Physiological responses of children with surgically corrected congenital heart disease during high-altitude trekking: an exploratory observational study
Kwang Ho Choi, Woong-Han Kim, Ja-Kyoung Yoon

TL;DR
Children with surgically corrected heart defects can safely trek at high altitudes, showing good physiological adaptation.
Contribution
This study explores physiological responses of children with CHD during high-altitude trekking, offering new insights into their cardiovascular adaptation.
Findings
Oxygen saturation declined similarly in children with CHD and adults during ascent.
Children with CHD showed increased heart rate but stable blood pressure at high altitudes.
No evidence of maladaptation or altitude-related illness was observed in CHD participants.
Abstract
Children with surgically corrected congenital heart disease (CHD) are often perceived as fragile and discouraged from engaging in physical activity, despite evidence that structured exercise improves functional capacity and quality of life. However, data on their physiological responses to extreme environments, such as high-altitude exposure, remain limited. We conducted an exploratory observational study during an Annapurna Base Camp trek (maximum altitude 4,150 m) in February 2024. Children with surgically corrected congenital heart disease and accompanying healthy adults participated in the expedition. Oxygen saturation (SpO2), heart rate (HR), and blood pressure (SBP and DBP) were recorded daily at sequential altitudes, and adverse events were monitored. From 1,350 m to 4,150 m, SpO2 showed a similar pattern of decline in children (−9.8%) and adults (−8.1%). CHD participants…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1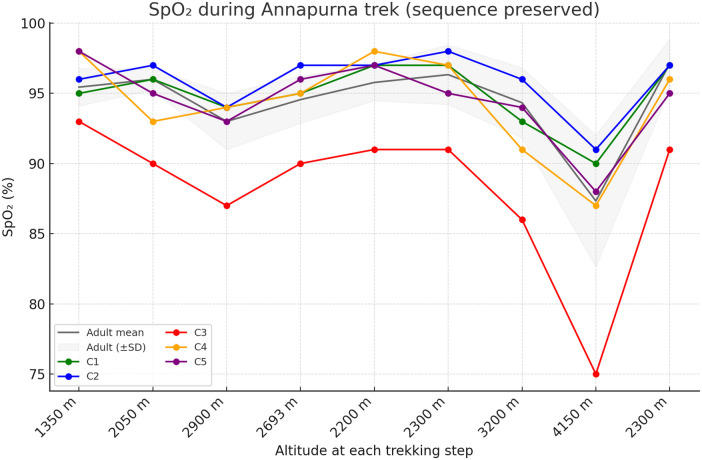 Figure 2
Figure 2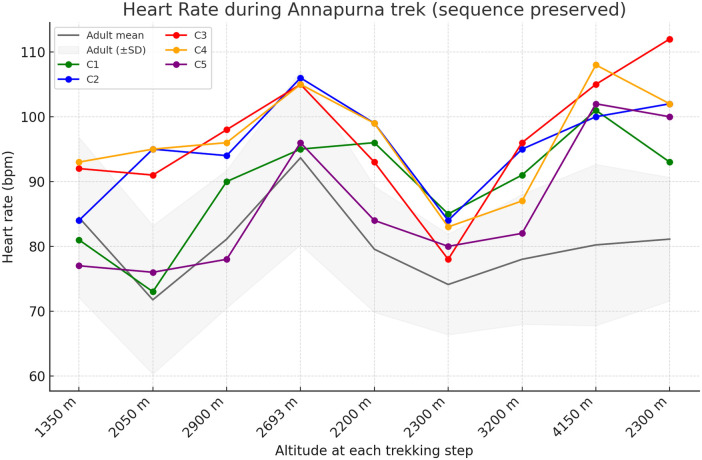 Figure 3
Figure 3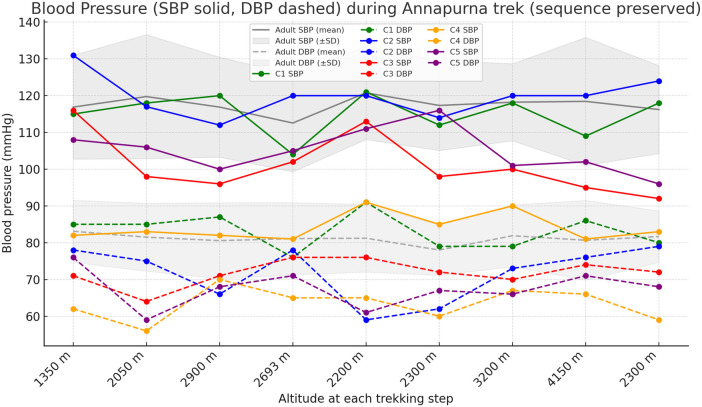 Figure 4
Figure 4| Patient | Diagnosis | Surgical procedures (type and year) | Time since last surgery (year) | Residual lesions |
|---|---|---|---|---|
| C-1 | PA/IVS | Pulmonary valvotomy and infundibulectomy (2003) | 21 | Mild to moderate PR and TR |
| C-2 | CoA with ASD | CoA repair (2011) | 13 | Mild AS |
| C-3 | ccTGA, UVH, DILV | PA banding (2012), Glenn (2013), ECC fontan without fenestration (2015) | 9 | Mild AR |
| C-4 | DORV with VSD, PS | Initial total correction (2012), Pulmonary valve replacement (2021) | 3 | Mild to moderate PR, Mild AR |
| C-5 | TGA with VSD | Arterial switch operation (2013) | 11 | Mild AR |
| Baseline altitude (1350 m) | Highest altitude (4150 m) | Δ | ||
|---|---|---|---|---|
| SpO2 (%) | CHD | 96.0 ± 2.1 | 86.2 ± 6.5 | −9.8 |
| Adults | 95.4 ± 1.3 | 87.3 ± 4.7 | −8.1 | |
| Heart rate (bpm) | CHD | 85.4 ± 6.9 | 103.2 ± 3.3 | +17.8 |
