Case Report: Midgut malrotation presenting as left-sided appendicitis with secondary omental torsion: a diagnostic challenge in a child
Han Yao, Puneng Ma, Ruiqi Gao, Chenghao Zhanghuang, Xin Yi

TL;DR
A 12-year-old child presented with left-sided appendicitis and omental torsion due to congenital midgut malrotation, highlighting the need for early diagnosis in atypical cases.
Contribution
This case report emphasizes the diagnostic importance of considering midgut malrotation in children with left-sided appendicitis and omental abnormalities.
Findings
Midgut malrotation can lead to atypical presentations such as left-sided appendicitis and omental torsion.
Ultrasound is effective in detecting omental changes, while upper gastrointestinal contrast confirms malrotation.
Collaboration between radiologists and surgeons is crucial for managing atypical acute abdomen cases.
Abstract
Omental torsion is an uncommon cause of acute abdomen in children and is usually secondary to other intra-abdominal pathology. Congenital midgut malrotation can alter anatomic relationships and lead to atypical presentations. This case report aims to highlight that congenital malrotation should be considered when left-sided appendicitis is suspected, especially when omental abnormalities are present. We report a 12-year-old child who presented to a tertiary children's hospital in Southwest China with more than 48 h of abdominal pain and 24 h of fever after heavy intake of indigestible meat-based snacks. Initial ultrasound showed diffuse omental thickening in the left abdomen. Repeat ultrasound revealed a hypoechoic avascular area in the perisplanic omentum, raising suspicion of omental torsion. Preoperative computed tomography demonstrated left-sided ileocecal localization consistent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
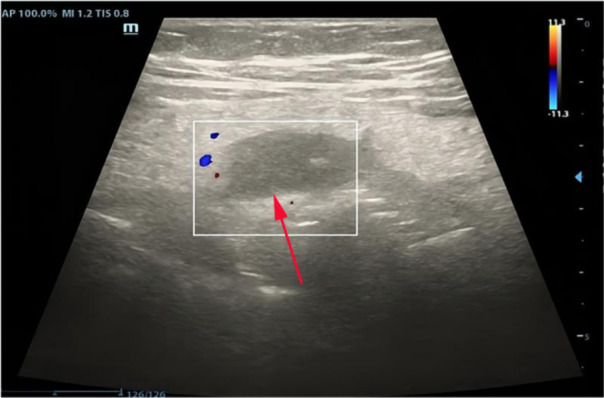 Figure 1
Figure 1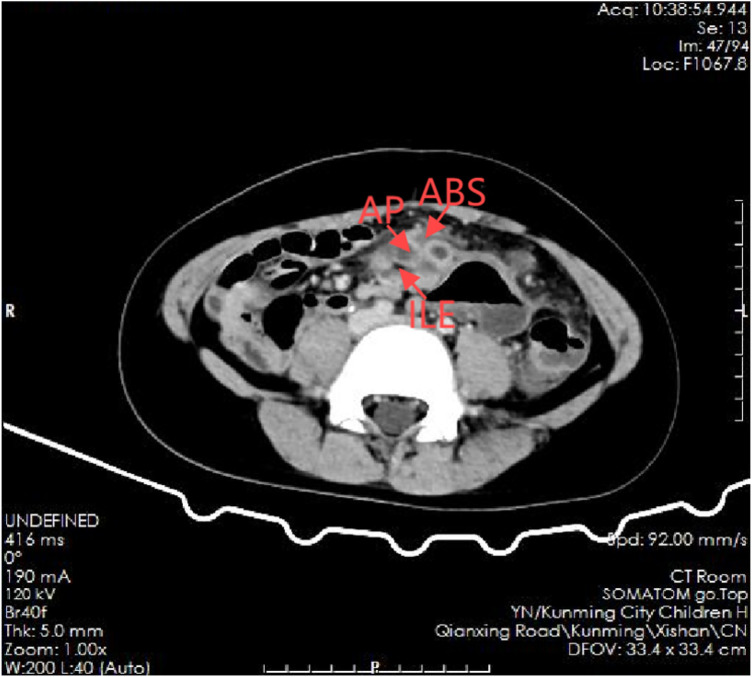 Figure 2
Figure 2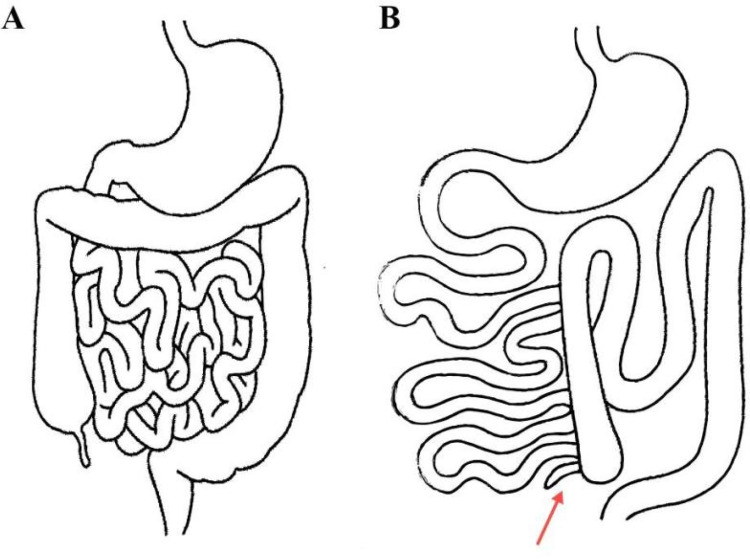 Figure 3
Figure 3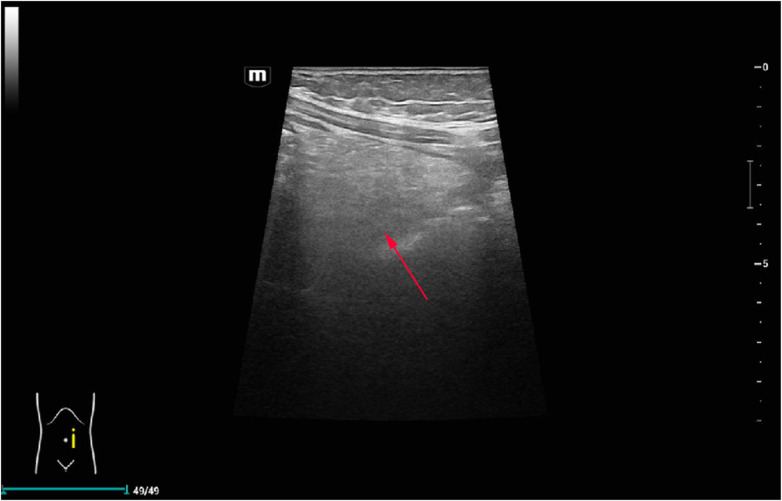 Figure 4
Figure 4| Step | Time point/stage | Key clinical & imaging findings | Diagnostic reasoning (What we thought) | Management decision (What we did) |
|---|---|---|---|---|
| 1 | Initial presentation (ED admission) | 12-year-old child with >48 h abdominal pain and 24 h fever; pain started after heavy intake of indigestible meat-based snacks; maximal tenderness and rebound in the left lower quadrant; bowel sounds present | Suspected acute peritonitis with a left-sided inflammatory focus; typical right-sided appendicitis pattern not present | Admitted with a working diagnosis of “abdominal pain; acute peritonitis?” and ordered laboratory tests and abdominal ultrasound |
| 2 | First ultrasound | Marked thickening of the mesentery and greater omentum in the left lower quadrant and lower abdomen; no confidently thickened appendix identified | Favored “left-sided omental/mesenteric inflammatory changes,” but appendicitis not confirmed; atypical acute abdomen | Continued close clinical observation and planned repeat imaging due to persistent symptoms |
