A study of three-time-point dynamic changes in aPS/PT and standard aPL antibodies and their association with IVF pregnancy outcomes in APS-related recurrent pregnancy loss
Fenjian Lu, Penghao Li, Panyu Yang

TL;DR
This study tracks antibody levels in APS-related recurrent pregnancy loss patients over time and finds that specific patterns are linked to successful or failed pregnancies.
Contribution
The study reveals distinct dynamic profiles of aPS/PT antibodies associated with pregnancy outcomes in APS-RPL patients.
Findings
Higher aPS/PT IgM and aCL IgG levels in APS-RPL patients compared to healthy controls.
Successful pregnancies correlate with reduced aCL IgG, aPS/PT IgM, and aβ2GPI IgM levels post-treatment and during early pregnancy.
Pregnancy loss is associated with elevated aPS/PT IgM and IgG levels during early pregnancy.
Abstract
This study aimed to evaluate dynamic anti-phosphatidylserine/prothrombin (aPS/PT) and antiphospholipid (aPL) antibody changes in antiphospholipid syndrome-recurrent pregnancy loss (APS-RPL) patients and their relationship with pregnancy outcomes. This study included 100 RPL patients with APS features and 30 healthy women who had a normal delivery from 2020 to 2022. First, the differences in aPL and aPS/PT antibody levels between the study group and the control group were compared. Then, a mixed-design repeated measures analysis of variance (RM-ANOVA) was used to assess the time effects, group effects, and their interactions. Pairwise comparisons between time points within each group were performed using one-way repeated measures ANOVA. Finally, antibody levels at each time point were compared between the successful pregnancy group and the pregnancy loss group. (1) The levels of aPS/PT…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
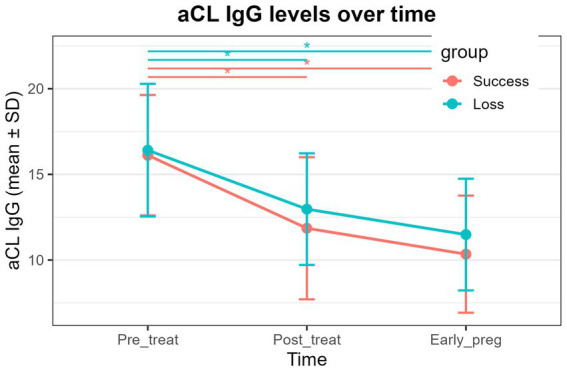 Figure 1
Figure 1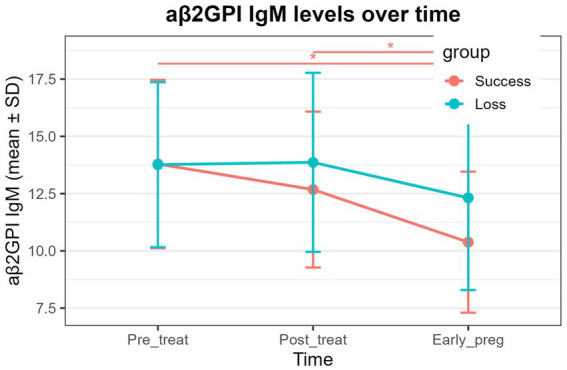 Figure 2
Figure 2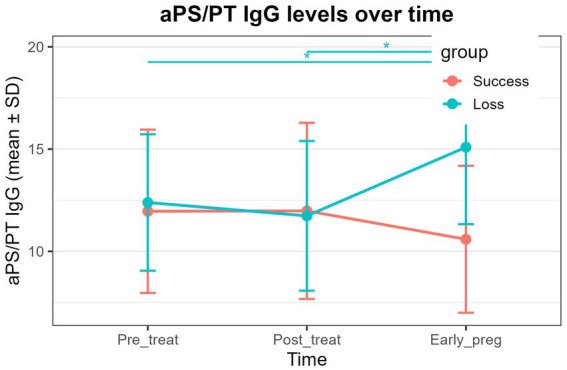 Figure 3
Figure 3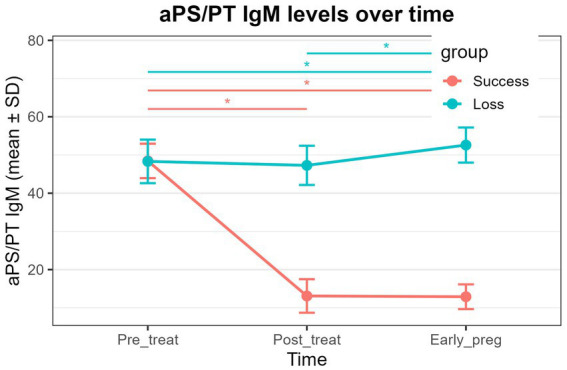 Figure 4
Figure 4| Characteristic | Study population ( | Successful pregnancy ( | Pregnancy loss ( | |
|---|---|---|---|---|
| Recurrent pregnancy loss ≥3 episodes before 10 weeks | 100 | 55 | 35 | – |
| History of fetal demise (≥10 weeks) | 0 | 0 | 0 | – |
| Previous placental insufficiency | 0 | 0 | 0 | – |
| Prior severe preeclampsia (<34 weeks) | 0 | 0 | 0 | – |
| Use of low-dose aspirin | 100 (100%) | 55 (100%) | 35 (100%) | – |
| Use of low-molecular-weight heparin | 100 (100%) | 55 (100%) | 35 (100%) | – |
| Use of hydroxychloroquine | 32 (32%) | 17 (31%) | 13 (37%) | 0.702 |
| Use of prednisone | 13 (13%) | 8 (15%) | 4 (11%) | 0.760 |
| Group | Study group ( | Control group ( | |
|---|---|---|---|
| Age (years) | 32.56 ± 4.51 | 31.43 ± 4.13 | 0.206 |
| Weight (kg) | 55.96 ± 5.09 | 55.01 ± 5.04 | 0.368 |
| Height (m) | 1.54 ± 0.05 | 1.54 ± 0.05 | 0.750 |
| BMI | 23.61 ± 2.55 | 23.37 ± 3.00 | 0.688 |
