Paracentral Acute Middle Maculopathy Associated With Dengue Fever
Salil Mehta

TL;DR
A rare case of paracentral acute middle maculopathy (PAMM) is reported in a patient following dengue fever, highlighting the need for ocular evaluation in such cases.
Contribution
This case report is one of the few to associate PAMM with dengue fever and suggests a possible link between dengue-induced inflammation and retinal ischemia.
Findings
A 33-year-old male developed PAMM following dengue fever with symptoms including blurred vision and a scotoma.
OCT imaging showed hyperreflective areas in the inner retina, consistent with PAMM.
Treatment with prednisolone led to improved visual acuity and reduced retinal lesions.
Abstract
Newer imaging technique systems have led to an increased interest in the anatomical localization of retinal disease. The clinical and optical coherence tomography (OCT) features of paracentral acute middle maculopathy (PAMM) have been increasingly described and are classically defined by a hyperreflective band at the level of the inner nuclear layer (INL). Symptoms typically include blurred central vision with a paracentral scotoma. Potential causes include retinal vascular diseases and systemic disorders. We present the clinical and OCT findings of a 33-year-old male patient with PAMM following dengue fever. The patient presented with a five-day history of fever, chills, severe body aches, and a generalized body rash. On day 1, he had undergone a series of investigations to determine the cause, and the test results were positive for dengue fever (Rapid NS antigen 1 45.47 S/Co…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
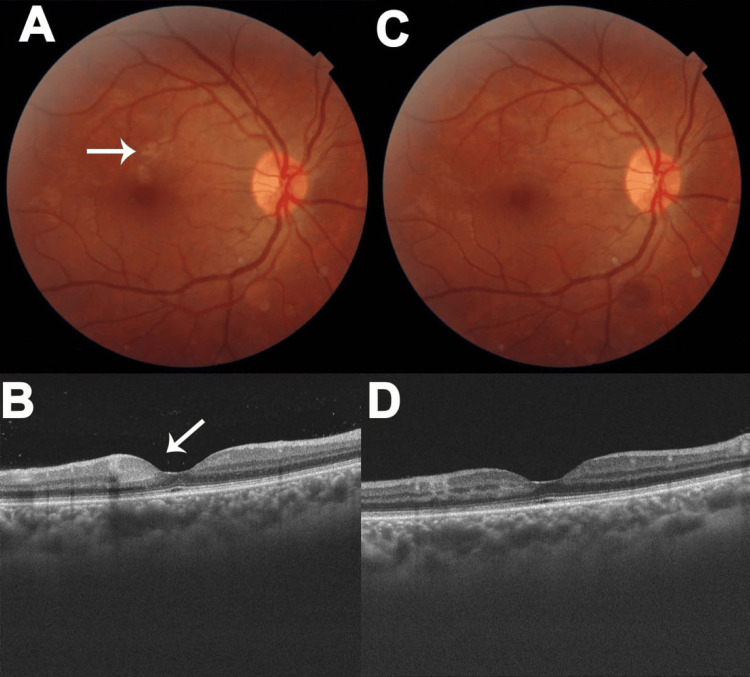 Figure 1
Figure 1| Parameter | Values | Normal Range |
| Day1 - Day 2 | ||
| Hemoglobin | 16.0 gm/dl | 13.0-17.0 gm/dl |
| Hematocrit | 48.2% | 40-50% |
| White Cell Count | 2530/mm3 | 4000-10,000 /mm3 |
| Platelet Count | 122,000/mm3 | 150,000-410,000 /mm3 |
| Day 5 | ||
| Hemoglobin | 14.50 gm/dl | 13.0-17.0 gm/dl |
| Hematocrit | 43.30% | |
| White Cell Count | 5700 | 4000-10,000/mm3 |
| Absolute Neutrophil Count | 1100 | 2000-7000 |
| Absolute Lymphocyte Count | 3800 | 1000-3000 |
| Absolute Eosinophil Count | 0.0 | 20-500 |
| Absolute Basophil Count | 0.0 | 20-100 |
| Neutrophils | 20.00 | 40.0-80.0% |
| Lymphocytes | 66.00 | 20.0-40.0% |
| Monocytes | 14.00 | 2.0-10.0% |
| Eosinophils | 0.0 | 1.0-6.0% |
| Basophils | 0.0 | 1.0-2.0% |
| Platelet Count | 77,000 | 150,000-410,000/mm3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Retinal and Optic Conditions · Ocular Diseases and Behçet’s Syndrome
Introduction
A number of lesions, termed white dot syndromes, marked by multiple, white-to-yellow inflammatory lesions, located at the level of the outer retinal layers and the choroid, have been reported in the literature. These include acute posterior multifocal placoid pigment epitheliopathy, multiple evanescent white dot syndrome, multifocal choroiditis with panuveitis, and acute zonal occult outer retinopathy [1]. One phenotype, acute macular neuroretinopathy (AMN), first described by Bos and Deutman, is classically described as reddish-brown, wedge-shaped lesions in the macular area. In contrast to other white dot syndromes, which are primarily inflammatory, AMN is thought to be a consequence of the noninflammatory ischemia of the retinal capillaries, usually the outer plexiform layer (OPL) and outer nuclear layer (ONL) [2].