| 3 | Follow-up ultrasound (after 1 day of persistent symptoms) | Repeat color Doppler US: diffuse mesenteric and omental thickening, predominantly on the left; thickened perisplenic omentum with a hypoechoic, avascular patch | New key sign of suspected omental torsion → high suspicion of secondary omental torsion | Listed “omental torsion + acute peritonitis” as major diagnostic consideration; decided to perform CT to evaluate bowel position and related pathology |
| 4 | Preoperative CT | CT confirmed the ileocecal region in the left lower abdomen; no midgut volvulus; localized inflammatory changes and small-volume ascites | Established: (1) left-sided ileocecal region → congenital midgut malrotation; (2) left-sided appendicitis with localized peritonitis; (3) omental involvement explaining US findings as secondary omental torsion | Reached a high preoperative suspicion of “left-sided appendicitis with secondary omental torsion on the background of malrotation”; planned emergency diagnostic laparoscopy. |
| 5 | Laparoscopic exploration | Purulent ascites; greater omentum migrated into the left lower abdomen, enveloping bowel; torsion of the omentum around the lower pole of the spleen; perforated appendix within a left lower quadrant abscess | Confirmed: congenital malrotation → left-sided cecum and appendix → perforated left-sided appendicitis + abscess → contiguous greater omentum with secondary torsion | Prioritized sepsis control: performed appendectomy with lavage and drainage; due to gross contamination, dense adhesions, and absence of frankly necrotic omentum, no formal omental resection or detorsion was attempted |
| 6 | Early postoperative course | Intravenous ceftriaxone + metronidazole for 1 week, plus ulinastatin; abdominal pain and fever resolved, inflammatory markers normalized, bowel function returned; discharged on postoperative day 10 | Clinical response confirmed that the initial operative strategy was effective and infection was controlled | No immediate Ladd procedure; planned clinical and imaging follow-up instead |
| 7 | Early postoperative ultrasound follow-up (∼1 week) | Doppler US: ileocecal region still located in the left abdomen (persistent malrotation) without volvulus; left abdominal greater omentum less thickened with homogeneous echotexture and preserved internal blood flow | Indicates that the omental torsion had resolved without infarction; malrotation persists as a stable anatomic substrate rather than an acute event | Continued conservative management with documentation of malrotation and explanation to the family about future risk and the need for vigilance |