| Menstrual cycle (days) | 28.46 ± 3.48 | 29.73 ± 4.61 | 0.170 |
| Group | Normal pregnancy group ( | Pregnancy loss group ( | |
|---|---|---|---|
| Age (years) | 32.62 ± 4.58 | 32.17 ± 4.62 | 0.655 |
| Weight (kg) | 55.89 ± 4.89 | 56.57 ± 5.46 | 0.554 |
| Height (m) | 1.54 ± 0.04 | 1.54 ± 0.05 | 0.836 |
| BMI | 23.53 ± 2.36 | 23.92 ± 2.84 | 0.505 |
| Menstrual cycle (days) | 28.40 ± 4.00 | 28.49 ± 2.80 | 0.905 |
| Number of pregnancy losses | 3.15 ± 0.62 | 3.00 ± 0.64 | 0.292 |
| Group | aCL IgG (CU) | aCL IgM (CU) | aCL IgA (CU) | aβ2GPI IgG (RU/mL) | aβ2GPI IgM (RU/mL) | aβ2GPI IgA (RU/mL) | LA1 (sec) | LA2 (sec) | LA1 (SCT) (sec) | LA2 (SCT) (sec) | aPS/PT IgG (U/mL) | aPS/PT IgM (U/mL) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study group ( | 16.39 ± 3.63 | 10.7 ± 3.57 | 10.35 ± 4.47 | 12.69 ± 4.52 | 14.11 ± 3.82 | 7.46 ± 3.55 | 35.75 ± 3.63 | 33.37 ± 3.46 | 58.42 ± 4.96 | 36.54 ± 3.65 | 12.24 ± 3.76 | 48.73 ± 5.07 |
| Control group ( | 12.53 ± 5.24 | 11.26 ± 3.8 | 9.89 ± 3.84 | 11.95 ± 2.85 | 12.67 ± 4.73 | 8.14 ± 2.78 | 37.1 ± 4.11 | 34.16 ± 2.29 | 58.79 ± 4.77 | 35.64 ± 4.21 | 12.78 ± 3.32 | 10.89 ± 5.83 |
| 5.45 × 10−4* | 0.477 | 0.589 | 0.284 | 0.135 | 0.273 | 0.114 | 0.151 | 0.715 | 0.299 | 0.456 | <2.2 × 10−16* |
| Antibody | Group effect F | Time effect F | Group × time F | |||
|---|---|---|---|---|---|---|
| aCL IgG | 4.71 | 0.033 | 44.23 | <0.001* | 0.34 | 0.714 |
| aCL IgM | 0.05 | 0.828 | 0.12 | 0.884 | 1.23 | 0.295 |
| aCL IgA | 2.17 | 0.144 | 0.41 | 0.663 | 0.88 | 0.417 |
| aβ2GPI IgG | 0.80 | 0.374 | 1.53 | 0.220 | 0.98 | 0.377 |
| aβ2GPI IgM | 5.03 | 0.028 | 11.35 | <0.001* | 1.69 | 0.187 |
| aβ2GPI IgA | 1.28 | 0.262 | 0.35 | 0.709 | 1.02 | 0.364 |
| LA1 | 10.65 | 0.002* | 3.67 | 0.027 | 0.24 | 0.789 |
| LA2 | 6.36 | 0.013 | 0.79 | 0.456 | 0.49 | 0.616 |
| LA1 (SCT) | 8.86 | 0.004* | 0.58 | 0.562 | 0.95 | 0.391 |
| LA2 (SCT) | 0.39 | 0.533 | 2.32 | 0.101 | 0.79 | 0.454 |
| aPS/PT IgG | 11.48 | 0.001* | 1.42 | 0.244 | 9.28 | <0.001* |
| aPS/PT IgM | 1899.52 | <0.001* | 403.46 | <0.001* | 483.95 | <0.001* |
| Antibodies | Group | Pre-treatment | Post-treatment | Post-pregnancy | Time effect (RM-ANOVA | Pre-treatment vs. post-treatment | Pre-treatment vs. post-pregnancy | Post-treatment vs. post-pregnancy |
|---|---|---|---|---|---|---|---|---|
| aCL IgG | Success | 16.12 ± 3.52 | 11.85 ± 4.15 | 10.34 ± 3.42 | 1.1 × 10−6* | 8.5 × 10−10* | 0.13 | |
| Loss | 16.41 ± 3.87 | 12.97 ± 3.26 | 11.49 ± 3.26 | 0.001* | 3 × 10−5* | 0.331 | ||
| aβ2GPI IgM | Success | 13.79 ± 3.67 | 12.68 ± 3.40 | 10.38 ± 3.08 | 0.209 | 6.2 × 10−6* | 0.0025* | |
| Loss | 13.76 ± 3.60 | 13.87 ± 3.91 | 12.32 ± 4.02 | 0.174 | 1.00 | 0.45 | 0.25 | |
| aPS/PT IgG | Success | 11.96 ± 3.99 | 11.98 ± 4.31 | 10.59 ± 3.59 | 0.144 | 1.00 | 0.28 | 0.28 |
| Loss | 12.39 ± 3.34 | 11.73 ± 3.66 | 15.09 ± 3.76 | 1.00 | 0.0033* | 0.0013* | ||
| aPS/PT IgM | Success | 48.44 ± 4.51 | 13.10 ± 4.39 | 12.89 ± 3.24 | <2 × 10−16* | <2 × 10−16* | 1.00 | |