| Adults | 84.4 ± 12.4 | 80.2 ± 12.4 | −4.2 | |
| Systolic BP (mmHg) | CHD | 110.4 ± 18.0 | 101.4 ± 14.7 | −9.0 |
| Adults | 116.9 ± 14.1 | 118.4 ± 17.4 | +1.5 | |
| Diastolic BP (mmHg) | CHD | 71.3 ± 11.2 | 65.8 ± 9.6 | −5.5 |
| Adults | 79.4 ± 10.8 | 77.9 ± 11.6 | −1.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHigh Altitude and Hypoxia · Congenital Heart Disease Studies · Cardiovascular and Diving-Related Complications
Introduction
1
Congenital heart disease (CHD) is the most common birth defect, and advances in surgical and medical care have markedly improved survival, resulting in individuals reaching childhood, adolescence, and adulthood. Nevertheless, many children with CHD continue to face challenges beyond the operating room, particularly regarding exercise capacity and participation in physical activities. Exercise capacity in this population is frequently reported as lower than that of healthy peers, with reductions in peak oxygen uptake, oxygen pulse, and maximal work rates (1, 2). Such limitations may arise from residual anatomical lesions, impaired ventricular function, or reduced capacity for stroke volume augmentation after surgical correction (3).
Beyond physiological constraints, misperceptions of fragility and excessive protection often reinforce inactivity, further compromising physical and psychosocial development (4, 5). Children with CHD are sometimes excluded from physical activity or discouraged from pursuing physically demanding activities, which may contribute to reduced self-confidence and social isolation. Conversely, structured and supervised physical activity has been shown to improve exercise capacity, enhance resilience, and foster social integration (1, 4, 5). And recent randomized evidence indicates that exercise-based rehabilitation can increase overall physical activity levels and improve health-related quality of life in children with CHD (6).
Despite these recognized benefits, little is known about how children with surgically corrected CHD respond to environmental stressors such as high-altitude exposure. Exposure to hypobaric hypoxia provokes characteristic cardiopulmonary adaptation—including hyperventilation, sympathetic activation, tachycardia, and mild pulmonary vasoconstriction—that help maintain oxygen delivery under reduced ambient oxygen tension (7, 8) These responses may vary in children with repaired CHD depending on ventricular reserve, pulmonary vascular reactivity, and residual hemodynamic burden (3, 8). Understanding these mechanisms under hypoxic stress is essential for assessing safety and exercise feasibility in the context of high-altitude trekking in this vulnerable yet capable population.
