Postoperative exercise rehabilitation and patient experience among breast cancer survivors under the “Healthy China” initiative: an integrative review
Binyu Zhao, Xuefei Li, Cong Fu, Ying Bian, Yafei Gong, Lina Zhu, Xiaochun Wang

TL;DR
This review examines how post-surgery exercise helps breast cancer survivors in China, highlighting the need for personalized and supported rehabilitation programs.
Contribution
The study provides a comprehensive review of exercise rehabilitation for breast cancer survivors under the 'Healthy China' initiative, emphasizing localized and interdisciplinary approaches.
Findings
Exercise interventions improve physical function and reduce lymphedema risk among breast cancer survivors.
Combined exercise modalities are more effective than single-mode approaches in rehabilitation.
Patient adherence is often hindered by side effects and lack of individualized support.
Abstract
This integrative review synthesizes current evidence on postoperative exercise rehabilitation and patient experiences among breast cancer survivors, aiming to inform the development of scientific, standardized, and contextually appropriate rehabilitation protocols under the “Healthy China” initiative. A comprehensive literature search was conducted across seven Chinese and English databases, identifying 23 eligible studies published between 2015 and 2024, including randomized controlled trials and qualitative research. Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT). The findings revealed substantial heterogeneity in exercise prescription parameters and a lack of unified guidelines. Exercise interventions were generally effective in improving physical function, reducing lymphedema risk, and enhancing psychological well-being, yet patient experiences…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
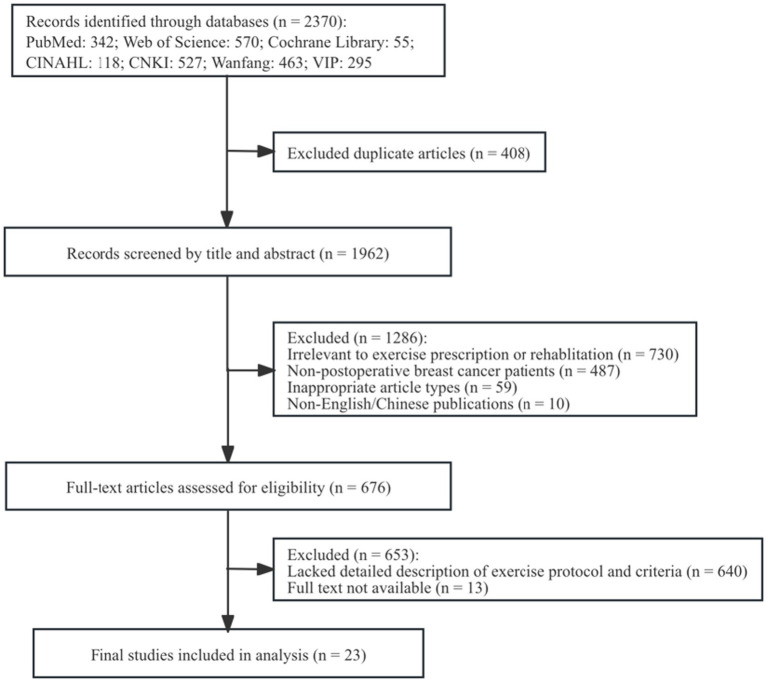 Figure 1
Figure 1| No. | Author(s) | Title | Year | Country | Sample size | Study design | Quality score |
|---|---|---|---|---|---|---|---|
| 1 |
| Design and implementation of exercise prescription to prevent upper limb lymphedema in breast cancer survivors | 2021 | China | 106 | Quasi-experimental (non-randomized) | 100% |
| 2 |
| Effects of forearm resistance exercises on breast cancer-related lymphedema using segmental bioelectrical impedance analysis: a pilot RCT | 2024 | Korea | 18 | Randomized controlled trial | 80% |
| 3 |
| Does a resistance training program affect between-arms volume difference and shoulder disabilities in female breast cancer survivors? secondary outcomes of the EFICAN trial | 2023 | Spain | 60 | Randomized controlled trial | 100% |
| 4 |
| Application of “Internet+” home-based exercise prescription in postoperative rehabilitation of breast cancer patients | 2023 | China | 117 | Randomized controlled trial | 100% |
| 5 |
| Mobile health and supervised rehabilitation versus mobile health alone in breast cancer survivors: RCT | 2020 | Spain | 80 | Randomized controlled trial | 100% |
| 6 |
| Design and application of a virtual reality rehabilitation system for postoperative breast cancer patients | 2018 | China | 76 | Randomized controlled trial | 100% |
| 7 |
| Application of “shoulder joint eight movements” in postoperative functional training for breast cancer patients | 2021 | China | 102 | Randomized controlled trial | 100% |
| 8 |
| The recovery of reaching movement in breast cancer survivors: two different rehabilitative protocols in comparison | 2021 | Italy | 66 | Randomized controlled trial | 100% |
| 9 |
| Exercise: a path to wellness during adjuvant chemotherapy for breast cancer? | 2015 | Norway | 27 | Qualitative study | 100% |
| 10 |
| Finding the optimal exercise dose while living with cancer-related fatigue: a qualitative study | 2023 | USA | 11 | Qualitative study | 100% |
| 11 |
| Physical activity and exercise self-regulation in cancer survivors: a qualitative study | 2018 | USA | 35 | Qualitative study | 100% |
| 12 |
| Preferences for mHealth physical activity interventions during chemotherapy for breast cancer: a qualitative evaluation | 2020 | USA | 30 | Qualitative study | 100% |
| 13 |
| Multidisciplinary rehabilitation program after breast cancer: benefits on physical function, anthropometry, and quality of life | 2017 | Belgium | 209 | Non-randomized controlled trial | 100% |
| 14 |
| Post-cancer rehabilitation: multidisciplinary exercise program organization and feasibility | 2024 | France | 655 | Retrospective review | 100% |
| 15 |
| Effects of aerobic and resistance exercise on metabolic syndrome, sarcopenic obesity, and circulating biomarkers in overweight or obese breast cancer survivors: a randomized controlled trial | 2018 | USA | 100 | Randomized controlled trial | 100% |
| 16 |
| Reduction of breast lymphedema secondary to breast cancer: a randomized controlled exercise trial | 2020 | Australia | 88 | Randomized controlled trial | 100% |
| 17 |
| The impact of online yoga on sleep and quality of life in women with breast cancer: a randomized trial | 2024 | Germany | 173 | Randomized controlled trial | 100% |
| 18 |
| The analgesic effect of resistance training after breast cancer (ANTRAC): a randomized controlled trial | 2022 | Denmark | 20 | Randomized controlled trial | 80% |
| 19 |
| Effects of a multimodal training program on muscle deoxygenation in women with breast cancer: a randomized controlled trial | 2022 | France | 32 | Randomized controlled trial | 80% |
| 20 |
| The health effects of Baduanjin exercise in breast cancer survivors in China: a randomized, controlled, single-blind trial | 2019 | China | 86 | Randomized controlled single-blind trial | 100% |
| 21 |
| Effects of exercise therapy dosing schedule on impaired cardiorespiratory fitness in patients with primary breast cancer: a randomized controlled trial | 2020 | USA | 174 | Randomized controlled trial | 100% |
| 22 |
| Early implementation of exercise to facilitate recovery after breast cancer surgery: a randomized clinical trial | 2024 | Korea | 56 | Randomized controlled trial | 100% |
| 23 |
| Application of a progressive exercise prescription in breast cancer patients undergoing postoperative radiotherapy | 2024 | China | 132 | Non-randomized controlled trial | 100% |
| Author | Population | Intervention | Comparison | Outcome | Study design |
|---|---|---|---|---|---|
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | The upper limb strength and cardiopulmonary endurance were improved, and the incidence of lymphedema was reduced. | Quasi-experimental study (non-randomized). | |
|