| Loss | 48.32 ± 5.70 | 47.28 ± 5.13 | 52.59 ± 4.60 | 1.00 | 0.0063* | 4.9 × 10−5* |
| Group | aCL | aCL IgM (CU) | aCL IgA (CU) | aβ2GPI IgG (RU/mL) | aβ2GPI IgM (RU/mL) | aβ2GPI IgA (RU/mL) | LA1 (sec) | LA2 (sec) | LA1 (SCT) (sec) | LA2 (SCT) (sec) | aPS/PT IgG (U/mL) | aPS/PT IgM (U/mL) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pregnancy group, pre-treatment ( | 16.12 ± 3.52 | 10.43 ± 3.78 | 10.50 ± 4.73 | 12.56 ± 4.05 | 13.79 ± 3.67 | 7.36 ± 3.48 | 35.02 ± 4.03 | 33.47 ± 3.37 | 59.52 ± 4.97 | 36.31 ± 3.77 | 11.96 ± 3.99 | 48.44 ± 4.51 |
| Loss group, pre-treatment ( | 16.41 ± 3.87 | 11.48 ± 3.12 | 10.42 ± 4.49 | 12.76 ± 4.55 | 13.76 ± 3.60 | 7.29 ± 3.58 | 36.59 ± 2.57 | 32.90 ± 3.28 | 56.82 ± 4.56 | 36.58 ± 3.74 | 12.39 ± 3.34 | 48.32 ± 5.70 |
| P1 value | 0.717 | 0.160 | 0.941 | 0.836 | 0.971 | 0.927 | 0.026 | 0.423 | 0.010 | 0.738 | 0.584 | 0.913 |
| Pregnancy group, post-treatment ( | 11.85 ± 4.15 | 10.86 ± 3.94 | 9.15 ± 4.53 | 12.32 ± 3.37 | 12.68 ± 3.4 | 8.26 ± 2.8 | 34.13 ± 3.26 | 34.16 ± 3.39 | 59.44 ± 4.35 | 36.39 ± 3.6 | 11.98 ± 4.31 | 13.10 ± 4.39 |
| Loss group, post-treatment ( | 12.97 ± 3.26 | 10.54 ± 2.19 | 10.68 ± 2.48 | 10.94 ± 4.50 | 13.87 ± 3.91 | 6.96 ± 3.18 | 35.10 ± 2.99 | 32.66 ± 3.97 | 58.26 ± 3.04 | 35.27 ± 4.36 | 11.73 ± 3.66 | 47.28 ± 5.13 |
| P2 value | 0.159 | 0.627 | 0.042 | 0.124 | 0.145 | 0.052 | 0.153 | 0.069 | 0.132 | 0.209 | 0.775 | <2.2 × 10−16* |
| Pregnancy group, post-pregnancy ( | 10.34 ± 3.42 | 10.99 ± 4.02 | 9.87 ± 2.97 | 12.32 ± 3.72 | 10.38 ± 3.08 | 7.19 ± 3.81 | 33.76 ± 3.91 | 34.40 ± 2.96 | 58.63 ± 4.88 | 35.15 ± 3.82 | 10.59 ± 3.59 | 12.89 ± 3.24 |
| Loss group, post-pregnancy ( | 11.49 ± 3.26 | 10.54 ± 1.82 | 10.56 ± 3.33 | 12.18 ± 3.37 | 12.32 ± 4.02 | 7.20 ± 2.77 | 35.36 ± 2.58 | 33.17 ± 2.59 | 57.77 ± 4.83 | 35.19 ± 3.05 | 15.09 ± 3.76 | 52.59 ± 4.60 |
| P3 value | 0.116 | 0.470 | 0.326 | 0.858 | 0.018 | 0.986 | 0.022 | 0.040 | 0.412 | 0.960 | 3.48 × 10−7* | <2.2 × 10−16* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Reproductive System and Pregnancy · Rheumatoid Arthritis Research and Therapies
Introduction
1
Recurrent pregnancy loss (RPL) is defined by the European Society of Human Reproduction and Embryology (ESHRE) as two or more consecutive pregnancy failures, with identifiable etiologies found in approximately 50% of affected individuals (1, 2). Epidemiological studies indicate that RPL affects up to 6% of women of reproductive age (3–5), with antiphospholipid syndrome (APS) recognized as one of the most important and identifiable causes. APS is an autoimmune disorder characterized by a hypercoagulable state, typically presenting with thrombotic events or obstetric complications, accompanied by the persistent presence of antiphospholipid (aPL) antibodies targeting phospholipid-binding proteins on cellular membranes (6–8). APS accounts for approximately 5–20% of RPL cases (2, 9).