Furthermore, most children with CHD reside at sea level and have no prior acclimatization experience, raising additional questions about their tolerance to rapid ascent and low-oxygen environments. Clinical data describing such real-world adaptations are scarce.
This study was designed as an exploratory observational analysis rather than a comparative trial. We investigated the physiological responses—oxygen saturation, heart rate, and blood pressure—of children with surgically corrected CHD during a high-altitude trekking expedition to the Annapurna Base Camp. By analyzing individual-level physiological trends of children with CHD during the high-altitude trek, we aimed to describe how these children adapt to hypobaric hypoxia in a real-world setting, providing preliminary insights into the safety and feasibility of such physical challenges.
Materials and methods
2
Study design
2.1
This was an exploratory observational study based on physiological monitoring data collected during a high-altitude trekking expedition for children with surgically corrected CHD and accompanying adults. Measurements were originally obtained as part of routine safety monitoring and were subsequently analyzed retrospectively.
Participants
2.2
The trekking team comprised children with surgically corrected congenital heart disease and accompanying healthy adults, including medical staffs and parents. All participants lived at sea level in Korea and had no prior experience of high-altitude exposure or acclimatization training.
The children had undergone definitive surgical repair 7–12 years before the expedition and were clinically stable in daily life. Although formal pre-expedition cardiology evaluations were not performed for every child, all were known to have no functional limitations in ordinary activities and had undertaken structured physical preparation for approximately one year, hiking nearly every week, including multiple supervised hikes and winter ascents in domestic mountains reaching elevations of around 1,700 m, to improve endurance and adaptation capacity before the expedition.
The medical staff accompanied the expedition both as participants and as safety supervisors. They were prepared to respond to emergencies and routinely evaluated the physical condition of all participants at each destination. Figure 1 presents a photograph of the expedition team in front of the Annapurna Base Camp sign.
Photograph of the expedition team at Annapurna Base Camp, comprising children with surgically corrected congenital heart disease (CHD), their parents, and medical staff.
Trekking course
2.3
An 11-day expedition to Annapurna Base Camp (maximum elevation 4,150 m) was conducted in Nepal between February 2 and 12, 2024. The course included both ascending and descending segments, rather than a simple upward profile, allowing gradual altitude gain and staged acclimatization.
The itinerary was deliberately designed to include approximately two additional days at intermediate altitudes to allow acclimatization or decent in case of altitude illness. However, no child experienced symptoms requiring schedule modification, and the trek was completed as planned.
Physiological monitoring
2.4
Physiological parameters—including oxygen saturation (SpO_2_; %), heart rate [HR; beats per minute (bpm)], and both systolic and diastolic blood pressure (SBP and DBP; mmHg)—were measured at designated elevation levels encountered during the trekking sequence. Participants rested for more than one hour before each measurement to minimize exertional effects. Portable finger-type pulse oximeter (MD300 C22) and an automated oscillometric blood pressure monitor (HEM-7156) were used for non-invasive monitoring. To ensure stabilized measurements after altitude gain, all variables were recorded after more than one hour of rest at each daily destination. Assessments were performed indoors or in sheltered using the same devices throught the expedition, warm environments whenever possible to minimize cold-induced artifacts.
SpO₂ and HR were obtained once after confirming a stable plethysmographic waveform. BP was measured once in the seated position using an appropriately sized cuff. All measurements were performed by three trained medical staff members.
Statistical analysis
2.5
Group means and standard deviations were calculated for CHD and control participants at each elevation level. Change (Δ) from the baseline (1,350 m) to highest altitude (4,150 m) were computed. Given the small sample size and observational nature of the study, no formal hypothesis testing was performed, and the results are presented descriptively.
For children with CHD, individual trajectories were examined to illustrate inter-individual variability, and adult data were presented separately to demonstrate general altitude-related patterns.