| 8 | Mid-term outpatient follow-up (∼6 months) | Patient asymptomatic with no recurrent abdominal pain or obstructive symptoms | Supports that left-sided appendicitis and secondary omental torsion were successfully treated in a single operation and that malrotation is currently silent | Recommended long-term follow-up and advised that any new abdominal pain should prompt reassessment and consideration of elective Ladd procedure |
| Feature | Primary omental torsion | Secondary omental torsion |
|---|---|---|
| Underlying cause | Idiopathic; anatomical variants (redundant omentum, focal fat accumulation) | Occurs secondary to another intra-abdominal pathology (e.g., appendicitis, hernia, tumors, adhesions) |
| Typical age/population | More common in adults; rare in children | Relatively more frequent in children when torsion is triggered by focal inflammation |
| Usual location | Predominantly right-sided greater omentum | Corresponds to site of underlying pathology; may be left-sided or atypical |
| Imaging findings (US/CT) | Focal, right-sided, heterogeneous fatty mass with concentric or whirl-like pattern; no clear adjacent inflammatory source | Omental thickening or “whirl” adjacent to an identifiable inflammatory focus (e.g., inflamed appendix or abscess) |
| Management | Often surgical resection; laparoscopic omentectomy increasingly used | Management directed at primary pathology; omental resection or detorsion considered if necrotic, otherwise conservative management may be feasible |
| Prognosis | Good with timely diagnosis and treatment | Depends on control of underlying disease and extent of omental involvement |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOmental and Epiploic Conditions · Intestinal Malrotation and Obstruction Disorders · Congenital Anomalies and Fetal Surgery
Background
1
Omental torsion leading to omental infarction is a relatively rare condition, categorized into primary and secondary types, with the secondary form being more prevalent (1). Secondary omental torsion typically arises from underlying abdominal pathologies, such as appendicitis or other inflammatory processes, and is often identifiable (2). The greater omentum, a large apron-like structure composed of fatty and areolar tissue, is prone to torsion due to its mobility and variable attachments (3). This condition predominantly occurs on the right side due to the anatomical length of the right omentum.
The clinical presentation of omental torsion can be deceptive, often mimicking other acute abdominal conditions like appendicitis, leading to misdiagnosis (4). Pain is initially diffuse due to the stimulation of omental autonomic nerves and becomes localized as ischemia progresses and necrosis sets in. Ultrasound imaging is a valuable tool for detecting omental abnormalities, including omental thickening, increased echogenicity, and the characteristic “whirlpool sign.” However, differentiating omental torsion from other conditions can be challenging, especially when coexisting pathologies are present (5).