According to the 2006 Sydney classification criteria, the diagnosis of APS requires at least one clinical criterion and one laboratory criterion, including persistent positivity for lupus anticoagulant (LA), anticardiolipin (aCL) IgG/IgM, or anti-β2-glycoprotein I (aβ2GPI) IgG/IgM (10). Clinical criteria encompass vascular thrombosis and a range of pregnancy morbidities, such as ≥3 consecutive miscarriages before 10 weeks of gestation in the absence of hormonal, anatomical, or chromosomal abnormalities; a single unexplained fetal loss after 10 weeks; or preterm delivery before 34 weeks due to severe preeclampsia, eclampsia, or placental insufficiency. However, recent studies have reported that some women who meet the clinical criteria for APS or experience RPL test negative for conventional aPL antibodies, a condition referred to as seronegative APS (11, 12), highlighting limitations of current laboratory markers.
Consequently, the search for new aPL antibodies with clinical relevance has intensified over the past decade. Among them, anti-phosphatidylserine/prothrombin (aPS/PT) antibodies have emerged as notable non-criteria aPL markers (11). Accumulating evidence indicates that aPS/PT antibodies serve as strong predictors of thrombotic events and obstetric complications (13–15), participate in the pathophysiology of APS (16, 17), and represent potential serological biomarkers for the disease (11). Nevertheless, their association with pregnancy outcomes remains controversial, with some studies failing to demonstrate significant correlations (18–20), while others have reported clear links between aPS/PT antibodies and miscarriage or pregnancy-related complications (19, 20).
Given these inconsistencies and the fact that the majority of previous studies relied on single time-point antibody measurements, the present study evaluated the dynamic changes in aPS/PT and standard aPL antibodies before treatment, after treatment, and during early pregnancy and examined their relationship with pregnancy outcomes in APS-RPL patients. This approach aims to provide a more comprehensive understanding of the immunological mechanisms underlying APS-RPL and offer more reliable evidence for clinical assessment and management.
Materials and methods
2
Study participants
2.1
This study was designed as a single-center retrospective analysis. The study group consisted of 153 women diagnosed with APS-RPL at Sichuan Jinxin Xinan Women and Children’s Hospital between 2020 and 2022.
Inclusion criteria
2.1.1
The inclusion criteria were as follows:
(1) patients who met the definition of RPL as outlined by the ESHRE, (2) patients who met the clinical criteria for APS, (3) patients who underwent testing for aPS/PT antibodies and standard aPL antibodies, and (4) patients who underwent assisted reproductive treatment (in vitro fertilization, IVF).
Exclusion criteria
2.1.2
(1) Patients with gynecological disorders, including endometritis, uterine fibroids, or hydrosalpinx; (2) patients with anatomical abnormalities of the reproductive tract, such as endometrial polyps, intrauterine adhesions, or congenital uterine malformations; (3) patients with genetic abnormalities, including those with abnormal embryonic karyotypes; (4) patients with confirmed systemic autoimmune diseases—such as systemic lupus erythematosus, Sjögren’s syndrome, systemic sclerosis, idiopathic inflammatory myopathies, or systemic vasculitis—as well as individuals clinically suspected of having systemic autoimmune disease (e.g., persistently high-titer antinuclear antibody (ANA) positivity accompanied by relevant clinical manifestations); and patients with isolated low-titer ANA positivity, without a definitive diagnosis or clinical features of systemic autoimmune disease, were not excluded; (5) patients with other systemic conditions known to contribute to RPL, including endocrine disorders, obesity, hypertension, cardiovascular disease, or renal disease; (6) patients with recurrent implantation failure (RIF); and (7) patients with a history of major adverse obstetric outcomes were excluded, including: (i) intrauterine fetal demise at ≥10 weeks of gestation in a prior pregnancy, (ii) severe preeclampsia occurring before 34 weeks of gestation, and (iii) previous pregnancies complicated by placental insufficiency resulting in adverse outcomes.