Paracentral acute middle maculopathy (PAMM) is now increasingly being recognized as another ischemic pathology characterised by the appearance of hyperreflective lesions at the level of the inner nuclear layer (INL), more superficial than the lesions seen in AMN. Symptoms typically include blurred central vision with a paracentral scotoma. Potential causes include retinal vascular diseases and systemic disorders, including diabetic retinopathy and arterial and venous occlusions [2]. PAMM following dengue fever has only rarely been reported. We present the clinical and optical coherence tomography (OCT) findings of a 33-year-old male patient with PAMM following dengue fever.
Case presentation
A 33-year-old male presented with a five-day history of fever, chills, severe body ache, and a generalized body rash. On day one, he had undergone a series of investigations for the cause, and test results were positive for dengue fever (Rapid NS antigen 1 45.47 S/Co (positive > 1.0 S/Co) with dengue immunoglobulin (Ig)M positivity. At this time, his platelet count was 123,000 (normal 200,000 to 500,000/mm3). Test results for chikungunya infection were negative.
On day five, he noticed bleeding from his gums, which correlated to a drop in his platelet count to 77,000/mm^3^. He was admitted for observation. On admission, he was afebrile with normal examination findings of the cardiovascular, respiratory, and nervous systems. The salient hematological test results on day one/two and day five are shown in Table 1.
At this time, he complained of a scotoma in front of the right eye with mildly blurred vision. His visual acuity was 6/12, N8 in the right eye and 6/6, N6 in the left eye. Slit lamp examination of the anterior segment was normal in either eye. The clinical and OCT findings of a dilated fundus examination are shown in Figure 1. This revealed multiple grayish-white areas of retinitis in the superior macula of the right eye, with associated hemorrhages (Figure 1A). An OCT scan revealed multiple areas of hyperreflectivity in the inner retina, primarily from the inner nuclear and inner plexiform layers (Figure 1B). Assuming an immune-mediated etiology, he was treated empirically with oral prednisolone 40 mg/day with tapering every week. At day seven, there was a significant reduction in his symptoms, with an increase in visual acuity to 6/9, N6, and a decrease in the size of the retinal lesions (Figure 1C) and the inner retina hyperreflectivity (Figure 1D). The left eye was normal on both occasions.
Optical coherence tomography of dilated right eye fundusA) Fundus photograph of the right eye, showing grayish-white retinal lesions (arrow); B) OCT scan showing hyperreflectivity of the inner nuclear and inner plexiform layers; C) Fundus photograph on day five showing reduction of the retinal lesions; D) OCT scan showing reduction of the hyperreflectivity
Discussion
PAMM was initially described as a variant of AMN. Rahimy et al. were the first to describe PAMM and its clinical and OCT findings, in the form of hyper-reflective lesions in the middle retina, usually located in the INL or outer plexiform layer junction (OPL) [3]. Several subsequent studies have expanded our understanding of PAMM. In a large retrospective study, Limoli et al. identified 78 patients from a diverse background. Simultaneous retinal vascular disease occurred in 38 patients (16 with arterial occlusion and 20 with venous occlusion) as compared to 40 patients without. The average age at presentation was 54.5 years, with a largely male cohort. PAMM was seen as an isolated phenomenon or secondary to retinal vascular disease. In the absence of retinal vascular disease, patients tended to have an increased prevalence of systemic vasculopathies, suggesting the pivotal role of ischemia [4].
The capillary plexuses of the retina are organized into three layers: the superficial capillary plexus (SCP), intermediate capillary plexus (ICP), and deep capillary plexus (DCP). These plexuses are independently autoregulated, thus ensuring an adequate blood flow to all parts of the inner and middle retina. The DCP perfuses the middle retina, but its perfusion pressure is lower compared to the SCP and the ICP. Additionally, the high metabolic demand of the outer nuclear layer has led to the development of a watershed zone concept that renders the DCP uniquely vulnerable to hemodynamic dysfunction, with a subsequent ischemia of the middle retina, specifically, the inner nuclear layer, with a possible extension to the inner plexiform layer. The inner nuclear layer thinning following PAMM tends to confirm this hypothesis [5].
Dengue fever is a viral fever that is caused by one of the four serotypes of the dengue virus, which are members of the flaviviridae family. An estimated 100-400 million infections occur every year, with the disease being endemic in parts of Africa, the Americas, and Southeast Asia. Numerous hematological abnormalities occur in acute dengue infection, including thrombocytopenia, leukopenia, and increased hematocrit. Of these, a rise in hematocrit is an indicator of plasma leakage into the extravascular spaces and the subsequent reduction of intravascular volume, which could lead to circulatory disturbances. This could be widespread ischemia or localized organ ischemia [6].