Ethics statement
2.6
Measurements were collected for safety monitoring during the trekking expedition and analyzed retrospectively. No additional interventions were performed beyond routine non-invasive monitoring. The requirement for institutional review board approval was waived in accordance with national and institutional regulations, as the study involved retrospective analysis of de-identified safety data. All participants provided written informed consent, with parental consent obtained for children. The study adhered to the principles of the Declaration of Helsinki.
Written informed consent was also obtained from the participants’ legal guardians for the publication of any potentially identifiable images or data included in this article.
Results
3
Study population and preparation
3.1
A total of fourteen participants, including five boys with surgically corrected congenital heart disease (mean age, 12.8 years) and nine healthy adults (mean age, 47.3 years), successfully completed the 11-day Annapurna Base Camp expedition to a maximum elevation of 4,150 m. No child experienced altitude sickness requiring medical intervention, cardiovascular events or required interruption of the trek.
Individual clinical characteristics—including diagnosis, surgical procedure, time since last surgery, and residual lesions on echocardiographic examination—are summarized in Table 1. The time since the last surgery ranged from 7 to 12 years, and all children were clinically stable in daily life without heart failure symptoms.
Oxygen saturation
3.2
At 1,350 m, the mean SpO_2_ was 96.0% ± 2.1% in the CHD group and 95.4% ± 1.3% in adults. At 4,150 m, the mean SpO_2_ declined to 86.2% ± 6.5% in children with CHD and 87.3% ± 4.7% in adults (Δ −9.8% vs. −8.1%). Individual SpO_2_ trajectories of the five children are displayed in Figure 2, illustrating heterogeneous but well-tolerated desaturation patterns that paralleled the overall trend observed in adults.
Individual oxygen saturation (SpO2) responses during the Annapurna trekking expedition. Oxygen saturation was measured sequentially at each trekking step while maintaining the original ascent and descent sequence. Colored solid line represents individual children with surgically corrected congenital heart disease, and the gray line and shaded area represents the mean ± SD of adult participants.
However, one child (C3) consistently showed lower absolute SpO_2_ values and a more pronounced decline across altitudes compared with the other participants.
Heart rate
3.3
The mean HR increased from 85.4 ± 6.9 bpm at 1,350 m to 103.2 ± 3.3 bpm at 4,150 m in children with CHD. In contrast, the adults showed a slight decline (84.4 ± 12.4 bpm–80.2 ± 12.4 bpm; Δ + 17.8 bpm vs. −4.2 bpm). Individual HR curves (Figure 3) showed a consistent chronotropic response across all children, indicating reliance on heart-rate augmentation to maintain cardiac output at higher altitude.
Heart rate responses during the Annapurna trekking expedition. Heart rate changes are shown in sequential trekking order. Colored solid line represents individual children with surgically corrected CHD, while the gray line and shaded area represents the mean ± SD of adult participants.
Blood pressure
3.4
Both SBP and DBP were measured and described. SBP decreased from 110.4 ± 18.0 mmHg at 1,350 m to 101.4 ± 14.7 mmHg at 4,150 m in children with CHD, whereas SBP remained similar in adults (116.9 ± 14.1 mmHg vs. 118.4 ± 17.4 mmHg; Δ −9.0 mmHg vs. +1.5 mmHg).
DBP showed a modest decline in children with CHD (71.3 ± 11.2 mmHg to 65.8 ± 9.6 mmHg; Δ −5.5 mmHg), while adults exhibited relatively little variation (79.4 ± 10.8 mmHg to 77.9 ± 11.6 mmHg; Δ −1.5 mmHg).
Individual SBP and DBP trajectories are shown in Figure 4, demonstrating mild, well-compensated reductions without hypotensive symptoms.
Systolic and diastolic blood pressure responses during the Annapurna trekking expedition. Systolic blood pressure (SBP; solid line) and diastolic blood pressure (DBP; dashed lines) are displayed for each child with surgically corrected CHD. The gray solid and dashed lines represent the adult mean SBP and DBP, respectively, with shaded areas indicating ± SD of adult participants.
Table 2 summarizes the mean physiological values at baseline (1,350 m) and at the highest altitude (4,150 m) for both groups.