The control group included women who underwent in vitro fertilization (IVF) treatment at the same reproductive center during the same period and had a documented history of previous full-term normal delivery. All controls had no history of RPL, no venous or arterial thrombotic events, and no pregnancy complications meeting the diagnostic criteria for APS, such as fetal demise ≥10 weeks, severe preeclampsia, or placental insufficiency. In addition, none of the control participants had any known autoimmune diseases. All control subjects were tested for standard aPL antibodies and aPS/PT antibodies. None met the laboratory classification criteria for APS, defined as the absence of persistently high-titer aCL antibodies, aβ2GPI antibodies, LA, or triple antibody positivity. Baseline antibody levels in the control group were defined using the measurements obtained prior to their IVF treatment. For the study group, baseline values were based on antibody tests performed before the initiation of IVF and any APS-related therapy. All participants in both the study and control groups underwent IVF treatment at the same reproductive center, following a fully standardized clinical protocol.
Ovarian stimulation protocols: All patients received standardized controlled ovarian stimulation using either a gonadotropin-releasing hormone (GnRH) antagonist protocol or a long GnRH agonist protocol. The initial gonadotropin dose and subsequent adjustments were determined according to uniform criteria, taking into account patient age, ovarian reserve, and follicular response. When the leading follicles reached an appropriate size, oocyte maturation was triggered according to a fixed schedule, followed by transvaginal oocyte retrieval.
Embryo culture and transfer strategy: All embryos were cultured under identical laboratory conditions using a unified grading system. All patients underwent single blastocyst transfer. Endometrial preparation and luteal phase support were standardized across both groups, and embryo selection criteria were identical, ensuring full comparability of procedural factors.
Patient group definitions
2.1.3
A total of 100 patients were ultimately included in the study based on the inclusion and exclusion criteria. Relevant clinical data and laboratory test results were collected, and patients were categorized into three groups according to pregnancy outcomes.
Successful pregnancy group (n = 55)
2.1.3.1
The successful pregnancy group was defined as women who achieved a pregnancy ≥34 weeks and delivered a live-born infant without evidence of fetal growth restriction. In addition, no patients in this group experienced APS-related pregnancy complications, such as placental insufficiency, before 34 weeks of gestation.
Pregnancy loss group (n = 35)
2.1.3.2
This group included patients who experienced recurrent pregnancy loss despite treatment. Pregnancy loss was defined as fetal demise before 20 weeks of gestation.
Lost to follow-up group (n = 10)
2.1.3.3
This group included patients for whom complete follow-up data were not available after treatment.
Treatment protocol in this study: All patients in the study group (including both the successful pregnancy group and the pregnancy loss group) received a standardized anticoagulation regimen. Low-dose aspirin (75–100 mg/day) was administered to 100% of patients, initiated prior to ovarian stimulation or during the oocyte retrieval cycle, and continued throughout the pregnancy. Similarly, all patients received low-molecular-weight heparin (LMWH, 4,000–5,000 IU/day, subcutaneously), also with a 100% usage rate, starting at the initiation of luteal support and continuing for the duration of pregnancy. Immunomodulatory therapy was evaluated and adjusted by the same reproductive immunology team according to antibody profiles and clinical manifestations. Hydroxychloroquine (200 mg/day) was used in 31% of patients in the successful pregnancy group and 37% in the pregnancy loss group; treatment was initiated at least 1 month before ovarian stimulation and continued until approximately 12 weeks of gestation. Low-dose prednisone (5–10 mg/day) was used in 15% of the successful pregnancy group and 11% of the pregnancy loss group, initiated during the embryo transfer cycle or after a positive pregnancy test, and continued until 8–12 weeks of gestation. The specific clinical and treatment characteristics of the study population are outlined in Table 1.
Experimental methods
2.2
Sample collection and processing
2.2.1
- For the detection of aPS/PT IgM/IgG, aCL IgM/IgG/IgA, and aβ2GPI IgM/IgG/IgA, serum was separated using yellow-topped tubes. The serum was stored at 2–8 °C and should be tested within 72 h.
- For lupus anticoagulant (LA) detection, serum was separated using blue-topped tubes. The serum was then transferred to bullet tubes and stored at below −20 °C. After thawing and returning to room temperature, testing was conducted within 96 h.
- Timing of blood collection: Blood samples were collected during the luteal phase before treatment, again during the luteal phase 1 to 3 months after treatment, and during early pregnancy (5–8 weeks) for pregnancy-related blood sampling.
Methods, instruments, and reagents
2.2.2
The detection of aPS/PT IgM/IgG and aβ2GPI IgM/IgG/IgA was performed using an enzyme-linked immunosorbent assay (ELISA) with manual procedures. The final results were read by an ELISA reader. The relevant reagents were purchased from Wofen Medical Equipment Trading Co., Ltd., and Omon Medical Diagnostics Co., Ltd.
The detection of aCL IgM/IgG/IgA was carried out using chemiluminescence, performed by a fully automated chemiluminescence immunoanalyzer (BIO-FLASH). Reagents were purchased from Wofen Medical Equipment Trading Co., Ltd.
Lupus anticoagulant (LA) detection was performed using the Dilute Russell’s Viper Venom Time (DRVVT) and silica clotting time (SCT) methods on a CS5100 automated coagulometer. Reagents were purchased from Siemens Medical Diagnostics GmbH, Germany.
