The infection–microbiome–immunity axis in bladder cancer: mechanistic insights and therapeutic perspectives
Shen Pan, Wanlin Cui, Jiaman Lin, Zhujun Wang, Zhenhua Li, Bitian Liu

TL;DR
This review explores how infections, gut and urinary microbiome imbalances, and immune system aging contribute to bladder cancer and suggests new treatment strategies.
Contribution
The paper provides a conceptual framework linking infection, microbiome dysbiosis, and immune dysfunction in bladder cancer.
Findings
Microbial dysbiosis and chronic infections drive bladder cancer through inflammation and immune disruption.
Immunosenescence worsens microbial persistence and weakens antitumor immunity in bladder cancer.
Microbiome-targeted and immunomodulatory therapies show promise for restoring immune-microbial balance.
Abstract
Bladder cancer (BC) represents a paradigm of infection-associated malignancy in which microbial dysbiosis, immune aging, and tumor microenvironmental remodeling converge to shape disease progression. Increasing evidence highlights the dual role of the urinary and gut microbiota in modulating bladder carcinogenesis through infection-driven inflammation and immune dysfunction. Chronic exposure to uropathogens and microbial imbalance disrupts epithelial integrity, promotes extracellular matrix degradation, and reprograms local immune signaling, collectively fostering a tumor-permissive niche. Concurrently, immunosenescence exacerbates microbial persistence and impairs antitumor immunity, reinforcing a pathogenic feedback loop between infection and immune decline. This review integrates current insights from microbiome research, tumor immunology, and microbial pathogenesis to delineate the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
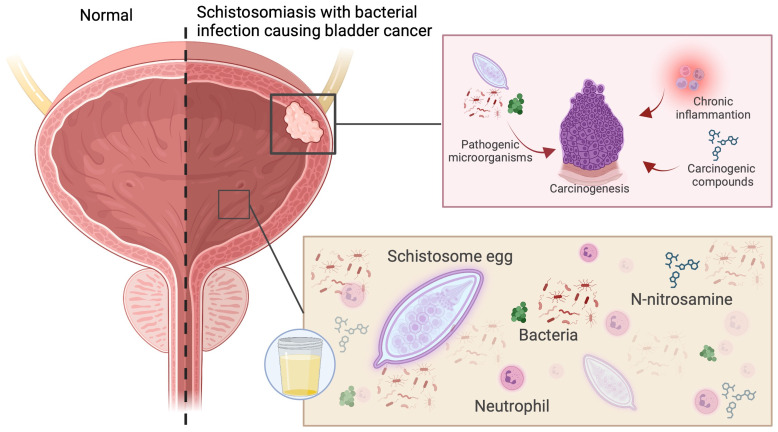 Figure 1
Figure 1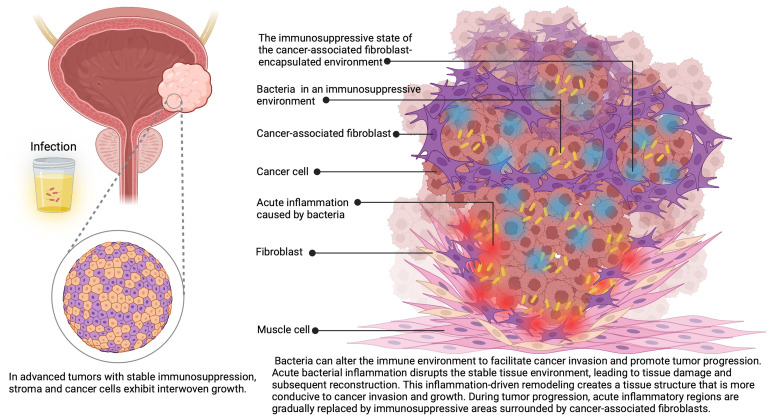 Figure 2
Figure 2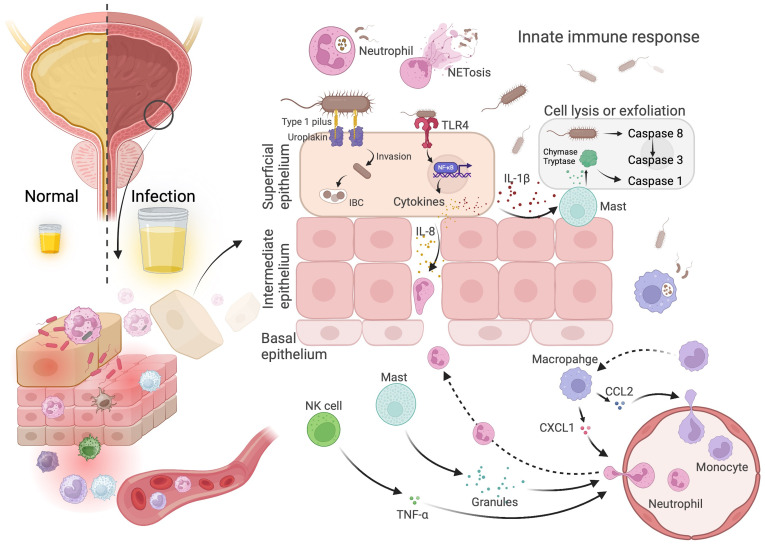 Figure 3
Figure 3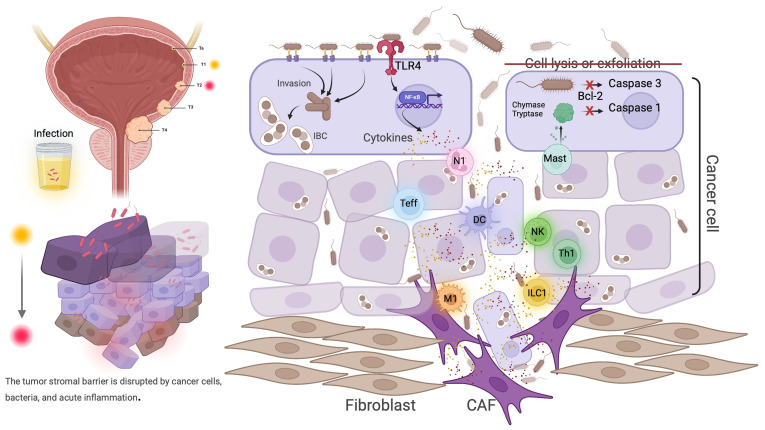 Figure 4
Figure 4| Study | Year | BCa | Non-BCa | Sample | Alpha diversity | Beta diversity | Increase in abundance/phyla | Increase in abundance/genera | Study purpose |
|---|---|---|---|---|---|---|---|---|---|
| Bučević Popović et al. ( | 2018 | 12 | 11 | Mid-stream urine | NS | NS | Actinobacteria, Proteobacteria (BC); Firmicutes, Bacteroidetes (controls) | Fusobacterium, Streptococcus, Peptoniphilus (BC); Corynebacterium | BC vs. healthy controls |
| Wu et al. ( | 2018 | 31 (26 NMIBC and 5 MIBC) | 18 | Mid-stream urine | Different | Different | Proteobacteria, Firmicutes, Actinobacteria, Bacteroidetes (BC) | Acinetobacter, Anaerococcus, Rubrobacter, Sphingobacterium (BC) | BC vs. healthy controls |
| Bi et al. ( | 2019 | 29 | 26 | Mid-stream urine | Different | Different | Tenericutes, Proteobacteria (BC) | Actinomyces (BC) | BC vs. healthy controls |
| Liu et al. ( | 2019 | 22 (17 MIBC and 5 NMIBC) | 12 | Tissue | Different (Shannon index) | Different | Proteobacteria, Actinobacteria (BC); Firmicutes, Bacteroidetes (non-tumor tissue) | Escherichia-Shigella, Acinetobacter, Ralstonia, Cupriavidus, Pelomonas, Sphingomonas (BC); Lactobacillus, Prevotella_9, Ruminococcaceae (non-tumor tissue) | BC vs. adjacent non-cancerous |
| Chipollini et al. ( | 2020 | 27 (15 MIBC and 12 NMIBC) | 10 | Mid-stream urine | Different | NS | NR | Bacteroides and Faecalbacterium (BC) | BC vs. healthy controls |
| Zeng et al. ( | 2020 | 62 males (51 NMIBC and 11 MIBC) | 19 | Mid-stream urine | Different | Different | Proteobacteria, Actinobacteria (BC) | Acinetobacter, Anaerococcus, Sphingobacterium (BC) | BC vs. controls; recurrence analysis |
| Mansour et al. ( | 2020 | 10 urine, 14 tumor tissues | Mid-stream urine | NS | NS | Firmicutes, Proteobacteria (BC tissues); Firmicutes, Actinobacteria, Cyanobacteria, Bacteroidetes (urine) | Akkermansia, Bacteroides, Clostridium sensu stricto, Enterobacter, Klebsiella (BC tissues); Lactobacillus, Corynebacterium, Streptococcus, Actinomyces (urine) | BC tissues vs. urine samples | |
| Pederzoli et al. ( | 2020 | 49 | 59 | Mid-stream urine | NS | Different (BC vs. Controls in Female urine) | Klebsiella (female BC urine); Burkholderia (BC tissue) | Not provided | Sex-based microbiota differences |
| Hussein et al. ( | 2021 | 43 (29 NMIBC and 14 MIBC) | 10 | Mid-stream urine (healthy), Cath/cystoscopy (cancer patients) | NS | Different (BC vs. controls) | Proteobacteria (NMIBC); Firmicutes, Proteobacteria (MIBC); Firmicutes, Proteobacteria (BCG responders) | Cupriavidus (NMIBC); Hemophilus, Veillonella (MIBC); Serratia, Brochothrix, Negativicoccus, Escherichia-Shigella, Pseudomonas (BCG responders) | NMIBC vs. MIBC; BCG post-therapy recurrence analysis |