| Patients with unilateral breast cancer-related lymphedema; Intervention group ( | Control group ( | Resistance training of forearm may be effective in the management of lymphedema | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | Resistance training may improve shoulder function in breast cancer survivors. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; The intervention group ( | Control group ( | The “Internet+” home-based exercise prescription is convenient, visual, and user-friendly, significantly improving adherence and reducing the incidence of upper limb lymphedema while enhancing shoulder mobility. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | It is superior to the simple mobility health program in improving quality of life, upper limb function and symptom management. | Randomized controlled trial. | |
|
| Patients with unilateral or bilateral modified radical mastectomy; Intervention group ( | Control group ( | VR-assisted rehabilitation significantly improved shoulder, increased training adherence, and reduced limb edema. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | The patients’ compliance was improved, the upper limb function was restored, and the pain, daily activity ability, range of motion and muscle strength were improved. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; The intervention group ( | The control group ( | The pain was relieved and the function of upper limb was improved. The individualized rehabilitation showed better performance in the quality of movement. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | Multidisciplinary rehabilitation programs have achieved significant improvements in most aspects of physical function, body composition, and quality of life. | Non-randomized controlled trial. | |
|
| Post-operative patients with breast cancer; ( | Control group ( | The program is feasible, sustainable and delivers positive treatment outcomes for a large number of patients | Retrospective review. | |
|
| 100 overweight or obese Post-operative patients with breast cancer; the intervention group ( | The control group ( | Significantly improved metabolic syndrome, sarcopenic obesity, and related biomarkers in overweight or obese breast cancer survivors. | Randomized controlled trial. | |
|
| Women with stable breast cancer-related lymphedema; Exercise group ( | Control group ( | Aerobic and resistance training program was safe for patients with secondary breast cancer-related lymphedema and significantly reduced symptoms and physical indicators without exacerbating swelling. | Single-blind randomized controlled | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | Online yoga is a safe, low-cost, and easily implementable intervention that effectively improves dyspnea, physical activity levels, and sleep quality. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | The pain threshold and maximum muscle strength were increased, and the mechanical pain sensitivity was decreased. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer who have received adjuvant chemotherapy; Intervention group ( | Control group ( | It improved muscle oxygenation, muscle strength, endurance and reduced fatigue. | Randomized controlled trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | Improved heart rate variability, shoulder joint range of motion, depressive symptoms, and quality of life | Randomized, single-blind controlled trial. | |
|
| Postmenopausal breast cancer patients with impaired VO₂peak; Standard-dose group ( | The control group ( | Better tolerance to non-linear motion, significantly improved quality of life and reduced fatigue | Parallel-group randomized controlled trial. | |
|
| Early-stage postoperative patients with breast cancer; Intervention ( | Control ( | The shoulder joint function, physical activity level and quality of life were improved. | Parallel-group, two-arm randomized clinical trial. | |
|
| Post-operative patients with breast cancer; Intervention group ( | Control group ( | The incidence of upper limb lymphedema was decreased after the operation. | Non-randomized controlled trial |
| Parameter category | Strength indicator | Effective range in original study | Number of studies participated in | Efficacy consistency assessment basis |
|---|---|---|---|---|
| Aerobic exercise intensity | HRR | 40–60% HRR ( | 2 | Middle: The effective range of the report is wide (40–85%), but the number of studies is small. |
| RPE | RPE 9–13 ( | 3 | High: All three RPE-based studies reported efficacy in the ‘mild to moderate’ range. | |
| HRmax | 40–60% HRmax ( | 1 | Cannot evaluate: Only 1 study used. | |
| Resistance exercise intensity | 1-RM | 40–50% 1RM → 50–70% 1RM ( | 5 | High: All five studies demonstrated effectiveness within the 40–80% 1RM range, with most employing progressive overload. |
| RM | 10–12 RM ( | 1 | Cannot evaluate: Only 1 study used. | |
| Progression plan | Strength progress | Increase 5–10% of 1RM every 1–2 weeks ( | 7 | High: All 7 studies describing progress programs used progressive intensity increases and reported positive effects. |
| Duration progress | Add 5–10 min every 1–2 weeks ( | 2 | Middle: The number of studies describing this approach is small, but the direction is consistent. |
| Exercise intervention model | Studies | Upper limb function | Lymphedema (improved/reported) | Quality of life (improved/reported) | Adherence (completion/dropout) |
|---|---|---|---|---|---|
| combined mode (aerobic + resistance, etc.) | 8 | 7/7 | 4/4 | 1/2 | Completion rates:>80% ( |
| Single mode: resistance training | 4 | 3/4 | 3/3 | 0/0 | Completion rate: 100% ( |
| single mode: aerobic training | 1 | 0/0 | 0/0 | 0/0 | Completion rate: 82% ( |
| Traditional physical and mental exercises (Baduanjin, yoga, etc.) | 3 | 2/2 | 1/1 | 3/3 | Completion rate: 89% ( |
| Digital/Remote Guidance | 3 | 3/3 | 2/2 | 1/2 | Completion rate: 92.11% ( |
| Theme | Category | Illustrative quote | Number of studies participated in |
|---|---|---|---|
| Positive Impact of Exercise on Physical and Mental Health | Physical health | “I had been down and sorry for myself, thinking life was terrible… Then I realized sitting around feeling sorry would not help. If I went out and did something and thought positively, I’d feel better.” — | 2 items ( |
| “I felt energized and happy… more alert and ready to take on the day.” — | |||
| Mental health | “After I finish exercising, I usually feel energized… my mood is definitely better; I feel like my mind works better when I exercise.” — | 3 items ( | |