Statistical analysis
2.3
Statistical analyses were performed using R software (version 4.2.2) and RStudio. A 2 × 3 mixed-design repeated measures ANOVA was conducted, with time (pre-treatment, post-treatment, and early pregnancy) as the within-subject factor and pregnancy outcome (successful vs. pregnancy loss) as the between-subject factor, to evaluate the main effects of time, group, and their interaction. When a significant overall time effect or time×group interaction was observed, one-way repeated measures ANOVA was performed within each group, followed by Bonferroni-corrected paired t-tests for pairwise comparisons between time points. In addition, independent-samples t-tests were used to compare differences between the successful pregnancy and pregnancy loss groups at each individual time point.
Continuous variables are presented as mean ± standard deviation (mean ± SD). All statistical tests were two-sided, and a p-value of < 0.01 was considered statistically significant.
Results
3
Baseline comparisons between the study group and the control group
3.1
There were no significant statistical differences in baseline characteristics, such as age, weight, height, body mass index (BMI), and menstrual cycle, between the study group and the control group (Table 2). Furthermore, there were no significant differences between the normal pregnancy group and the pregnancy loss group in terms of age, weight, height, BMI, menstrual cycle, and number of miscarriages (Table 3).
Baseline clinical characteristics and treatment regimens of the study population
3.2
Table 1 summarizes the baseline clinical characteristics and treatment regimens of the study cohort. All enrolled patients met the diagnostic criteria for recurrent pregnancy loss (≥3 consecutive miscarriages before 10 weeks of gestation). No patient had a history of fetal death at ≥10 weeks, prior placental insufficiency, or severe preeclampsia diagnosed before 34 weeks.
All participants received standardized anticoagulation therapy, including low-dose aspirin and low-molecular-weight heparin. There were no significant differences between the successful pregnancy and pregnancy loss groups in the use of hydroxychloroquine (31% vs. 37%, p = 0.702) or prednisone (15% vs. 11%, p = 0.760).
Comparison between the study and control groups
3.3
Serum aPS/PT IgM and aCL IgG in the study group were significantly higher than those in the control group (Table 4, P < 0.01). However, no significant differences were observed between the two groups for other antibodies, including aβ2GPI IgM/IgG/IgA, aCLIgM/IgA, aPS/PT IgG, and LA.
Results of the 2 × 3 mixed-design repeated measures ANOVA
3.4
The 2 × 3 mixed-design repeated measures ANOVA showed significant time effects for aCL IgG, aβ2GPI IgM, and aPS/PT IgM across the three time points (pre-treatment, post-treatment, and early pregnancy) (Table 5, P < 0.01). Significant group effects were also observed for LA1, LA1-SCT, aPS/PT IgG, and aPS/PT IgM, indicating marked differences between the successful pregnancy and pregnancy loss groups (Table 5, P < 0.01). In addition, both aPS/PT IgG and aPS/PT IgM demonstrated significant time × group interactions (Table 5, P < 0.01), reflecting distinct dynamic trajectories between the two outcome groups.
Within-group repeated measures ANOVA with Bonferroni-corrected pairwise comparisons
3.5
- aCL IgG: Both the successful pregnancy group and the pregnancy loss group exhibited significant time effects (Table 6, P < 0.01). In both groups, aCL IgG levels at post-treatment and early pregnancy were significantly lower than pre-treatment levels (Figure 1 and Table 6, P < 0.01), whereas no significant difference was observed between the post-treatment and early-pregnancy time points.
- aβ2GPI IgM: A significant time effect was detected in the successful pregnancy group (Table 6, P < 0.01), with early-pregnancy levels significantly lower than both pre-treatment and post-treatment levels (Figure 2 and Table 6, P < 0.01). No significant temporal changes were observed in the pregnancy loss group.
- aPS/PT IgG: A significant time effect was observed only in the pregnancy loss group (Table 6, P < 0.01). Early-pregnancy aPS/PT IgG levels were significantly higher than levels at both pre-treatment and post-treatment (Figure 3 and Table 6, P < 0.01). No significant temporal differences occurred in the successful pregnancy group. In addition, aPS/PT IgG levels showed minimal changes after treatment in both groups; however, the successful pregnancy group exhibited a slight decline in early pregnancy, whereas the pregnancy loss group demonstrated a marked increase (Table 6 and Figure 3). Consequently, the two groups displayed distinctly different patterns of change during early pregnancy (Table 5 and Figure 3, P interaction < 0.001).
- aPS/PT IgM: Both groups showed significant time effects (Table 6, P < 0.01), but the directions of change differed. In the successful pregnancy group, aPS/PT IgM levels at post-treatment and early pregnancy were significantly lower than pre-treatment levels (Figure 4 and Table 6, P < 0.01). In contrast, in the pregnancy loss group, early-pregnancy levels were significantly higher than both pre-treatment and post-treatment levels (Figure 4 and Table 6, P < 0.01). Moreover, aPS/PT IgM levels in the successful pregnancy group declined rapidly after treatment and remained consistently low thereafter (Table 6 and Figure 4). In contrast, the pregnancy loss group showed minimal change following treatment but exhibited a marked increase during early pregnancy (Table 6 and Figure 4), resulting in a dynamic trajectory that differed significantly from that of the successful pregnancy group (Table 5 and Figure 4, P interaction < 0.001).
