHOR CONTRIBUTIONS
CO and SO coordinated the screening and data extraction, performed the data analysis, interpreted the results, and drafted the manuscript. AO contributed to the screening, data extraction, and analysis and drafting of the manuscript. MO and FO contributed to the screening and drafting of the manuscript. ON participated in interpretation of the results and writing of the manuscript. CCP contributed to the development of the research question and drafting of the manuscript. MM conceptualized the study, coordinated its planning and implementation, and supervised the analysis of the data and writing of the manuscript. All authors commented on and approved the final manuscript.
FUNDING INFORMATION
This work received funding from the Government of Norway and the UNDP‐UNFPA‐UNICEF‐WHO‐World Bank Special Programme of Research, Development, and Research Training in Human Reproduction (HRP), a cosponsored programme executed by the World Health Organization (WHO).
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest.
Supporting information
Table S1: Search strategy.
Table S2: a‐e: GRADE tables.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization, United Nations Population Fund & United Nations Children's Fund (UNICEF) . Female genital mutilation: a joint WHO/UNICEF/UNFPA statement. World Health Organization; 1997 [WHO website]. Accessed May 14, 2023. https://iris.who.int/handle/10665/41903
- 2United Nations Children's Fund . Female Genital Mutilation: A global concern. 2024 Update. UNICEF; 2024 Accessed April 3, 2025. https://data.unicef.org/resources/female‐genital‐mutilation‐a‐global‐concern‐2024/
- 3World Health Organization . Female genital mutilation. World Health Organization (WHO). January 31, 2025. Accessed April 5, 2025. https://www.who.int/news‐room/fact‐sheets/detail/female‐genital‐mutilation
- 4Yoder PS , Abderrahim N , Zhuzhuni A . Female Genital Cutting in the Demographic and Health Surveys: A Critical and Comparative Analysis. DHS Comparative Reports No. 7. ORC Macro; 2004.
- 5World Health Organization . Female Genital Mutilation. Integrating the Prevention and the Management of the Health Complications into the curricula of nursing and midwifery: Teachers Guide. 2001 [WHO website]. Accessed May 16, 2023. https://www.who.int/publications/i/item/WHO‐RHR‐01.16
- 6Chalmers B , Omer‐Hashi K . What Somali women say about giving birth in Canada. J Reprod Infant Psychol. 2002;20:267‐282.
- 7Doucet MH , Pallitto C , Groleau D . Understanding the motivations of health‐care providers in performing female genital mutilation: an integrative review of the literature. Reprod Health. 2017;14(1):46.28335771 10.1186/s 12978-017-0306-5PMC 5364567 · doi ↗ · pubmed ↗
- 8Balde MD , O'Neill S , Sall AO , et al. Attitudes of health care providers regarding female genital mutilation and its medicalization in Guinea. P Lo S One. 2021;16(5):e 0249998.33983949 10.1371/journal.pone.0249998 PMC 8118326 · doi ↗ · pubmed ↗