| “It feels amazing when you realize you have done it—you are sticking with it—and you are part of a study focusing on physical activity. It makes me feel like I’m in control and that things will get better.” — | |||
| “I rewarded myself with a chocolate bar and a piece of cake—and I felt great, no guilt at all.” — | |||
| Exploring and Adjusting Exercise Dose | Treatment-related barriers | “I experienced menopausal symptoms during chemo—hot flashes, sweating, and hair loss—which made me feel really uncomfortable. Exercising during hot flashes can feel awful.” — | 2 items ( |
| “I was exhausted for days. Not just the first day—also the second, and third. I did not realize how tired I’d be.” — | |||
| Goal setting | “I just wanted to become more active. That helped me get back into my routine, more than doing specific exercises.” — | 3 items ( | |
| “Participating in this program, going out for walks—I see it as something I’m doing to get better.” — | |||
| “It’s always about what your previous baseline was, and what your new baseline is… It’s frustrating and depressing.” — | |||
| Finding the right dose | “Every day I wonder: is this too much, or just right?” — | 3 items ( | |
| “Programs should account for side effects and how patients respond, while encouraging them to stay active. Toward the end of treatment, side effects worsen. Some days rest may be better than exercise.” — | |||
| “I felt something tight in my arm. After using the resistance band a couple of times, it went away. I still feel a little tightness sometimes, but the exercise helps.” — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Lymphatic System and Diseases · Nutrition and Health in Aging
Introduction
1
Breast cancer is one of the most common malignancies among women (Sung et al., 2021). Although advances in comprehensive treatment have significantly extended survival, a range of postoperative complications continue to pose serious challenges to patients’ quality of life (Ghanei Gheshlagh et al., 2022). Among these, upper limb dysfunction and lymphedema are particularly prevalent, leading not only to reduced capacity for daily activities but also to considerable psychological distress, including anxiety and depression, which hinder patients’ return to normal life and social participation (Wu P. P. et al., 2023). Evidence shows that scientifically designed exercise interventions can effectively improve limb function and reduce the incidence of lymphedema (Feng et al., 2024; Liu et al., 2023). Domestic and international research has explored various forms of rehabilitation: resistance training to enhance muscle function by overcoming external resistance, such as using equipment and resistance bands (Li et al., 2018; Wu M. L. et al., 2023), aerobic exercise to improve cardiopulmonary endurance through sustained rhythmic activity, such as brisk walking or cycling (Dieli-Conwright et al., 2018; Huang et al., 2023), Flexibility training through stretching body parts to increase joint mobility (Liu et al., 2021), in addition, there are traditional Chinese sports that emphasize the unity of body and mind and slow movements, such as Baduanjin and Taijiquan (Liu et al., 2019; Wang et al., 2019). Under the “Healthy China 2030″ initiative, which emphasizes the integration of medicine and physical activity, studies have demonstrated that a 12-week exercise prescription can significantly enhance muscle strength and cardiopulmonary endurance in breast cancer patients (Liu et al., 2021). Furthermore, home exercise prescriptions based on “Internet+” technology—personalized workout plans created by healthcare professionals for patients through digital platforms like smart wearables and mobile apps, supported by remote monitoring and guidance—have been proven to significantly improve patients’ exercise adherence (Jiang et al., 2023).
However, significant challenges remain in the clinical application of exercise prescriptions. On one hand, there is no consensus on standardized implementation guidelines either domestically or internationally. Core parameters such as frequency, intensity, type, and duration vary widely across studies, leaving healthcare professionals without clear guidance when designing and implementing rehabilitation programs (Dieli-Conwright et al., 2018; Drozd et al., 2024). This lack of standardization compromises both the scientific basis and effectiveness of exercise interventions. On the other hand, common clinical issues such as insufficient individualization of exercise plans and poor patient adherence persist. Approximately 30% of patients report fear of exercise (Chang et al., 2024), and treatment-related side effects such as fatigue and pain further reduce patients’ motivation and continuity in participating in exercise rehabilitation, significantly limiting its benefits (Chen et al., 2022).
Due to significant heterogeneity in existing literature regarding exercise intervention protocols, outcome measures, and study designs, the data cannot be subjected to clinically meaningful meta-analysis. Therefore, this study adopted the integrative review method proposed by Whittemore and Knafl (2005), and guided by the PICOS framework, systematically explored the components of exercise prescriptions for postoperative breast cancer patients and their patient experience.
This review is guided by the central question: How to create localized exercise prescriptions and support strategies in China to better improve the exercise experience of Chinese breast cancer postoperative survivors? By synthesizing evidence from multiple sources, this review aims to provide a comprehensive understanding of the current state of exercise rehabilitation therapy for breast cancer patients after surgery. Ultimately, the goal is to support the development of a scientific, standardized, and localized rehabilitation framework tailored to China’s context, thereby improving recovery outcomes for breast cancer patients and advancing the goals of the “Healthy China” initiative.
It is worth noting that the “Healthy China 2030” initiative, with its core principle of integrating medicine and physical activity, aligns with the goals of the World Health Organization’s’ Global Action Plan for Physical Activity 2018–2030, which also advocates for incorporating physical activity into healthcare systems to prevent and manage non-communicable diseases. Although this study is rooted in the China context, it addresses a universal challenge in cancer rehabilitation. Therefore, the insights generated by this study can provide valuable references for developing culturally adapted rehabilitation models in other global healthcare settings.
