Suprascapular nerve entrapment syndrome caused by a spinoglenoid notch cyst with a concomitant giant lipoma: a case report
Zaichao Ma, Mengxue Guan, Maimaitiyibubaji Abudukadier, Xiaoping Han, Tao Huang, Zengqiang Yang, Biao Li, Yong Cui

TL;DR
A rare case of shoulder nerve compression caused by a cyst and lipoma highlights the importance of early diagnosis for effective treatment.
Contribution
This case report presents a unique 'double-crush' suprascapular nerve entrapment caused by a spinoglenoid notch cyst and giant lipoma.
Findings
A paralabral cyst occupied both the suprascapular and spinoglenoid notches, causing rapid neurological deficits.
Isolated infraspinatus weakness and atrophy were observed in a patient with no clear traumatic history.
Early recognition and systematic evaluation led to successful management and neurological recovery.
Abstract
Suprascapular nerve entrapment is a cause of shoulder pain and dysfunction, often complicated by symptomatic overlap with other shoulder pathologies. Entrapment most commonly occurs at two anatomical constrictions: the suprascapular notch and the spinoglenoid notch. Compression of the nerve's inferior branch at the spinoglenoid notch by a paralabral cyst, leading to isolated infraspinatus weakness and atrophy, is a relatively common pattern. Diagnosis relies on a detailed physical examination, multimodal imaging evaluation including MRI and ultrasound, and confirmation by electromyography. For patients who do not respond to conservative management or who have definitive space-occupying compression, surgical decompression is an effective treatment option. This is the case of a 27-year-old man presenting with progressive right shoulder weakness and pain over just one month, already…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
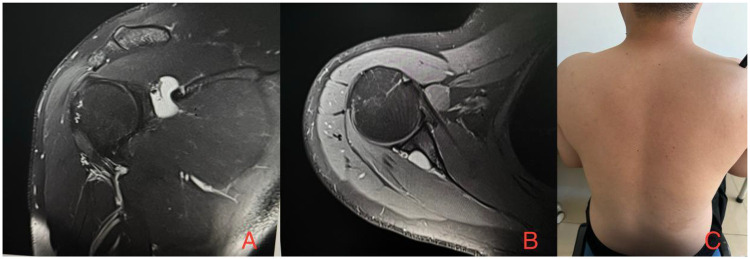 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Nerve Injury and Rehabilitation
Background
Suprascapular nerve entrapment is a recognized cause of shoulder pain, accounting for approximately 2% of cases. Its diagnosis is frequently delayed or missed during initial assessment due to symptomatic overlap with other shoulder pathologies and the need for differentiation from cervical spine disorders (1, 2). This diagnostic challenge stems from its complex and multifactorial etiology, which includes traumatic causes such as scapular fractures and glenoid labral tears, static compression from anatomical variations like the suprascapular transverse ligament or the spinoglenoid ligament, and space-occupying lesions such as ganglion cysts and tumors (3). The suprascapular nerve originates from the upper trunk of the brachial plexus, traverses the suprascapular notch to innervate the supraspinatus muscle and provide sensory fibers to the shoulder joint capsule, and then its inferior branch passes through the spinoglenoid notch to supply the infraspinatus muscle. Entrapment most commonly occurs at either the suprascapular notch or the spinoglenoid notch, with the former being more frequent (2, 4–6). Compression of the inferior branch at the spinoglenoid notch by a ganglion cyst is relatively common, while concomitant compression by fatty tissue is less frequently observed (7). Classical classification systems primarily distinguish between entrapment at the suprascapular notch, affecting the main nerve trunk, and at the distal spinoglenoid notch, affecting only the infraspinatus branch, with significant differences in clinical presentation, imaging features, and treatment strategies between the two types (8). Recent work by Al-Redouan et al. has further elucidated the pathogenic mechanisms and clinical implications of this classification (9–11). The radiating pain from suprascapular nerve entrapment typically localizes around the lateral scapula and superior shoulder. Proximal brachial plexus pain also differs in localization from cervical radiculopathy and pain from distal terminal nerve branches. The nerve is most commonly compressed at two anatomical sites: the suprascapular notch and the spinoglenoid notch. Compression at the spinoglenoid notch typically results in infraspinatus weakness and atrophy. Clinically, patients present with posterior shoulder pain and functional limitations. Magnetic resonance imaging is the key modality for confirming the presence of a ganglion cyst and assessing the degree of nerve compression. Currently, ultrasound is an emerging and increasingly utilized diagnostic tool (12–14). Furthermore, nerve conduction velocity/electromyography studies are often integral to the overall diagnostic workup. For patients who do not respond to conservative management or who have a cyst definitively associated with nerve compression, surgical intervention is recommended—encompassing open or arthroscopic decompression, with or without cyst aspiration (15–18). This case presents an instance of suprascapular nerve entrapment where a cyst occupied the entire suprascapular nerve pathway, concurrently compressing both the suprascapular and spinoglenoid notches. The patient achieved a favorable recovery following arthroscopic decompression combined with open neurolysis.
