Potential benefits of JAK inhibitor therapy in Blau syndrome: a case report
Yu Wang, Xiao-juan Yu, Zhuoli Zhang

TL;DR
A patient with Blau syndrome showed improved kidney function after treatment with the JAK inhibitor baricitinib, suggesting it may be an effective therapy for this rare inflammatory disorder.
Contribution
This case report highlights baricitinib as a potential treatment for Blau syndrome, particularly in cases with renal involvement.
Findings
Baricitinib rapidly normalized renal function in a Blau syndrome patient with granulomatous nephritis.
JAK inhibition may offer advantages over TNF-α inhibitors in managing Blau syndrome.
The p.R334W NOD2 mutation in this case caused constitutive NF-κB activation and excessive cytokine production.
Abstract
Blau syndrome is a rare autoinflammatory disorder caused by gain-of-function mutations in the NOD2 (nucleotide binding oligomerization domain containing 2 receptor) gene. Blau Syndrome presents with the diagnostic triad of chronic polyarticular synovitis, recurrent uveitis, and dermatitis. Notably, patients often develop systemic granulomatous inflammation affecting multiple organs, particularly the kidney and liver. Here we report a case of Blau syndrome presented with early-onset arthritis, uveitis, and renal involvement, evidenced by granulomas tubulointerstitial nephritis. Genetic testing showed a pathogenic p.R334W NOD2 mutation demonstrating constitutive NF-κB activation and excessive proinflammatory cytokine production. While initial corticosteroid therapy improved articular and ocular symptoms, renal dysfunction persisted until baricitinib (4 mg/day) initiation, which rapidly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1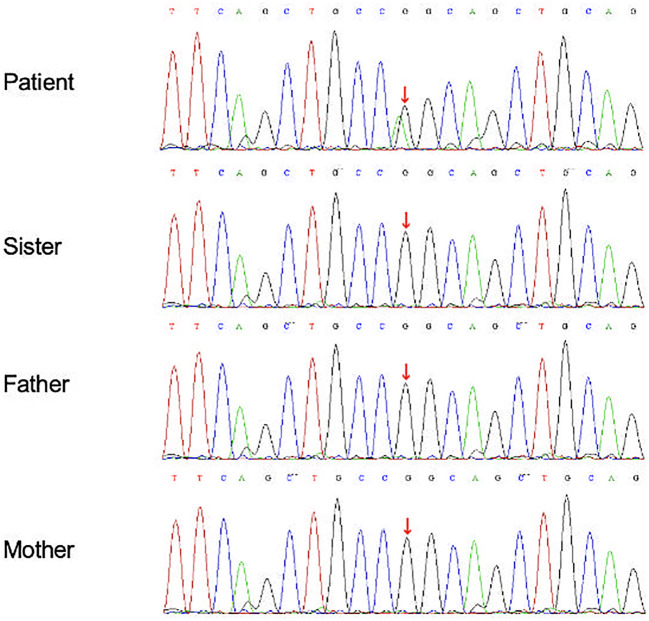 Figure 2
Figure 2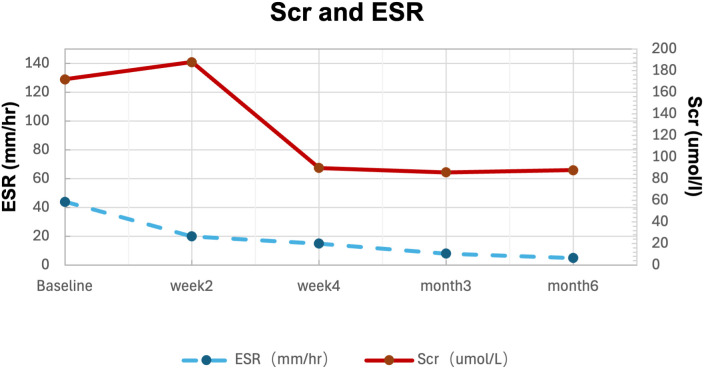 Figure 3
Figure 3| Baseline | week2 | week4 | month3 | month6 | Normal range | |
|---|---|---|---|---|---|---|
| ESR (mm/hour) | 44 | 20 | 15 | 8 | 5 | 0-20 |
| CRP (mg/L) | 11.2 | 8 | 6 | 4 | 5 | <10 |
| WBC (/ul) | 8240 | 9800 | 6900 | 4230 | 4780 | 4000-10000 |
| Neutrophils (/ul) | 7200 | 8230 | 4820 | 4130 | 3720 | 1500-8000 |
| Lymphocytes (/ul) | 950 | 900 | 850 | 740 | 780 | 700-3100 |
| Hemoglobin (g/l) | 110 | 115 | 114 | 120 | 118 | 130-175 |
| Platelets (/ul) | 280,000 | 275,000 | 208,000 | 214,000 | 202,000 | 100,000-300,000 |
| Scr (umol/L) | 172 | 188 | 90 | 86 | 88 | 65.4-119.3 |
| urinary microalbumin (mg/L) | 87.3 | 65.2 | 19 | 17 | 15 | 0-19 |
| urinary red blood cells (/HP) | 10 | 5 | 2 | 3 | 2 | 0-3 |
| prednisone (mg/d) | 60 | 55 | 50 | 30 | 5 | |
| Baricitinib (mg/d) | 0 | 4 | 4 | 4 | 4 |
- —National Natural Science Foundation of China10.13039/501100001809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Amyloidosis: Diagnosis, Treatment, Outcomes · Eosinophilic Disorders and Syndromes
Introduction