Materials and methods
2
This integrative review was conducted following the methodology outlined by Whittemore and Knafl (2005) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure a transparent, reproducible, and credible review process, thereby providing methodological assurance for the scientific conclusions.
We selected the integrative review method for its ability to synthesize diverse types of evidence—both quantitative and qualitative—within a single review. Unlike systematic reviews that typically focus on quantitative data and meta-analysis, or scoping reviews that aim to map the extent of research in a field, the integrative review allows for a comprehensive understanding of complex phenomena by integrating findings from varied study designs. Given that our research question encompasses both the effectiveness of exercise interventions (quantitative evidence) and the subjective experiences of patients (qualitative evidence), the integrative review provided a suitable framework to address both aspects holistically.
Scope of the study
2.1
The research question was formulated according to the PICOS framework to guide the review. The population (P) of interest comprised adult women following surgery for breast cancer. The intervention (I) was defined as any structured, postoperative exercise program or prescription. These interventions were evaluated in comparison (C) to routine care (e.g., standard physiotherapy or educational advice) or other non-exercise interventions. The outcomes (O) of primary interest were upper limb function, the incidence of lymphedema, and health-related quality of life. Finally, eligible study designs (S) included randomized controlled trials, quasi-experimental studies, and qualitative research, in order to synthesize both quantitative efficacy and qualitative experiential evidence.
Literature search strategy
2.2
A systematic literature search was conducted from inception until December 30, 2024, across seven electronic databases: PubMed, Web of Science, the Cochrane Library, CINAHL, China National Knowledge Infrastructure (CNKI), Wanfang Data, and VIP Chinese Journal Database (VIP). The search strategy was developed using a combination of Medical Subject Headings (MeSH) terms and free-text keywords related to three core concepts: “breast neoplasms,” “postoperative period,” and “exercise therapy.” The search strategy was tailored to the specific syntax of each database. The full search strategies are provided in Supplementary File 1.
Inclusion and exclusion criteria
2.3
Inclusion criteria:(1) Participants were adult women after breast cancer surgery; (2) The intervention involved a structured exercise program; (3) Study types included original research (e.g., randomized controlled trials, quasi-experimental studies, qualitative studies).
Exclusion criteria:(1) Studies with unclear descriptions of the exercise intervention protocol; (2) Publication types such as letters, conference abstracts, commentaries, or reviews; (3) Non-English or non-Chinese publications; (4) Duplicate publications or studies with highly overlapping content; (5) Studies for which the full text was unavailable.
Rationale for language restriction: The exclusion of publications in languages other than English or Chinese was a practical decision based on the research team’s language proficiency and the availability of translation resources. We acknowledge that this may introduce a potential for language bias by omitting relevant studies published in other languages. However, given that the major international (English) and the most relevant regional (Chinese) evidence bases were comprehensively searched, we believe the retrieved literature adequately represents the current state of knowledge on this topic, particularly within the context of the ‘Healthy China’ initiative.
Literature screening and quality appraisal
2.4
Literature management and screening were performed using Zotero 7. Following prior team training in systematic review methods, two researchers independently executed the study selection and quality appraisal processes. The literature screening (kappa = 0.86) and methodological assessment using the Mixed Methods Appraisal Tool (MMAT; kappa = 0.83) were conducted independently, with any discrepancies resolved through discussion or arbitration by a third researcher. For the MMAT, each study was rated on specific criteria, and a total quality score (percentage of criteria met) was calculated. The MMAT scores for all included studies are presented in Table 1.
Data extraction and analysis
2.5
This study adopts the strategy of thematic aggregation and interpretative integration, and regards the quantitative and qualitative evidence as complementary evidence body, which is equally weighted to construct the overall interpretation of the research problem. Extracted data included basic study characteristics (author, year, country/region), exercise prescription parameters (frequency, intensity, type, duration, total volume, and progression), study conclusions, and themes with supporting data in qualitative studies. In this study, qualitative data analysis was independently conducted by two researchers using NVivo 12.0 software for data management, coding, and theme extraction. A combination of inductive and deductive coding methods was employed to systematically analyze raw data, with continuous refinement of coding definitions until no new codes emerged and data saturation was achieved. Disputes during coding were resolved through bilateral discussions, with a third researcher intervening if consensus remained unattained. Cohen’s Kappa coefficient (Kappa = 0.82) demonstrated strong intercoder consistency, indicating high reliability in the analysis.
Results
3
Literature search results
3.1
A total of 2,370 records were initially retrieved from the databases, including 342 from PubMed, 570 from Web of Science, 55 from the Cochrane Library, 118 from CINAHL, 527 from CNKI, 463 from Wanfang Data, and 295 from VIP. After removing duplicates and screening titles, abstracts, and full texts, 23 studies were ultimately included. The methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT). The overall quality of the evidence was high, with 20 studies scoring 100% and 3 studies scoring 80% (Hiraoui et al., 2022; Rasmussen et al., 2022; Son et al., 2024), providing a reliable foundation for the subsequent synthesis of results. The literature selection process is presented in Figure 1.
PRISMA flow diagram of literature screening.
Methodological quality of included studies
3.2
The methodological quality of the 23 included studies was assessed using the Mixed Methods Appraisal Tool (MMAT), with detailed scores for each study provided in Table 1 and Supplementary File 2. The overall quality of the evidence was high. Twenty studies (87%) fulfilled all MMAT criteria, achieving a score of 100%. The remaining three studies (Hiraoui et al., 2022; Rasmussen et al., 2022; Son et al., 2024) met 80% of the criteria. No studies were excluded based on quality assessment, all were deemed to provide valuable evidence for this integrative review. The high methodological quality across the included literature provides a reliable foundation for the subsequent synthesis of results.
Basic characteristics of included studies
3.3
Among the 23 included studies, 15 were randomized controlled trials (RCTs), 3 were non-randomized controlled trials, 4 were qualitative studies, and 1 was retrospective. Six studies were conducted in China, while the remaining 17 were from countries such as the United States, France, and Germany. The included studies were published between 2015 and 2024. Detailed characteristics of the included studies are presented in Table 1.