Case report
A 27-year-old male patient was admitted due to “right shoulder pain with limited movement for one month.” The patient is a young male with an insidious onset. One month ago, he developed persistent dull pain in the right shoulder joint without an obvious cause, which did not radiate elsewhere but was accompanied by progressively worsening limitation of shoulder flexion and abduction. The relationship between pain and activity was clear: it significantly worsened with activity and markedly improved with rest. Physical examination revealed mild hollowing of the infraspinatus fossa of the right shoulder, suggesting possible atrophy of the infraspinatus muscle. The muscle strength of external rotation and abduction of the right shoulder joint was both grade 3, significantly weaker than on the healthy side. Tenderness was present at the spinoglenoid notch, and positive findings on the abduction resistance test, cross-arm test, and scapular traction test all indicated involvement of the suprascapular nerve. Electromyography showed a significantly reduced amplitude of the compound muscle action potential (CMAP) in the infraspinatus muscle during suprascapular nerve motor conduction studies, while findings for the supraspinatus muscle were largely normal. Ultrasound revealed a well-defined, regularly shaped unilocular hypoechoic cystic structure within the deep muscle groups of the right shoulder. It clearly demonstrated signs of the nerve being elevated, displaced, or compressed and flattened by the cyst. MRI of the right shoulder displayed a unilocular abnormal high-signal focus at the spinoglenoid notch, with clear boundaries and close anatomical relationships to the suprascapular nerve and blood vessels. Based on imaging and anatomical correlations, this case clearly demonstrates a cyst occupying the entire suprascapular nerve pathway, compressing both the suprascapular notch and the spinoglenoid notch, resulting in suprascapular nerve entrapment (Figure 1).
MRI of the right shoulder demonstrates a well-defined, unilocular abnormally hyperintense lesion (cyst) measuring approximately 2 cm × 2 cm at the spinoglenoid notch, which is in close proximity to the suprascapular nerve and adjacent vessels. (A), Coronal view. (B), Axial view. (C) Preoperative visual inspection revealed a mild depression in the right infraspinous fossa.
Under general anesthesia, the patient was placed in the beach-chair position. Conventional shoulder arthroscopy was performed via posterior and anterosuperior portals to examine the glenohumeral joint and subacromial space. The glenoid labrum was intact without tear, though slightly frayed at the margin. The supraspinatus and infraspinatus tendons were intact. Adhesions were observed between the middle glenohumeral ligament and the subscapularis tendon. The fascia of the deltoid and trapezius was exposed, followed by blunt dissection of the trapezius fascia. The supraspinatus and infraspinatus muscles were separated, and the infraspinatus was mobilized. The posterior glenoid cavity and spinoglenoid notch were exposed, revealing a cyst measuring approximately 2 cm × 2 cm, with adipose tissue visible posteriorly. The suprascapular nerve was severely compressed and appeared pale locally.The cyst wall was resected with an arthroscopic shaver, and viscous, yellowish, jelly-like fluid was released. Subsequently, a lipoma-like mass was identified posteriorly and inferiorly to the cyst. Due to limited operating space, the arthroscope was withdrawn. The skin over the scapular spine was cleansed with alcohol, and an incision was made along the spine through the skin and subcutaneous tissue. Hemostasis was achieved with electrocautery. Part of the trapezius was incised, and blunt dissection was performed to expose the supraspinatus muscle. The posterior glenoid and spinoglenoid notch were subsequently exposed, revealing the lipoma-like adipose mass posterior to the original cyst attachment site, which was completely excised. Hemostatic material was applied to the wound and joint cavity for local hemostasis. The surgical site was irrigated with normal saline. The muscle and subcutaneous layers were closed in layers with absorbable sutures. The skin around the incision was disinfected again with alcohol and closed with intradermal sutures. The arthroscopic portal sites were closed with full-thickness sutures.
Postoperatively, the rehabilitation department was consulted to assist with functional exercise rehabilitation. Shoulder abduction and external rotation strength gradually recovered to grade 5. At the 6-month outpatient follow-up, shoulder motion had returned to normal with good stability. Follow-up MRI showed complete resolution of the spinoglenoid notch cyst and adipose tissue.