Systemic auto-inflammatory diseases (SAIDs) are a growing group of disorders caused by a dysregulation of the innate immune system. Furthermore, it has been observed that 40-60% of patients exhibiting symptoms consistent with the typical presentations of SAIDs do not receive a definitive diagnosis. Although corticosteroids is the most used drug due to anti-inflammatory effect, its use seems insufficient in Blau syndrome. 68% of the patients with ocular manifestations needed a combination therapy with immunosuppressive agents and/or biological drugs (1). Methotrexate, thalidomide, sulfasalazine, mycophenolate et al. were used to treat Blau syndrome, however, the efficacy is difficult to ascertain and may have side effects. Considering Blau syndrome as a poor factor for uveitis, monoclonal antibody drug such as adalimumab and infliximab is preferred biological therapies, and short-term systemic corticosteroid should be considered only as bridging therapy. Here, we present a case of successful treatment of baricitinib in combination with steroids in a patient diagnosed with early onset sarcoidosis (EOS) or Blau syndrome with a NOD2 gene mutation.
Case report
A 22-year-old male presented with a 15-year history of progressive arthritis and joint deformities, accompanied by recent-onset blurred vision and elevated serum creatine persisting for 3 months. Previous treatment with traditional Chinese herbs had proven ineffective.
Physical examination revealed multiple joint deformities, particularly in the hands, with no associated skin changes. Radiographs demonstrated joint space narrowing, without erosion (Figure 1A, B). Ophthalmological evaluation identified the presence of bilateral granulomatous anterior uveitis (Panel c and d), evidenced by mutton-fat keratic precipitates, a positive Tyndall phenomenon and visual acuity of 0.6 and 0.8 in the right and left eyes, respectively. Intraocular pressure was normal. Urinalysis showed proteinuria with microalbumin 87.3 mg/L (0–19) and microscopic hematuria (10 red blood cells/HP). Serum creatinine (172 μmol/L) and urea (8.77 mmol/L) were elevated, alongside increased erythrocyte sedimentation rate (ESR) of 44 mm/h and C-reactive protein (CRP) of 11.2 mg/L. Autoantibody screening was negative. The serum angiotensin-converting enzyme was found to be within normal parameters. Infectious etiologies (cytomegalovirus, HIV and syphilis) and tuberculosis (interferon-gamma release assay and PPD) were excluded. A subsequent renal biopsy revealed non-necrotizing granuloma (Panel E).
(a) Symmetric flexion contractures of bilateral proximal interphalangeal joints 2 to 5. (b) Joint space narrowing and sclerosis on X-ray. (c) off-white deposits-mutton fat keratic precipitates on the inner corneal surface in the right eye (arrows). (d) Bilateral retinal vasculitis on fluorescein angiography. (e) Pathology showed granulomatous tubulointerstitial nephritis. Multiple focal and patchy infiltrate of lymphocytes, monocytes, and some plasma cells in the renal interstitium with fibrosis, and granulomatous structures (arrowhead), accompanied by multinucleated giant cell reactions (dotted arrow).