Summary of changes
3.5
From the baseline to the highest altitude, both groups showed similar patterns of oxygen desaturation.
Children with CHD showed a more pronounced chronotropic response and modest declines in SBP and DBP, whereas adults showed little variation in cardiovascular parameters. These observations suggest that children with surgically corrected CHD were able to maintain overall hemodynamic stability at high altitude through heart rate augmentation and mild vascular relaxation.
Discussion
4
This study shows the feasibility and physiological safety of high-altitude trekking for children with surgically corrected CHD. All participants successfully completed the Annapurna Base Camp expedition without adverse clinical events. The physiological responses observed in this study provide preliminary insight into how this population adapts to hypobaric hypoxia during high-altitude trekking.
Exposure to reduced barometric pressure at altitude triggers characteristic cardiopulmonary responses, including hyperventilation, sympathetic activation, and mild pulmonary vasoconstriction, to maintain oxygen delivery despite ambient oxygen tension (7, 8). In this study, children with CHD showed these expected adaptive responses, suggesting preserved compensatory capacity despite their surgically repaired hearts. Previous exercise studies altitude have similarly shown that hypobaric hypoxia imposes persistent constraints on maximal oxygen uptake and cardiac performance, even after acclimatization (9, 10)
Between 1,350 m and 4,150 m, SpO_2_ decreased similarly in both groups (−9.8% in CHD vs. −8.1% in adults), suggesting that arterial oxygenation was maintained to a similar extent under hypoxic stress. One child (C3) demonstrated lower absolute SpO_2_ values and a slightly larger decline with altitude compared with the other children. This child had univentricular physiology and had undergone extracardiac conduit Fontan operation, and individuals with Fontan circulation are known to have modestly lower baseline arterial oxygen saturation due to passive pulmonary blood flow and mild systemic venous desaturation. These features may contribute to a more pronounced desaturation response under hypobaric hypoxia, while the overall trend remained consistent with the rest of the group.
Children with CHD showed a more pronounced chronotropic response, whereas adults demonstrated little variation in HR. The more pronounced increase in HR observed in the children is consistent with known pediatric cardiovascular physiology, in which cardiac output during physiological stress is achieved predominantly through chronotropic augmentation rather than stroke volume expansion (11).
Children with CHD also exhibited mild decreases in SBP and DBP, whereas adults showed little variation in cardiovascular parameters. These parallel reduction in SBP and DBP may reflect adaptive vasodilation under hypobaric hypoxia, which has been described as part of normal altitude acclimatization (7, 8).
Because altitude-related physiological responses may exhibit delayed components, we acknowledge that dwell times at each elevation were not identical during the trekking itinerary. However, all measurements were performed indoors after more than one hour of rest using same devices and trained personnel, minimizing the influence of delayed physiological adjustment on the recorded values.
Our observations align with previous studies reporting reduced exercise capacity in children and adolescents with CHD compared with healthy peers (2, 4, 12–14), often attributed to limited stroke volume reserve or residual hemodynamic burden (3, 7). The present findings extend these findings by providing real-world physiological data under hypobaric conditions, showing that, when adequately prepared and supervised, children with repaired CHD can exhibit effective cardiopulmonary adaptations even during physical demanding activity.
From a clinical perspective, these results reinforce current AHA and ESC guidelines, which emphasize that most children with CHD can safely engage in appropriately designed physical activity (5, 15). The findings also complement recent randomized evidence demonstrating that structured exercise-based rehabilitation can improve physical activity levels and health-related quality of life in this population (6). Together, this study adds preliminary evidence supporting outdoor and endurance-type programs aimed at improving fitness, confidence, and social participation in this population.
This study has several limitations, which must be acknowledged. The small sample size and heterogeneity of diagnoses limit generalizability. The adult participants were older rather than age-matched, so direct comparisons should be interpreted cautiously. The observational design precludes causal inference. Future work including age-matched cohorts, detailed cardiopulmonary exercise testing, and echocardiographic or hemodynamic monitoring could better characterize altitude adaptation mechanisms in this group. Although all physiological measurements were standardized and obtained indoors after more than one hour of rest to minimize short-term variability, minor differences in dwell time at each altitude were inherent to the trekking itinerary. This residual variation is unlikely to have materially influenced the overall physiological patterns observed. In addition, repeated measurements at each elevation were not feasible in this field setting, and individual differences in physical conditioning may have contributed to subtle variability across participants.