| Parra-Grande et al. ( | 2021 | 32 | 26 | Tissue | Different | NR | Proteobacteria, Fusobacteria (BC) | Fusobacterium, Barnesiella, Escherichia-Shigella (BC) | BC vs. adjacent non-cancerous |
| Oresta et al. ( | 2021 | 51 | 10 | Mid-stream urine and catharized urine | Different (MIBC vs. NMIBC) | Different (MIBC vs. NMIBC) | Proteobacteria, Firmicutes (NMIBC) | Veillonella, Corynebacterium, Ruminococcus (NMIBC) | MIBC vs. NMIBC |
| Qiu et al. ( | 2022 | 40 (12 recurrent, 28 non-recurrent NMIBC) | Mid-stream urine | Different (Higher alpha diversity in recurrent) | Different | Proteobacteria, Actinobacteria, Firmicutes (recurrence) | Pseudomonas, Acinetobacter, Staphylococcus, Corynebacterium (recurrence) | Recurrence analysis | |
| Sun et al. ( | 2023 | 22 (15 MIBC, 7 NMIBC) | Tissue | Different | Different | Proteobacteria (dominant in MIBC) | Ralstonia (dominant in MIBC) | MIBC vs. NMIBC | |
| Hussein et al. ( | 2023 | 68 (26 non-recurrent and 42 recurrent) | Urine | NS | Different | NR | Escherichia-Shigella, Helococcus (BCG responders); Veillonella, Bifidobacterium (BCG non-responders) | BCG post-therapy recurrence analysis | |
| Bilski et al. ( | 2024 | 41 (21 males and 20 females) urine | 10 tissues | Mid-stream urine | Different | Different | Proteobacteria (male urine), Firmicutes (female urine); Proteobacteria (BC tissue), Firmicutes (non-tumor tissue) | Escherichia (male urine), Streptococcus (female urine); Fusobacterium, Prevotella (BC tissue), Lactobacillus (non-tumor tissue) | Sex-based microbiota differences (urine) |
| Yao et al. ( | 2024 | 22 | 22 | Tissue | Different (except for BCG therapy) | Different (except for BCG therapy) | Proteobacteria (BC); Actinobacteria (non-tumor tissue) | Pseudomonas, Porphyrobacter, Acinetobacter (BC); Staphylococcus, Lactobacillus (non-tumor tissue); Erythrobacter, Corynebacterium, Streptomyces, Mycolicibacterium (BCG durable responders); Pasteurella, Simkania (BCG non-durable responders) | BC vs. adjacent non-cancerous; BCG post-therapy recurrence analysis |
| Knorr et al. ( | 2024 | 11 (urine); 57 (10 fresh tissue, 23 FFPE BCG responders, 24 FFPE BCG non-responders) | Urine | Different | Different | NR | Lactobacillus gasseri, Lactobacillus johnsonii (BCG Responders); Corynebacterium kroppenstedtii, Streptococcus spp. (BCG Non-Responders) | BCG post-therapy recurrence analysis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Gut microbiota and health · Urinary Tract Infections Management
Introduction
1
Bladder cancer (BC) is the second most common genitourinary malignancy globally, with around 550,000 new cases and 200,000 deaths each year (1). Despite significant advances in surgical and systemic therapies, BC continues to exhibit high recurrence rates and poor survival, particularly in advanced or muscle-invasive disease. For advanced BC, the prognosis remains poor, with a 5-year survival rate below 40% (2). This persistent clinical burden underscores the need to better understand non-genetic and microenvironmental factors that shape tumor initiation and progression. In addition to microbial and immune factors, key environmental risk factors for BC include tobacco smoking, which accounts for approximately 50% of cases in developed countries, and occupational exposure to aromatic amines and other toxic chemicals (e.g., in dye, rubber, and leather industries), which contribute to 5-10% of cases. These exposures can induce DNA damage and chronic inflammation, potentially interacting with the urinary microbiome by promoting dysbiosis—such as reduced microbial diversity and enrichment of pro-inflammatory taxa like Proteobacteria—which may exacerbate infection-driven carcinogenesis (3, 4). Exploring these links could reveal how smoking-induced alterations in gut and urinary microbiota amplify oxidative stress and immune dysregulation in the bladder. In recent years, the human microbiome has emerged as a critical determinant of oncogenesis, influencing cancer risk, immune modulation, and therapeutic outcomes across multiple organ systems. The discovery of a resident microbiota within the urinary tract has challenged the long-held assumption of its sterility, paving the way for new research exploring the role of host-microbe interactions in bladder carcinogenesis.