Given the triad of arthritis, uveitis, and systemic granulomatous involvement, Blau syndrome and sarcoidosis were considered. Subsequent gene screening revealed a de novo NOD2 mutation (c.1001G>A, chr16:50744823 p. Arg334Gln), absent in his parents and sister, confirming a diagnosis of EOS with NOD2 mutation (Figure 2).
Gene sequencing of the NOD2 gene by sanger whole genome sequencing (WGS) for the patient and his family. The patient had a de-novo heterozygous mutation in the NOD2 gene (c.1001G>A, chr16:50744823 p. Arg334Gln). The gene analysis of his parents and sister were normal.
Initial therapy with prednisone 1mg/kg/d improved uveitis and arthritis within 2 weeks, but Scr rose to 188 umol/L. Since he refused injectable therapies, baricitinib 4mg/day was initiated as a steroid-sparing agent based on its JAK1/2 inhibitory mechanism. Within two weeks, arthritis and uveitis resolved completely, serum Scr normalized (90 umol/L), and inflammatory markers (ESR <15 mm/hour, and CRP <5mg/L) remained suppressed. Over six months, prednisone was successfully tapered to 5mg daily without disease relapse or any side effects (Figure 3; Table 1).
Serum creatine and ESR changes with timing in response to treatments.
Discussion
Blau syndrome (2) is a rare autosomal dominant disorder characterized by clinical triad of arthritis, uveitis, skin rash and granulomatous inflammation. The causative gene CARD15/NOD2 was identified in 2001, and encodes a protein involved in innate immune regulation, with shared pathogenic mechanisms in inflammatory bowel disease (3). The NOD2 gene encodes three functional domains: 2 caspase recruitment domains (CARDs), a central nucleotide oligomerization domain (NOD/NACHT) and a C-terminal leucine-rich repeat region (LRR).
In the present case, genetic analysis revealed a pathogenic NOD2 gain-of-function mutation (p.R334W), which has been previously associated with panuveitis (4). This mutation induces constitutive activation of NF-κB pathway, independent of peptidoglycan-independent mechanism, resulting in excessive production of proinflammatory cytokines (5). Furthermore, IFN-γ has been identified as a critical mediator in the pathogenesis of granulomatous inflammation, a hallmark feature of this disorder. Blau syndrome typically manifests in early childhood, with classical triad of polyarticular synovitis, granulomatous uveitis and papular rash. Systemic involvement may also extend to multiple organs, including renal (glomerulonephritis), hepatic (granulomatous hepatitis), neurological (cranial neuropathies), and vascular (arteritis) systems. Ocular manifestations often progress relentlessly, potentially leading to severe visual impairment. The same phenotype occurring without family history is termed Early Onset Sarcoidosis, though both inherited and sporadic forms are now commonly classified under the umbrella term Blau syndrome. The differential diagnosis of Blau syndrome should include juvenile idiopathic arthritis, especially in cases presenting with atypical features such as camptodactyly, cutaneous eruptions, or granulomatous panuveitis, particularly with a positive family history of similar symptoms. Early diagnosis is crucial to prevent irreversible end-organ damage, particularly vision loss from progressive ocular inflammation.
Pediatric anterior uveitis may frequently present asymptomatically in until advanced, irreversible sight-threatening complications develop. While anterior chamber inflammation is often difficult to be detected, the presence of mutton-fat keratic precipitates can be seen with the naked eyes. The presence of these large deposit (macroscopic aggregates of polymorphonuclear cells, lymphocytes, and epithelioid cells) strongly suggests a pathognomonic feature of granulomatous disease and warrants immediate intervention (2). Current therapeutic strategies include corticosteroids, interlukin-1 inhibitors, and TNF-α antagonists, with varying degrees of efficacy reported in a few clinical studies (6). Emerging evidence suggests the JAK inhibitors may represent a promising therapeutic alternative for refractory cases. Tofacitinib has shown clinical efficacy in previous reports (7), with one documented case of successful maintenance therapy following discontinuation (8).
In our patient, while corticosteroids therapy achieved partial improvement in arthritis and uveitis within the first week, renal dysfunction persisted. Initiation of baricitinib 4mg/day resulted in rapid resolution of both articular and ocular manifestations, with concomitant normalization of renal function. Sustained clinical remission was achieved, enabling prednisone tapering to 5mg/day by 6 months of follow-up.