Discussion
This case report describes the typical presentation of isolated shoulder external rotation weakness and infraspinatus atrophy due to compression of the inferior branch of the suprascapular nerve by a spinoglenoid notch cyst. Arthroscopic exploration revealed no associated labral injury, and the cyst contained adipose tissue, a finding that differs from the common mechanism of cyst formation secondary to labral tears (3). In contrast to most reports in the literature, where spinoglenoid cysts are associated with SLAP lesions or posterior labral tears, isolated cysts without an obvious labral injury, as seen in this case, have also been reported, with their etiology possibly involving synovial fluid extrusion through a labral recess or a microscopic channel (6). This finding suggests that cyst compression remains a possible etiology for suprascapular nerve entrapment even when conventional MRI does not show a definitive labral tear. The diagnostic and therapeutic process in this case adds several insights to the existing literature. Diagnostically, it reinforces the value of combining targeted physical examination—such as specific external rotation strength testing and inspection of the infraspinatus fossa—with multimodal imaging (MRI for definitive identification of the mass, ultrasound for dynamic nerve assessment, and electromyography to confirm nerve injury) (3, 19). This approach is particularly useful for early or atypical presentations, helping to avoid misdiagnosis as common cervical or shoulder soft-tissue disorders. Therapeutically, for cysts with no clear communication to the joint cavity and containing atypical components, arthroscopic exploration combined with limited open excision may be a reasonable option. This combined technique allows for assessment and management of possible concomitant intra-articular pathology while ensuring, via an open approach, complete excision of the cyst, particularly one with atypical contents, offering distinct advantages compared to isolated arthroscopic decompression or open surgery alone (20, 21). The patient in this case was treated with arthroscopic exploration and limited open excision, and at the 6-month follow-up, demonstrated significant symptomatic relief and excellent functional recovery. This aligns with literature reporting favorable neurological outcomes following early surgical decompression (17, 20, 21). Especially for patients with existing muscle atrophy but a relatively short symptom duration, timely relief of compression creates favorable conditions for neural recovery. A 2022 review also noted that the degree of post-decompression strength recovery is inversely correlated with the duration of preoperative nerve compression and the severity of muscle atrophy, underscoring the importance of early diagnosis and intervention (22). This study has certain limitations. First, it is a single-center case report, and caution should be exercised in generalizing the conclusions. Second, the patient's follow-up period was only 6 months; longer-term follow-up would be helpful to assess the final functional plateau and potential cyst recurrence.
Conclusion
This report highlights the classic clinical and imaging features of an isolated compression neuropathy of the inferior branch of the suprascapular nerve by a spinoglenoid notch cyst. The case of a young man without a history of trauma, who presented with progressive isolated shoulder external rotation weakness and infraspinatus atrophy, serves as a well-localized diagnostic paradigm. The convergence of a characteristic clinical presentation, pathognomonic MRI findings, and confirmatory electrodiagnostic and ultrasonographic studies provides a complete chain of evidence. This case emphasizes that this diagnosis should be considered in patients presenting with shoulder pain and predominant external rotation weakness, even in the absence of a clear traumatic history or imaging evidence of a labral tear. Early evaluation through meticulous physical examination and multimodal imaging, followed by an individualized surgical approach tailored to the cyst's characteristics and the intra-articular findings, can lead to favorable neurological recovery. Further studies are needed to clarify the pathogenesis and optimal management strategy for such isolated cysts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moen TC Babatunde OM Hsu SH Ahmad CS Levine WN. Suprascapular neuropathy: what does the literature show? J Shoulder Elbow Surg. (2012) 21(6):835–46. 10.1016/j.jse.2011.11.03322445163 · doi ↗ · pubmed ↗
- 2Prenaud C Loubeyre J Soubeyrand M. Decompression of the suprascapular nerve at the suprascapular notch under combined arthroscopic and ultrasound guidance. Sci Rep. (2021) 11(1):18906. 10.1038/s 41598-021-98463-134556759 PMC 8460809 · doi ↗ · pubmed ↗
- 3Katsuura Y Hill AJ 4th Colón LF Dorizas JA. MRI diagnosis of suprascapular neuropathy using spinoglenoid notch distension. Radiol Med. (2019) 124(7):643–52. 10.1007/s 11547-019-01005-z 30835024 · doi ↗ · pubmed ↗
- 4Boykin RE Friedman DJ Higgins LD Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. (2010) 92(13):2348–64. 10.2106/JBJS.I.0174320926731 · doi ↗ · pubmed ↗
- 5Ayik G Kolac UC Kaymakoglu M Mc Farland E Huri G. Dark side of the shoulder: suprascapular and axillary nerve compressions. Int Orthop. (2025) 49(5):1153–65. 10.1007/s 00264-025-06465-940082300 PMC 12003475 · doi ↗ · pubmed ↗
- 6Joo YB Lee WY Chung HJ. Suprascapular nerve entrapment caused by a large hematoma of the scapula: a case report. BMC Musculoskelet Disord. (2023) 24(1):589. 10.1186/s 12891-023-06723-037468872 PMC 10354896 · doi ↗ · pubmed ↗
- 7Knudsen ML Hibbard JC Nuckley DJ Braman JP. Anatomic landmarks for arthroscopic suprascapular nerve decompression. Knee Surg Sports Traumatol Arthrosc. (2016) 24(6):1900–6. 10.1007/s 00167-014-3149-424990663 · doi ↗ · pubmed ↗
- 8Cummins CA Messer TM Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. (2000) 82(3):415–24. 10.2106/00004623-200003000-0001310724234 · doi ↗ · pubmed ↗