Historically, the role of infection in BC was recognized in regions endemic for Schistosoma haematobium, where chronic parasitic inflammation predisposes to squamous cell carcinoma of the bladder (5–7). Beyond schistosomiasis, growing evidence indicates that bacterial infections—particularly recurrent urinary tract infections (UTIs)—contribute to urothelial carcinogenesis through persistent inflammation, oxidative stress, and epithelial injury. Uropathogenic Escherichia coli (UPEC), responsible for over 70% of UTIs, can invade bladder epithelial cells, form intracellular bacterial communities, and establish chronic reservoirs that are resistant to host clearance. These persistent infections elicit prolonged inflammatory signaling and reactive oxygen species (ROS) production, both of which promote DNA damage and mutagenesis (8–10). Moreover, interactions between schistosomes and cohabiting bacteria—such as Fusobacterium, Sphingobacterium, and Enterococcus—can enhance carcinogenicity through the generation of N-nitrosamines and estrogen-like DNA-reactive metabolites (11–13) (Figure 1). Epidemiologic studies further suggest that recurrent UTIs, pyuria, and chronic cystitis correlate with increased risk of BC recurrence and progression, reinforcing the clinical relevance of infection-mediated pathways.
Schistosoma infection is often accompanied by microbial infections, which can trigger chronic inflammation and the accumulation of harmful substances, collectively contributing to the development of bladder cancer.
An additional layer of complexity arises from aging-related immune decline, or immunosenescence. Bladder cancer predominantly affects older adults, with a median age at diagnosis of approximately 73 years (14). Aging is accompanied by diminished immune surveillance, reduced antigen presentation, and impaired cytotoxic T-cell responses, which collectively reduce the host’s ability to eliminate pathogens and emerging tumor cells (2, 15, 16). Immunosenescence also facilitates microbial persistence, establishing a vicious cycle in which chronic infection perpetuates inflammation, and inflammation accelerates immune deterioration (17–21). This interplay between microbial dysbiosis and immune aging represents a critical yet underexplored determinant of BC pathogenesis. Understanding this dynamic crosstalk may reveal why elderly individuals are more susceptible to both infection and cancer, and why immune-based therapies exhibit variable efficacy in this population.
The duality of microbes as both carcinogenic agents and therapeutic tools further highlights the complexity of host–microbe interactions in BC. The attenuated strain Mycobacterium bovis Bacillus Calmette–Guérin (BCG) remains the cornerstone of intravesical therapy for non–muscle-invasive bladder cancer (NMIBC), harnessing microbial activation of innate and adaptive immunity to suppress tumor recurrence (22). This paradox—where microbes can either promote or suppress tumorigenesis—underscores the necessity of disentangling the mechanistic nuances governing microbial behavior within the bladder milieu. Clarifying the context-dependent effects of microbial exposure is essential to advancing precision interventions that exploit beneficial microbial functions while mitigating pathogenic consequences (23).
In this context, the present review aims to synthesize current knowledge on the microbiome–infection axis in bladder cancer and to propose a unifying conceptual framework linking microbial dysbiosis, chronic inflammation, and immunosenescence to tumor initiation and progression. We first examine evidence from clinical and experimental studies delineating how infection-driven inflammatory signaling contributes to urothelial carcinogenesis. We then explore the composition and ecological dynamics of urinary and gut microbiota in BC, identifying microbial signatures associated with disease progression and therapeutic response. Subsequently, we integrate mechanistic insights into how microbes and immune aging remodel the tumor microenvironment (TME) through epithelial barrier disruption, immune reprogramming, and extracellular matrix modification. Finally, we discuss therapeutic implications, emphasizing microbiome-targeted and immunomodulatory strategies that hold promise for restoring microbial–immune homeostasis and improving clinical outcomes.
By bridging microbiology, immunology, and cancer biology, this review positions the microbiome not as a peripheral feature but as a central determinant of bladder cancer pathogenesis. Understanding the intricate relationship between infection, microbial ecology, and host immunity will be essential for developing next-generation diagnostic tools and personalized therapeutic strategies that move beyond the tumor-centric paradigm toward a holistic model of host–microbe–tumor interaction.
Infection-driven microbiome dysregulation in BC
2
Chronic and recurrent infections are among the most significant environmental pressures shaping the bladder’s microbial ecosystem and influencing tumor initiation. The urothelial surface, once thought to be sterile, is now recognized as a dynamic microbial niche whose composition is constantly modulated by host immunity, urinary flow, and exposure to pathogens. When these regulatory mechanisms fail—particularly under conditions of persistent infection or age-related immune decline—the resulting microbial imbalance, or dysbiosis, can initiate a cascade of inflammatory and mutagenic processes that contribute to bladder carcinogenesis.
Pathogenic infections and carcinogenic inflammation
2.1
Chronic infection by E. coli, the primary pathogen responsible for 70% of UTIs, has been implicated as a potential carcinogenic factor. Histopathological studies show that persistent E. coli infection alone induces epithelial dysplasia in the mucosal lining and promotes inflammatory cell infiltration into the lamina propria. When combined with nitrosamine precursors, chronic infection significantly increases the incidence of bladder lesions, surpassing the effects of nitrosamine precursors alone. This synergy highlights the critical role of infection-driven inflammation in bladder carcinogenesis (17). Kawai et al. further demonstrated that E. coli-derived lipopolysaccharide (LPS) significantly enhances N-methyl-N-nitrosourea (MNU)-induced bladder carcinogenesis, with inflammation and oxidative stress, driven by reactive oxygen species (ROS), playing key roles in this process (24). However, these findings, largely based on animal models, may not fully capture the complexities of human BC. Additionally, genetic and environmental variations limit the direct applicability of these results to clinical settings. Therefore, future research should focus on validating these mechanisms in human populations while accounting for these influencing factors.
UTIs and prognosis of BC
2.2
The connection between inflammation and bladder cancer (BC) progression is well-established. Sazuka et al. found that preoperative pyuria is closely associated with intravesical recurrence after transurethral resection of bladder tumor (TURBT), suggesting its role in predicting recurrence risk (19). Similarly, Jing et al. highlighted the importance of tumor-neutrophil interactions within the TME as a key driver of BC progression, emphasizing the critical role of inflammation in this process (25). Abd-El-Raouf et al. demonstrated that E. coli infection accelerates BC progression by inducing epithelial-mesenchymal transition (EMT), stem cell-like behaviors, and metabolic reprogramming (26). Nesi et al., in their systematic review, identified chronic inflammation as a central mechanism in BC pathophysiology (27), while Russell et al. further supported the inflammatory hypothesis by showing that epigenetic reprogramming induced by uropathogenic E. coli influences BC outcomes (28). Although the role of inflammation in BC progression is widely recognized, there remains some disagreement on its exact contribution. While some studies focus on the direct effects of inflammation on tumorigenesis, others suggest a more complex interplay involving microbial dysbiosis and immune suppression. Furthermore, most studies rely on mechanistic or single-center data, which may oversimplify the multifactorial nature of BC progression. To address these discrepancies, future research should adopt longitudinal studies with integrated approaches that assess inflammation, microbial composition, and tumor dynamics across diverse populations.