Blau syndrome represents a severe autoinflammatory disorder characterized by frequent treatment resistance. The absence of established therapeutic guidelines, compounded by the rarity of the disease, necessitates reliance on expert consensus for clinical management. Although corticosteroids remain the most frequently employed first-line therapy, they often prove inadequate for complete disease control, particularly in cases with multiorgan involvement (1). Notably, ocular manifestations affect 32% of patients with Blau syndrome frequently result in permanent visual impairment. Patients with systemic involvement typically require aggressive immunosuppressive regimens, with biologic agents reserved for refractory cases. While evidence remains limited for IL-1, IL-6, and JAK inhibitors, TNF-α antagonists have demonstrated efficacy in inducing hepatic remission, in 5 Blau syndrome patients as reported by Sinharay et al (9). Our findings align with previous reports of Baricitinib efficacy in a treatment-resistant Blau syndrome under after methotrexate, adalimumab, and tofacitinib failure (8), particularly in cases with renal granulomatous involvement. As a selective inhibition of JAK1/JAK2 inhibitor, the mechanism of baricitinib can directly targets the pathological activation of granulomatous inflammation, in modulating the dysregulated inflammatory cascade in Blau syndrome, offering a targeted therapeutic approach for this challenging condition.
Conclusion
Baricitinib emerges as a viable therapeutic option for refractory Blau syndrome, particularly in cases with renal granulomatous involvement. Its demonstrated efficacy in achieving rapid clinical remission and steroid-sparing effects warrants further investigation through controlled clinical studies to establish optimal dosing protocols and long-term safety profiles in this rare disease population.
Serum creatine (solid line) and ESR (dotted line) levels. Left arrow indicates prednisone 60mg/d; right arrow indicates Baricitinib 4mg/d.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lassoued Ferjani H Kharrat L Ben Nessib D Kaffel D Maatallah K Hamdi W . Management of Blau syndrome: review and proposal of a treatment algorithm. Eur J Pediatr. (2024) 183:1–7., PMID: 37735224 10.1007/s 00431-023-05204-9 · doi ↗ · pubmed ↗
- 2Imaging inflammation in early-onset sarcoidosis: granulomatous anterior uveitis in a 7-year-old girl. Lancet. (2023) 401:1963., PMID: 37301585 10.1016/S 0140-6736(23)00550-0 · doi ↗ · pubmed ↗
- 3Pillai P Sobrin L . Blau syndrome-associated uveitis and the NOD 2 gene. Semin Ophthalmol. (2013) 28:327–32., PMID: 24010719 10.3109/08820538.2013.825285 · doi ↗ · pubmed ↗
- 4Zhong Z Ding J Su G . Genetic and clinical features of blau syndrome among chinese patients with uveitis. Ophthalmology. (2022) 129:821–8. 10.1016/j.ophtha.2022.03.01435314268 · doi ↗ · pubmed ↗
- 5Sfriso P Caso F Tognon S Galozzi P Gava A Punzi L . Blau syndrome, clinical and genetic aspects. Autoimmun Rev. (2012) 12:44–51. 22884558 10.1016/j.autrev.2012.07.028 · doi ↗ · pubmed ↗
- 6Matsuda T Kambe N Takimoto-Ito R . Potential benefits of TNF targeting therapy in blau syndrome, a NOD 2-associated systemic autoinflammatory granulomatosis. Front Immunol. (2022) 13:895765., PMID: 35711422 10.3389/fimmu.2022.895765 PMC 9195515 · doi ↗ · pubmed ↗
- 7Zhang S Cai Z Mo X Zeng H . Tofacitinib effectiveness in Blau syndrome: a case series of Chinese paediatric patients. Pediatr Rheumatol Online J. (2021) 19:160., PMID: 34781959 10.1186/s 12969-021-00634-x PMC 8594202 · doi ↗ · pubmed ↗
- 8Álvarez-Reguera C Prieto-Peña D Herrero-Morant A . Clinical and immunological study of tofacitinib and baricitinib in refractory blau syndrome: Case report and literature review. Ther Adv Musculoskelet Dis. (2022) 14:1759720 X 221093211., PMID: 35510170 10.1177/1759720 X 221093211 PMC 9058350 · doi ↗ · pubmed ↗