As shown in Table 1, the literature included in this study exhibits significant methodological heterogeneity across multiple dimensions, including research design, exercise intervention protocols, participant characteristics, and outcome measurement indicators. The most prominent source of heterogeneity stems from substantial variations in core parameters such as exercise prescription types, intensity levels, and frequency. The diversity of exercise prescription interventions highlights the urgent need for integrated analysis.
Core principles of postoperative exercise prescription for breast cancer patients
3.4
Table 2 systematically summarizes the core elements, implementation processes, and intervention outcomes of postoperative exercise prescriptions for breast cancer patients based on the PICOS framework. From the integrated results of 23 studies, it is clear that the core composition dimensions of postoperative exercise prescriptions for breast cancer patients are well-defined, covering six key aspects: exercise frequency, intensity, duration, type, total volume, and progression methods. These dimensions collectively form the core framework of postoperative exercise prescription intervention, providing a fundamental reference for the clinical development of targeted exercise prescriptions. However, considerable variability exists across studies in how these principles are defined and applied. Exercise frequency is expressed in diverse ways, such as a fixed number of sessions per week or a total number of minutes per week, with no unified standard. This inconsistency makes it difficult to compare the effects of frequency on rehabilitation outcomes across studies. Exercise intensity indicators are complex and differ between aerobic and resistance training. For example, methods such as heart rate reserve (HRR) and the Borg Rating of Perceived Exertion (RPE) scale are commonly used, but their variability increases the difficulty of determining appropriate intensity levels in clinical settings. Exercise duration is inconsistently reported, with some studies using minutes per session and others using hours per week, making it challenging to accurately assess the impact of exercise duration on outcomes. Total exercise volume is also quantified in various ways, including MET-min/week, kcal/week, and minutes/week. The lack of consensus on the most effective unit hampers the evaluation of the relationship between exercise volume and rehabilitation efficacy. In addition, descriptions of exercise progression are often vague or absent, limiting the ability to implement and adjust exercise prescriptions scientifically. Overall, these inconsistencies reflect a lack of standardization and normativity in the application of core principles in postoperative exercise prescription for breast cancer patients. This hinders the development of evidence-based, standardized rehabilitation protocols.
To systematically analyze the clinical application status and efficacy consistency of core parameters of exercise prescription, this study summarized the intensity, frequency, duration and progression scheme included in the literature. The results are shown in Table 3.
Table 3 analysis reveals that resistance exercise intensity (40% ~ 80% 1-RM) and progressive loading schemes demonstrate the highest consistency in effectiveness. For aerobic exercises, the intensity range based on Borg’s subjective fatigue rating (RPE 9 ~ 15) also shows strong consistency. The current primary gap lies in significant heterogeneity regarding the quantification and reporting of core parameters (e.g., intensity, frequency, total exercise volume), coupled with vague descriptions of exercise progression principles, which directly hinders the development of standardized exercise prescription guidelines.
Evaluation of the effectiveness of postoperative exercise prescriptions for breast cancer patients
3.4.1
Evaluating the effectiveness of postoperative exercise prescriptions is a critical component of rehabilitation nursing, as both the scientific rigor and individualization of such prescriptions directly impact recovery outcomes and quality of life. Among these, interventions that combine aerobic and resistance training, incorporate natural daily activities, integrate digital technologies, and utilize traditional Chinese exercise modalities provide patients with more accessible, enjoyable, and personalized exercise experiences. This integration of exercise into everyday life enhances feasibility and patient acceptance, making such approaches more suitable for broad implementation. Detailed findings are presented in Table 4.
Effect of different exercise modes on outcome index in postoperative patients with breast cancer
3.4.2
Table 4 demonstrates the effects of different exercise intervention models on upper limb function, lymphedema, quality of life, and adherence in postoperative breast cancer patients. Regarding the impact of exercise modalities on outcome indicators, both combined modalities (aerobic plus resistance training) and single resistance training showed significant positive effects on improving upper limb function and lymphedema (Dieli-Conwright et al., 2018; Esteban-Simon et al., 2023; Kilbreath et al., 2020), establishing them as core measures for enhancing physical function. Notably, two small-sample exploratory studies reported 100% completion rates of resistance training with no participant withdrawals (Rasmussen et al., 2022; Son et al., 2024), preliminarily confirming its safety and acceptability under strict supervision. This provides foundational evidence for the safe and systematic clinical implementation of such training. In terms of improving quality of life and psychological adaptability, traditional mind–body exercises (e.g., Baduanjin, yoga) demonstrated unique advantages (Wang et al., 2019; Xu and Wang, 2021), with all studies reporting positive outcomes. Digital remote guidance has proven to be an effective strategy for improving intervention adherence, with high completion rates (92–94%) and accessibility contributing to enhanced outcomes (Jiang et al., 2023; Jin et al., 2018). Comprehensive analysis indicates that selecting exercise rehabilitation programs for postoperative breast cancer patients requires a holistic approach that considers core rehabilitation goals, individual capabilities, and medical resources to achieve personalized outcomes and maximize benefits.
Factors influencing adherence to exercise prescription for breast cancer
3.4.3
Table 4 reveals variations in adherence across exercise modalities. The combined modalities and digital remote guidance demonstrated higher completion rates (>80 to 94%), while traditional physical and mental exercises also showed strong performance (89–93%). However, treatment withdrawal for combined modalities was primarily attributed to adverse effects (e.g., fatigue, pain) and personal reasons, whereas traditional exercises and digital guidance were mainly discontinued due to personal time conflicts and loss to follow-up. Notably, qualitative research data indicates that some patients still experience lymphedema-related fear during resistance training (Husebø et al., 2015), which correlates with adherence patterns observed in quantitative studies. This finding highlights a critical consideration in designing intervention strategies: treatment-related side effects (fatigue, pain) and specific psychological barriers (e.g., lymphedema fear) serve as major obstacles to exercise adherence, while accessible intervention formats (e.g., digital guidance) and culturally adapted exercise approaches can enhance long-term patient engagement.