Prognostic biomarkers in infection-associated BC
2.3
Clinical studies have identified pyuria and recurrent UTIs as negative prognostic factors in BC patients. Vermeulen et al. reported that recurrent UTIs significantly increase the risk of developing BC (29). Azuma et al. identified pyuria as a poor prognostic indicator in patients with NMIBC and found it correlated with lower survival rates (21). Similarly, Singh et al. showed that preoperative pyuria and an elevated neutrophil-to-lymphocyte ratio (NLR) independently predict poor outcomes (18). Satake et al. also highlighted the prognostic value of preoperative pyuria in NMIBC patients (20). Although these studies emphasize the relevance of pyuria and recurrent UTIs as prognostic markers, inconsistencies remain in sample sizes and study designs. Many rely on single-center populations or small cohorts, which may introduce sampling bias and limit the generalizability of the results. To improve the accuracy of prognostic assessments, future studies should adopt multicenter designs with larger and more diverse populations to better define the value of these biomarkers across different clinical and demographic contexts.
Microbiome composition and its clinical correlates
3
The recognition that the bladder harbors a distinct microbial ecosystem has fundamentally transformed our understanding of urinary tract biology and its contribution to disease. Advances in metagenomic sequencing and culture-independent techniques have revealed that both the urinary and gut microbiota undergo profound compositional shifts during BC development. These alterations—manifesting as reduced microbial diversity, loss of beneficial commensals, and enrichment of opportunistic pathogens—reflect a disrupted ecological equilibrium, or dysbiosis, that can influence immune homeostasis, inflammatory signaling, and tumor behavior. Importantly, the specific microbial signatures observed in urine, tissue, and stool samples from BC patients provide valuable insights into the pathophysiology of the disease and its potential diagnostic and prognostic biomarkers (12, 30–35) (Table 1).
Urinary microbiota and BC
3.1
Studies on the urinary microbiome in BC patients have revealed significant alterations in microbial diversity and composition. However, findings across studies remain inconsistent. Popovic et al. and Wu et al. analyzed urine samples using 16S rRNA sequencing but reported differing results. Popovic et al. observed no significant differences in microbial diversity or abundance between BC patients and healthy controls, while Wu et al. reported higher alpha diversity in BC patients, noting differences at the genus level (36, 37). Wu et al. specifically identified higher Shannon and Simpson diversity indices in BC patients compared to controls, with Streptococcus and Escherichia-Shigella as dominant taxa (36, 37). Bi et al. found reduced abundances of Bifidobacterium and Lactobacillus in BC patients and identified Actinomyces europaeus as a potential biomarker for the disease (38). In contrast, Chipollini et al. reported reduced alpha diversity in BC patients, whereas Zeng et al. found alpha diversity significantly higher in BC patients, with a 145% increase in the Chao1 index and a 123% increase in the Ace index compared to controls (35, 39). Hussein et al. further supported the reduction of Lactobacillus abundance in urine of BC patients (40). These discrepancies may arise from variations in sequencing platforms, data analysis strategies, sample types (urine vs. tissue), and patient characteristics such as tumor stage and treatment history. Additionally, the urinary microbiome is highly influenced by external factors, including diet and antibiotic use, which may not be uniformly controlled across studies. To better elucidate the role of the urinary microbiome in BC, future research should incorporate larger cohorts and standardized methodologies for sample collection and data analysis.
Tissue-resident microbiota and BC
3.2
Changes in the microbiota within BC tissues are closely linked to the TME. Liu et al. performed 16S rRNA sequencing on 22 cancerous and 12 adjacent normal tissues, reporting significantly lower alpha diversity in cancer tissues, indicating reduced microbial diversity in BC (41). Mansour et al. compared microbiota in 10 catheter urine samples and 14 TURBT-resected tumor tissues, finding significantly higher abundances of Akkermansia, Bacteroides, Clostridium, Enterobacter, and Klebsiella in cancer tissues, while Staphylococcus and Lactobacillus were consistently present in both sample types (42). Further studies corroborated these findings. Parra-Grande et al. observed lower microbial richness in tumor tissues compared to paired non-tumor tissues, alongside higher Actinobacteria levels in non-tumor samples, supporting its potential protective role against BC (43). Similarly, Pederzoli et al. identified Klebsiella as more prevalent in the urine of female BC patients, while Burkholderia was enriched in cancer tissues (44). Yao et al., using RNA sequencing, highlighted the enrichment of Pseudomonas, Porphyrobacter, and Acinetobacter in cancer tissues, suggesting their potential involvement in BC progression (45). While multiple studies consistently report a reduction in microbial diversity within BC tissues compared to normal tissues. These variations may stem from differences in sample types (tumor tissue vs. urine), patient demographics (gender, age, lifestyle), and analytical approaches (16S rRNA sequencing vs. metagenomic sequencing). Additionally, the microbial composition may undergo dynamic changes at different stages of BC. Therefore, future longitudinal studies with standardized methodologies are essential to elucidate the evolving role of microbiota in BC development and progression.
Microbes associated with BC progression and recurrence
3.3
Alterations in the bladder microbiome are closely associated with BC progression and recurrence, with distinct microbial patterns influencing disease outcomes and therapeutic responses. Oresta et al. reported significant increases in Veillonella and Corynebacterium and a reduction in Ruminococcus in urine samples from BC patients, with these shifts correlating with disease advancement (46). Sun et al., using 2bRAD-M sequencing, found that NMIBC tissues exhibited higher microbial diversity than muscle-invasive bladder cancer (MIBC) tissues, with Ralstonia sp. dominating in MIBC, contrasting with Acinetobacter guillouiae and Anoxybacillus rupiensis in NMIBC (47). High-grade tumors were linked to reduced microbial diversity and richness. Bilski et al. reported lower Chao1 and Shannon indices in high-grade tumors compared to low-grade tumors, with notable sex-related differences in microbial composition at the phylum level (e.g., Firmicutes dominance in males, Proteobacteria in females) (48).
In recurrence, specific microbial patterns also emerged. Yao et al. identified higher levels of Mycolicibacterium and Streptomyces in patients with sustained responses to BCG therapy, while Knorr et al. found increased Lactobacillus levels in BCG responders, suggesting protective effects of these genera (45, 49). Conversely, Micrococcus and Brachybacterium were enriched in recurrent patients (39). Hussein et al. observed post-TURBT increases in Veillonella and Bifidobacterium in recurrent cases, while Escherichia-Shigella and Helococcus were more abundant in non-recurrent cases (50). Qiu et al. linked higher alpha diversity in recurrent patients with elevated abundances of Pseudomonas, Corynebacterium, and Acinetobacter, potentially facilitating immune evasion and tumor growth (51). Particular attention should be given to BCG-refractory tumors, where up to 30-50% of NMIBC patients fail to respond to BCG intravesical therapy, leading to higher recurrence and progression rates (52–54). Microbial signatures in these cases often show enrichment of certain taxa associated with poor response (e.g., reduced Lactobacillus or altered diversity), which may impair BCG-induced immune activation by promoting an immunosuppressive TME (40, 55, 56). Recent studies suggest that gut or urinary microbiota modulation (e.g., via probiotics or potential fecal microbiota transplantation in preclinical models) could influence BCG responsiveness by enhancing Th1 responses and modulating immune cell infiltration (57, 58). Mechanisms involve altered TLR signaling and cytokine profiles, highlighting the need for microbiome-based predictors of BCG failure to guide alternative therapies like radical cystectomy or ICIs (59).