Dynamic changes in aCL IgG levels in the successful pregnancy group and the pregnancy loss group at three time points (pre-treatment, post-treatment, and early pregnancy). The lines represent group mean values over time, with error bars indicating standard deviations. Asterisks above the plot denote statistically significant pairwise comparisons between time points (P < 0.01).
Dynamic changes in aβ2GPI IgM levels in the successful pregnancy group and the pregnancy loss group at three time points (pre-treatment, post-treatment, and early pregnancy). The lines represent group mean values over time, with error bars indicating standard deviations. Asterisks above the plot denote statistically significant pairwise comparisons between time points (P < 0.01).
Dynamic changes in aPS/PT IgG levels in the successful pregnancy group and the pregnancy loss group at three time points (pre-treatment, post-treatment, and early pregnancy). The lines represent group mean values over time, with error bars indicating standard deviations. Asterisks above the plot denote statistically significant pairwise comparisons between time points (P < 0.01).
Dynamic changes in aPS/PT IgM levels in the successful pregnancy group and the pregnancy loss group at three time points (pre-treatment, post-treatment, and early pregnancy). The lines represent group mean values over time, with error bars indicating standard deviations. Asterisks above the plot denote statistically significant pairwise comparisons between time points (P < 0.01).
Comparison between the pregnancy loss group and successful pregnancy group
3.6
The pregnancy loss group exhibited significantly higher aPS/PT IgM levels both after treatment and during early pregnancy compared with the successful pregnancy group (Table 7, p < 0.01). In addition, aPS/PT IgG levels during early pregnancy were also markedly higher in the pregnancy loss group (Table 7, p < 0.01). Apart from these differences, no significant variations were observed between the two groups across the three time points for the remaining antibodies, including β2GPI IgM/IgG/IgA, aCL IgM/IgG/IgA, and LA.
Discussion
4
This study systematically evaluated the dynamic changes of standard aPL antibodies and aPS/PT antibodies in APS-RPL patients before treatment, after treatment, and during early pregnancy, with the aim of elucidating the potential immunomodulatory mechanisms underlying pregnancy maintenance. By comparing the temporal antibody profiles between women with successful pregnancies and those who experienced pregnancy loss, we sought to investigate the association between immune dynamics and pregnancy outcomes from a longitudinal immunological perspective. Unlike traditional analyses focusing on antibody levels at a single time point, this study highlights the importance of antibody trajectories and group-specific differences over time. Such an approach provides valuable insights into the evolving immune responses associated with APS and their clinical implications while also offering new avenues for identifying high-risk individuals and optimizing pregnancy management strategies.
Previous studies have shown that aPS/PT antibodies have high diagnostic values in Chinese aPS patients and serve as important biomarkers and risk predictors for thrombosis and pregnancy loss (17). Elevated aPS/PT IgM levels in APS and RPL populations are strongly associated with adverse pregnancy outcomes (11, 12), and their sensitivity appears to exceed that of aCL and aβ2GPI antibodies (21). As one of the standard aPL antibodies, aCL—particularly aCL IgG—is well-recognized for its association with an increased risk of spontaneous miscarriage (22, 23). In line with these findings, our study demonstrated significantly higher levels of aPS/PT IgM and aCL IgG in the study group compared with the control group, suggesting that both antibodies may represent important immunologic contributors to heightened miscarriage risk. By contrast, no significant differences were observed in aβ2GPI antibodies or LA levels between the two groups. Although these markers are conventionally linked to thrombosis and pregnancy complications (24–26), the lack of association in our study may reflect factors such as limited sample size, substantial inter-individual variability in antibody levels, and differences in assay sensitivity across platforms (27, 28).
The mixed-design repeated measures ANOVA revealed heterogeneous patterns across different antibodies with respect to time effects, group effects, and their interactions. Among the standard aPL antibodies, aCL IgG and aβ2GPI IgM exhibited significant time effects, suggesting that immunotherapy and physiological changes during pregnancy may modulate their levels to varying degrees, whereas other standard antibodies showed no notable temporal fluctuations. Notably, both aPS/PT IgG and aPS/PT IgM exhibited significant group effects and time × group interactions, indicating that their temporal trajectories differed markedly between the successful pregnancy and pregnancy loss groups. These findings imply that, compared with traditional aPL antibodies, aPS/PT antibodies may possess greater sensitivity and clinical value in reflecting pregnancy-related immune alterations and predicting pregnancy outcomes (11). This observation provides a foundation for subsequent analyses of antibody dynamics and their clinical implications.
Further within-group repeated measures analyses revealed that the successful pregnancy group displayed a more consistent downward trend across multiple antibodies over time. Levels of aCL IgG, aβ2GPI IgM, and aPS/PT IgM were all significantly lower in early pregnancy compared with pre-treatment levels. This decline aligns with previous hypotheses proposing that “post-treatment immune burden reduction and early pregnancy-associated immune tolerance” contribute to favorable pregnancy outcomes (29, 30). In contrast, the pregnancy loss group exhibited distinctly different temporal patterns: although aCL IgG declined after treatment, aPS/PT IgG and aPS/PT IgM were not adequately suppressed and instead rose substantially during early pregnancy. Particularly for aPS/PT IgM, levels decreased in the successful group but increased in the loss group, demonstrating opposite directions of change. These divergent patterns suggest that whereas reductions in standard aPL antibodies may reflect partial treatment effects, the dynamic profiles of aPS/PT antibodies more accurately capture the success or failure of early pregnancy-related immune regulation.