Safety of exercise prescription in patients with breast cancer
3.4.4
A limited number of studies have documented mild, transient, and reversible adverse effects, primarily associated with initial exercise loads. These include delayed onset muscle soreness during resistance training, a normal physiological adaptation that typically resolves with continued training (Dieli-Conwright et al., 2018) and reversible fatigue exacerbation in some patients following low-intensity activities during chemotherapy or radiotherapy (Wechsler et al., 2023) Medical staff should accurately identify the nature of the discomfort in the affected limb, distinguish between benign functional adaptation and adverse overload, and dynamically adjust the intensity and duration of exercise based on the patient’s treatment stage and individual response.
Comparison of exercise prescription for Chinese breast cancer patients with international exercise prescription
3.4.5
To gain a deeper understanding of the localization characteristics of postoperative exercise rehabilitation for breast cancer in China, this study conducted a stratified comparison of 6 Chinese studies and 17 international studies. The comparison revealed significant differences in intervention strategies and focal points. In terms of exercise types, Chinese studies showed a marked preference for traditional mind–body exercises such as Baduanjin and the “Eight Shoulder Joint Exercises” based on qigong, whose gentle and continuous nature better aligns with the local cultural perception of rehabilitation, while international studies focused more on modern resistance and aerobic training. In terms of intervention models, Chinese studies integrated “Internet+” and digital technologies, such as WeChat platforms and VR systems, earlier and more extensively, accounting for 50% of the cases, highlighting their infrastructure advantages in digital health applications. In terms of rehabilitation priorities, international studies paid more attention to the impact of exercise on long-term biomedical indicators such as metabolic syndrome and sarcopenic obesity, while Chinese studies focused more on improving upper limb function, preventing lymphedema, and enhancing short-term treatment adherence. The patient showed excellent adherence. The completion rate was between 82 and 94% in the nurse-coordinated and led rehabilitation intervention, and there was a sustained and significant improvement in key rehabilitation outcomes, including upper limb function and lymphedema control (Liu et al., 2021; Xu and Wang, 2021). These differences reflect different medical cultures, resource endowments, and research orientations, suggesting that when formulating rehabilitation plans in China, the acceptance of local culture and the accessibility of existing technical resources must be fully considered.
Postoperative exercise experiences among breast cancer patients
3.5
Qualitative studies have explored the multifaceted experiences of breast cancer patients with postoperative exercise. Husebø et al. (2015) described the multidimensional benefits of exercise-including psychological, physiological, and social improvements-through a qualitative approach. Wechsler et al. (2023) focused on patients experiencing cancer-related fatigue, emphasizing personalized strategies for regulating exercise dosage. Drawing on self-regulation theory, Tsai et al. (2018) analyzed factors influencing exercise behavior among cancer survivors. Nielsen et al. (2020) proposed an exercise intervention framework based on mHealth technology tailored to chemotherapy patients. Together, these studies highlight the complexity and individualization of exercise rehabilitation for breast cancer patients, offering valuable insights into clinical nursing practice. Details are summarized in Table 5.
Positive effects of exercise on physical and mental health
3.5.1
On the physical health level, one patient stated: “I had been down and sorry for myself, thinking life was terrible… Then I realized sitting around feeling sorry would not help. If I went out and did something and thought positively, I’d feel better.” (Husebø et al., 2015), affirming the role of exercise in alleviating negative emotions. Another patient shared: “I felt energized and happy… more alert and ready to take on the day.” (Wechsler et al., 2023), highlighting the enhancement of vitality through exercise.
Regarding mental health, one participant described: “After I finish exercising, I usually feel energized… my mood is definitely better; I feel like my mind works better when I exercise.” (Wechsler et al., 2023), suggesting potential cognitive benefits from physical activity. Another patient expressed: “It feels amazing when you realize you have done it—you are sticking with it—and you are part of a study that focuses on physical activity. It makes me feel like I’m in control and that things will get better.” (Husebø et al., 2015), reflecting an improvement in self-efficacy. In some cases, patients also employed self-reward strategies: “I rewarded myself with a chocolate bar and a piece of cake—and I felt great, no guilt at all.” (Tsai et al., 2018).
Variability in postoperative exercise experiences among breast cancer patients
3.5.2
Patients exhibit differing levels of tolerance and responses to treatment-related side effects, resulting in highly individualized exercise experiences. Exercise goals vary across individuals—some patients prefer incorporating natural, everyday physical activities into their routines, while others favor more structured exercise programs. This reflects the personalized nature of exercise needs (Tsai et al., 2018). When attempting to determine an optimal exercise dose, patients often rely on their own perceptions of fatigue and physical response. However, in the absence of professional guidance, this trial-and-error process frequently leads to frustration. Additionally, the available online information does not adequately meet patients’ needs for exercise-related support during chemotherapy, highlighting the urgent need for precise and personalized clinical exercise guidance (Nielsen et al., 2020).
Integrative discovery: the connection between evidence and experience
3.6
This study reveals the dynamic process and underlying mechanisms of postoperative exercise prescription from theoretical formulation to clinical practice effectiveness by integrating quantitative and qualitative evidence.
Dual pathways of efficacy: physiological improvement and psychological empowerment
3.6.1
Quantitative results demonstrated that the aerobic-resistance combined training model showed the most significant improvement in upper limb function among breast cancer postoperative patients (see Section 3.4). Qualitative findings provided crucial psychological insights: Participants in this structured program consistently reported enhanced self-control and increased sense of achievement (see Section 3.5). This indicates that the integrated training approach not only delivers multidimensional physiological stimulation but, more importantly, provides patients with continuous “success experiences” through measurable rehabilitation progress, thereby effectively boosting their self-efficacy. The elevated self-efficacy further translates into sustained motivation for exercise and overcoming challenges, creating a virtuous cycle of “functional improvement → psychological reinforcement → behavioral maintenance” in rehabilitation.
The real dilemma of compliance: between self-regulation and symptom burden
3.6.2
Quantitative analysis indicates that treatment-related adverse reactions are one of the primary reasons for patients to discontinue exercise (see 3.4). Qualitative experiences further depict the individualized landscape of this dilemma: patients persistently struggle with symptoms such as fatigue and pain during the process of “exploring appropriate exercise intensity” (see 3.5). The combination of these findings suggests that poor adherence is not solely due to “lack of motivation,” but rather results from the disruption of behavioral regulation caused by the severe and unstable symptom burden during the disease recovery phase, which impairs the patient’s self-regulation capacity. Therefore, the focus of improving adherence should not be limited to education and supervision, but rather on helping patients master more flexible self-regulation strategies to enhance their coping ability during symptom fluctuation periods.