Gut microbiota and BC
3.4
Emerging evidence indicates that the gut microbiota exerts distal effects on bladder carcinogenesis through systemic immune modulation and metabolic signaling—a concept known as the “gut–bladder axis.” A case-control study in Harbin indicated that BC patients exhibited a significant reduction in gut microbiota diversity, with a notable decrease in the abundance of Clostridium cluster XI and Prevotella. This reduction was closely associated with low fruit intake among BC patients, and a significant decrease in butyrate concentration in their feces was also observed (60). Butyrate, a crucial short-chain fatty acid, plays a vital role in anti-inflammatory processes and in protecting the intestinal barrier. Its reduction may increase intestinal permeability, leading to chronic inflammation induced by elevated levels of LPS and D-lactic acid, thereby accelerating the development of BC. Furthermore, evidence from Mendelian randomization studies indicates a significant causal relationship between specific gut microbiota, such as Bilophila, and BC. This may occur through the modulation of amino acid and NAD metabolism pathways, promoting the onset of BC (61). Other microbiota, such as Bifidobacterium and Actinobacteria, are also associated with an increased risk of BC, while Allisonella has been found to be linked with a reduced risk of both bladder and prostate cancers (62). These microbiota alterations may influence tumorigenesis by modulating host metabolic pathways, immune signaling, and inflammatory responses. In the field of cancer immunotherapy, further research has uncovered the role of gut microbiota in regulating the therapeutic efficacy of BC treatments. The abundance of Parabacteroides distasonis was significantly higher in healthy controls than in BC patients. This bacterium enhances the infiltration of CD4+ and CD8+ T cells within tumors and activates anti-tumor immune pathways, thereby significantly improving the efficacy of anti-PD-1 treatment (63). This finding suggests that specific gut microbiota could serve as a potential adjunct to immunotherapy.
Mechanistic interplay: microbes, immunosenescence, and TME
4
Microbial modulation of epithelial integrity and EMT activation
4.1
Microbial dysbiosis and EMT activation
4.1.1
Recent bioinformatics studies analyzing the microbial communities in BC have identified strong associations between specific microorganisms and the expression of EMT-related genes. Specifically, an analysis of tumor samples from over 400 patients with MIBC revealed significant correlations between various microorganisms, including E. coli, butyrate-producing bacterium SM4/1, and an Oscillatoria species, and the expression of classic EMT-related genes such as E-cadherin, vimentin, snail family transcriptional repressor 2 (SNAI2), snail family transcriptional repressor 3 (SNAI3), and twist family BHLH transcription factor 1 (TWIST1). Additionally, the study uncovered significant links between these microorganisms and the expression of extracellular matrix (ECM)-related genes, particularly those encoding collagen and elastin. These findings suggest that intratumoral microbiota may influence EMT and, consequently, clinical outcomes in BC (64). However, it is crucial to emphasize that these results are derived primarily from correlation-based bioinformatics analyses, and a direct causal relationship between microbial presence and EMT gene regulation remains to be established. While these associations provide compelling evidence for a potential microbial role in tumor progression, mechanistic insights into how these bacteria modulate EMT in BC are still lacking and require experimental validation.
Moreover, intratumoral bacteria are not randomly distributed but are highly organized within distinct ecological niches that are often characterized by immunosuppressive conditions and poor vascularization. By remodeling the TME and promoting cellular heterogeneity, bacteria may exert profound effects on tumor progression (65). Bacterial invasion can induce the upregulation of genes associated with inflammation, EMT, hypoxia response, and DNA repair, leading to the emergence of distinct cancer cell subpopulations with enhanced invasive potential. For example, in colorectal cancer (CRC), Fusobacterium nucleatum infection has been shown to drive the transition from collective migration to single-cell invasion, with significant activation of tumor progression signaling pathways (65). While these observations have been experimentally validated in CRC, direct evidence supporting a similar bacterial-driven EMT mechanism in BC is currently lacking. Thus, although bioinformatics analyses provide valuable insights into potential microbial contributions to EMT and tumor progression pathways, further in-depth mechanistic studies are necessary to confirm the direct role of specific bacteria in BC pathogenesis.
Bacterial ECM degradation and remodeling
4.1.2
In BC, bacteria residing within the tumor stroma may influence extracellular matrix (ECM) integrity through the secretion of proteolytic enzymes. Bacterial proteases such as collagenase, elastase, and alkaline protease are capable of degrading key ECM components including collagen and elastin, thereby weakening structural barriers and potentially facilitating bacterial persistence (66, 67). Among these enzymes, collagenases are particularly relevant due to their broad substrate specificity and their ability to disrupt intercellular junctions and tissue organization (68–70).
Additionally, several Gram-positive bacteria produce hyaluronidase, an enzyme that hydrolyzes hyaluronic acid (HA), a major ECM component involved in tissue cohesion and cell adhesion. The degradation of HA provides nutrients for bacterial metabolism and may enhance tissue permeability, conditions that could theoretically support local invasion (71).
Beyond structural effects, bacterial proteases have been implicated in modulating host immune signaling in other pathological contexts by degrading cytokines and growth factors (72, 73). However, direct evidence of such mechanisms in BC remains scarce. While these findings collectively suggest that bacterial proteolytic activity might contribute to ECM remodeling within the bladder microenvironment (Figure 2), further mechanistic studies are needed to confirm its direct role in tumor progression and immune modulation in BC.
In progressive bladder cancer, cancer cells and CAFs grow intertwined. CAFs create an immunosuppressive environment that facilitates the rapid proliferation of cancer cells. Along with inflammation induced by bacterial infections, they manipulate and exploit the immune response, synergistically driving rapid cancer progression.
Post-translational modulation by microbes
4.1.3
In addition to enzymatic ECM degradation, bacteria can also induce post-translational modifications (PTM) of host proteins, altering the biochemical and physical properties of the TME. For instance, Porphyromonas gingivalis, a known periodontal pathogen, produces peptidylarginine deiminase, an enzyme responsible for citrullination of collagen type I, which can disrupt the interactions between fibroblasts and collagen fibers (74, 75). These modifications may alter ECM stiffness and architecture, further promoting cancer cell invasion and metastasis. However, the functional significance of such bacterial-driven ECM modifications in BC and other solid tumors remains unclear. Although PTM-induced ECM alterations have been observed in multiple cancer types, their specific contribution to BC progression is yet to be fully elucidated and requires further experimental investigation.
Immunosenescence: the aging immune system and infection susceptibility
4.2
Immunosenescence—the progressive decline of immune function associated with aging—represents a critical but underappreciated determinant of host susceptibility to infection-driven carcinogenesis. In the context of bladder cancer (BC), recurrent microbial exposure and chronic urinary tract infections act as persistent antigenic stimuli that accelerate immune exhaustion and cellular senescence. This infection-induced immune aging not only impairs pathogen clearance but also fosters a permissive microenvironment that supports tumor initiation and progression (76, 77). Therefore, immunosenescence should not be viewed solely as an age-related phenomenon but as an integral component of the infection–microbiota–tumor axis.