A wide spectrum of ocular complications has been described in dengue. The pathogenesis of dengue fever-related ocular manifestations is now thought to be immune-mediated. Most lesions appear approximately a week after the appearance of fever. In one study, as many as 24.1% of inpatients noted visual symptoms, commonly blurred vision or scotomas [7]. Potential mechanisms include immune complex deposition, complement activation, and autoantibody formation. Interestingly, the dengue virus may incite autoimmune reactions against numerous ocular tissues, such as the retina, retinal pigment epithelium, or the choroid. Commonly seen lesions include subconjunctival hemorrhage, anterior uveitis, intermediate uveitis, and posterior uveitis (retinitis, chorioretinitis, and neuroretinitis) or retinal vasculitis [7].
Retinal vasculitis is commonly seen and usually co-exists with retinitis or retinochoroiditis. The use of Fundus fluorescein angiography (FFA), led to the discovery of the classical findings including early vascular blockage or delayed perfusion, followed by mid- and late-phase vessel wall hyperfluorescence and localized areas of blocked fluorescence. The increasing use of OCT permitted the characterization of AMN with the identification of disruptions of the ellipsoid zone, external limiting membrane, and interdigitation zones and hyperreflectivity of the ONL and the OPL [8].
PAMM following dengue fever has only rarely been reported. In a single case report, Ferreira et al. describe a 19-year-old patient with symptoms suggestive of dengue fever. Dilated fundus evaluation revealed bilateral optic disc edema and deep hemorrhages. An OCT evaluation revealed a hyperreflectivity involving the outer nuclear and plexiform layers. Following a course of oral steroids, the visual acuity significantly improved with residual INL thinning [9].
The patient we describe was diagnosed with dengue fever based on a positive rapid NS1 and positive IgM titers. Thrombocytopenia was noticed on admission, but this rapidly improved on supportive therapy. His hematocrit was normal on day 1 and day 5, suggesting the absence of a profound systemic plasma leakage. The retinal lesions were in the middle retina layers of the peripheral macula rather than in the central macula. The clinical phenotype would be consistent with a diagnosis of PAMM.
We hypothesize that dengue-induced local inflammatory or hemoconcentration processes may have led to DCP circulatory compromise, leading to ischemia, especially in the area supplied by the DCP. Chanthick and co-workers have suggested that a viral endotheliitis may lead to the production of proinflammatory cytokines and chemokines and consequent leakage. Transcellular hyperpermeability is also hypothesized to be important in the pathogenesis of plasma leakage in patients with dengue fever [10]. The findings we describe are those detected during his hospitalization. A further follow-up would have led to a changed OCT picture, which would shed further light on the long-term evolution of these lesions. This remains an area for future study.
Conclusions
Dengue fever is a common infectious disease with multiple hematological and ocular manifestations. While many manifestations, especially the hemorrhagic lesions, are well described, PAMM has only recently been described. While an ophthalmic evaluation is not yet part of the standard protocol for these patients, we suggest adopting it, as asymptomatic patients or those with subtle symptoms may be overlooked. In particular, the onset of a central scotoma may suggest the onset of PAMM, and this is an OCT test to rule out this possibility. Ophthalmologists should be aware of this entity and its differential diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The white dot syndromes Am J Ophthalmol Quillen DA Davis JB Gottlieb JL Blodi BA Callanan DG Chang TS Equi RA 53855013720041501387810.1016/j.ajo.2004.01.053 · doi ↗ · pubmed ↗
- 2Acute macular neuroretinopathy: a comprehensive review of the literature Surv Ophthalmol Bhavsar KV Lin S Rahimy E Joseph A Freund KB Sarraf D Cunningham ET Jr 5385656120162697328710.1016/j.survophthal.2016.03.003 · doi ↗ · pubmed ↗
- 3Paracentral acute middle maculopathy spectral-domain optical coherence tomography feature of deep capillary ischemia Curr Opin Ophthalmol Rahimy E Sarraf D 2072122520142461414810.1097/ICU.0000000000000045 · doi ↗ · pubmed ↗
- 4Exploring patient demographics and presence of retinal vascular disease in paracentral acute middle maculopathy Am J Ophthalmol Limoli C Raja LD Wagner SK 18218926020243810475810.1016/j.ajo.2023.12.010 · doi ↗ · pubmed ↗
- 5Paracentral acute middle maculopathy and the organization of the retinal capillary plexuses Prog Retin Eye Res Scharf J Freund KB Sadda S Sarraf D 1008848120213278395910.1016/j.preteyeres.2020.100884 · doi ↗ · pubmed ↗
- 6Severe dengue in the intensive care unit J Intensive Med Tejo AM Hamasaki DT Menezes LM Ho YL 1633420243826396610.1016/j.jointm.2023.07.007PMC 10800775 · doi ↗ · pubmed ↗
- 7Dengue-related ocular complications: spectrum, diagnosis, and management Pathogens Deng J Zou Y Yang M 14202510.3390/pathogens 14090872 PMC 1247284441011772 · doi ↗ · pubmed ↗
- 8Ophthalmic complications of dengue Emerg Infect Dis Chan DP Teoh SC Tan CS 2852891220061649475610.3201/eid 1202.050274 PMC 3373088 · doi ↗ · pubmed ↗