Insights from localization practices: cultural identity enhances intervention affinity
3.6.3
In quantitative studies conducted in China, intervention programs that integrate traditional physical and mental exercises with digital health technologies have demonstrated better patient acceptance and rehabilitation outcomes. Qualitative experiences further reveal that patients value the “harmony of form and spirit” emphasized by such exercise methods, as well as the “convenience” and “sense of companionship” brought by digital tools (see 3.5). This suggests that rehabilitation measures tailored to patients’ cultural backgrounds and health concepts are more likely to stimulate their intrinsic motivation for participation, enhance the affinity and sustainability of interventions, and provide practical evidence for achieving truly “patient-centered” rehabilitation care.
Sensitivity analysis
3.7
To ensure the reliability of the qualitative synthesis conclusions in this study, we conducted subgroup analyses based on exercise types, surgical approaches, and intervention duration. Through systematic exclusion of low-quality studies, small-sample studies, and special intervention protocols, we validated the results. The core finding that “structured exercise has rehabilitative benefits for breast cancer postoperative patients” remained consistent across different subgroups and literature subsets after exclusion, demonstrating strong stability. The heterogeneity of existing evidence did not undermine this core conclusion but instead highlighted the need for systematic and standardized development of exercise prescription parameters.
Discussion
4
Scientific rigor and standardization of exercise prescriptions
4.1
The results of this study show that resistance training has positive effects on the function of the upper limb and lymphedema in breast cancer patients, with the highest evidence strength. The scientifically designed postoperative exercise rehabilitation intervention for breast cancer patients can significantly improve the upper limb motor function of the patients (Leclerc et al., 2017), and at the same time, it will not increase the risk of postoperative lymphedema (Đorđević et al., 2024). This is consistent with the current research conclusions focusing on postoperative exercise rehabilitation for breast cancer (Li et al., 2018), further confirming the core value and evidence-based basis of standardized exercise intervention in the postoperative rehabilitation of breast cancer. But, our results confirm that the scientific rigor and standardization of postoperative exercise prescriptions remain insufficient, as evidenced by the substantial heterogeneity in core parameters (e.g., intensity, frequency) summarized in Table 3. Although traditional Chinese practices such as Baduanjin have shown unique advantages, particularly their integrative mind–body nature that combines meditation, breathing regulation, and structured movements, which aligns well with cultural preferences and provides a holistic approach to recovery (Wang et al., 2019), quantitative analysis of key parameters is still limited. To address these challenges, future research should aim to establish a multidimensional standard system that integrates both objective measurements and subjective assessments. Enhanced digital monitoring and personalized guidance are needed, alongside strengthened evidence-based research on traditional exercise modalities. Long-term follow-up studies and stage-based interventions should also be conducted to develop more scientific, precise, and sustainable exercise prescriptions for breast cancer survivors.
Personalization and adherence in exercise prescription
4.2
Postoperative exercise rehabilitation for breast cancer patients faces significant challenges in terms of personalization and adherence (Wechsler et al., 2023). The postoperative exercise compliance of breast cancer patients is constrained by factors such as treatment-related side effects like fatigue, pain, fear-induced lymphedema, and lack of personalized support (Husebø et al., 2015; Wechsler et al., 2023), which is consistent with the existing research conclusions (Wang et al., 2022). This further validates the prevalence of influencing factors for exercise compliance in postoperative breast cancer patients in clinical practice. Current exercise prescriptions often lack a comprehensive and systematic assessment of patients’ health status, functional capacity, and psychological needs, resulting in a poor match between the prescription and individual patient characteristics (Li et al., 2025). First, patients exhibit substantial variability in their exercise experiences (Deng et al., 2021). Qualitative studies (Husebø et al., 2015; Tsai et al., 2018) have confirmed that while exercise can improve mood, enhance self-efficacy, and alleviate physical discomfort, treatment-related side effects and exercise-related fear frequently serve as major barriers to adherence (Nielsen et al., 2020). Second, contradictions exist in intervention strategies. On the one hand, external feedback—such as motivational text messages and goal-oriented tasks—can help maintain exercise behaviors in some patients (Nielsen et al., 2020). On the other hand, some patients prefer autonomy in selecting the type and timing of their activities and may resist overly structured interventions (Tsai et al., 2018). This tension reveals a critical shortcoming of current strategies: they fail to respect individual autonomy and apply a one-size-fits-all approach that does not meet the diverse needs of patients. Regarding the positive effects of “Internet+” digital technology and China traditional exercise on improving postoperative compliance and quality of life for breast cancer patients, the current evidence is of moderate strength. Although the quality of relevant randomized controlled trials is high and shows significant benefits, the number of studies in this field remains relatively limited, and the mechanisms of traditional exercises and the long-term effects of digital technology have not been fully elucidated. More research is needed in the future to consolidate these findings.
To address these issues, the following strategies are recommended:
Before developing an exercise prescription, breast cancer patients should undergo comprehensive health assessments and physical fitness evaluations. The prescription should then be dynamically tailored to match patients’ physical condition, treatment stage, exercise habits, and psychological needs. It is essential to ensure that exercise programs are not only safe and effective but also personalized. During implementation, a balance should be maintained between professional guidance and patient autonomy, with full consideration given to multidimensional factors such as age, physiological function, and individual exercise preferences.