Immune aging in the TME
4.2.1
Such senescent immune phenotypes are further aggravated by recurrent infections, particularly in the bladder where chronic bacterial exposure induces continuous antigenic stimulation. This suggests that infection not only coexists with immune aging but actively accelerates it, shaping a tumor-permissive environment. Senescence affects both innate and adaptive immune cells, compromising their surveillance, cytotoxicity, and signaling capacity. CD8^+^ T cells exhibit classic immunosenescent phenotypes: loss of CD28, upregulation of KLRG1 and CD57, and metabolic dysregulation involving oxidative phosphorylation, ROS accumulation, and mitochondrial remodeling (78–86). Unlike exhausted T cells, senescent T cells are metabolically active but irreversibly dysfunctional, limiting the efficacy of checkpoint blockade therapies (87, 88). Thymic involution further restricts naïve T cell output, exacerbating immune decline. Clinical and preclinical studies have shown that the TME directly induces immunosenescence in tumor-infiltrating lymphocytes. For instance, CD8^+^ T cells in breast cancer brain metastases lose migratory and cytotoxic function despite originating from healthy lymphoid niches (78, 89).
NK cells and myeloid compartments are similarly affected. NK cells in the elderly show altered subset distributions (e.g., CD56dim accumulation), reduced activating receptor expression, and metabolic rewiring induced by tumor-secreted cAMP (90–92). Aging macrophages often display reduced antigen presentation and altered Toll-like receptor (TLR) signaling; however, their polarization state appears context-dependent. Many studies report a shift toward M2-like, pro-tumor phenotypes that reinforce immunosuppression and angiogenesis (93–101). However, others have documented sustained or even heightened pro-inflammatory M1-like activity associated with systemic “inflammaging” (102, 103). This bidirectional plasticity underscores the complexity of macrophage aging within the TME. Regarding BCG therapy in BC, which promotes macrophage repolarization from M2 (immunosuppressive) to M1 (pro-inflammatory) phenotypes to enhance anti-tumor immunity (104, 105), comparative analyses with other cancers reveal limitations. In colorectal and lung cancers, M1 macrophages can paradoxically promote tumor progression by secreting pro-angiogenic factors or fostering chronic inflammation, leading to mixed M1/M2 states that support metastasis (106). Unlike BC, where BCG-induced M1 shifts are often beneficial in NMIBC, these approaches have been less successful in solid tumors like melanoma, where M1 activation may exacerbate TME heterogeneity and resistance (107, 108). This highlights the tumor-specific context of macrophage reprogramming and the need for targeted strategies to avoid unintended pro-tumor effects. Senescent neutrophils contribute to tumor progression through the senescence-associated secretory phenotype (SASP), promoting myeloid-derived suppressor cells (MDSCs) recruitment and ECM remodeling. Markers such as TREM2 and CXCR4+CD62L^low phenotypes are associated with metastasis and therapeutic resistance (109–115). In addition, senescent dendritic cells, often modulated by tumor-derived γδ regulatory T cells (Tregs), suppress effector T cell differentiation via PD-L1 and STAT3 signaling (116).
Impact on tumor surveillance and chronic inflammation
4.2.2
Infection acts as both a trigger and an amplifier of immunosenescence. Recurrent bacterial colonization, especially by uropathogens, perpetuates inflammatory signaling that exhausts immune competence. Immunosenescence also impacts systemic immune equilibrium, particularly mucosal immunity and microbial recognition. B cell senescence manifests as reduced bone marrow output, metabolic inflammation, and impaired antibody production (117–121). This state not only affects pathogen clearance but also contributes to T cell dysfunction via pro-inflammatory cytokines and clonal restriction of the T cell receptor repertoire (119). These immune alterations collectively diminish host capacity to eliminate pathogens, creating a permissive environment for microbial colonization and chronic infection. In the bladder, age-related immune decline may promote the persistence of uropathogens and delay resolution of UTIs, especially in elderly patients. This in turn can lead to prolonged inflammation, epithelial damage, and microbial-driven carcinogenesis. From a translational perspective, immunosenescence represents a potential therapeutic target. Rejuvenation strategies, such as senolytic therapies, metabolic reprogramming, and targeted epigenetic modulation, may help restore immune competence in elderly patients and improve response to both immunotherapy and microbiome-modulating interventions. Thus, age-related immune decline and infection-induced inflammation converge to form a pathogenic feedback loop that sustains microbial persistence and tumor-promoting chronic inflammation in the bladder.
Immune reprogramming in response to microbial infections
4.3
Uropathogenic E. coli and host immune modulation
4.3.1
The innate immune system promptly detects uropathogenic Escherichia coli (UPEC) through pattern recognition receptors (PRRs), particularly Toll-like receptor 4 (TLR4), which recognizes bacterial LPS. Activation of TLR4 initiates the NF-κB signaling pathway and stimulates the release of pro-inflammatory cytokines such as IL-6, IL-8, and TNF-α, which recruit neutrophils and macrophages (122–125). These immune cells utilize phagocytosis, ROS, and neutrophil extracellular traps (NETs) to eliminate bacterial invaders (126–129). Macrophages further contribute to immune activation through secretion of chemokines such as CXCL1 and CCL2, while dendritic cells (DCs) function as antigen-presenting cells that activate adaptive immune responses by priming T cells (130–134). Interestingly, bacterial products may also exert anti-tumor effects. For instance, E. coli supernatants downregulate c-MYC and pro-inflammatory cytokines like IL-1β and CCL2, while upregulating NQO1 expression. These changes promote apoptosis via BAX activation and suppression of anti-apoptotic BCL2 in bladder cancer cells (135–138). However, while bacterial-induced apoptosis may initially appear beneficial, it can also modulate the TME in ways that support immune evasion or chronic inflammation. UPEC adheres to bladder epithelial cells via type 1 pili and FimH adhesin, initiating actin reorganization and PI3-kinase signaling to promote bacterial internalization (139–143) (Figure 3). The formation of intracellular bacterial communities (IBCs) enables UPEC to evade host immunity, persist intracellularly, and drive chronic inflammation—factors that may contribute to bladder cancer progression.
Bladder infections caused by E. coli activate the innate immune response. Immune cells are recruited to the infection site to capture and clear E. coli. Neutrophils and macrophages eliminate E. coli through phagocytosis, while mast cells facilitate the shedding and death of epithelial cells infected by E. coli. E. coli can evade the acute inflammatory response by invading and colonizing host cells.
Infection-induced epithelial exfoliation and barrier disruption
4.3.2
Bladder epithelial cell exfoliation is a key host defense strategy against UTI. Upon E. coli infection, bladder epithelial cells secrete IL-1β, which recruits mast cells (MCs) to the infection site. These MCs release granules rich in chymase and tryptase, triggering apoptosis and exfoliation of infected cells (144–147). This response reduces bacterial burden and promotes epithelial renewal. Notably, mast cells undergo functional switching from a pro-inflammatory to an anti-inflammatory state approximately six hours post-infection, facilitating immune resolution and tissue repair (146, 148). UPEC-derived virulence factors, such as hemolysin, may further contribute to epithelial disruption (140, 149). While exfoliation is essential for bacterial clearance, it may also expose basal epithelial cells to inflammation-induced stress, potentially initiating or exacerbating malignant transformation.