Congenital midgut malrotation, a developmental anomaly of intestinal rotation and fixation, can profoundly alter the anatomical relationships within the abdomen. These changes may predispose to atypical localization of the appendix and to unusual patterns of omental involvement. This case highlights the diagnostic complexity of secondary omental torsion in a pediatric patient with midgut malrotation and underscores the importance of a high index of suspicion and comprehensive imaging for accurate diagnosis and management in a tertiary pediatric center.
Case report
2
A 12-year-old child presented to a tertiary pediatric referral center in Southwest China in May 2024 with more than 48 h of abdominal pain and 24 h of fever. Symptoms began after heavy intake of indigestible meat-based snacks. The pain was constant and non-radiating, without a clear relationship to movement or meals. The child had reduced appetite, malaise, and loose stools but no vomiting and maintained normal urine output. Intermittent fever peaked at 38.7°C and recurred despite antipyretics administered at a local facility.
On admission, the working diagnosis was acute abdominal pain with suspected peritonitis, and laboratory tests and abdominal ultrasound were arranged.
Physical examination
2.1
The child was febrile (38.3°C) with tachycardia (108 beats/min) and a respiratory rate of 21 breaths/min. The general condition was stable. Abdominal examination revealed guarding and generalized tenderness, most prominent in the left lower quadrant with rebound tenderness. Bowel sounds were present.
Initial diagnostic investigations
2.2
Baseline abdominal ultrasound demonstrated marked thickening of the mesentery in the left lower quadrant and lower abdomen. The appendix was not clearly visualized or confidently identified as abnormal (Figure 1).
Initial abdominal ultrasound in the left lower quadrant. The greater omentum appears thickened with an internal hypoechoic avascular area (arrow), raising early suspicion of omental ischemia in an atypical left-sided acute abdomen.
Follow-up ultrasound findings
2.3
Because of persistent pain and fever, repeat color Doppler ultrasound was performed the next day. It showed diffuse mesenteric and omental thickening predominantly on the left side, and a hypoechoic avascular area within the perisplenic omentum, strongly suggestive of omental ischemia and torsion.
Contrast-enhanced CT showing a left-sided ileocecal region (arrow) and inflammatory changes consistent with left-sided appendicitis. AP, appendix; ABS, abscess; ILE, ileocecal region.
Preoperative CT findings
2.4
Preoperative contrast-enhanced CT demonstrated abnormal left-sided positioning of the ileocecal region, consistent with midgut malrotation, without evidence of midgut volvulus. Mild left-sided peritoneal thickening and a small volume of ascites were present. The appendix was identified in the left mid-abdomen with surrounding inflammatory changes, suggestive of appendicitis with localized peritonitis (Figure 2).
Intraoperative findings
2.5
Laparoscopy revealed purulent ascites. The greater omentum had migrated into the left lower abdomen and partially enveloped the bowel. Omental torsion was identified near the lower pole of the spleen. A left lower quadrant abscess contained a perforated, inflamed appendix. After confirmation, appendectomy with peritoneal lavage and drainage was performed. The ileocecal region was located in the left lower abdomen and was densely adherent to the sigmoid colon, omentum, and abdominal wall. Given the severe contamination and the lack of obvious omental necrosis, no additional procedure for the omentum was undertaken at the index operation. A schematic illustration of the intraoperative anatomic configuration is provided in Figure 3.
Schematic anatomy. (A) Normal intestinal rotation with the ileocecal region in the right lower quadrant and freely mobile greater omentum. (B) Midgut malrotation in the present case showing a left-sided ileocecal region and appendix (red arrow) with adjacent greater omentum in the left abdomen.
Postoperative diagnosis
2.6
The final diagnosis was congenital midgut malrotation with a left-sided appendix, complicated by perforated appendicitis, purulent peritonitis, and secondary omental torsion, without midgut volvulus.
Postoperative course
2.7
The child received intravenous ceftriaxone and metronidazole for 7 days. Abdominal pain and fever resolved, inflammatory markers normalized, and bowel function recovered. The patient was discharged on postoperative day 10 in good condition.