Between-group comparisons across the three time points further highlighted the discriminative value of aPS/PT antibodies. Although baseline antibody levels were largely comparable between the groups, the pregnancy loss group showed significantly higher aPS/PT IgM levels after treatment and during early pregnancy, accompanied by an early-pregnancy elevation in aPS/PT IgG. Moreover, while the successful pregnancy group exhibited an overall decline or stabilization of immune markers in early pregnancy, the loss group displayed persistent or even exacerbated immune burden. These findings indicate that baseline antibody levels alone are insufficient to predict pregnancy outcomes; instead, the dynamic trajectories—particularly those of aPS/PT IgM and aPS/PT IgG—may serve as more informative immunological indicators. This conclusion is consistent with earlier reports identifying aPS/PT antibodies as risk-associated markers and further supports their potential clinical utility as predictors of adverse pregnancy outcomes (18–20).
This study has several limitations. First, as a retrospective analysis, inherent biases in data collection and documentation cannot be entirely avoided. Second, the sample size is relatively limited; although the results demonstrated highly consistent trends, their generalizability requires confirmation in larger, multicenter cohorts. In addition, variations in sensitivity and specificity across different detection platforms may introduce methodological variability. Finally, because low-titer ANA-positive patients were not stratified separately, the potential influence of ANA status on certain immune parameters cannot be completely excluded. Despite these limitations, the present study offers several notable strengths. To the best of our knowledge, this is the first investigation to use a longitudinal self-comparison design, evaluating dynamic changes in antibody levels at three key time points—before treatment, after treatment, and during early pregnancy—within both the successful pregnancy and pregnancy loss groups. In contrast to previous studies that predominantly relied on cross-sectional analyses, this three-time-point within-subject approach effectively minimizes inter-individual variability and strengthens the reliability of interpreting true immunological trajectories. Moreover, by applying a mixed-design repeated measures ANOVA, we systematically assessed time effects, group effects, and their interactions. The results clearly revealed significant time × group interactions for both aPS/PT IgG and aPS/PT IgM, with the two groups exhibiting opposite temporal trends. This pronounced immunodynamic divergence has not been adequately characterized in prior literature, underscoring the unique contribution of our study design. Complementing this, three-time-point between-group comparisons further revealed that the pregnancy loss group consistently maintained elevated levels of aPS/PT IgM and IgG after treatment and during early pregnancy, whereas the successful pregnancy group showed marked reductions or stabilization. These findings provide compelling evidence linking differential immune regulation to pregnancy outcomes.
Looking ahead, we plan to expand the sample size and conduct multicenter studies to enhance the robustness and generalizability of our conclusions. Additionally, integrating multi-platform testing and incorporating other immunologic markers—such as stratified ANA analyses—may offer a more comprehensive understanding of the maternal immune environment in pregnancy maintenance. Such efforts are expected to further support the development of more precise immunological intervention strategies for patients with recurrent pregnancy loss.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rai R Regan L. Recurrent miscarriage. Lancet. (2006) 368:601–11. doi: 10.1016/S 0140-6736(06)69204-0, 16905025 · doi ↗ · pubmed ↗
- 2Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. (2012) 98:1103–11. doi: 10.1016/j.fertnstert.2012.06.048, 22835448 · doi ↗ · pubmed ↗
- 3Ford HB Schust DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol. (2009) 2:76–83. 19609401 PMC 2709325 · pubmed ↗
- 4Vomstein K Feil K Strobel L Aulitzky A Hofer-Tollinger S Kuon RJ . Immunological risk factors in recurrent pregnancy loss: guidelines versus current state of the art. J Clin Med. (2021) 10:1–21. doi: 10.3390/jcm 10040869, 33672505 PMC 7923780 · doi ↗ · pubmed ↗
- 5Hennessy M Dennehy R Meaney S Devane D O'Donoghue K. A protocol for a systematic review of clinical practice guidelines for recurrent miscarriage. HRB Open Res. (2020) 3:12. doi: 10.12688/hrbopenres.13024.3, 33005862 PMC 7477641 · doi ↗ · pubmed ↗
- 6Pham M Orsolini G Crowson C Snyder M Pruthi R Moder K. Anti-phosphatidylserine prothrombin antibodies as a predictor of the lupus anticoagulant in an all-comer population. J Thromb Haemost. (2022) 20:2070–4. doi: 10.1111/jth.15792, 35722911 · doi ↗ · pubmed ↗
- 7Garcia D Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med. (2018) 378:2010–21. doi: 10.1056/NEJ Mra 1705454, 29791828 · doi ↗ · pubmed ↗
- 8Cervera R Serrano R Pons-Estel GJ Ceberio-Hualde L Shoenfeld Y de Ramón E . Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. (2015) 74:1011–8. doi: 10.1136/annrheumdis-2013-204838, 24464962 · doi ↗ · pubmed ↗