Tumor susceptibility to bacterial invasion
4.4
Morphological and barrier defects
4.4.1
BC cells exhibit significant morphological alterations compared to normal urothelial cells, which enhance their susceptibility to bacterial infection. Normal urothelial cells form a well-organized epithelial barrier with tight and adherens junctions, preventing bacterial adherence and protecting against infection (150–152). These cells are typically flat, multilayered, and exhibit apical-basal polarity, with smooth membranes and limited adhesion sites. Tight junction proteins, such as Occludin, Claudins, and E-cadherin, play a crucial role in maintaining this barrier function (153–155).
In contrast, bladder cancer cells display surface microvilli proliferation, pseudopod formation, and altered glycosylation patterns, including the abnormal expression of Tn and sialyl-Tn antigens, which provide additional bacterial adhesion sites (156, 157). Loss of cellular polarity and weakened intercellular junctions result in larger gaps between cells, exposing extracellular matrix components like fibronectin and laminin, which serve as binding sites for bacterial adhesion (158). Moreover, bladder cancer cells often resist infection-induced apoptosis, partly due to increased BCL2 expression, which allows them to persist in inflammatory environments triggered by infection, further promoting tumor proliferation and invasion (Figure 4).
In superficial bladder cancer, acute inflammatory responses triggered by bacterial infections can significantly promote cancer progression. While acute inflammation can inhibit and kill cancer cells, cancer cells differ from normal urothelial cells by upregulating anti-apoptotic genes such as BCL2, thereby suppressing apoptosis. Infected cancer cells are less prone to detachment or death, exhibit morphological changes, and have disrupted intercellular connections, leading to widespread invasion and intracellular bacterial colonization. The deep invasion of acute inflammation can cause substantial damage to the stroma. Cancer cells are more prone to invasion and growth, and can drive the malignant transformation of fibroblasts through inflammation.
Clinically, these morphological changes contribute to the increased risk of UTIs in BC patients, with bacterial adhesion exacerbating disease progression. Targeting bacterial adhesion, for instance by inhibiting lectin-glycan interactions, may reduce colonization. These altered morphological features could also serve as biomarkers for assessing infection risk in BC.
Immunosuppressive tumor states
4.4.2
The immunosuppressive microenvironment in bladder cancer facilitates bacterial colonization by dampening the host’s immune response. In healthy urothelial tissue, antimicrobial peptides like β-defensins, along with cytokines such as IL-6 and IL-8, are secreted to recruit immune cells and combat pathogens (159–162). However, BC cells often secrete immunosuppressive cytokines, including TGF-β and IL-10, which impair immune cell activity and local immune responses (163–166). Treg infiltration further diminishes effector T cell function, hindering the clearance of pathogens and tumor cells (167).
BC cells also frequently downregulate MHC class I expression, reducing antigen presentation and immune recognition of both bacterial pathogens and tumor cells (168, 169). This creates an immunosuppressive TME that favors bacterial persistence. Studies have shown that bacterial presence in BC tissues correlates with increased infiltration of CD66b+ neutrophils and higher levels of immunosuppressive molecules like ARG1 and CTLA4. Additionally, activation of mitogen-activated protein kinase (MAPK) signaling in this context supports chronic bacterial colonization and inflammation, potentially accelerating tumor progression (65).
Clinically, targeting immunosuppressive pathways—such as blocking ARG1 or CTLA4—could enhance the immune system’s ability to clear both bacterial infections and cancer cells. Moreover, microbiome-based interventions, such as probiotics or engineered bacteria, may help modulate the TME and reduce bacterial infections, offering a potential complement to conventional cancer therapies.
Gut microbiota and immunosenescence
4.5
Immunosenescence, the gradual decline in immune system function during aging, is closely associated with chronic inflammation (inflammaging) and the onset of age-related diseases, such as cancer and infections. The gut microbiota plays a central role in this process. With aging, the composition and functionality of the gut microbiota undergo significant changes, manifested as a reduction in diversity, a decrease in beneficial bacteria (e.g., Faecalibacterium prausnitzii and Akkermansia muciniphila), and an increase in pro-inflammatory bacteria (e.g., Enterobacteriaceae and Proteobacteria) (170). These changes are closely related to T-cell aging, especially in middle-aged and older individuals. Individuals with lower gut microbiota richness show significantly higher mRNA biomarkers of T-cell senescence, and Shannon diversity is negatively correlated with the epigenetic age of T-cell DNA methylation (171). Additionally, metagenomic analysis of centenarians (≥90 years) revealed that age-related changes in the gut microbiota, chronic inflammation, and microbial metabolic reprogramming are key drivers of immunosenescence (172). These alterations in the gut microbiota accelerate the process of immune aging through various mechanisms. This process is accompanied by functional decline in specific immune cells, such as long-term stimulation by symbiotic bacteria that leads to the proliferation arrest and aging of germinal center (GC) B cells in Peyer’s patches (PPs), resulting in the loss of PP function. This damage, through bacterial-dependent compensatory mechanisms, promotes further aging of B cells in lymphoid follicles (ILFs), ultimately leading to a significant reduction in IgA production and diversity. This weakens the regulation of the gut microbiota, creating a vicious cycle between gut microbiota and immunosenescence (173).
Interventions targeting the gut microbiota are considered an important strategy to delay immunosenescence. For example, probiotics, such as Lactobacillus plantarum, can restore aging-related dendritic cell function and improve gut immune regulation in elderly individuals (174). Lifestyle interventions, such as caloric restriction, can reshape the gut microbiota and promote the functional recovery of T cells and B cells, thereby mitigating immunosenescence (175). Furthermore, fecal microbiota transplantation and combined interventions with prebiotics and probiotics have been shown to improve the composition of the gut microbiota in elderly patients, enhancing their response to immune checkpoint blockade (ICB) therapy, which provides anti-tumor benefits (176). Studies have also demonstrated that ICB therapy is associated with the enrichment of specific microbiota, particularly in elderly patients. The modulation of age-related gut microbiota is considered a key factor in improving ICB efficacy (177).
Therapeutic implications and future perspectives
5
The future of BC treatment lies in innovative, integrated strategies that combine microbiome modulation and immune therapies. These approaches focus on overcoming challenges such as microbial dysbiosis and immunosenescence, leveraging cutting-edge technologies like artificial intelligence (AI) and CRISPR for precision medicine. The integration of gut–bladder axis interventions with microbiome–immune therapies provide new avenues to improve clinical outcomes for BC patients. This chapter explores three major therapeutic strategies that hold great promise in advancing BC treatment.
Personalized microbiota modulation
5.1
Microbiome alterations in BC present a unique opportunity for personalized treatment strategies. Dynamic changes in microbial communities, such as shifts in urinary or stool microbiota, offer potential biomarkers for tumor progression and therapeutic response. Non-invasive microbiome analyses can enable real-time monitoring, guiding therapeutic interventions. For instance, machine learning algorithms can identify specific taxa like Lactobacillus or Veillonella, which are associated with either tumor progression or favorable responses to immunotherapy. Additionally, CRISPR-based microbial engineering could be harnessed to generate beneficial metabolites like short-chain fatty acids (SCFAs) or indole derivatives, potentially enhancing immune responses and improving the TME. Personalized microbiome modulation could significantly optimize treatment efficacy and patient outcomes (178).