Beyond physiological findings observed during this trek, this study highlights the psychosocial dimensions of living with CHD. Misperceptions of fragility and excessive protection can perpetuate inactivity and social isolation, whereas structured opportunities for physical achievement may foster resilience, and self-efficacy.
The motto of the Korea Congenital Heart Disease Patients Group—“We are Different, We are not Different”—captures this dual reality: although these children are born with unique challenges, proper preparation and support enable them to thrive their peers.
Conclusion
5
Children with surgically corrected CHD successfully completed a high-altitude trekking expedition and showed preserved oxygenation and well-compensated cardiovascular responses during trekking. These findings may support the possibility that, when adequately trained and medically supervised, such children are capable of safely participating in physical demanding activities. Future collaborative studies may help establish structured exercise guidelines tailored to this growing population. Beyond physiology, this study highlights the broader message that although children with CHD are born different, with appropriate surgical correction, preparation, and supervision, they are not different in their ability to adapt, endure, and thrive alongside their peers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duppen N Takken T Hopman MT ten Harkel AD Dulfer K Utens EM Systematic review of the effects of physical exercise training programmes in children and young adults with congenital heart disease. Int J Cardiol. (2013) 168(3):1779–87. 10.1016/j.ijcard.2013.05.08623746621 · doi ↗ · pubmed ↗
- 2Villaseca-Rojas Y Varela-Melo J Torres-Castro R Vasconcello-Castillo L Mazzucco G VilaróJ Exercise capacity in children and adolescents with congenital heart disease: a systematic review and meta-analysis. Front Cardiovasc Med. (2022) 9:874700. 10.3389/fcvm.2022.87470035600470 PMC 9114479 · doi ↗ · pubmed ↗
- 3Baumgartner H De Backer J Babu-Narayan SV Budts W Chessa M Diller GP 2020 ESC guidelines for the management of adult congenital heart disease. Eur Heart J. (2021) 42(6):563–645. 10.1093/eurheartj/ehaa 55432860028 · doi ↗ · pubmed ↗
- 4Gomes-Neto M Saquetto MB da Silva CM Conceição CS Carvalho VO. Impact of exercise training in aerobic capacity and pulmonary function in children and adolescents after congenital heart disease surgery: a systematic review with meta-analysis. Pediatr Cardiol. (2016) 37(2):217–24. 10.1007/s 00246-015-1270-x 26396114 · doi ↗ · pubmed ↗
- 5Longmuir PE Brothers JA de Ferranti SD Hayman LL Van Hare GF Matherne GP Promotion of physical activity for children and adults with congenital heart disease: a scientific statement from the American Heart Association. Circulation. (2013) 127(21):2147–59. 10.1161/CIR.0b 013e 318293688 f 23630128 · doi ↗ · pubmed ↗
- 6Amedro P Gavotto A Huguet H Souilla L Huby AC Matecki S Early hybrid cardiac rehabilitation in congenital heart disease: the QUALIREHAB trial. Eur Heart J. (2024) 45(16):1458–73. 10.1093/eurheartj/ehae 08538430485 PMC 11032713 · doi ↗ · pubmed ↗
- 7Bärtsch P Gibbs JS. Effect of altitude on the heart and the lungs. Circulation. (2007) 116(19):2191–202. 10.1161/CIRCULATIONAHA.106.65079617984389 · doi ↗ · pubmed ↗
- 8Parati G Agostoni P Basnyat B Bilo G Brugger H Coca A Clinical recommendations for high altitude exposure of individuals with pre-existing cardiovascular conditions: a joint statement by the European Society of Cardiology, the council on hypertension of the European Society of Cardiology, the European society of hypertension, the international society of mountain medicine, the Italian society of hypertension and the Italian society of mountain medicine. Eur Heart J. (2018) 39(17):1546–54. 10.1093/eurh · doi ↗ · pubmed ↗