Follow-up Doppler ultrasound one week after surgery confirmed persistent malrotation without volvulus and showed preserved perfusion of the previously thickened omentum, indicating spontaneous resolution of the torsion without infarction (Figure 4). The patient remained asymptomatic at 6-month follow-up.
Postoperative follow-up Doppler ultrasound. The previously thickened left-sided omentum demonstrates restored internal blood flow (arrow) and more homogeneous echotexture, indicating resolution of the secondary torsion without infarction; persistent malrotation is noted without volvulus.
Diagnostic reasoning and missed preoperative diagnosis
2.8
Although preoperative CT suggested left-sided ileocecal localization compatible with congenital midgut malrotation, the working diagnosis focused on diffuse peritonitis and suspected omental pathology owing to the prominent inflammatory changes on ultrasound and the child's rapid clinical deterioration. In retrospect, malrotation should be framed as the primary anatomic substrate, with left-sided appendicitis and secondary omental torsion as downstream consequences.
In emergency settings, ultrasound and CT are typically obtained first. When the patient is hemodynamically stable, an upper gastrointestinal (UGI) contrast study remains the reference test for diagnosing malrotation with or without volvulus. In this emergency scenario, a preoperative UGI series was not performed, which limited the level of anatomic certainty before surgery. Table 1 summarizes the sequential diagnostic reasoning process from initial clinical suspicion through imaging, operative findings, and final diagnosis.
Discussion
3
Omental torsion is rare in children and most often occurs as a downstream event secondary to other intra-abdominal pathology. In our patient, congenital midgut malrotation—without volvulus—established an atypical left-sided ileocecal position that predisposed to left-sided appendicitis and localized peritonitis; the resulting inflammation likely triggered secondary torsion of the adjacent greater omentum. This causal hierarchy reconciles the imaging and operative findings and also explains why the initial ultrasound, although sensitive to omental abnormalities, did not immediately reveal the underlying anatomic variant. The comparison summary table of primary and secondary greater omentum torsion is shown in Table 2.
To our knowledge, this combination of congenital midgut malrotation, left-sided perforated appendicitis, and secondary omental torsion has rarely been reported in children.
Mechanistically, malrotation alters cecal and small-bowel fixation, narrows the mesenteric base, and reconfigures the spatial relationship between bowel and omentum. These changes can facilitate tethering or torque on the omentum in the presence of adjacent inflammation (e.g., appendicitis), predisposing to secondary torsion. A closely analogous presentation has been described by Emanuwa et al., where a left-sided cecum was found tethered by torted omentum at laparotomy, supporting the same causal sequence proposed here (6).
From an imaging perspective, both ultrasound and computed tomography (CT) play essential roles in the diagnosis and evaluation of omental lesions. Ultrasound can delineate the characteristic echogenic thickening of the greater omentum and is particularly advantageous in identifying focal hypoechoic regions with absent internal Doppler signals. These features are critical for distinguishing the nature of omental pathology. For instance, in cases of inflammatory myofibroblastic tumor (IMT), ultrasound may reveal a hypoechoic mass, consistent with the typical sonographic appearance of omental lesions (7). However, when the child is hemodynamically stable, an upper gastrointestinal (UGI) contrast study remains the reference investigation for establishing the diagnosis of malrotation (with or without volvulus) (8). In our emergency setting, a preoperative UGI was not obtained, which is a recognized limitation that can reduce anatomic certainty before surgery.
The Ladd procedure is widely regarded as the standard treatment for intestinal malrotation. It entails division of the Ladd bands, widening of the mesenteric base, repositioning the small bowel to the right and the colon to the left, and appendectomy, with the goal of preventing volvulus and future obstructive events. With advances in minimally invasive surgery, laparoscopic Ladd has become an increasingly feasible option, particularly in the absence of midgut volvulus (9). The laparoscopic approach offers the advantages of minimal invasiveness and a shorter recovery period. Studies demonstrate that laparoscopic Ladd in adults and adolescents is safe and effective, relieving symptoms and improving quality of life (10). In addition, it is associated with shorter operative and hospital times and a lower rate of postoperative complications, making it an attractive therapeutic choice (11). Given this child's perforated appendicitis and purulent peritonitis, our index operation prioritized source control (appendectomy, lavage, drainage), with planned interval assessment for the need and timing of Ladd based on recovery and follow-up.