Microbiome–immunotherapy combinations
5.2
The combination of microbiome modulation with immunotherapies represents a highly promising therapeutic strategy. Recent studies have shown that prebiotics, synbiotics, and microbiota-derived metabolites, such as butyrate, can work synergistically with immune checkpoint inhibitors (ICIs). These compounds enhance tumor-infiltrating lymphocyte (TIL) activity and modulate immunosuppressive cells like MDSCs and Tregs. Additionally, engineered microbial therapeutics that secrete immune-activating molecules (e.g., IL-15, GM-CSF) or anti-inflammatory agents (e.g., IL-10) could help reverse immunosenescence, particularly in aging populations. Preclinical studies have shown that Lactobacillus reuteri can translocate into tumors and release the tryptophan metabolite indole-3-aldehyde (I3A), which activates the aryl hydrocarbon receptor in CD8^+^ T cells and enhances anti-PD-L1 immune checkpoint blockade efficacy in melanoma models (179). Additionally, engineered bacterial platforms releasing PD-L1 nanobodies have demonstrated tumor-localized immune activation and reduced systemic toxicity in breast cancer models, highlighting the potential of microbiome-based strategies to modulate the TME and improve immunotherapy outcomes (180). While these findings suggest a promising direction for microbiome engineering in cancer therapy, comparable work specific to bladder cancer models has not yet been reported. This combination approach has the potential to enhance immune responses during various stages of treatment, from reducing preoperative infection risks to boosting immune memory during ICI therapy. Future research will focus on optimizing microbiome–immunotherapy interactions and tailoring these approaches to individual patient needs.
Gut–bladder axis therapeutic targeting
5.3
The interaction between the gut and bladder microbiota plays a crucial yet underexplored role in BC progression. Gut-derived metabolites, such as SCFAs and indoles, influence bladder immunity through systemic circulation and can modulate the bladder’s immune microenvironment. Targeting this “gut-bladder axis” with therapeutic interventions could offer a novel approach to improving the TME. For example, dietary modifications, such as high-fiber diets, or probiotic formulations that promote butyrate production, could boost systemic T-cell regeneration and enhance TIL activity within the bladder. These strategies could potentially reduce chronic inflammation, improve antigen presentation, and modulate the immune responses in the bladder, ultimately contributing to better treatment outcomes (178).
Multi-modal microbiome therapies
5.4
Future BC treatments will likely involve multi-modal strategies that combine microbiome-based therapies with conventional cancer treatments. Personalized microbiome modulation can complement traditional therapies like chemotherapy and radiotherapy, as well as advanced treatments such as ICIs. Customized microbial formulations may also enhance post-surgical recovery, improve patients’ immune response, and reduce recurrence rates in high-risk individuals. Furthermore, microbiome interventions could be incorporated into tumor vaccines to boost long-term anti-tumor immunity. As microbiome data accumulation accelerates, AI will play a critical role in optimizing these multi-modal strategies by identifying microbial targets, predicting patient-specific responses, and enabling truly personalized therapies. Examples of enhanced BCG-based approaches in bladder cancer include the use of PD-1/PD-L1 inhibitors such as pembrolizumab, which as monotherapy has demonstrated complete response rates of ~40% in BCG-unresponsive NMIBC cohorts (181). Recombinant BCG strains engineered to express IL-15 fused with antigen 85B have shown enhanced immunogenicity and prolonged survival in preclinical mouse bladder cancer models, associated with increased neutrophil and chemokine responses (182). Additionally, BCG combined with chemotherapy agents such as gemcitabine is being evaluated in clinical settings, with some early studies reporting promising response rates, though results remain preliminary and variable (183).
Conclusion
6
The relationship between the microbiome and BC is increasingly recognized as a critical factor in tumor initiation, progression, and recurrence. Both urinary and gut microbiota have significant roles in shaping the TME, with microbial infections serving as key drivers of cancer development. Disruptions in microbial communities—microbial dysbiosis—are strongly associated with chronic inflammation, immune modulation, and alterations in urothelial integrity, all of which contribute to tumor progression and metastasis. Bacterial infections, particularly those involving uropathogenic species, exacerbate these processes, facilitating the initiation and invasiveness of BC.
Infection-induced mechanisms, including microbial dysbiosis, drive important changes in the immune landscape of the TME. These changes are often exacerbated by immunosenescence, which weakens immune surveillance and increases susceptibility to persistent infections. Immunosenescence, while not the primary driver of BC, enhances the persistence of microbial dysbiosis by impairing the body’s ability to mount effective immune responses against both pathogens and tumor cells. This immune decline creates a favorable environment for tumorigenesis, as chronic inflammation and microbial imbalance promote immune evasion and tumor progression.
Future research should focus on elucidating how the gut and urinary microbiota interact to influence BC, particularly through their impact on immune responses and TME remodeling. Understanding the mechanisms by which microbial dysbiosis influences the development of BC will be essential for the development of novel diagnostic and therapeutic approaches. Microbiome-based therapies, particularly those targeting microbial imbalances and combined with immune modulation, offer promising avenues for personalized BC treatment. A more comprehensive understanding of these interactions will not only advance our knowledge of BC pathogenesis but also provide new strategies for improving early detection, prognosis, and treatment outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Compérat E Amin MB Cathomas R Choudhury A De Santis M Kamat A . Current best practice for bladder cancer: a narrative review of diagnostics and treatments. Lancet. (2022) 400:1712–21. doi: 10.1016/s 0140-6736(22)01188-6, PMID: 36174585 · doi ↗ · pubmed ↗
- 2Antoni S Ferlay J Soerjomataram I Znaor A Jemal A Bray F . Bladder cancer incidence and mortality: A global overview and recent trends. Eur Urol. (2017) 71:96–108. doi: 10.1016/j.eururo.2016.06.010, PMID: 27370177 · doi ↗ · pubmed ↗
- 3Siegel RL Miller KD Wagle NS Jemal A . Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763, PMID: 36633525 · doi ↗ · pubmed ↗
- 4Burger M Catto JW Dalbagni G Grossman HB Herr H Karakiewicz P . Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. (2013) 63:234–41. doi: 10.1016/j.eururo.2012.07.033, PMID: 22877502 · doi ↗ · pubmed ↗
- 5Mantica G Terrone C Der Merwe AV . Bladder cancer and associated risk factors: the african panorama. Eur Urol. (2021) 79:568–70. doi: 10.1016/j.eururo.2020.11.041, PMID: 33280932 · doi ↗ · pubmed ↗
- 6Honeycutt J Hammam O Fu CL Hsieh MH . Controversies and challenges in research on urogenital schistosomiasis-associated bladder cancer. Trends Parasitol. (2014) 30:324–32. doi: 10.1016/j.pt.2014.05.004, PMID: 24913983 PMC 4085545 · doi ↗ · pubmed ↗
- 7Barsoum RS . Urinary schistosomiasis: review. J Adv Res. (2013) 4:453–9. doi: 10.1016/j.jare.2012.08.004, PMID: 25685452 PMC 4293885 · doi ↗ · pubmed ↗
- 8El-Rifai W Kamel D Larramendy ML Shoman S Gad Y Baithun S . DNA copy number changes in Schistosoma-associated and non-Schistosoma-associated bladder cancer. Am J Pathol. (2000) 156:871–8. doi: 10.1016/s 0002-9440(10)64956-5, PMID: 10702404 PMC 1876852 · doi ↗ · pubmed ↗