The critical role of multidisciplinary collaboration in exercise rehabilitation for postoperative breast cancer patients
4.3
With the continuous advancement of the “integration of medicine and physical activity” model, greater professional competence is expected of nurses in the field of exercise rehabilitation (Zhou et al., 2024). However, many nurses currently lack sufficient knowledge and skills in this area, as well as systematic training in sports medicine, making it difficult for them to accurately assess patients’ exercise capacity and formulate scientifically sound exercise prescriptions (Gao et al., 2020). Furthermore, due to heavy clinical workloads, nurses often have limited time and capacity to conduct detailed follow-up and supervision, which compromises the effectiveness of exercise rehabilitation (Wang et al., 2022). To enhance the role of nurses in postoperative exercise rehabilitation for breast cancer patients, medical institutions should strengthen specialized training programs and promote the development of breast cancer case managers. This will help improve nurses’ competencies in exercise prescription development, injury prevention, and rehabilitation guidance. Effective allocation of nursing human resources is also essential to ensure that nurses or case managers have sufficient time and energy to support patients’ rehabilitation processes. In addition, nurses or case managers should lead the establishment of multidisciplinary exercise rehabilitation teams, fostering close collaboration and communication among nurses, physicians, physical therapists, and mental health professionals. By providing comprehensive, high-quality, and coordinated exercise rehabilitation services, such teams can promote the development of more scientific and personalized approaches to postoperative recovery in breast cancer patients.
Strengths and limitations
4.4
This study strictly followed the PRISMA guidelines and the MMAT quality assessment standards, including high-quality evidence-based studies. It integrated quantitative and qualitative research, covered both domestic and international practices, and closely aligned with the “Healthy China 2030” planning outline and clinical needs. The conclusions have clear practical guidance value for the formulation of localized rehabilitation plans. The limitations mainly lie in the existence of language and publication bias risks in the literature inclusion, and significant heterogeneity in the exercise prescription parameters and outcome indicator measurement methods of the included studies. This has to some extent affected the comprehensiveness of the research results and the direct comparability of conclusions among different studies. Future research can further optimize by expanding the language coverage and promoting parameter standardization.
Conclusion
5
The “Healthy China 2030” Planning Outline explicitly proposes “promoting the deep integration of medicine and physical activity, improving the chronic disease prevention and rehabilitation service system, and achieving a shift from disease treatment to health management” (Lian et al., 2023). This integrative review, which focuses on postoperative exercise prescriptions for breast cancer, is deeply aligned with this initiative and provides strong support for implementing the national health strategy in the field of breast cancer rehabilitation. The research results show that combining aerobic exercise with resistance training, integrating natural physical activities into daily routines, utilizing digital technology, and adopting exercise therapies rooted in China’s traditional culture, such as Baduanjin and Tai Chi, can effectively improve upper limb function. However, existing exercise prescriptions lack standardization across core components such as exercise type, intensity, frequency, and total volume. Inadequate personalization and poor patient adherence remain major barriers to the effective implementation of exercise rehabilitation. Therefore, we call for the national health authorities to lead the effort in collaborating with experts from rehabilitation medicine, sports science, and nursing to develop a “Postoperative Rehabilitation Exercise Guide for Breast Cancer” tailored to China’s specific conditions. By integrating the principles of “standardization” and “personalization,” we aim to establish an effective localized intervention program. Additionally, training programs should be expanded to improve nurses’ knowledge and skills in exercise rehabilitation, and more breast cancer case managers should be developed. Establishing multidisciplinary rehabilitation teams will be essential for promoting localized, scientific, and precise exercise rehabilitation practices, ultimately improving overall recovery outcomes for breast cancer patients and advancing the goals of the “Healthy China” initiative.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chang X. T. Zhu X. J. Wu W. Y. Shen L. Jiang C. E. (2024). Latent profile analysis and influencing factors of kinesiophobia in postoperative patients with.Breast cancer. Chin. Nurs. Res. 38, 4341–4348. doi: 10.12102/j.issn.1009-6493.2024.24.003 · doi ↗
- 2Chen C. M. Pan L. Y. Zheng J. Y. (2022). Analysis of current status of kinesiphobia and related risk factors in patients after modified radical mastectomy for breast cancer. Chin. Gen. Pract. Nurs. 20, 5158–5160. doi: 10.12104/j.issn.1674-4748.2022.36.031 · doi ↗
- 3Deng Y. Q. Pan C. Wang Q. L. Wang D. (2021). Qualitative research on exercise experience of patients with breast cancer: a meta-synthesis. J. Nurs. 28, 34–39. doi: 10.16460/j.issn 1008-9969.2021.13.034 · doi ↗
- 4Dieli-Conwright C. M. Courneya K. S. Demark-Wahnefried W. Sami N. Lee K. Buchanan T. A. . (2018). Effects of aerobic and resistance exercise on metabolic syndrome, sarcopenic obesity, and circulating biomarkers in overweight or obese survivors of breast cancer: a randomized controlled trial. J. Clin. Oncol. 36, 875–883. doi: 10.1200/JCO.2017.75.7526, 29356607 PMC 5858524 · doi ↗ · pubmed ↗
- 5ĐorđevićD. Garnier J. van Mackelenbergh T. Seitz S. Mundhenke C. (2024). The impact of online yoga on sleep and quality of life in women with breast cancer: a randomized trial. Arch. Gynecol. Obstet. 310, 571–575. doi: 10.1007/s 00404-024-07563-6, 38814454 · doi ↗ · pubmed ↗
- 6Drozd C. Jacquinot Q. Paget-Bailly S. Mansi L. Paillard M.-J. Bazan F. . (2024). Postcancer rehabilitation: multidisciplinary exercise – programme organisation and feasibility. BMJ Support. Palliat. Care 15, 789–795. doi: 10.1136/spcare-2024-005068, 39740960 PMC 12573348 · doi ↗ · pubmed ↗
- 7Esteban-Simon A. Diez-Fernandez D. M. Rodriguez-Perez M. A. Artes-Rodriguez E. Casimiro-Andujar A. J. Soriano-Maldonado A. (2023). Does a resistance training program affect between-arms volume difference and shoulder-arm disabilities in female breast cancer survivors? The role of surgery type and treatments. Secondary outcomes of the EFICAN trial. Arch. Phys. Med. Rehabil. 105, 647–654. doi: 10.1016/j.apmr.2023.11.010, 38043674 · doi ↗ · pubmed ↗
- 8Feng Y. Wei H. Y. Wang W. N. (2024). Effect of different exercise modalities to improve shoulder function in postoperative breast cancer patients: a network meta-analysis. J. Nurs. Sci. 39, 81–85. doi: 10.3870/j.issn.1001-4152.2024.19.081 · doi ↗