In our patient, the index operation prioritized source control in the context of perforated appendicitis with purulent peritonitis. Extensive adhesions, gross contamination, and the lack of obvious omental necrosis led us to manage the omental torsion conservatively. This approach was justified by the subsequent ultrasound, which demonstrated preserved omental perfusion and resolution of edema. In children with partial omental torsion and severe peritonitis, limiting operative time and avoiding additional resection may be reasonable, provided that close postoperative imaging and clinical follow-up are ensured.
When contextualizing this case, we found only a few pediatric reports describing the combination of congenital malrotation, left-sided appendicitis, and secondary omental torsion. Most published pediatric series of omental torsion involve primary right-sided lesions without malrotation. Our case therefore adds to the limited literature and underscores that left-sided omental abnormalities in children should prompt deliberate consideration of malrotation, especially when imaging suggests an atypical location of the appendix or ileocecal region.
This report has several limitations. No intraoperative photographs were captured because of the emergent and contaminated field; a schematic illustration (Figure 3) is therefore used to depict the malrotated anatomy and left-sided appendix. Although this limits direct visual corroboration, the integrated clinical, imaging, and operative data provide educational value and highlight a practical diagnostic pitfall—namely, that left-sided omental abnormalities with appendiceal signs should trigger careful assessment for malrotation in the preoperative differential diagnosis. Longer-term follow-up is also needed to determine whether and when a Ladd procedure will be required to mitigate future volvulus or obstruction risk.
Conclusion
4
In children with left-sided appendicitis and omental abnormalities, congenital midgut malrotation should be considered early as the primary anatomic substrate to optimize diagnosis and operative planning. Ultrasound and CT rapidly characterize inflammation and abnormal localization, whereas a UGI series remains the reference test for confirming malrotation in stable patients. In contaminated emergencies, operative priorities should focus on source control, with interval assessment of the need and timing of a Ladd procedure under close clinical and imaging follow-up.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu J Tang R Duan G. Laparoscopic treatment of primary omental torsion in children: a case report. Asian J Surg. (2023) 46(9):4046–7. 10.1016/j.asjsur.2023.04.04737117059 · doi ↗ · pubmed ↗
- 2Le Roux F Gennuso F Lipsker A Mauvais F. Omental torsion, a rare cause of acute surgical abdomen. J Visc Surg. (2013) 150(6):421–2. 10.1016/j.jviscsurg.2013.09.00124269124 · doi ↗ · pubmed ↗
- 3PogorelićZ KatićJ Gudelj K MrklićI VilovićK Perko Z. Unusual cause of acute abdomen in a child–torsion of greater omentum: report of two cases. Scott Med J. (2015) 60(3):e 1–4. 10.1177/003693301558112925838282 · doi ↗ · pubmed ↗
- 4Madha ES Kane TD Manole MD. Primary omental torsion in a pediatric patient: case report and review of the literature. Pediatr Emerg Care. (2018) 34(2):e 32–4. 10.1097/PEC.000000000000123028816771 · doi ↗ · pubmed ↗
- 5Alexopoulos V Sinopidis X Louta A Damaskos C Garmpis N Tsourouflis G Primary omental torsion in children in the laparoscopy era: what have we learned so far? in Vivo. (2024) 38(3):1030–41. 10.21873/invivo.1353638688642 PMC 11059881 · doi ↗ · pubmed ↗
- 6Emanuwa OF Ayantunde AA Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J Emerg Surg. (2011) 6(1):22. 10.1186/1749-7922-6-2221801417 PMC 3158108 · doi ↗ · pubmed ↗
- 7Chen Z Sang L Zhang Y Bian D Tao C Wang X. Greater omentum imaging-reporting and data system: establishing the grade of benign and malignant lesions of the greater omentum using ultrasonography. Cancer Imaging. 2020 20(1):54. 10.1186/s 40644-020-00332-z 32746917 PMC 7398257 · doi ↗ · pubmed ↗
- 8Birajdar S Rao SC Bettenay F. Role of upper gastrointestinal contrast studies for suspected malrotation in neonatal population. J Paediatr Child Health. (2017) 53(7):644–9. 10.1111/jpc.13515 PMID: 28425590.28425590 · doi ↗ · pubmed ↗